Multiscale Entropy Analysis of Heart Rate Variability for Assessing the Severity of Sleep Disordered Breathing

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection from Polysomnography (PSG), Definitions, and Patient Grouping
2.3. Heart Rate Variability and Multiscale Entropy Index (MEI) Analysis
- Define the data series x(n) with length N and the two parameters of m and r (where m = Embedded dimension of the vector; r = tolerance)
- Define N – m + 1 vectors, each of size m, composed as follows:
- Define d[um(i), um(j)] as the maximum value: d[um(i), um(j)] = max{|xi + k − xj + k|: 0 ≤ k ≤ m − 1}(i ≠ j). Calculate the number of d[um(i), um(j)] within distance r and calculate the ratio of the number to the total N – m for each value of i ≤ N − m + 1 and an average to all points is defined as:
- Increase the embedded dimension to m + 1, gives:
- Therefore, sample entropy (SE) is defined as:
2.4. Statistical Analysis
3. Results
3.1. Study Subjects
3.2. Frequency Domain Analysis of Heart Rate Variability
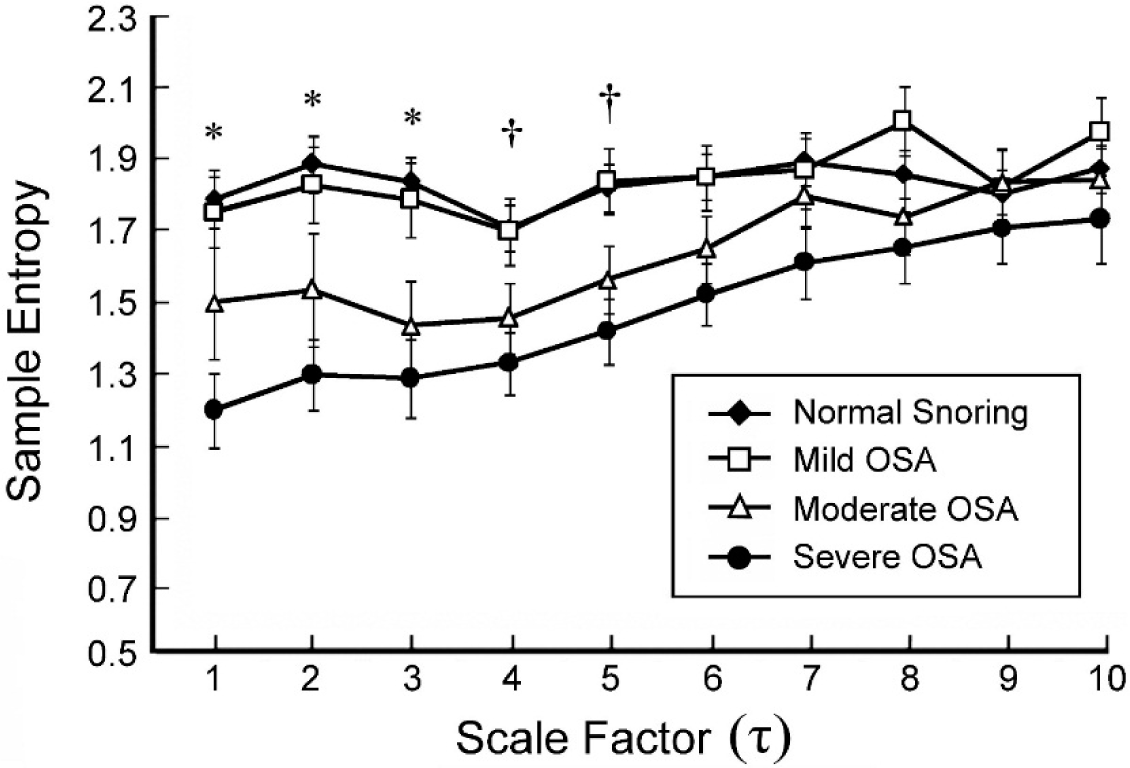
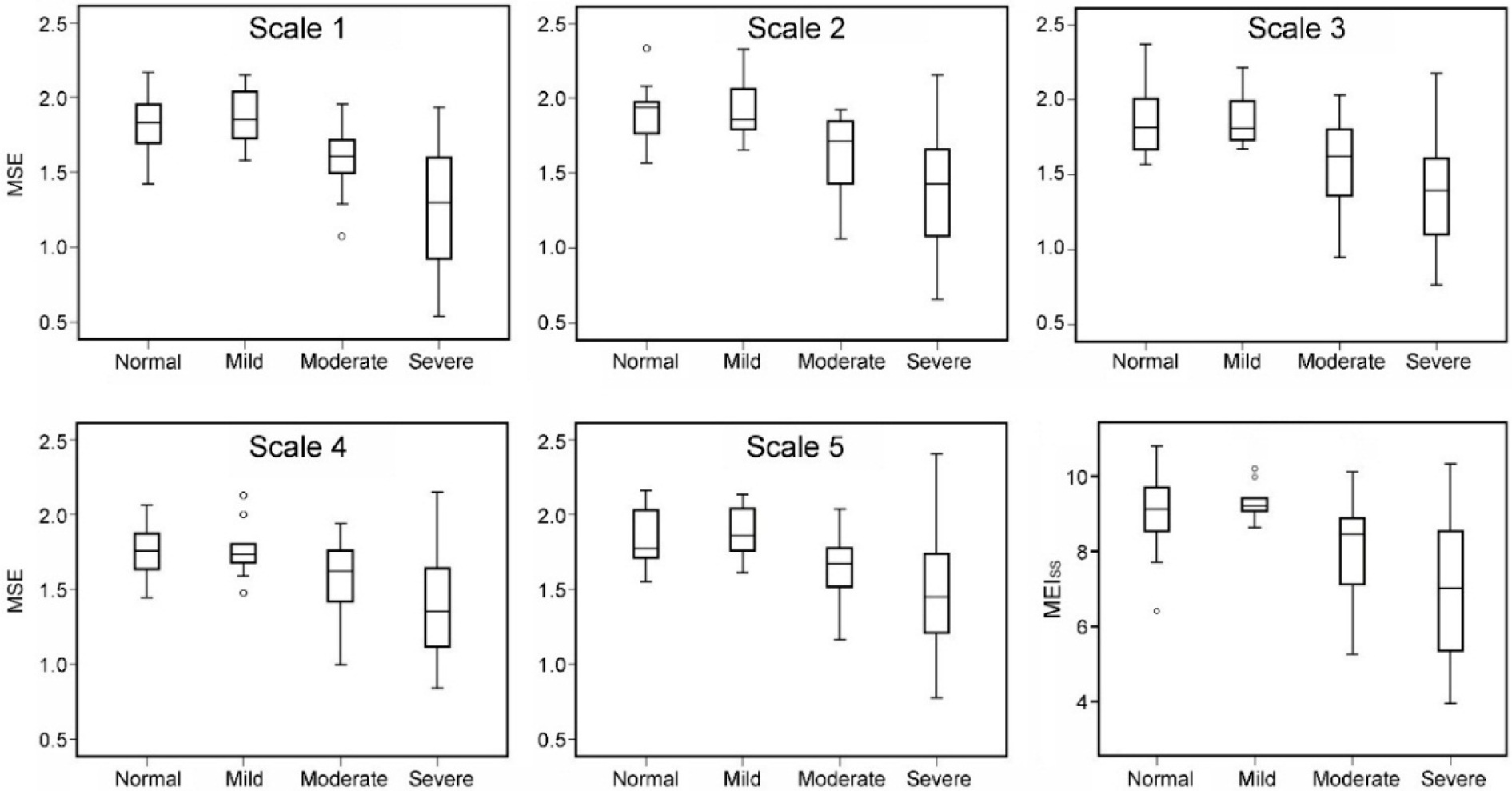
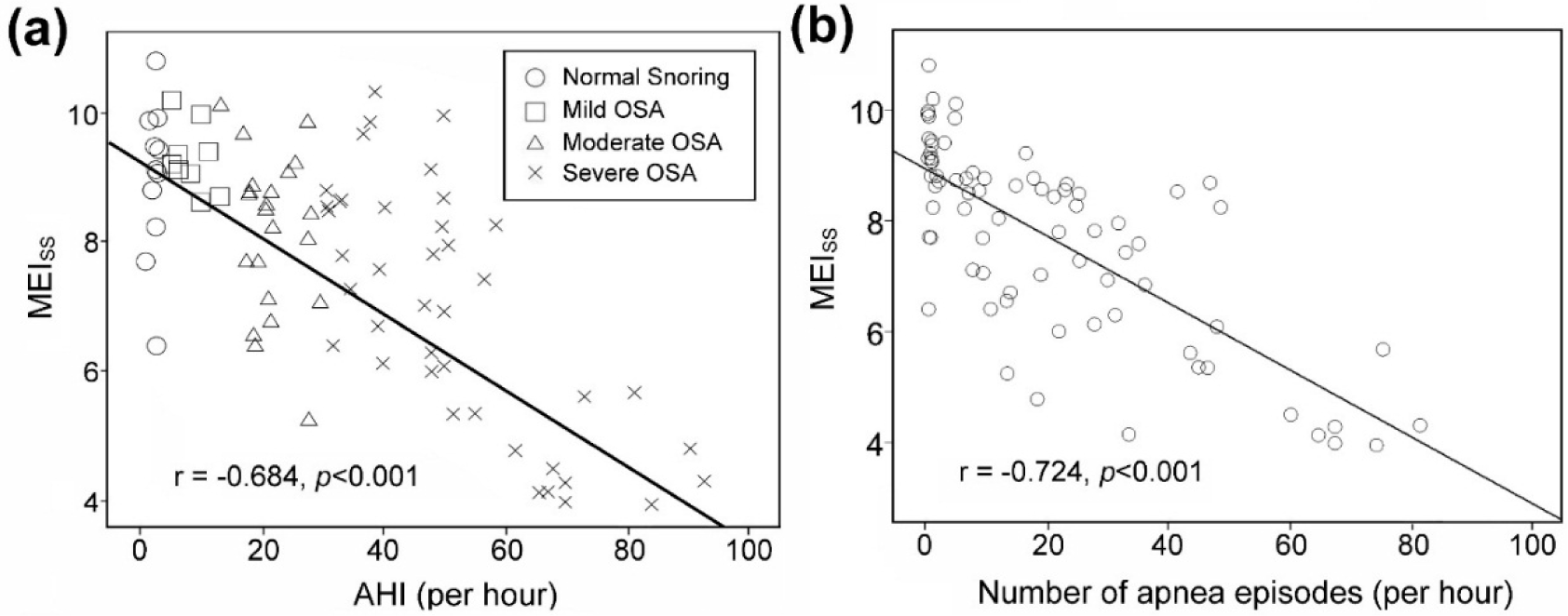
3.3. Multiscale Entropy Index for Groups
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fogel, R.B.; Malhotra, A.; White, D.P. Sleep 2: Pathophysiology of obstructive sleep apnoea/hypopnoea syndrome. Thorax 2004, 59, 159–163. [Google Scholar]
- Lopez-Jimenez, F.; Sert Kuniyoshi, F.H.; Gami, A.; Somers, V.K. Obstructive sleep apnea: Implications for cardiac and vascular disease. Chest 2008, 133, 793–804. [Google Scholar]
- Shepard, J.W., Jr. Hypertension, cardiac arrhythmias, myocardial infarction, and stroke in relation to obstructive sleep apnea. Clin. Chest Med. 1992, 13, 437–458. [Google Scholar]
- Society, A.T. Standards and indications for cardiopulmonary sleep studies in children. American Thoracic Society. Am. J. Respir. Crit. Care Med. 1996, 153, 866–878. [Google Scholar]
- Wolk, R.; Kara, T.; Somers, V.K. Sleep-disordered breathing and cardiovascular disease. Circulation 2003, 108, 9–12. [Google Scholar]
- Gottlieb, D.J.; Yenokyan, G.; Newman, A.B.; O’Connor, G.T.; Punjabi, N.M.; Quan, S.F.; Redline, S.; Resnick, H.E.; Tong, E.K.; Diener-West, M.; et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: The sleep heart health study. Circulation 2010, 122, 352–360. [Google Scholar]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065.
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar]
- Al-Angari, H.M.; Sahakian, A.V. Use of sample entropy approach to study heart rate variability in obstructive sleep apnea syndrome. IEEE Trans. Biomed. Eng. 2007, 54, 1900–1904. [Google Scholar]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of complex physiologic time series. Phys. Rev. Lett. 2002, 89. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71. [Google Scholar] [CrossRef]
- Lishner, M.; Akselrod, S.; Avi, V.M.; Oz, O.; Divon, M.; Ravid, M. Spectral analysis of heart rate fluctuations. A non-invasive, sensitive method for the early diagnosis of autonomic neuropathy in diabetes mellitus. J. Auton. Nerv. Syst. 1987, 19, 119–125. [Google Scholar]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar]
- Quan, S.F.; Gillin, J.C.; Littner, M.R.; Shepard, J.W. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurements techniques in clinical research. editorials. Sleep 1999, 22, 667–689. [Google Scholar]
- Lin, Q.-C.; Chen, L.-D.; Chen, G.-P.; Zhao, J.-M.; Chen, X.; Huang, J.-F.; Wu, L.-H. Association between nocturnal hypoxia and liver injury in the setting of nonalcoholic fatty liver disease. Sleep Breath 2014. [Google Scholar] [CrossRef]
- Elsenbruch, S.; Harnish, M.J.; Orr, W.C. Heart rate variability during waking and sleep in healthy males and females. Sleep 1999, 22, 1067–1071. [Google Scholar]
- Wu, H.T.; Hsu, P.C.; Sun, C.K.; Wang, H.J.; Liu, C.C.; Chen, H.R.; Liu, A.B.; Tang, C.J.; Lo, M.T. Assessment of autonomic dysfunction in patients with type 2 diabetes using reactive hyperemia. J. Theor. Biol. 2013, 330, 9–17. [Google Scholar]
- Kamath, M.V.; Fallen, E.L. Power spectral analysis of heart rate variability: A noninvasive signature of cardiac autonomic function. Crit. Rev. Biomed. Eng. 1993, 21, 245–311. [Google Scholar]
- Guzzetti, S.; Dassi, S.; Balsama, M.; Ponti, G.B.; Pagani, M.; Malliani, A. Altered dynamics of the circadian relationship between systemic arterial pressure and cardiac sympathetic drive early on in mild hypertension. Clin. Sci. (Lond.) 1994, 86, 209–215. [Google Scholar]
- Saul, J.P.; Arai, Y.; Berger, R.D.; Lilly, L.S.; Colucci, W.S.; Cohen, R.J. Assessment of autonomic regulation in chronic congestive heart failure by heart rate spectral analysis. Am. J. Cardiol. 1988, 61, 1292–1299. [Google Scholar]
- Malliani, A.; Lombardi, F.; Pagani, M. Power spectrum analysis of heart rate variability: A tool to explore neural regulatory mechanisms. Br. Heart J. 1994, 71, 1–2. [Google Scholar]
- Koenig, J.; Jarczok, M.N.; Ellis, R.J.; Warth, M.; Hillecke, T.K.; Thayer, J.F. Lowered Parasympathetic Activity in Apparently Healthy Subjects with Self-Reported Symptoms of Pain: Preliminary Results from a Pilot Study. Pain Pract. 2014. [Google Scholar] [CrossRef]
- Yeh, R.G.; Chen, G.Y.; Shieh, J.S.; Kuo, C.D. Parameter Investigation of Detrended Fluctuation Analysis for Short-term Human Heart Rate Variability. J. Med. Biol. Eng. 2010, 30, 277–282. [Google Scholar]
- Kuo, C.D.; Chen, G.Y. Comparison of three recumbent positions on vagal and sympathetic modulation using spectral heart rate variability in patients with coronary artery disease. Am. J. Cardiol. 1998, 81, 392–396. [Google Scholar]
- Wu, H.T.; Hsu, P.C.; Lin, C.F.; Wang, H.J.; Sun, C.K.; Liu, A.B.; Lo, M.T.; Tang, C.J. Multiscale entropy analysis of pulse wave velocity for assessing atherosclerosis in the aged and diabetic. IEEE Trans. Biomed. Eng. 2011, 58, 2978–2981. [Google Scholar]
- Baumert, M.; Javorka, M.; Seeck, A.; Faber, R.; Sanders, P.; Voss, A. Multiscale entropy and detrended fluctuation analysis of QT interval and heart rate variability during normal pregnancy. Comput. Biol. Med. 2012, 42, 347–352. [Google Scholar]
- Javorka, M.; Trunkvalterova, Z.; Tonhajzerova, I.; Javorkova, J.; Javorka, K.; Baumert, M. Short-term heart rate complexity is reduced in patients with type 1 diabetes mellitus. Clin. Neurophysiol. 2008, 119, 1071–1081. [Google Scholar]
- Turianikova, Z.; Javorka, K.; Baumert, M.; Calkovska, A.; Javorka, M. The effect of orthostatic stress on multiscale entropy of heart rate and blood pressure. Physiol. Meas. 2011, 32, 1425–1437. [Google Scholar]
- Weitzman, E.D.; Kripke, D.F.; Goldmacher, D.; McGregor, P.; Nogeire, C. Acute reversal of the sleep-waking cycle in man. Effect on sleep stage patterns. Arch. Neurol. 1970, 22, 483–489. [Google Scholar]
- Deng, Z.D.; Poon, C.S.; Arzeno, N.M.; Katz, E.S. Heart rate variability in pediatric obstructive sleep apnea, Proceedings of 28th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBS’06), New York, NY, USA, 30 August–3 September 2006; pp. 3565–3568.
- Toscani, L.; Gangemi, P.F.; Parigi, A.; Silipo, R.; Ragghianti, P.; Sirabella, E.; Morelli, M.; Bagnoli, L.; Vergassola, R.; Zaccara, G. Human heart rate variability and sleep stages. Ital. J. Neurol. Sci. 1996, 17, 437–439. [Google Scholar]
- Cabiddu, R.; Cerutti, S.; Viardot, G.; Werner, S.; Bianchi, A.M. Modulation of the Sympatho-Vagal Balance during Sleep: Frequency Domain Study of Heart Rate Variability and Respiration. Front. Physiol. 2012, 3. [Google Scholar] [CrossRef]
- Mortara, A.; Sleight, P.; Pinna, G.D.; Maestri, R.; Prpa, A.; La Rovere, M.T.; Cobelli, F.; Tavazzi, L. Abnormal awake respiratory patterns are common in chronic heart failure and may prevent evaluation of autonomic tone by measures of heart rate variability. Circulation 1997, 96, 246–252. [Google Scholar]
- Narkiewicz, K.; Montano, N.; Cogliati, C.; van de Borne, P.J.; Dyken, M.E.; Somers, V.K. Altered cardiovascular variability in obstructive sleep apnea. Circulation 1998, 98, 1071–1077. [Google Scholar]
- Muzumdar, H.V.; Sin, S.; Nikova, M.; Gates, G.; Kim, D.; Arens, R. Changes in heart rate variability after adenotonsillectomy in children with obstructive sleep apnea. Chest 2011, 139, 1050–1059. [Google Scholar]
- Gula, L.J.; Krahn, A.D.; Skanes, A.; Ferguson, K.A.; George, C.; Yee, R.; Klein, G.J. Heart rate variability in obstructive sleep apnea: A prospective study and frequency domain analysis. Ann. Noninvasive Electrocardiol. 2003, 8, 144–149. [Google Scholar]
- Penzel, T.; Kantelhardt, J.W.; Grote, L.; Peter, J.H.; Bunde, A. Comparison of detrended fluctuation analysis and spectral analysis for heart rate variability in sleep and sleep apnea. IEEE Trans. Biomed. Eng. 2003, 50, 1143–1151. [Google Scholar]
- Grote, L.; Ploch, T.; Heitmann, J.; Knaack, L.; Penzel, T.; Peter, J.H. Sleep-related breathing disorder is an independent risk factor for systemic hypertension. Am. J. Respir. Crit. Care Med. 1999, 160, 1875–1882. [Google Scholar]
- Lavie, L.; Vishnevsky, A.; Lavie, P. Evidence for lipid peroxidation in obstructive sleep apnea. Sleep 2004, 27, 123–128. [Google Scholar]
- Papaioannou, V.E.; Chouvarda, I.; Maglaveras, N.; Dragoumanis, C.; Pneumatikos, I. Changes of heart and respiratory rate dynamics during weaning from mechanical ventilation: A study of physiologic complexity in surgical critically ill patients. J. Crit. Care 2011, 26, 262–272. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Normal Snoring (n = 11) | Mild OSA (n = 10) | Moderate OSA (n = 24) | Severe OSA (n = 45) | |
|---|---|---|---|---|---|
| Gender (men/women) | 7/4 | 8/2 | 14/10 | 43/2 | |
| Age (years) | 41 (50.0–36.0) | 45.5 (64.0–35.5) | 48.5 (59.7–48.5) | 46 (56.0–41.0) | |
| Body mass index (BMI, kg/m2) | 24.4 (25.0–22.1)‡ | 23.5 (28.0–22.0)‡ | 26.5 (30.57–22.62) | 26.8 (29.3–25.6) | |
| Neck circumference (cm) | 36 (37.5–33.0)‡ | 37 (39.0–34.7) | 36.5 (40.7–34.2) | 40 (42.0–37.6)† | |
| Sleep efficiency (%) | 88.6 (92.6–63.1) | 75.2 (93.0–63.1) | 83.7 (91.4–79.7) | 85.2 (89.4–75.0) | |
| LSaO2 (%) | 93 (95–87)* | 89.5 (91–82) | 83 (84–76) | 70 (82–59)† | |
| AHI (per hour) | 2.4 (2.7–1.8)₤ | 8.9 (10.3–5.8) | 21.1 (26.9–18.3) | 49.9 (67.3–38.8)† | |
| Breathing Frequency (Hz) | 0.216 (0.225–0.208)‡ | 0.223 (0.230–0.208) | 0.215 (0.222–0.201) | 0.143 (0.159–0.128)† | |
| RR interval(ms) | 1005 (1147–892) | 1018 (1133–942) | 986 (1058–930) | 977 (1017–905) | |
| HR(beats/min) | 59.7 (67.2–52.3) | 58.9 (63.8–52.9) | 60.8 (64.4–56.7) | 61.4 (66.3–58.9) | |
| Sleep Stage | Stage N1 (%) | 32.3 (43.7–10.2)‡ | 32.1 (34.7–17.8) | 29.2 (44.4–23.3) | 61.9 (76.7–40.5)† |
| Stage N2 (%) | 50.7 (59.7–39)‡ | 49.1 (58.5–45.4) | 47.9 (55.8–35.3) | 18.5 (40.0–7.8)† | |
| Stage N3 (%) | 0.9 (12.5–0.6)‡ | 0 (6.9–0) | 0.5 (5.4–0) | 0 (0.6–0) | |
| REM (%) | 16.5 (23.7–13.7) | 17.7 (24.2–10.8) | 18.6 (21.9–16.6) | 16.1 (19.9–14.1) | |
| Parameter | Normal Snoring | Mild OSA | Moderate OSA | Severe OSA |
|---|---|---|---|---|
| nLF | 0.36 (0.46–0.29) | 0.38 (0.56–0.24) | 0.45 (0.53–0.36) | 0.56 (0.61–0.43)* |
| nHF | 0.57 (0.65–0.38)‡ | 0.47 (0.72–0.35)¶ | 0.37 (0.50–0.30) | 0.29 (0.41–0.24) |
| LF/HF | 0.63 (1.24–0.44)† | 0.91 (1.59–0.33) | 1.13 (1.55–0.73) | 1.74 (2.51–1.06)* |
| Parameter | Normal Snoring | Mild OSA | Moderate OSA | Severe OSA |
|---|---|---|---|---|
| MEISS | 9.13 (9.89–8.24)* | 9.17 (9.55–8.69)* | 8.32 (8.88–6.84) | 7.02 (8.55–5.35) |
| MEILS | 9.43 (10.40–8.66) | 9.19 (10.36–8.78) | 9.15 (10.21–8.20) | 8.37 (9.68–7.12) |
© 2015 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, W.-Y.; Su, M.-C.; Wu, H.-T.; Lin, M.-C.; Tsai, I.-T.; Sun, C.-K. Multiscale Entropy Analysis of Heart Rate Variability for Assessing the Severity of Sleep Disordered Breathing. Entropy 2015, 17, 231-243. https://0-doi-org.brum.beds.ac.uk/10.3390/e17010231
Pan W-Y, Su M-C, Wu H-T, Lin M-C, Tsai I-T, Sun C-K. Multiscale Entropy Analysis of Heart Rate Variability for Assessing the Severity of Sleep Disordered Breathing. Entropy. 2015; 17(1):231-243. https://0-doi-org.brum.beds.ac.uk/10.3390/e17010231
Chicago/Turabian StylePan, Wen-Yao, Mao-Chang Su, Hsien-Tsai Wu, Meng-Chih Lin, I-Ting Tsai, and Cheuk-Kwan Sun. 2015. "Multiscale Entropy Analysis of Heart Rate Variability for Assessing the Severity of Sleep Disordered Breathing" Entropy 17, no. 1: 231-243. https://0-doi-org.brum.beds.ac.uk/10.3390/e17010231