
Imaging Techniques Used for Wound Healing Assessment: A Systematic Review Part 1 Chronic Wounds


1
Burns Centre, Queen’s University Hospital, University Hospitals Birmingham Foundation Trust, University of Birmingham, Scar Free Foundation for Conflict Wound Research, Birmingham B15 2TH, UK
2
Royal Victoria Infirmary, Newcastle NE1 4LP, UK
*
Authors to whom correspondence should be addressed.
Eur. Burn J. 2021, 2(4), 194-214; https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040015
Submission received: 11 September 2021
/
Revised: 12 October 2021
/
Accepted: 15 October 2021
/
Published: 19 October 2021
Abstract
:Background: chronic wounds are complex to manage and require an objective assessment for diagnosis and prognosis purposes. Therefore, this article aims to provide an overview of available noninvasive imaging techniques for chronic wound healing described in the literature. Methods: a systematic literature review using electronic databases was performed with appropriate “Mesh” terms. The primary outcome was the validity and reliability of the instrument, whilst the secondary outcome was its feasibility, such as speed of assessment, ease of use and cost of the tool. All studies underwent quality assessment of diagnostic accuracy studies (QUADAS) to ensure the quality of the data. Results: 44 articles were identified evaluating six wound assessment modalities. Most studies (n = 9) reported on a two-dimensional device with a mean error ranging from 1.9–5.1% and an inter/intra rater correlation over 0.9 with a high ICC (>95%). The average QUADAS score was 13, with the lowest being 9 and the highest being 14. Conclusion: this review collectively evaluates objective, reliable, quantitative, and innovative tools to assess wound healing objectively. The most superior wound measuring device was two dimensional. However, hyperspectral imaging had strong potential but required further development in its technology and future clinic validation studies.
1. Introduction
Chronic wounds are a significant and common cause of morbidity and mortality. These wounds are often multifactorial and pose a challenge to manage [1]. There are approximately 1,596,840 wounds in the U.K., costing the NHS £7.06 billion annually, excluding the cost of associated comorbidities to manage [2].
To compound this, multi-morbidity prevalence is estimated to increase in the ageing population. Over the next few years, individuals with four or more diseases will double along with increased numbers of cancer, respiratory disease, and diabetes [3]. This would result in higher rates of complex chronic wounds, significantly increasing the financial burden on the National Health Service.
Despite this, Guest et al., 2015, found that 30% of wounds lacked a defined diagnosis [2]. Without an accurate diagnosis, a wound management plan would be difficult. This leads to either wasting resources or worsening the disease, requiring more sophisticated and expensive wound management techniques.
This shortcoming is partly due to the problem with wound assessment techniques. Traditionally, wounds have been assessed visually [4] or with subjective methods such as scales [5]. These techniques are quick to complete and easy to implement; however, the evidence suggests that subjective assessments are operator dependent and have a degree of unavoidable bias, limiting their reliability [5].
An alternative to subjective wound assessment is using objective measurement tools that are quantified and not observer-dependent. There are several technologies available in the market which can be subcategories based on several quantitative modalities. The wound assessment can include measuring the wound dimension over time which correlates with healing potential [6]. Alternatively, several methods accurately calculate the changes in light absorption by the various skin structures, such as collagen, melanin and inflammatory cells, during the healing phases [7]. Finally, some modalities directly visualise the anatomical changes during wound healing, such as epithelisation and contraction of the wound by myofibroblast in real-time [8].
Aim
An objective evaluation of wounds is necessary to determine the progression of healing, which guides treatment strategies by providing a standardised, comparable assessment of wound characteristics.
The purpose of this review is to provide an overview of various noninvasive imaging techniques for chronic wound healing assessment described in the literature, subcategorised into anatomical, physiological, and wound dimension measurements.
2. Materials and Methods
2.1. Search Strategy
This systematic review was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist [9]. In April 2020, we searched PubMed, Scottish Network, EMBASE and Cochrane library for all available publications using the search terms “Wound healing”, “Monitoring, physiologic”, “perfusion imaging or mapping”, “regional blood flow or oximetry” and “healing potential”. Search terms were adapted for each database. All databases were searched from their date of inception up to July 2019. Full mesh terms are documented in the appendix. References for all papers were examined in detail, and additional relevant publications were included in the review.
2.2. Inclusion and Exclusion Criteria
Two investigators independently reviewed articles for inclusion and exclusion criteria. Disagreement was resolved after a discussion with the senior author. Studies must have been written in English with a title, abstract and full manuscript available. All study types, including case reports and case series, were included. Full publications were then reviewed to confirm the use of a contactless wound assessment device which measures healing in chronic wounds and does not need post imaging processing. All included articles must have evaluated the validity, reliability and feasibility of the device on measuring chronic wound healing.
2.3. Study Selection and Data Extraction
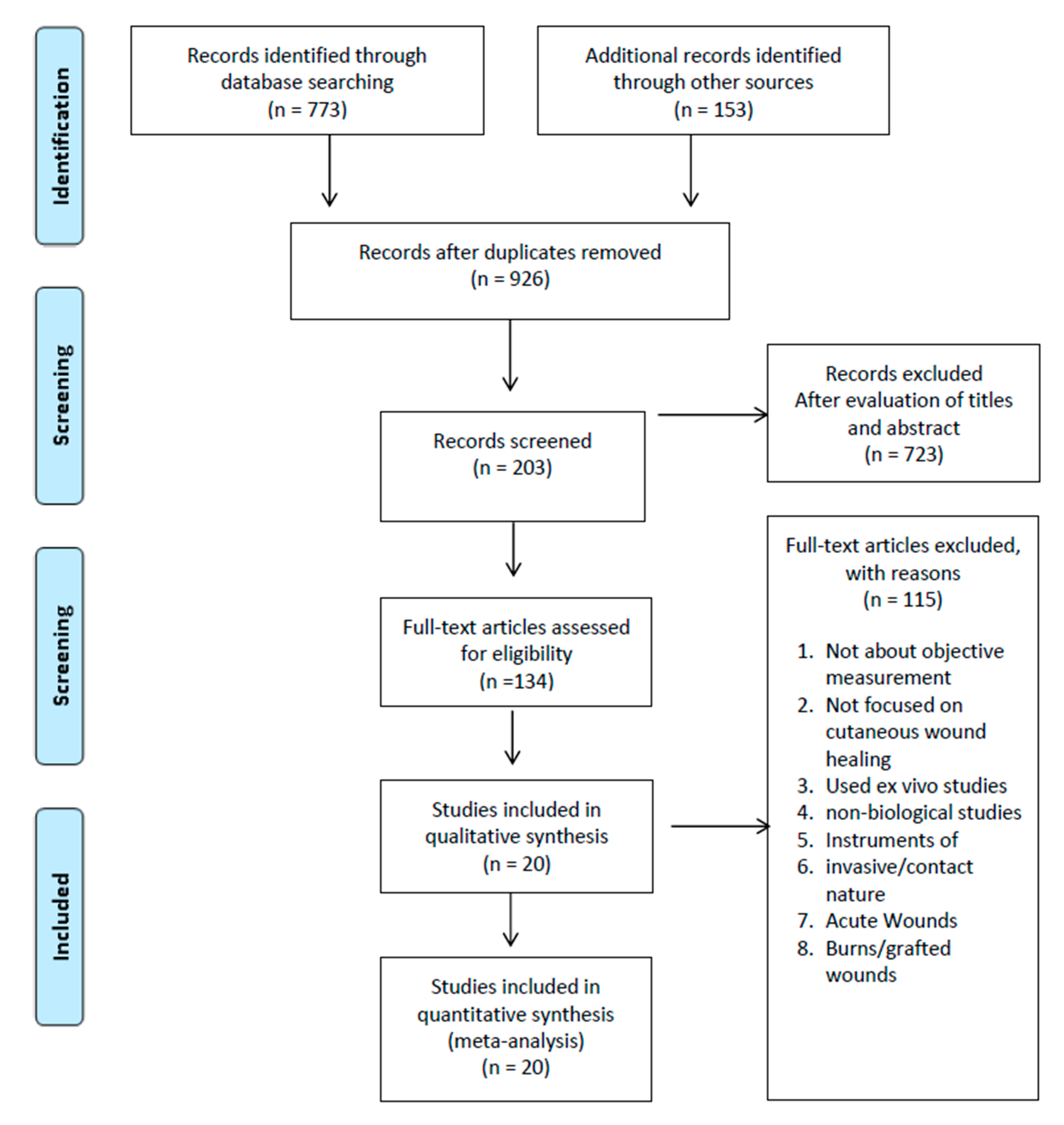
Titles and abstracts from the initial search from the various electronic databases were first uploaded onto Rayyan QCRI (Available at: https://rayyan.qcri.org (accessed on 9 November 2020)) for initial analysis of titles and abstracts. From this, full papers were retrieved, and studies to be included were identified. Data from the included studies were extracted into Microsoft Excel 2013 (Microsoft Corp, Redmond, WA, USA www.microsoft.com) for further analysis. Studies eligible for this review were defined using the population, intervention, comparison and outcome (PICO) strategy. The study populations were humans and animals with chronic wounds. Types of intervention were the instruments used in the evaluation of the wound. The comparator was assessed by histopathological analysis or clinical assessment where available. The primary outcome was the validity and reliability of the instrument, whilst the secondary outcome was the instrument’s feasibility, such as its speed of assessment, ease of use and the cost of the tool. Each article was reviewed for the year of publication, type of device used, type of wound, the number of cases, measurement statistics, wound healing outcomes and feasibility. Data were summarised based on the technology used, and a sub-analysis was done per category when possible. The authors checked data extraction, and any discrepancies were resolved by discussion. (Figure 1).
2.4. Quality Assessment
The quality score was judged based on the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool. The QUADAS tool consists of 14 phrased questions, each with a response category of “yes”, “no” or “unclear”. For each question, “yes” indicates adequate information and that the risk of bias is considered unlikely, whereas “no” indicates sufficient information but with a potential bias in the design. An “unclear” score indicates inadequate information to determine the potential risk of bias. The maximum score is 14, where “yes” is scored one and “no” or “unclear” are scored zero. A QUADAS score of 10 or greater was considered high quality with a low risk of bias, whereas a score of less than 10 indicates low quality with an increased risk of bias (Table 1).
3. Results
Seven hundred seventy-three articles were produced from the initial search, and an additional 153 were added when examining systematic reviews/metanalyses of a similar nature. In combination, a total of 926 articles were generated after duplications were removed. After filtering by reviewing titles and abstracts, 203 articles were chosen and 723 articles were excluded. Full articles were obtained, and a further 115 articles were removed after evaluating the full text. Reasons for this include not being about objective measurement, not being focused on cutaneous wound healing or that the study used ex vivo studies or non-biological studies, instruments of invasive/contact, acute wounds, burn wounds or grafted wounds. Thus, a total of 20 articles were selected in the final review. The selection process is outlined in Figure 1.
There was a total of 636 wounds, 599 wounds on humans and 37 on animals. All wounds categorised were chronic wounds. Six instruments were identified and subcategorised into morphological studies, physiological studies and wound area/volume studies.
All studies were published from 1998 and onwards. The flow chart of inclusion and exclusion studies is presented in Figure 1 below. Table 1 shows the QUADAS score for each included study. Overall, the studies’ were of high quality, with an average score ranging from 11 to 14. Table 2 summarises the scores for each instrument, covering each of the 14 QUADAS criteria.
3.1. Morphological Assessment
3.1.1. Optical Coherence Tomography
Optical coherence tomography (OCT) is an imaging technique that uses reflected light from tissue to create a three-dimensional cross-sectional construct of the skin structures. OCTs most commonly use infrared illumination, which is superimposed on a referenced light to generate a high resolution at a penetration depth of 2–3 mm. Thus, its use in superficial structures such as the eye, vessels and oral cavity have been well established [9] (Figure 2).
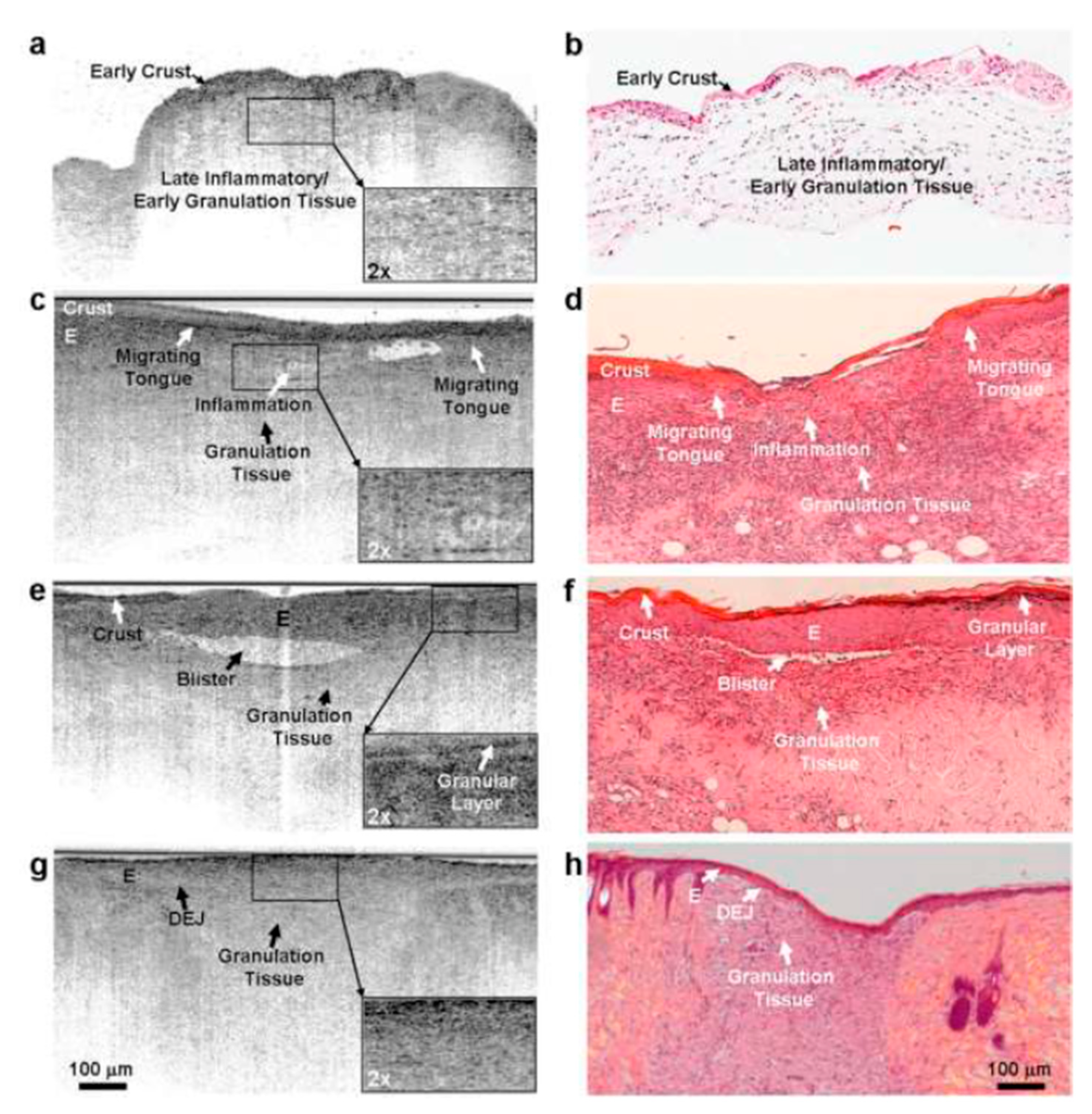
Monika Kuck et al., 2014, [8] looked at the chronic wounds of six patients to analyse each stage of healing and the appearance of OCT. The results of this were compared to archived histological sections. The author was able to identify and categorise findings on OCT and the stage of healing compared to the histological section, and found the differentiation of blood vessels to be difficult. They have concluded that OCT reduces the number of invasive steps but is not enough to appreciate the complexity of the wound at this stage.
Summary
In summary, OCT provides axial sectioned images of 3D tissue mass comparable to histological studies in humans and animals. In comparison to confocal microscopy, OCT has a lower resolution but has comparatively higher penetration. It was reported that OCT provides more detailed structural information than two-photon microscopies in large mass [10]. Currently, OCT is commercially available from NinePoint Medical and Thorlabs for $40,000.
3.1.2. Confocal Microscopy
Confocal microscopy (CLSM) is a noninvasive, real-time, near histological evaluation of the skin using either excitation and fluorescence detection or endogenous chromophores. It is based on the excitation of normal skin fluorophores such as NADH, FAD and collagen, which emit a fluorescence. An optically conjugated focal plane detector collected this. The data form a two-dimensional construct. Further acquired data from different depths are combined to form a three-dimensional image [11]. Endogenous fluorophores are essential markers of wound healing and can be used for diagnostic purposes [12].
Susanne Lange-Asschenfeldt et al., 2012, [11] studied 15 patients in three groups (superficial epidermal wound, superficial dermal wound and deep dermal wounds). Using the device, the authors could isolate and visualize each layer of the skin during healing, including changes at the dermal papillae and superficial dermal vasculature. This enables the investigator to observe the onset of inflammation, dynamics of wound closure and complete repair of acute wounds. CLSM required pre-examination preparation of the wound and was unable to differentiate inflammatory cells. The authors also noted low penetration depth (200 µm) due to significant resolution decay.
Summary
In summary, CLSM allows for cellular and subcellular analysis of healing wounds. However, it has a high cost and is limited to a small 8 × 8 mm imaging area. It is only helpful in minor acute superficial wounds, as deep wounds are complicated by slough build up, which detects underlying structures. CLSM is currently available through Vivascope in Amsterdam.
3.1.3. Multiphoton Tomography (MPT)
Multiphoton tomography is a high-resolution in vivo skin imaging technique. It is based on two-photon autofluorescence (A.F.) and second harmonic generation (SHG). The image is achieved by focusing laser radiation into the skin, which illuminates intrinsic fluorophores such as elastin and melanin, the photons released are then detected. The data attained are introduced into the software, which produces a high-resolution image. This is known as the post-processing technique.
Additionally, multiphoton tomography excites and detects electron carriers such as nicotinamide and flavin adenine dinucleotide, which provide information on the metabolic state. The high resolution and depth seen in multiphoton tomography are due to a combination of high tissue penetration due to low internal absorption and tight focusing of the laser beam. Tight focusing of the laser beam means a reduction in areas of non-focus and no photobleaching [13]. (Figure 3 and Figure 4).
In a study of ten chronic wounds and ten acute wounds, Karsten Konig et al., 2015, [14] demonstrated that MPT provided near-perfect information of skin architecture with two-photon autofluorescence imaging and functional images through time-resolved fluorescence detection. The device revealed inflammation, cellular proliferation, regeneration of the epidermal layer and reorganization of the dermal fibre net in acute wounds. In chronic wounds, a shift in the subcellular distribution of keratinocytes autofluorescence patterns was seen; thus, in combination with clinical observation and clinical scores, an evaluation of the degree of underlying chronic insufficiency can be made. The study, however, does not provide longitudinal readings.
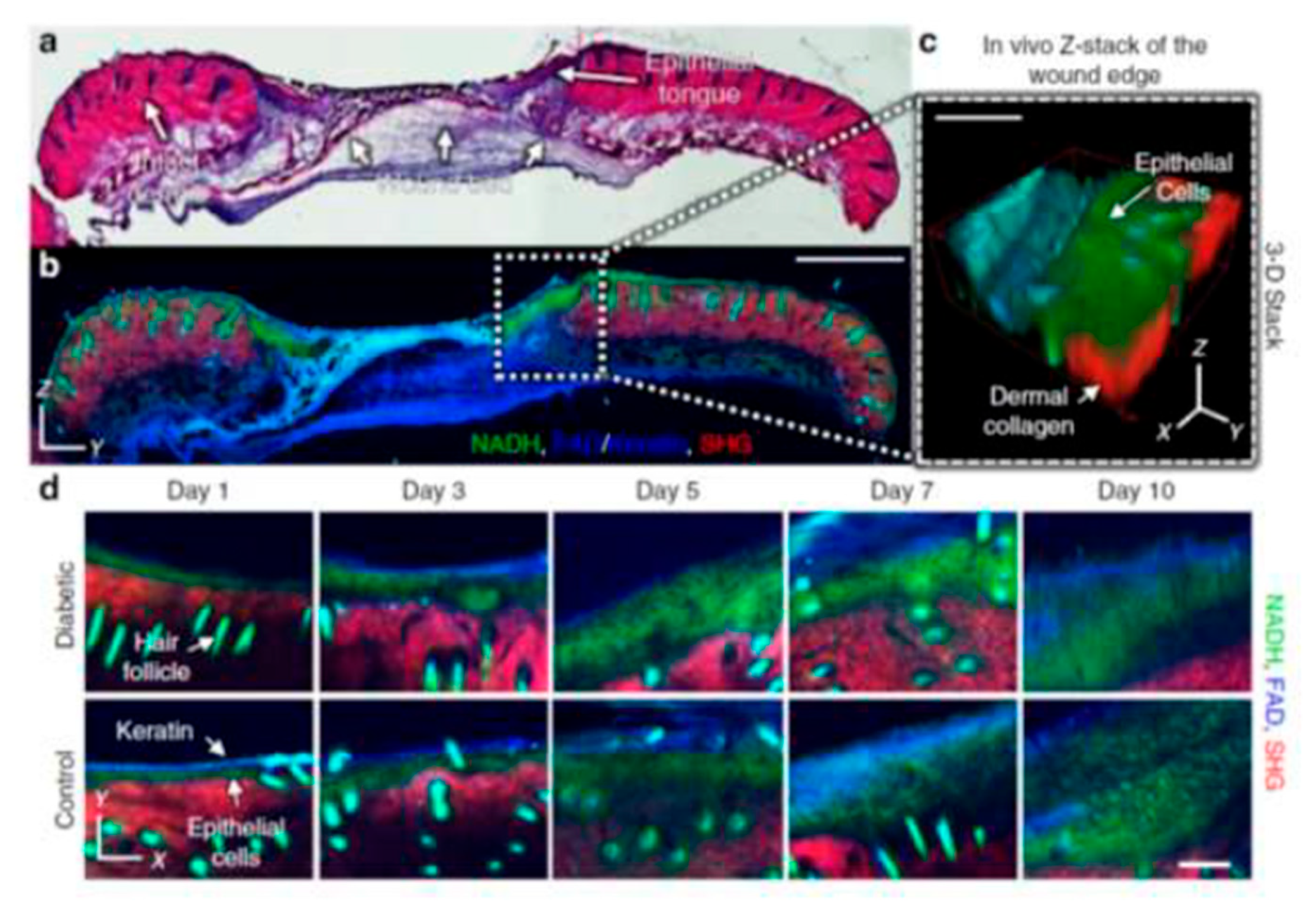
Jake D. Jones, 2018, [15] focused on the redox ratio of FAD/(NADH+FAD) autofluorescence. Using the device, the authors provided in vivo quantitative, longitudinal measurement of cell metabolism, critical in delayed wound healing [16]; the authors were able to isolate the keratinocytes within the edge of the wound from the surrounding chromophores such as haemoglobin and melanin with an optical redox ratio in vivo; thus providing quantitative metrics relevant to different stages of healing or lack of healing.
Summary
In conclusion, MPT is a high-resolution imaging device that can objectively define tissue morphology and the physiological status of the wound. Using the optical redox ratio autofluorescence, a detailed understanding of physiological status can be made, and this can guide treatment in non-healing or hard to heal wounds.
3.2. Physiology
3.2.1. Hyperspectral Imaging
The hyperspectral tissue oxygenation mapping system (HOTM) is a diagnostic tool based on the visible and near-infrared spectral range. Using a camera-like device, spectroscopic information for every pixel is captured and mapped. A single hyperspectral image has two spatial dimensions and one wavelength dimension. In combination, this creates a 3D data cube. In the healing wound, there are differences in the absorption of spectra of oxy- and deoxyhemoglobin and melanin. These are detected by the device and compared to a known reference.
Lalita Khaodhiar et al., 2007, [7] studied its use in 37 patients over a four–six-month period. In this study, the author measured oxyhaemoglobin (H.T. -OXY) and de-oxyhaemoglobin (HT-Deoxy), which determined the H.T. healing index of ulcers. They demonstrated that HT-index could be used to predict wound healing potential. In addition, HOTM accurately differentiates between healthy and unhealthy tissue with a sensitivity of 93% and specificity of 86% compared to clinical findings. The authors identified that the study was limited to type 1 diabetic foot ulcers, and these findings may not be relevant in other types of wounds.
A similar study was conducted by Aksone Nouvond et al., 2009, [17]. Here, the authors performed a prospective single-arm study with 66 patients. Using the exact measurements and healing index, as in Lalita Khaodhiar et al., 2007 [7], they predicted healing with a sensitivity of 80%, specificity of 74%, and a positive predictive value of 90%.
Summary
HOTM is a potentially helpful point of care for chronic wounds. It can accurately predict wound healing by measuring the local microvascular perfusion and, thus, it has a potential for good sensitivity and specificity [17]. Its limiting factor is the high cost secondary to the expensive components within the imaging tool [18]. Optoprim currently supplies HOTM in France to the European market.
3.3. Wound Size and Volume
Geometric measurement of wounds provides baseline measurement, healing rates and differentiates between healing and non-healing wounds. Steed et al. and Sheehan P et al. both indicated that a change in wound size after four weeks is a strong predictor of healing. Failure to reduce the ulcer size after four weeks or more of therapy indicates re-evaluation of management. Therefore, an accurate measurement of wound dimension is crucial for the early recognition of unresponsive wounds [19,20,21]. Various wound measurement techniques range from the simple ruler method, tracings, wound moulding and complicated 3D photography. Here we explore the use of 2D stereophotogrammetry techniques and 3D imaging.
3.3.1. 2D Imaging
2D optical measurements are based on stereophotogrammetry (SPG). The method involves two or more photographs taken at different angles. The photos are then rendered into models and dimensions taken by tracing the margins onscreen. The findings are then automatically compared to a standard reference within the image to estimate the area.
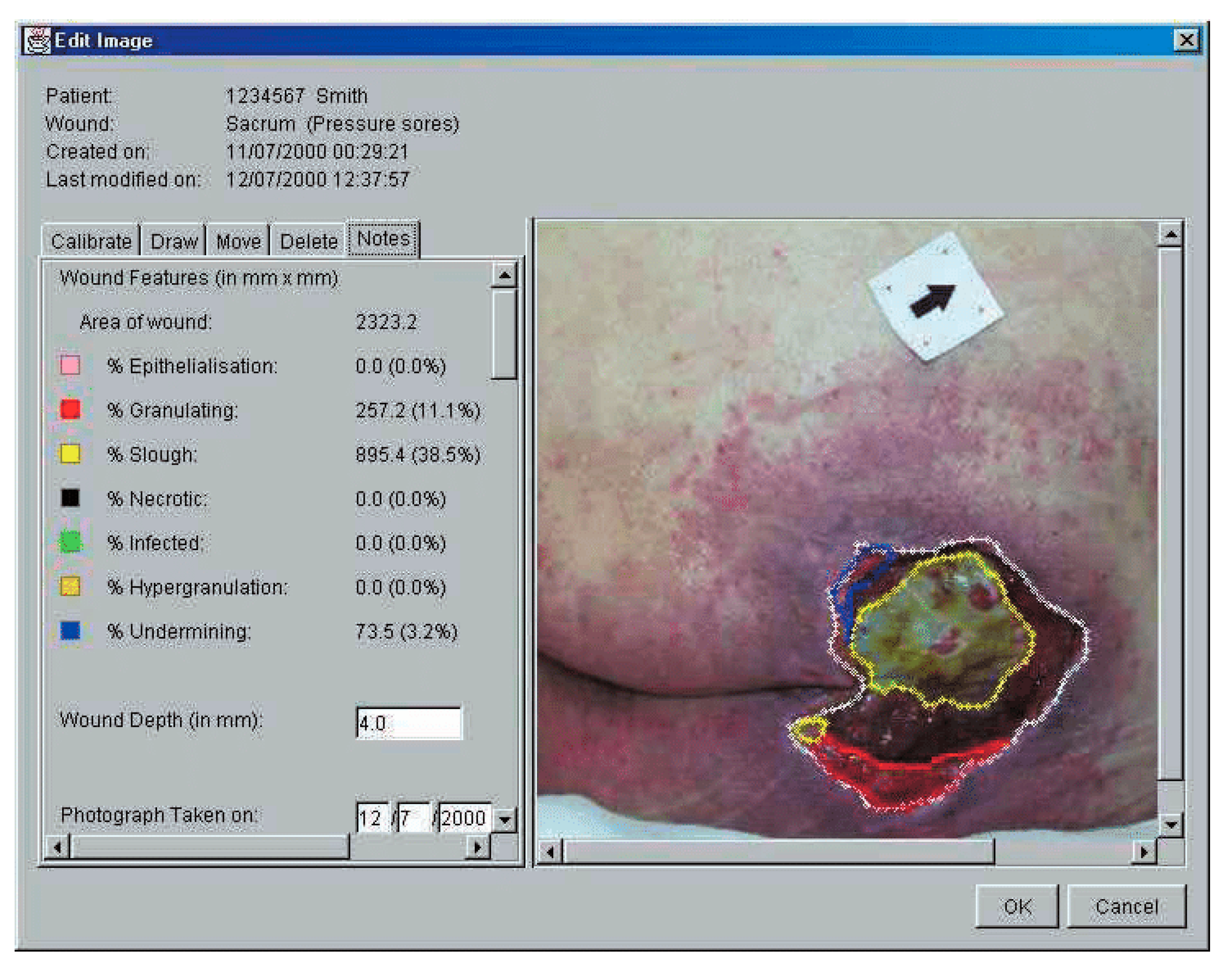
Santamaria et al., 2002 [6] explored the AMWIS post image processing software on 100 wounds of various pathology over multiple sites. They reported high accuracy of 94.9% with a measurement error of 5.1% and with a correlation coefficient r of 69.7. In addition, the authors performed a qualitative study on the user’s experience with AMWIS. They found that the system was accurate, easy to use and had a shallow learning curve. Despite the variation in complex wounds, they felt well informed to make better wound care management choices. Many of the users noted that documentation with the system was intuitive and reliable. The disadvantage was the significantly increased cost when the AMWIS system was adopted.
Stephen Springle et al., 2012, [22] explored the accuracy and reliability of handheld measuring devices (WMD) based on digital imaging with laser guidance. The authors concluded that the devices were accurate at different angles and consistent. The limitation was the effect of uneven ambient light or glare on the skin, which hinders laser detection, resulting in an overestimation of the wound. In addition, the device was found to be heavier than the standard camera, which sometimes made taking pictures cumbersome. Hammons and Nixon et al., 2011, [23] and Miller et al., 2012, [24] both studied a similar instrument (Silhouette Mobile). Both studies found overall reliability to be 0.99 and 0.985, respectively, however, lower reliability was seen in more minor wounds: 0.624.
Foltynski et al., 2013, [25] and ladysynski et al., 2011, [26] looked at the TeleDiaFos system, which is 2D imaging technology specific for wounds of the feet. In both studies, the device was compared with the Silhouette Mobile method and Vistrak digital planetary method. Both studies found the TeleDiafos system to be more accurate and of a higher reliability in comparison, although it was specific to foot wounds.
Digital imaging was compared with other planimetry methods (manual and digital) and was equally reliable. Thawar et al., 2002, [27] demonstrated strong agreement with excellent intra-rater (ICC 0.99) and inter-rater reliability (0.94) of digital imaging in comparison to digital planimetry, and the standard error of measurement was 0.18 for digital imaging. Bhedi et al., 2013, [28] concluded that there was no statistical difference in measurement between digital imaging and digital planetary in smaller wounds < 10 cm; however, digital imaging was more desirable, as it did not directly have contact with the ulcer. Rajbhandari et al., 1999, [29] found that digital imaging was superior with lower interobserver variability of 1.9% than the tracing method’s 26.7% in the measurement of foot ulcers. However, underestimation was seen where the ulcer was over the curved area.
Summary
Wound measurement techniques (2D imaging) are a non-contact method that are easy to use and accurate in measuring wound size and thus wound healing. The main drawback for two-dimensional imaging is the lack of depth measurement weight, producing a significant error in deep or undermined wounds.
3.3.2. 3D Imaging
3D imaging employs a 3D range camera/texture camera, stripe projector and an additional light source. The stripe projector produces a series of light and dark lines onto the wound. Using the lines as a reference, the computer observes the intersection points of the stripes with the wound surface and produces a three-dimensional representation of the observed area. This is known as triangulation [19]. (Figure 5 and Figure 6).
P. plassman et al., 1998, [19] conducted an extensive study with 50 patients comparing 3D imaging vs. manual planetary for wound area measurement and 3d imaging vs. alginate cast for volume measurement. The authors found that 3D imaging reduced standard deviation in wound area measurement from 4% in a large wound (>30 cm) and 20% in a small wound (<0.5 cm) to 3–5% in both when compared to planetary methods. Furthermore, in another study, the system displayed high inter-rater reliability (0.745) and intra-rater reliability (0.868).
Both authors have identified that 3D imaging was unsuitable for undermined, very deep or extensive wounds, as this may under or overestimate the wound.
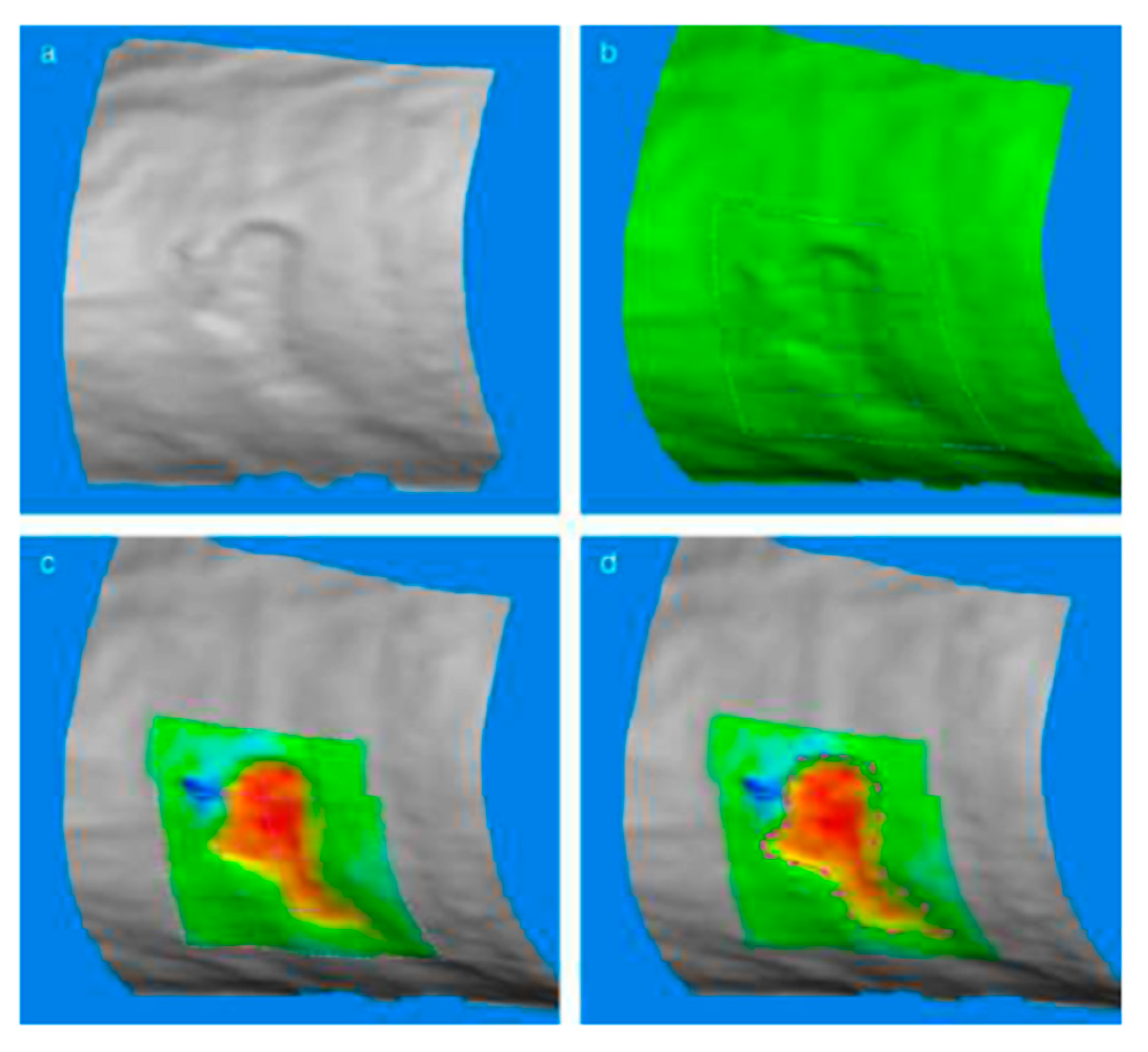
Kecelj-Leskovec et al., 2007, [30] compared laser three-dimensional measuring devices with 15 venous leg ulcers with computer planimetry assessment. Using bland Altman statistical analysis, the authors found that the 3D imaging method had an average of 9.7% area measurement and 7.5% for volume; comparatively, computer planetary assessment had 13.0% area measurement and did not measure volume. These were significantly better than the ruler method and mould method [31]. The discrepancy between the two systems was mainly the ability to appreciate the convexity of the skin.
Andreas Korber et al., 2006, [32] explored 3D imaging as a helpful documentation tool in chronic wounds. All three patients had venous/arterial ulcers and were being treated with vacuum therapy or dressings (acticoat and mepilex); they found that 3D imaging can capture changes in wound size, oedema and level of granulation over time. In addition, 3D imaging was able to detect minor substance defects despite complete epithelisation of the wound.
A. J. Davis et al., 2013, [33] determined the reliability of three-dimensional imaging in 13 chronic wounds over 18 months between multiple observers with varying expertise. They found high interrater reliability for wound measurement (ICC = 0.9867; p < 0.001), and there was no significant difference between non-expert and expert observers. In addition, it could discriminate between improving and static wounds (p < 0.05).
The disadvantages were the inaccurate measurement of wounds more significant than 6 cm and that the system was dependent on a high-quality, readable image obtained from the observer. Moist wounds affected the image quality by representing false peaks and pits during wound reconstruction; thus, 3D imaging required rigorous wound preparation. A further questionnaire describing the observer’s experience found that both expert and non-expert groups indicated that the system would improve their job performance and enhance their effectiveness.
Summary
In conclusion, 3D imaging is an accurate, reliable tool for wound healing. It has higher accuracy and reliability when compared to the moulding method and manual planetary method. As a long-term documentation tool, it identifies small changes that clinicians could easily miss. 3D imaging was limited by the size and shape of the wound.
4. Discussion
An objective evaluation of wounds is necessary to determine the progression of healing which guides treatment strategies. Several instruments have been developed over the years to meet the demands of the increasing burden of wounds. However, there has not been any validation study on the ideal instrument for chronic wounds.
Chronic wounds can be classified into vascular ulcers, diabetic ulcers and pressure ulcers. A common theme shared amongst these included a prolonged, extensive inflammatory phase with or without recurrence of infection and microbial biofilm formation. There is a failure of reparative stimuli for the dermal ecosystem and thus a failure to heal. In addition, there are underlying pathologies that differ depending on the category of chronic wounds. Therefore, by their nature alone, chronic wounds are complex and do not heal similarly to acute wounds [1].
To surmount such a challenge, we employ the use of the medical devices discussed in this article. Two dimensional devices are fast to use, accurate, reliable and entail a variety of two-dimensional-based instruments. The central systems presented were the AMWIS, Silhouette [23] and WMD [34], which measure all wounds, whilst the TeleDiafos was specific to foot wounds. The devices benefit from high accuracy (mean error ranged from 1.90% [22] to 5.1% [6]) and inter/intra correlation reliability (0.9, ICC > 95%) due to the ease of use. There is also a good body of evidence for its use in both acute [6,27,28,35,36] and chronic wounds (Table 2), with over 300 wounds analysed in this study alone. Its crucial disadvantage was the inability to account for undermined wounds and deep wounds, as previously discussed. Whilst there was a good mix of chronic wound types studied, there were no comparators in any of the articles included; hence, most of the studies were focused on the instrument’s reliability.
Comparatively, three-dimensional wound technology is equally accurate and reliable with the addition of depth measurement. It has a relatively low error of measurement (3–5%) in comparison to planetary methods (4–20%) and high interclass correlation (0.98). Inter and Intrarater reliability were also high (0.970, 0.981 respectively). Some 3D techniques include assessing additional wound characteristics such as inflammation using thermal imaging [19,37]. However, the feasibility of the current three-dimensional device is limiting. It is often high in cost and complex to set up. More user-friendly 3D tools have been developed, such as the Next Engine 3D system [38]; however, very little evidence supports its use. Most of the comparisons were against two-dimensional measuring techniques, which are not a fair comparison. Overall, the lack of a comparative gold standard weakens the validity of these studies.
More complex modalities described in this study present a significant advantage of two- or three-dimensional wound assessment, especially in chronic wounds. CLSM and MPM can provide information o with the cellular and subcellular level with very high precision. In addition, it includes information on the physiological properties of the wound through the measurement of the activities of various endogenous fluorophores. This is crucial in understanding the healing potential of chronic wounds. Both CLSM and MPM are fundamentally similar; however, unlike CLSM, MPT is unaffected by the variable pinhole in front of the detector, which determines the thickness of the optical section. In combination with SHG, MPM penetrates further into living tissue and is less damaging than the shorter wavelength photons in CLSM. Both MPM and CLSM suffer from resolution decay with increasing depth and are limited to several hundred micrometres.
OCT has better penetration depth but at the cost of lower resolution; nevertheless, it shows good potential as a tool for monitoring wound healing by direct visualisation through the stages of epithelisation, considering the epithelial tissue and scar formation. However, more studies are required for validation. Recent advances in OCT involve using polarised light to provide high-resolution images of the skin structure, collagen birefringence and blood flow, improving its image quality and functionality [39].
The Hyperspectral method was the most promising, as it provides information on the wound’s morphology and physiology, including an assessment of the microvascular oxygenation status of the wound, which is predictive of ulcer healing. In addition, the Hyperspectral method was easy to use, similar to a digital camera and with further development to employ inexpensive LED illumination instead of the LCTF; it could be an affordable tool [18]. The combination of portability and low-cost hyperspectral imaging could be helpful as an accurate, reliable point of care wound assessment tool.
While these techniques were more advanced, unfortunately, the lack of articles, little wounds and comparators make it difficult to suggest one instrument. Therefore, further validation studies with comparative clinical studies are required.
Based on the available evidence, the recommendation of this article is to adopt 2D imaging into clinical practice and to perform further validation studies. This would include a quantitative study on the cost and comparison of 2D instruments provided by each company, such as Silhouette mobile [23], Eykona Wound [40] or Mavis [19], and a qualitative study on the personal experience of health care professionals using the instrument on chronic wounds. The combination of these studies would improve on the evidence available, further supporting its effectiveness in clinical care.
Methodological qualities in the reviewed studies varied. With inter/intra rater satistics, the number of clinicians or the time interval between measurements was not always reported. The reported data were heterogeneous. Each study had a different statistical approach and did not present sufficient raw data. Therefore, a pooled analysis to determine the overall accuracy or reliability was not possible. Outcome measures between the categories differed. The two- and three-dimensional methods measured changes in size or volume whilst the anatomy/physiological-based instruments analysed morphological or physiological changes and, in some articles, H.T. healing index [7,17]. As there was no gold standard or reference for validation, comparison between modalities was difficult.
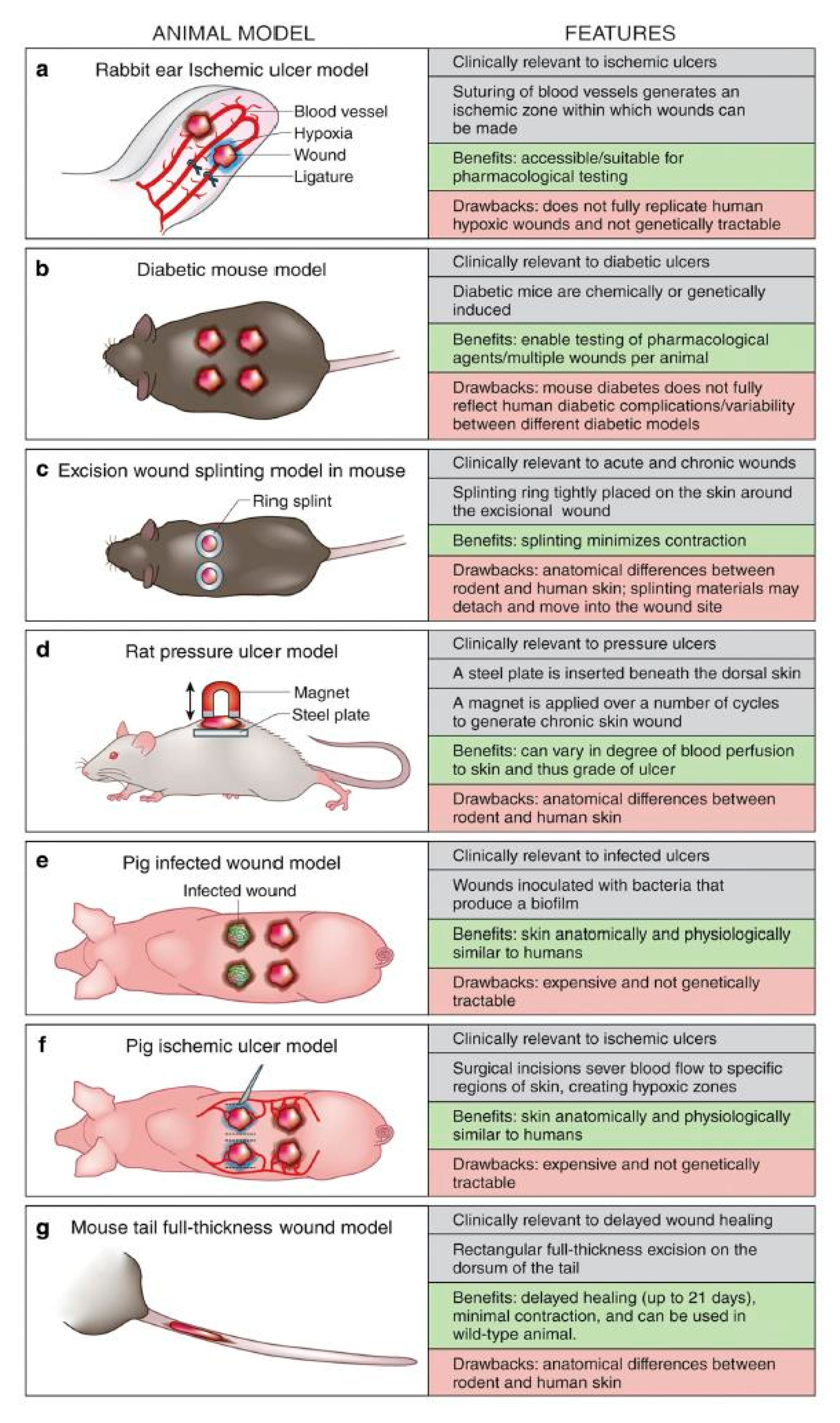
The inclusion or exclusion of animal studies is often debated. There are anatomical and physiological differences within the animal and human species, making reproducibility and translation to clinical reality a challenge (Figure 7) [41]. Wound healing in mice is different in that it is affected by hair cycles and dominated by myofibroblast-mediated contraction. To counter this, some researchers utilised an outbred hairless mouse and actively splinted the mouse skin to minimise contraction, thus allowing healing through granulation and re-epithelisation [42]. There are considerable differences in skin anatomy in pigs—high P.H., fatty sub cutus, predominant apocrine sweat gland and richer vasculature than in the human dermis [42]. These differences could have relevant implications for physiological studies. Despite this, wounds in all animals undergo the same stages of healing. The validity of the instruments explored here is fundamentally based on the accuracy of measuring progress through the stages rather than wound response. Furthermore, consistency of findings and interrater correlation was our focus and these unaffected by the physiological differences between animals and humans. Therefore, we can assume that animal models can be included in this study [25,26,31,42,43,44].
5. Conclusions
We have presented 11 devices measuring the biophysical parameters of chronic wounds. These devices demonstrated objectivity, reliability and accuracy and were all fast and noninvasive. From the available evidence, the most superior wound measuring device was two-dimensional. However, hyperspectral imaging had strong potential but required further development in its technology and future clinic validation studies.
Author Contributions
Conceptualization, N.M. and P.T.; methodology, P.T.; software, P.T.; validation, N.M. and P.T. and J.L.; formal analysis, P.T.; data curation, P.T. and J.L.; writing—original draft preparation, P.T.; writing—review and editing, N.M. and P.T.; supervision, N.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Frykberg, R.G.; Banks, J. Challenges in the Treatment of Chronic Wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guest, J.F.; Fuller, G.W.; Vowden, P. Cohort study evaluating the burden of wounds to the UK’s National Health Service in 2017/2018: Update from 2012/2013. BMJ Open 2020, 10, e045253. [Google Scholar] [CrossRef] [PubMed]
- Kingston, A.; Robinson, L.; Booth, H.; Knapp, M.; Jagger, C.; MODEM Project. Projections of multi-morbidity in the older population in England to 2035: Estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing 2018, 47, 374–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ud-Din, S.; Bayat, A. Non-invasive objective devices for monitoring the inflammatory, proliferative and remodelling phases of cutaneous wound healing and skin scarring. Exp. Dermatol. 2016, 25, 579–585. [Google Scholar] [CrossRef] [Green Version]
- Pillen, H.; Miller, M.; Thomas, J.; Puckridge, P.; Sandison, S.; Spark, J. Assessment of Wound Healing: Validity, Reliability and Sensitivity of Available Instruments. Wound Pract. Res. J. Aust. Wound Manag. Assoc. 2009, 17, 208–217. [Google Scholar]
- Santamaria, N.; Austin, D.; Clayton, L. A Multi-site Clinical Evaluation Trial of the Alfred/Medseed Wound Imaging System Prototype. Prim. Intent. Aust. J. Wound Manag. 2002, 10, 120–125. [Google Scholar]
- Khaodhiar, L.; Dinh, T.; Schomacker, K.T.; Panasyuk, S.V.; Freeman, J.E.; Lew, R.; Vo, T.; Panasyuk, A.A.; Lima, C.; Giurini, J.M.; et al. The Use of Medical Hyperspectral Technology to Evaluate Microcirculatory Changes in Diabetic Foot Ulcers and to Predict Clinical Outcomes. Diabetes Care 2007, 30, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Kuck, M.; Strese, H.; Alawi, M.S.A.; Meinke, M.C.; Fluhr, J.W.; Burbach, G.J.; Krah, M.; Sterry, W.; Lademann, J. Evaluation of optical coherence tomography as a non-invasive diagnostic tool in cutaneous wound healing. Ski. Res. Technol. 2014, 20, 1–7. [Google Scholar] [CrossRef]
- Cobb, M.J.; Chen, Y.; Underwood, R.A.; Usui, M.L.; Olerud, J.; Li, X. Noninvasive assessment of cutaneous wound healing using ultrahigh-resolution optical coherence tomography. J. Biomed. Opt. 2006, 11, 064002. [Google Scholar] [CrossRef]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.; Brezinski, M.E. Optical Coherence Tomography: An Emerging Technology for Biomedical Imaging and Optical Biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Lange-Asschenfeldt, S.; Bob, A.; Terhorst, D.; Ulrich, M.; Fluhr, J.W.; Mendez, G.; Roewert-Huber, H.-J.; Stockfleth, E.; Lange-Asschenfeldt, B. Applicability of confocal laser scanning microscopy for evaluation and monitoring of cutaneous wound healing. J. Biomed. Opt. 2012, 17, 076016. [Google Scholar] [CrossRef]
- Deka, G.; Wu, W.-W.; Kao, F.-J. In vivowound healing diagnosis with second harmonic and fluorescence lifetime imaging. J. Biomed. Opt. 2012, 18, 061222. [Google Scholar] [CrossRef] [Green Version]
- Riemann, I.; Ehlers, A.; LeHarzic, R.; Martin, S.; Reif, A.; König, K. In vivo multiphoton tomography of skin during wound healing and scar formation. Multiphot. Microsc. Biomed. Sci. VII 2007, 6442, 644226. [Google Scholar] [CrossRef]
- König, K.; Weinigel, M.; Bückle, R.; Kaatz, M.; Hipler, C.; Zens, K.; Schneider, S.W.; Huck, V. Monitoring wound healing by multiphoton tomography/endoscopy. Photonic Ther. Diagn. XI 2015, 9303, 93030F. [Google Scholar] [CrossRef]
- Jones, J.; Ramser, H.E.; Woessner, A.E.; Quinn, K.P. In vivo multiphoton microscopy detects longitudinal metabolic changes associated with delayed skin wound healing. Commun. Biol. 2018, 1, 198. [Google Scholar] [CrossRef]
- Springer, S.; Zieger, M.; Böttcher, A.; Lademann, J.; Kaatz, M. Examination of wound healing after curettage by multiphoton tomography of human skin in vivo. Ski. Res. Technol. 2017, 23, 452–458. [Google Scholar] [CrossRef]
- Nouvong, A.; Hoogwerf, B.; Mohler, E.; Davis, B.; Tajaddini, A.; Medenilla, E. Evaluation of Diabetic Foot Ulcer Healing With Hyperspectral Imaging of Oxyhemoglobin and Deoxyhemoglobin. Diabetes Care 2009, 32, 2056–2061. [Google Scholar] [CrossRef] [Green Version]
- Zhou, A.H. A Survey of Optical Imaging Techniques for Assessing Wound Healing. Int. J. Intell. Control Syst. 2012, 17, 79–85. [Google Scholar]
- Plassmann, P.; Jones, T. MAVIS: A non-invasive instrument to measure area and volume of wounds. Med. Eng. Phys. 1998, 20, 332–338. [Google Scholar] [CrossRef]
- Sheehan, P.; Jones, P.; Caselli, A.; Giurini, J.M.; Veves, A. Percent Change in Wound Area of Diabetic Foot Ulcers Over a 4-Week Period Is a Robust Predictor of Complete Healing in a 12-Week Prospective Trial. Diabetes Care 2003, 26, 1879–1882. [Google Scholar] [CrossRef] [Green Version]
- Steed, D.L.; Attinger, C.; Colaizzi, T.; Rn, M.C.; Franz, M.; Harkless, L.; Bs, A.J.; Moosa, H.; Robson, M.; Serena, T.; et al. Guidelines for the treatment of diabetic ulcers. Wound Repair Regen. 2006, 14, 680–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprigle, S.; Nemeth, M.; Gajjala, A. Iterative design and testing of a hand-held, non-contact wound measurement device. J. Tissue Viability 2012, 21, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Hammond, C.E.; Nixon, M.A. The Reliability of a Handheld Wound Measurement and Documentation Device in Clinical Practice. J. Wound Ostomy Cont. Nurs. 2011, 38, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Karimi, L.; Donohue, L.; Kapp, S. Interrater and Intrarater Reliability of Silhouette Wound Imaging Device. Adv. Ski. Wound Care 2012, 25, 513–518. [Google Scholar] [CrossRef]
- Foltynski, P.; Ladyzynski, P.; Sabalinska, S.; Wojcicki, J.M. Accuracy and Precision of Selected Wound Area Measurement Methods in Diabetic Foot Ulceration. Diabetes Technol. Ther. 2013, 15, 711–720. [Google Scholar] [CrossRef]
- Ladyzynski, P.; Foltynski, P.; Molik, M.; Tarwacka, J.; Migalska-Musial, K.; Mlynarczuk, M.; Wojcicki, J.M.; Krzymien, J.; Karnafel, W. Area of the Diabetic Ulcers Estimated Applying a Foot Scanner–Based Home Telecare System and Three Reference Methods. Diabetes Technol. Ther. 2011, 13, 1101–1107. [Google Scholar] [CrossRef]
- AThawer, H.; EHoughton, P.; Woodbury, M.G.; Keast, D.; Campbell, K. A comparison of computer-assisted and manual wound size measurement. Ostomy Wound Manag. 2002, 48, 46–53. [Google Scholar]
- Bhedi, A.; Saxena, A.K.; Gadani, R.; Patel, R. Digital Photography and Transparency-Based Methods for Measuring Wound Surface Area. Indian J. Surg. 2013, 75, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Rajbhandari, S.M.; Harris, N.D.; Sutton, M.; Lockett, C.; Eaton, S.; Gadour, M.; Tesfaye, S.; Ward, J.D. Digital imaging: An accurate and easy method of measuring foot ulcers. Diabet. Med. 1999, 16, 339–342. [Google Scholar] [CrossRef]
- Kecelj-Leskovec, N.; Jezeršek, M.; Možina, J.; Pavlović, M.D.; Lunder, T. Measurement of venous leg ulcers with a laser-based three-dimensional method: Comparison to computer planimetry with photography. Wound Repair Regen. 2007, 15, 767–771. [Google Scholar] [CrossRef]
- Gardner, S.E.; Frantz, R.A.; Hillis, S.; Blodgett, T.J.; Femino, L.M.; Lehman, S.M. Volume Measures Using a Digital Image Analysis System are Reliable in Diabetic Foot Ulcers. Wounds Compend. Clin. Res. Pract. 2012, 24, 146–151. [Google Scholar]
- Körber, A.; Rietkötter, J.; Grabbe, S.; Dissemond, J. Three-dimensional documentation of wound healing: First results of a new objective method for measurement. J. Der Dtsch. Dermatol. Ges. 2006, 4, 848–854. [Google Scholar] [CrossRef]
- Davis, A.; Nishimura, J.; Seton, J.; Goodman, B.; Ho, C.; Bogie, K. Repeatability and clinical utility in stereophotogrammetric measurements of wounds. J. Wound Care 2013, 22, 90–97. [Google Scholar] [CrossRef]
- Nemeth, M.; Sprigle, S.; Gajjala, A. Clinical usability of a wound measurement device. J. Spinal Cord Med. 2010. Available online: http://hdl.handle.net/1853/43276 (accessed on 19 November 2020).
- Chang, A.C.; Dearman, B.; Greenwood, J.E. A Comparison of Wound Area Measurement Techniques: Visitrak Versus Photography. Eplasty 2011, 11, e18. [Google Scholar]
- Haghpanah, S.; Bogie, K.; Wang, X.; Banks, P.G.; Ho, C.H. Reliability of Electronic Versus Manual Wound Measurement Techniques. Arch. Phys. Med. Rehabil. 2006, 87, 1396–1402. [Google Scholar] [CrossRef]
- Sirazitdinova, E.; Deserno, T.M. System design for 3D wound imaging using low-cost mobile devices. Burns 2017, 1, 761–769. [Google Scholar]
- Zvietcovich, F.; Castaneda, B.; Valencia, B.; Llanos-Cuentas, A. A 3D assessment tool for accurate volume measurement for monitoring the evolution of cutaneous Leishmaniasis wounds. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar]
- Pierce, M.C.; Strasswimmer, J.; Park, B.H.; Cense, B.; de Boer, J. Advances in Optical Coherence Tomography Imaging for Dermatology. J. Investig. Dermatol. 2004, 123, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Bowling, F.L.; King, L.; Fadavi, H.; Paterson, J.A.; Preece, K.; Daniel, R.W.; Matthews, D.J.; Boulton, A.J.M. An assessment of the accuracy and usability of a novel optical wound measurement system. Diabet. Med. 2009, 26, 93–96. [Google Scholar] [CrossRef]
- Grada, A.; Mervis, J.; Falanga, V. Research Techniques Made Simple: Animal Models of Wound Healing. J. Investig. Dermatol. 2018, 138, 2095–2105.e1. [Google Scholar] [CrossRef] [Green Version]
- Galiano, R.D.; Michaels, V.J.; Dobryansky, M.; Levine, J.P.; Gurtner, G.C. Quantitative and reproducible murine model of excisional wound healing. Wound Repair Regen. 2004, 12, 485–492. [Google Scholar] [CrossRef]
- Jørgensen, L.B.; ASørensen, J.; Jemec, G.B.; Yderstraede, K.B. Methods to assess area and volume of wounds—A systematic review. Int. Wound J. 2015, 13, 540–553. [Google Scholar] [CrossRef] [PubMed]
- Adão, T.; Hruška, J.; Pádua, L.; Bessa, J.; Peres, E.; Morais, R.; Sousa, J.J. Hyperspectral imaging: A review on UAV-based sensors, data processing and applications for agriculture and forestry. Remote Sens. 2017, 9, 1110. [Google Scholar] [CrossRef] [Green Version]
- Nunan, R.; Harding, K.G.; Martin, P. Clinical challenges of chronic wounds: Searching for an optimal animal model to recapitulate their complexity. Dis. Model Mech. 2014, 7, 1205–1213. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Prisma Table.

Figure 2.
OCT images and corresponding histology. Image taken at 3 days (a,b), 7 days (c–f), 12 days (g,h) Michael J. Cobb et al., 2006. [9].
Figure 2.
OCT images and corresponding histology. Image taken at 3 days (a,b), 7 days (c–f), 12 days (g,h) Michael J. Cobb et al., 2006. [9].

Figure 3.
Comparison of in vivo MPM imaging with histological section; (a) hematoxylin and eosin-stained tissue sections identify dermis, epithelial tongue and granulation tissue at five days post wound. (b) These same regions are visible through MPM imaging of an adjacent unstained section, which highlights NADH (green), FAD and keratin (blue) and collagen SHG (red). (c) Similar patterns of autofluorescence were detectable in the skin during in vivo acquisition of MPM z-stacks at the wound edge (scale bar = 200 µm). (d) Depth-resolved optical sections taken 125 µm deep into the wound edge demonstrate an ability to monitor the wound edge at all in vivo time points (scale bar = 100 µm) Jake D. Jones et al., 2018. [15].
Figure 3.
Comparison of in vivo MPM imaging with histological section; (a) hematoxylin and eosin-stained tissue sections identify dermis, epithelial tongue and granulation tissue at five days post wound. (b) These same regions are visible through MPM imaging of an adjacent unstained section, which highlights NADH (green), FAD and keratin (blue) and collagen SHG (red). (c) Similar patterns of autofluorescence were detectable in the skin during in vivo acquisition of MPM z-stacks at the wound edge (scale bar = 200 µm). (d) Depth-resolved optical sections taken 125 µm deep into the wound edge demonstrate an ability to monitor the wound edge at all in vivo time points (scale bar = 100 µm) Jake D. Jones et al., 2018. [15].

Figure 4.
Morphological changes in acute wound healing; area of acute wound with crust and signs of inflammation (A); wound after curettage (B); reduced collagen matrix on visit (C); tight plexiform connective tissue densely packed collagen fiber bundles found in nearly regular arrangement in different orientations (D); minimal local connective tissue cells, connective tissue cells and basic substance, Reprinted with permission from ref. [16]. Springer, S. et al., 2017.
Figure 4.
Morphological changes in acute wound healing; area of acute wound with crust and signs of inflammation (A); wound after curettage (B); reduced collagen matrix on visit (C); tight plexiform connective tissue densely packed collagen fiber bundles found in nearly regular arrangement in different orientations (D); minimal local connective tissue cells, connective tissue cells and basic substance, Reprinted with permission from ref. [16]. Springer, S. et al., 2017.

Figure 5.
3D measurement of leg ulcer; (a) three-dimensionally measured surface; (b) approximation of the NURBS surface over the ulcer region; (c) visualization of ulcer depth variation using a rainbow color palette; (d) selection of the ulcer boundary. Reprinted with permission from ref. [30], Nada Kecelj-Leskovec et al., 2007.
Figure 5.
3D measurement of leg ulcer; (a) three-dimensionally measured surface; (b) approximation of the NURBS surface over the ulcer region; (c) visualization of ulcer depth variation using a rainbow color palette; (d) selection of the ulcer boundary. Reprinted with permission from ref. [30], Nada Kecelj-Leskovec et al., 2007.

Figure 6.
AMWIS 3D imaging Calibrated wound image, demarcated wound areas and the associated measurements expressed in mm and as percentages of the total wound surface area. Santamaria N. et al., 2002. [6].
Figure 6.
AMWIS 3D imaging Calibrated wound image, demarcated wound areas and the associated measurements expressed in mm and as percentages of the total wound surface area. Santamaria N. et al., 2002. [6].

Figure 7.
Animal models of wound healing clinical relevance, advantage and disadvantage. (a) Rabbit ear model. (b) Chemically induced type 2 diabetic mouse model. (c) Excision wound splinting model in mouse (dorsal view). (d) Rat magnet ischemiareperfusion model (profile view). (e) Pig wound infection model (dorsal view). (f) Pig flap ischemia model (dorsal view). This method is also applicable to rodents and rabbits. (g) Mouse tail fullthickness wound model (dorsal view). Nunan et al., 2014. [45].
Figure 7.
Animal models of wound healing clinical relevance, advantage and disadvantage. (a) Rabbit ear model. (b) Chemically induced type 2 diabetic mouse model. (c) Excision wound splinting model in mouse (dorsal view). (d) Rat magnet ischemiareperfusion model (profile view). (e) Pig wound infection model (dorsal view). (f) Pig flap ischemia model (dorsal view). This method is also applicable to rodents and rabbits. (g) Mouse tail fullthickness wound model (dorsal view). Nunan et al., 2014. [45].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
QUADAS Score.
| Anatomical | No. Study | Average | Range |
|---|---|---|---|
| Optical coherence tomography | 1 | 13 | 13 |
| Confocal microscopy | 1 | 13 | 13 |
| Multiphoton tomography | 2 | 12 | 12 |
| Physiological | |||
| Hyperspectral imaging | 2 | 14 | 14 |
| Wound size and volume | |||
| 3D imaging | 6 | 11 | 9–13 |
| 2D imaging | 9 | 14 | 10–14 |
Table 2.
Morphological, physiological and wound size and volume measuring techniques.
| Paper | First Author | Year | Animal/Human | Patient NO | Wound Type | Statistical Method | Comparator | Outcome | Feasibility and Resolution | Companies |
|---|---|---|---|---|---|---|---|---|---|---|
| Optical coherence tomography | ||||||||||
| Evaluation of optical coherence tomography as a noninvasive diagnostic tool in Cutaneous wound healing. | Kuck, Monika | 2014 | human | 6 | Chronic wound | nil | histology | Visualisation of skin layers at each stage of healing | Lateral: 8 µm Axial: 5 µm Scan depth: 1–2 mm | Optovue, NinePoint Medical, and Thorlabs expensive |
| Multiphoton tomography | ||||||||||
| Monitoring Wound Healing by Multiphoton Tomography/Endoscopy | karsten konig | 2016 | human | 20 | Acutre and chronic | nil | nill | Detects tissue morphology and physiology changes during healing | Horizontal: 1 µm Vertical: 2 µm Scan depth: 200 µm 750 nm wavelength | Dermatinspectmost expensive |
| Invivo multiphoton micrsotoopy detects logitudinal metabolic changes associated with | jake D.jones | 2018 | animal | 37 | chronic and acute wound | ANOVA | normal wound | |||
| Confocal microscopy | ||||||||||
| Applicability of confocal laser scanning microscopy for evaluation and monitoring of cutaneous wound healing | susanne lange asschenfeldt | 2015 | human | 15 | acute woundchronic wounds | nil | nil | Detects tissue morphology and physiology changes during healing | Horizontal: 1.25 µm Vertical: 5.0 µm Scan depth: 200 µm | Vivascope less expensive |
| Hyperspectral imaging | ||||||||||
| Evaluation of Diabetic Foot Ulcer Healing With Hyperspectral Imaging of Oxyhemoglobin and Deoxyhemoglobin | Aksone Nouvong | 2009 | human | 72 | Foot ulcer | CHI square, T test | nil | H.T. index: sensitivity 80%, Specificity 74% positive predictive:90% | Lateral: 0.4–1.0 µm | Hyspex, Specim Cheapest |
| The Use of Medical Hyperspectral Technology to Evaluate Microcirculatory Changes in Diabetic Foot Ulcers and to Predict Clinical Outcomes. | Lalita Khaodhiar | 2007 | human | 21 | foot ulcer | ANOVA | nil | H.T. index: sensitivity 93%, Specificity 86% positive/negative predictive:93%/ 68% | ||
| 3D imaging | ||||||||||
| Three-dimensional documentation of wound healing: First results of a new objective method for measurement | Andreas Korber | 2006 | human | 3 | venous/arterial ulcer | non | non | Precise 3d rendition of the wound | 2–5 s | |
| MAVIS: a noninvasive instrument to measure area and volume of wounds | P.plassman | 1998 | human | 50 | variety | Pearson correlation coefficient standard deviation in % | manual planimetryalginate casts | STD deviation: Planetary: 4% (large wounds)-20% small wound mavis: 3–5% Wound volume Alginate: 5–40% Mavis: 5% smaller on average | non invasive fast and accurate | |
| Assessment of chronic wounds by three-dimensional optical imaging based on integrating geometrical, chromatic, and thermal data | Barone | 2011 | human | 7 | leg ulcers | Percentage difference to clinical assessment | Clinical assessment | Measurement of a known volume: 4–7% different on colour images, 5%–12% on thermal images | Lateral resolution: 0.2 mm Area 200 mm × 150 mm 3D scanner expensive | |
| Measurement of venous leg ulcers with a laser-based three-dimensional method comparison to computer planimetry with photography. | Kcelj leskovec | 2007 | human | 15 | venous ulcer | Bland altman analysis | computer planetary | Precision of 3d imaging Volume:7.5% Perimeter: 5.8% Area: 9.7% | area 100 × 100 × 100 mm | |
| Repeatability and clinical utility in stereophotogrammetric measurements of wounds | A.J.Davis | 2013 | human | 13 | chronic wound | Inter class correlation coefficient ANOVA | clinical assessment | Interclass correlation: 0.9867 | wound <6 cm | |
| Volume Measures Using a Digital Image Analysis System are Reliable in Diabetic Foot Ulcers | Gardner | 2012 | human | 34 | foot ulcer | inter rater and intrarater reliability | nil | inter rater reliability 0.970 intra rater reliability 0.981 | easy to use | |
| 2D Imaging | ||||||||||
 | santamaria | 2002 | human | 100 | multiple | measurement error pearson correlation coefficient | nil | measurement error:5.1% ICC: 69.7 (p < 0.01) | easy to use, more effective costly | |
| A comparison of computer-assisted and manual wound size measure-ment. | thawar et al. | 2002 | human | 83 | chronic wound + acute | interclass cofficient: ANOVA Standard error of measurement | nil | Planetary: ICC 0.99, SEM 0.18 Digital imaging: ICC 0.94, SEM 0.94 | digital imaging was costly | |
| Digital photography and transparency-based methods for measuring wound surface area. | Bhedi | 2013 | human | 40 | various wounds | mean values and standard deviation | nil | no significant difference between manual planimerty and digital imaging | n/a | |
| Digital imaging: an accurate and easy method of measuring foot ulcers | S.M.Rajbhandari | 2001 | human | 30 | foot ulcer | Reliability coefficicnet of variation | nil | CV: 16% for digital imaging. CV:27% for graph method | digital imaging was faster and easier. | |
| Iterative design and testing of a handheld, non-contact wound measurement device. | springle | 2011 | human | 19 | preassure ulcer | Mean arror intrer and inter class coefficient | nil | Mean errors for WMD were 1.90% at 0 degrees, 1° 76% at 5° and 4⋅28% at 10 degrees Intra-rater ICC for WMD > 0.975. Inter-rater ICC was 0.966 | WMD, low cost | |
| The reliability of a handheld wound measurement and documentation device in clinical practice. | Hammond and Nixon | 2011 | human | 5 | chronic wound | inter and intra-rater variation | nil | intra-rater: 97.4% inter-rater: 96.8% ICC: 99⋅76%. | n/a | |
| interrater and Intrarater reliability of silhouette wound imaging device. | miller | 2012 | human | 14 | Mix wounds | inter and intra-rater variation | nil | Inter rater: 0.985 (large), 0.624 (small) Intra rater: no difference | n/a | |
| Accuracy and Precision of Selected Wound Area Measurement Methods in Diabetic Foot Ulceration | Foltynski | 2013 | human | 16 | diabetic wounds | Relative error cofficient of variation | nil | RE: Vistrak 6.3, TeleDiafos 2.1, Silhouette 2.3 CV: Vistrak 6.3, TeleDiafos 1.6, Silhouette 3.1 | System limited to foot wounds | |
| Area of the diabetic ulcers estimated applying a foot scanner-based home telecare system and three reference methods. | Ladyzynski | 2011 | human | 36 | diabetic wounds | linear regression, Bland althman analysis | nil | ICC: TeleDiafos vs. Vistrak:0.985 TeleDiafos vs. Silhoutte: 0.987 | System limited to foot wounds |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tan, P.; Lim, J.; Moiemen, N. Imaging Techniques Used for Wound Healing Assessment: A Systematic Review Part 1 Chronic Wounds. Eur. Burn J. 2021, 2, 194-214. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040015
AMA Style
Tan P, Lim J, Moiemen N. Imaging Techniques Used for Wound Healing Assessment: A Systematic Review Part 1 Chronic Wounds. European Burn Journal. 2021; 2(4):194-214. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040015
Chicago/Turabian StyleTan, Poh, Joanne Lim, and Naiem Moiemen. 2021. "Imaging Techniques Used for Wound Healing Assessment: A Systematic Review Part 1 Chronic Wounds" European Burn Journal 2, no. 4: 194-214. https://0-doi-org.brum.beds.ac.uk/10.3390/ebj2040015