
Dental Patients’ Perspective on COVID-19: A Systematic Review



Department of Medical and Surgery Specialties, Dental School, University of Brescia, Radiological Sciences and Public Health, 25123 Brescia, Italy
*
Author to whom correspondence should be addressed.
Encyclopedia 2022, 2(1), 365-382; https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010022
Submission received: 17 January 2022
/
Accepted: 26 January 2022
/
Published: 1 February 2022
(This article belongs to the Collection Encyclopedia of COVID-19)
Definition
:The COVID-19 epidemic has changed patients’ approach to dental treatments. While dentists worldwide have shown an excellent level of adaptability to face the new challenges presented by the unprecedented situation due to the rapid spread of COVID-19, dental patients have witnessed a sudden suspension of elective treatments and a slow resumption of dental care activities after several national lockdowns. In addition, the general climate of anxiety and fear due to the high COVID-19 risk and the high level of mortality has influenced the perception and attitudes of people towards dental activity, inducing many dental patients to avoid appointments to the dentist if not highly urgent. We present an overview of the current state of knowledge about dental patients’ perception, perspective, attitude, and expectations towards a full resumption of regular dental treatments.
1. Introduction
Since the beginning of the COVID-19 pandemic, dental professionals have been exposed to a high level of anxiety and stress due to several changes that have affected dentistry in many ways. To date, many international and national guidelines and recommendations are available to support dentists in their everyday dental activities [1,2]. In addition, many studies have investigated dentists’ perceptions, problems, attitudes, and expectations worldwide to understand how dentists have faced the unprecedented situation due to the COVID-19 outbreak [3,4,5].
The management of the emergencies and urgencies in public and private dental clinics during the various national lockdown, the handling of COVID-19 patients in need of urgent dental treatments, the optimization of the personal protective equipment (PPE), and the appropriate approach to resume the regular dental activity with a high level of safety for dental staff and patients have been deeply analyzed [6,7,8,9,10].
In the first COVID-19 outbreak period, many countries adopted prudential measures to reduce the risk of contagion, such as suspending elective dental treatments and recommending executing only non-postponable dental treatments. However, after the first waves of COVID-19, the need to restart private and public dental activities has become the first and foremost goal of many dental professionals [11].
2. Synthesis
From the end of 2020, the availability of COVID-19 vaccines has supported a complete restart of dental activity, allowing the medical staff to resume their work with a certain level of safety and confidence [12,13].
Therefore, if, on the one hand, COVID-19 has created an unprecedented situation for all health services, on the other hand, this is also an unknown situation for patients, who have to handle fear of COVID-19 contagion and discomfort situations due to the suspension of planned dental treatments [14,15].
In this context, the psychological consequence of COVID-19 should not be neglected [16]. As emerged in a recent Chinese study, people living in a pandemic can suffer from different levels of psychological distress, experiencing increased fear of becoming infected [17]. In dentistry, this higher level of stress and anxiety can be translated into a series of ugly behaviors, such as avoidance of dental appointments, treatment delays, and adoption of therapies based on their experience and common sense without the support of their dentists [18].
This work aimed to review the current literature about the role of COVID-19 in the perceptions, perspectives, attitudes, and expectations of patients toward dental treatments and the risk of COVID-19 infection within dental clinics.
2.1. Methods
A systematic review of the current literature was performed following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [19]. On the basis of the inclusion criteria, we selected original studies reporting dental patients’ perceptions or perspectives during the COVID-19 pandemic and their attitudes and expectations about the safe restart of dental clinics and dental offices activities.
PubMed and Web of Science databases were searched using the following search terms: (COVID-19 [Title/Abstract]) AND (dental patient [Title/Abstract]) AND (perspective or perception [Title/Abstract]).
The search strategy was carried out from September to October 2021, without time and language restriction. First, the resultant citations were screened by title, followed by abstracts and then full texts. In addition to the initial search, references in the selected sources were checked manually, and further studies were included if relevant.
Additionally, hand searches were performed to identify possible articles other than those found in the electronic databases. Two reviewers (MLG and EA) performed the first (title/abstract screening) and second (full-text assessment) steps of the search process. Any disagreement was discussed and then solved by consensus.
All original peer-reviewed research publications were considered. Inclusion criteria for eligible studies were: (1) studies carried out on COVID-19 impact in dentistry; (2) studies reporting dental patients’ perceptions, perspectives, or attitudes toward dental treatment during the COVID-19 pandemic; (3) studies analyzing dental patients’ anxiety or fear.
Data extraction was organized in tables containing the following information:
- Study characteristics: first author, year, country.
- Study design, period, and setting.
- Sample size and patients’ characteristics (gender and age).
- Types of dental emergency/urgency.
- Questionnaire structure.
- Main outcomes.
No numerical information was extracted from the figures reported in the study publications.
The risk of bias was assessed through the CHERRIES (Checklist for Reporting Results of Internet E-Surveys) or SUrge (SUrvey Reporting GuidelinE), as suggested by Weir et al. [20].
Given the lack of a validated checklist to evaluate the surveys, we adapted the CHERRIES checklist for web-based surveys and SUrge for self-administered surveys non-online administered. For both checklists, we applied the following procedure. For each checklist item, we assigned a value of 1 if the topic was reported in the study, and a value of 0 if it was not registered. Each survey’s final score was determined by calculating the sum of all valid items divided by their number. Low-, moderate-, or high-quality studies were assessed according to the following evaluation: final score < 35% = low quality; 35% ≤ final score < 75% = moderate quality; final score ≥ 75% = high quality.
2.2. Study Selection
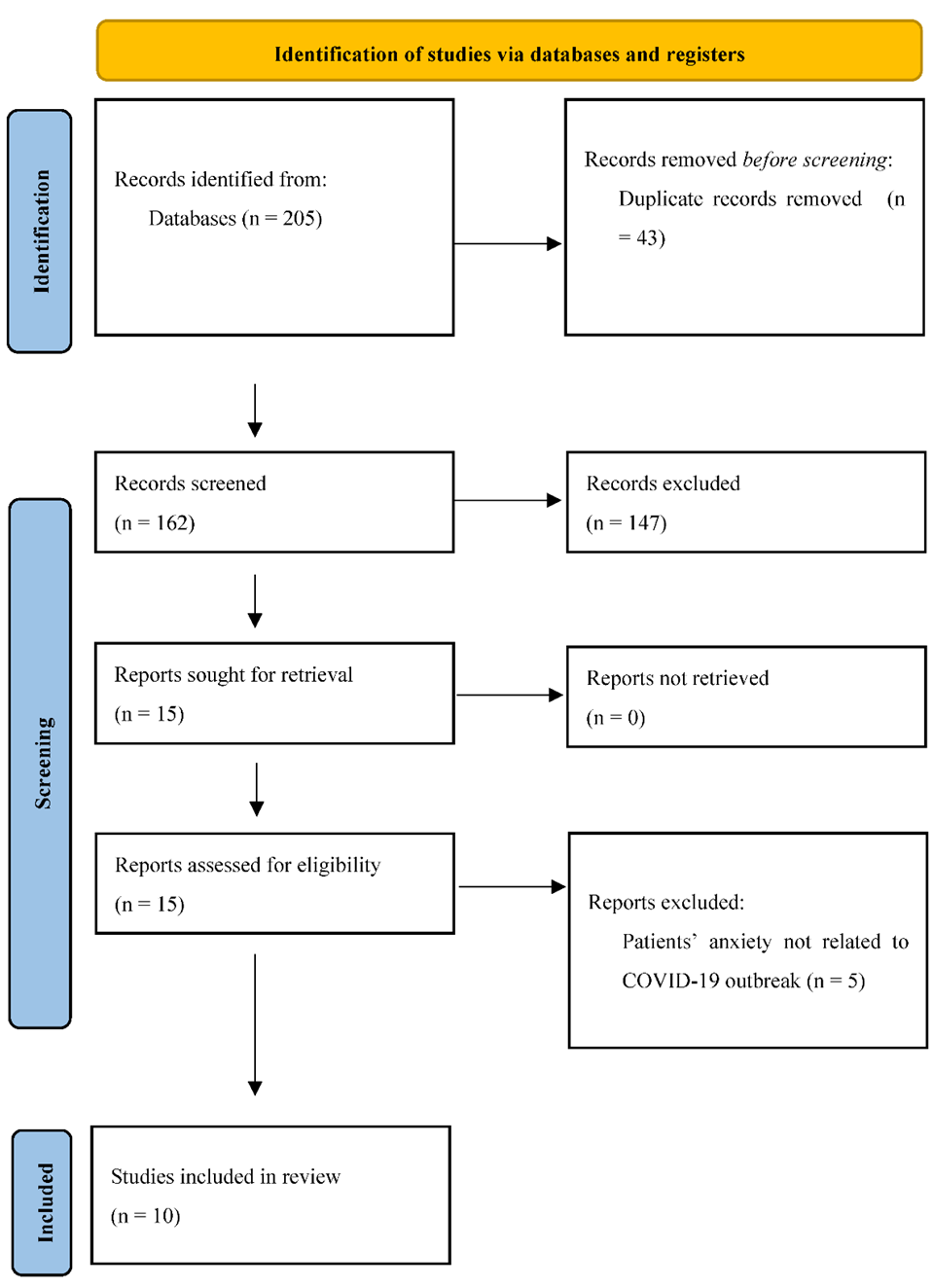
The literature search identified 205 studies. After removing duplicates and screening titles and abstracts, 15 full-text studies were reviewed. Ten studies between 2020 and 2021 met the inclusion and exclusion criteria. A flow diagram of the search strategy results is presented in Figure 1.
2.3. Risk of Bias
Given the lack of a specific tool for evaluating bias in surveys, we assessed the risk of bias using two checklists. The overall risk of bias assessment of the included studies is presented in Tables S1 and S2 in Supplementary Materials. Five studies reported a moderate level of bias [21,22,23,24,25], while the remaining five studies showed low quality [26,27,28,29,30].
In surveys administered through online platforms (Table S1 in Supplementary Materials), all studies reported the survey design describing the target population or sample frame. For IRB approval and informed consent process, IRB approval was obtained by seven out of eight studies [21,22,23,24,26,29,30], informed consent was obtained by four studies [22,25,28,29], and data protection was reported by only one study [22], while it was not applicable by four surveys [21,23,27,29]. Development and pre-testing were performed by only two studies [22,30]. For the recruitment process and description of the sample having access to the questionnaire, a closed survey was applied by all studies; only one indicated that the contact mode was not through the Internet [21], while advertising to announce the survey was carried out only by Moffat et al. [22]. All surveys were administered through the web or by email; six out of eight surveys described the context [21,22,23,24,28,30], and only two studies were not mandatory surveys [28,30]. Only one study used incentives [22], although this item was applicable for only two studies [21,22]. The timeframe was identified in five studies [21,22,23,24,28]. All included studies did not report the number of items, number of screens, and completeness check, while review steps were only adopted by Peloso et al. [29]. The unique visitor ID was assessed by two surveys [21,29], while none of the studies reported view rate, participation rate, and completion rate. For preventing multiple entries from the same individual, i.e., using cookies, IP check, log file analysis, and registration, no precautions were adopted by all surveys. Information about the handling of incomplete questionnaires was not described. Statistical corrections were adopted by five studies [21,22,23,24,28].
Two studies were evaluated through SUrge [25,27]. Although with slight differences, both studies lacked information regarding many items. Mainly, neither study reported the procedures used to develop, pre-test, and validate the new survey, sample size calculation and its representativeness, the type of contact, and incentives. Furthermore, the statistical analysis did not provide information about non-response error, response rate, and handling of missing data. In addition, neither study reported considerations about the non-response rate and possible differences in respondents’ samples and discussed the external validity of the findings. The complete results of risk of bias for both studies are reported in Table S2 (Supplementary Materials).
2.4. Study Characteristics
We provide a descriptive summary of the study design, period, setting, sample size, gender, age, types of dental emergency/urgency treated during the period of interest, and the questionnaire structure in Table 1. We included a total of 10 studies: 2 carried out in Brazil [26,29], 2 in the U.S.A. [22,25], 1 in Spain [21], Turkey [27], Italy [28], Saudi Arabia [23], China [24], and Nigeria [30], respectively.
Studies were carried out in 2020–2021: Quan et al. from February to March 2020, Gonzales et al. from March to June 2020, Moffat et al. in May 2020, Martina et al. from May to November 2020, Arqub from July to October 2020, and Nazir et al. from June to July 2020. Two studies [26,29] did not report the period of questionnaire administration but referred to that period being before the COVID-19 peak in Brazil: we presume before June 2020. Respondents were chosen in different settings: for four studies in public dental clinics or however related to academic scientific research units [24,26,28,29], three studies administered the questionnaires through private dental clinics [21,23,27], and two through web-survey addressed to local communities [21,22]. Only one study distributed the questionnaires to public and private dental clinics [30].
Six thousand three hundred and seventy (6370) patients were included in the studies. Three thousand seven hundred and forty-five (3745) respondents were female (female-male ratio 1.44). The mean age varied between 22.59 ± 8.28 [24] and 40 years [22]. Two studies reported age ranges instead of mean age [27,28], showing a high prevalence of young people (18–38 years) and a mild prevalence of older people (older than 60 years). Six studies involved mainly patients with orthodontic problems [21,23,24,27,29,30], two studies involved patients who received dental treatments after the COVID-19 outbreak [23,27], and the other two studies involved respondents who did not necessarily receive dental treatments after the COVID-19 outbreak [21,22].
All questionnaires were structured to gather data about socio-demographic questions (e.g., age, gender, education background, ethnicity, income, and city of residence). Three investigated COVID-19 and patient-related problems such as quarantine, COVID-19 symptoms, and COVID-19 infection [21,23,26]. Six studies investigated patients’ anxiety toward dental treatments through different validated or not-validated psychometric scales [21,23,24,25,26,27]. Nine studies investigated the risk perceptions, attitudes, avoidance behaviors, and beliefs toward the COVID-19 infection during dental treatments [21,22,23,24,25,26,28,29,30]. Five studies investigated protocols and procedures adopted by dental clinics to safeguard patients and allow them to feel comfortable about returning to the dental offices [22,25,26,29,30]. One study analyzed preferences regarding the urgency of following up treatments during the pandemic and preferred communication methods with the dentist [25]. Gonzales et al. only investigated possible reasons to avoid dental treatments [21].
2.5. Anxiety, Risk Perception, and Attitudes toward Dental Treatments during the Pandemic
Cotrin et al. [26], in a survey carried out presumably from March to June 2020, including 354 Brazilian respondents, reported a high level of anxiety (4.98 ± 2.42) among quarantine patients, with a substantial prevalence among females. Feelings about COVID-19 ranged from a relaxed (44.7%) or indifferent (5.6%) attitude to feelings of pain (3.4%), fear (23.4%), or anxiety (22.9%). Males were more willing to go to a dental appointment and more concerned about the delay in dental treatments due to COVID-19 restrictions. Dental appointment attendance continued to represent an important factor in everyday life, because 60.2% of the respondents would go to dental appointments for elective treatments. In comparison, only 25.1% of them would go only in case of urgency or emergency. About 15% of the respondents would not go to a dental appointment due to fear of contagion.
The same level of anxiety and fear emerged in Gonzales et al. study [21], which involved people living in Madrid. In an accurate comparison of the attitudes and perceptions of people toward dental treatment during the Spanish lockdown (March–June 2020), they showed that 30.9% of the respondents were afraid of going to the dentist because of the possibility of contagion with COVID-19. However, 56.3% of them continued to go to the dentist. More than 23% of the respondents decided to continue to go to the dentist because the planned dental treatment was not finished. The fear of COVID-19 impacted the start of new dental treatments such as orthodontics or implants: 42.5% of the Spanish respondents reported no intention to start a new treatment because of financial problems (16%) or fear of COVID-19 (24.5%). More than half of the interviewees would not go to the dentist until the disease was eradicated or an effective treatment was found. About 21% of the respondents stated they would not go to the dentist even in case of gum problems, 20.2% would not go even if they suspected cavities, and 16.3% would not go even if filling or teeth were fractured. The probability of dental avoidance due to the fear of COVID-19 infection was equal to 84% (OR = 5.18, 95%CI: 2.96–9.4) and increased to 88% in people older than 60 years (OR = 7.63, 95%CI: 3.56–15.35). Comparing infectability perception and aversion to germs at the beginning and at the end of the Spanish lockdown, Gonzales et al. showed an increase in the score of perceived vulnerability to disease, with a significant positive correlation between COVID-19 fear scale and infectability perception or aversion to germs in the post-lockdown period (p < 0.01).
In a study involving 300 patients who received dental treatments after the COVID-19 outbreak, Karagözoğlu et al. [27] reported a high level of anxiety (43.38 ± 8.34), especially in those who thought that COVID-19 could be transmitted through dental treatment (p < 0.001). Moreover, they showed that dental clinics were considered places with a high risk of contamination, given the close contact with dentists and other patients. Patients who would not seek dental treatment if their condition was not urgent also showed a higher level of anxiety (p < 0.003). On the contrary, a lower anxiety score was reported in patients who thought that adequate measures were taken in the dental unit (p < 0.001) and the measures taken by the dentists while treating patients were sufficient. A lower level of anxiety was also registered in patients who felt safe because healthcare professionals received the COVID-19 vaccine.
In a large study conducted in China involving 1078 orthodontic patients, Quan et al. [24] reported some difficulties for follow-up visits in 67.9% of respondents because of the risk of COVID-19 infection. However, during the pandemic crisis, 55.1% of the respondents contacted their attending doctors; on the contrary, 33.3% did not take any measure, and 23.1% even preferred to solve the problem according to their experience or common sense.
Two studies [23,25] did not report a significant level of dental anxiety related to the COVID-19 outbreak. However, Nazir et al. registered a higher level of dental fear among females (41.17 ± 17.94) than among males (37.65 ± 20.34) (p = 0.029).
In an American survey conducted in May 2020 through Amazon Mechanical Turk, Moffat et al. [22] interviewed 448 people. Many concerns were reported about contracting COVID-19 from dental professionals (3.7 ± 1.7) and other patients (3.3 ± 1.8) in the dental offices. However, the risk of getting COVID-19 in a dental office overweighed the risk of not getting necessary dental treatments.
Peloso et al. [29] in their study about patients’ perceptions in private dental clinics, that involved 595 Brazilians, showed that some interviewees were concerned about attending dental appointments because of the possibility of getting infected and/or of contaminating their family (18.5%), sometimes because dentists were considered at high risk of contamination. About 47% and 63% of the respondents reported increased feelings of anxiety, fear, or pain when the dental appointment was not postponable because of an emergency. About 20% of the respondents said that dental treatment could wait. In this study also, females were more worried about COVID-19 infection and less willing to go to dental appointments than males.
In a large study conducted on 1566 Italian orthodontic patients interviewed after the Italian lockdown (March–May 2020), Martina et al. [28] showed that 55.3% of the respondents believed there was a greater risk of COVID-19 infection during dental treatments. Furthermore, for 84.6% of patients, COVID-19 increased the fear of going to the dentist. Younger people and males were less scared to go to the dentist, while females and people older than 40 showed a high level of fear.
In a Nigerian survey conducted from 2020 until 2021 in public and private dental facilities involving 304 orthodontic patients, Umeh et al. [30] showed that people perceived themselves severely or moderately vulnerable to contracting COVID-19 (40.8% and 30.5%, respectively) but were willing to carry on with their dental treatments during the pandemic (72.4%). However, approximately 40% of the interviewees reported a certain level of fear of contracting the virus during dental appointments. In addition, the patients perceived the increase in treatment time and cost.
2.6. Protocols and Procedures for COVID-19 Infection Control in the Dental Setting
Five studies investigated the patients’ perception of protocols and procedures adopted in dental clinics to reduce the risk of COVID-19 infection [22,25,26,29,30].
Two studies [26,29], both carried out in Brazil, showed that wearing PPE improved patients’ confidence in dental professionals. In Cotrin et al. [26], more than 80% of the patients reported reduced anxiety and fear when dentists wore surgical masks and medical head caps during dental treatments; over half of the respondents reported a positive reduction of fear when dentists and medical staff wore face shields. In addition, some safety procedures, such as alcohol gel for patients and avoidance of crossing patients in the waiting areas, showed a positive effect in reducing the fear of COVID-19 infection in dental offices. The same trend, although with some percentage reductions, also emerged in Peloso et al. [29]
Moffat et al. [22] focused on patients’ confidence and awareness about the appropriate use of government recommendations within dental offices. The respondents reported low levels of trust that dental offices follow government recommendations to dental professionals during the COVID-19 pandemic (2.2 ± 1.2). At the same time, they perceived themselves as aware of the government recommendation to dental professionals for appropriate dental treatments during the COVID-19 outbreaks (3.8 ± 1.9).
In Arqub et al. [25], approximately 80% of the respondents believed that pretesting patients and medical staff during the pandemic reduced patients’ fear of COVID-19 infection in dental offices; wearing full PPE or N95 masks by dentists during dental treatments helped to increase patients’ trust in the safety of dental treatments.
Finally, Umeh et al. [30] reported that patients attributed a crucial role to many safety procedures to access dental offices: social distancing, temperature screening before access, relevant screening questions, limiting the number of adults accompanying a child, wearing facemasks, and handwashing were found to play a crucial role in enhancing patients’ trust.
3. Current Status
This work aimed to understand dental patients’ perspectives, perceptions, attitudes, and expectations toward dental treatments after the first year of the COVID-19 pandemic. In the last two years, many studies have investigated the role of dentists in reducing COVID-19 risk infection and resuming their daily activity keeping a high level of safety [31]. Although dental professionals have been considered at high risk due to the close contact with patients’ mouth and the upper respiratory tract [2] and the use of aerosol-generating procedures [32,33,34,35], many recommendations and guidelines have provided support to restart dental activity safely.
For the patients, returning to good oral health habits without increasing the risk of COVID-19 infection, and therefore returning to routine dental care, is very important as it provides extensive benefits to the population [22].
Many encouraging findings have emerged from our work. Patients are aware of the recommendation to reduce the risk of contagion and stringently follow them. Social distancing, handwashing with alcohol gel, wearing face masks, and avoiding close contact with other patients were perceived as safe procedures to access dental clinics. The same positive perception emerged when dentists wore all PPE and used N95 or FFP2 masks or face shields during dental treatments. The adoption of these procedures by dentists was not considered a hindrance to dental treatments. Still, it was an appropriate medical staff’s behavior to assure the optimal resumption of elective dental treatments. Assurances of public health officials and institutions of the safety restart of routine dental care have also been reported as determinants in enhancing trust in this resumption [22].
About anxiety and fear of COVID-19 infection during dental treatments, we observed an increased sense of pain and nervousness during the first COVID-19 outbreak. Due to stringent lockdowns, people closed in their homes suffered a higher level of anxiety [17], which necessarily had repercussions on behaviors and perceptions toward dental treatments. This perception should be considered as multifactorial. While a high level of dental anxiety was observed after confinement in different studies, with a prevalence ranging from 27.2 to 38.7% [36,37], it should be observed that dental treatments require patients to avoid, albeit for a short time, the use of personal protection, like masks and social distancing, tools that continue to be indicated as the first and essential barriers to prevent infection, even now that vaccines are available in many countries and large populations have already received two vaccine doses [38].
Females demonstrated a significantly higher dental anxiety and fear than males. This can be partly explained as the consequence of females’ higher level of anxiety toward dental treatments [39,40] and, in the last two years, toward the COVID-19 pandemic [41]. During the COVID-19 pandemic, males were more willing to attend a dental appointment, while females were strongly prevented from going to the dentist by their fear of infection, and a natural aversion to germs made them prefer to postpone non-urgent dental appointments [21].
About the behaviors of younger people, we report different findings. In Cotrin et al., the younger showed a higher level of anxiety and depressive symptoms toward dental treatments than older people [26]. On the contrary, Martina et al. reported a higher level of fear among younger people than among people over 40 years [28]. These contrasting results should be due to the different times of observation. During the evolution of the COVID-19 pandemic, scientific evidence has proved a higher risk of infection for older people that could have translated in a significant growing attention of the adults to avoid situations that could increase the risk of contagion. Thus, dentist avoidance emerged as a protective measure during quarantine, especially for patients who perceive a high risk of infection, are afraid of COVID-19, and are older than 60 years [21].
This study has several limitations. First, significant heterogeneity among the included studies was observed, preventing us from determining a quantitative prevalence of dental anxiety associated with the COVID-19 pandemic. Second, the sample sizes varied from hundreds of patients to more than 1500. Thus, in some cases, the sample size could not be representative of the reference population. Third, some studies reported dental anxiety and fear of patients not needing dental care and who would not schedule dental care at that time, so that the lack of a concrete need could have altered the perception. Fourth, the prevalence of COVID-19 infection and mortality in the interviewed area was not considered. Finally, all included studies had a cross-sectional design and were executed by adopting a self-reported questionnaire that, in some cases, used not-validated tools for psychometric measurements.
4. Conclusions and Prospects
The dental profession has always faced complex challenges related to viral pandemics. However, as demonstrated during the COVID-19 outbreak, dentists have promptly responded to new scenarios, improving safety. According to the COVID-19 guidelines, dentists change their workflows patterns or re-configure their clinic settings to ensure safety. Many precautions consist in increasing the use of protective materials and/or in prolonging the treatment time. If, on the one hand, these behaviors assure high safety standards for patients and dental treatments, on the other hand, they increase the cost of dental treatments. To reduce the impact of such new costs, some dentists have added significant charges for PPE to their bills, especially in the case of aerosol-generating procedures. In these cases, the cost of safety is entirely absorbed by patients who may be induced to go to the dentist only in cases of urgency. On the contrary, the lack of national policies to reduce the impact of the cost related to the proper application of the recommended guidelines, also in private dental offices, can increase the pressure on dentists and may set the stage for increased errors to avoid a significant rise of patients’ cost.
How to prevent such negative scenarios? These issues spotlight the need for shared national policies to reduce the negative impact of the COVID-19 crisis. As done in many countries to support national and local economies, in the new normalcy of dentistry after the COVID-19 outbreak, sharing costs among patients, dentists, and national policies may help restore the regular dental activity, helping patients not to renounce dental treatments.
In conclusion:
- The availability of vaccines for the population and the awareness of patients about recommended guidelines to prevent COVID-19 contagion support a safe and lasting resumption of routine dental activities
- Communication with patients about adopted precautions in dental clinics plays a fundamental role in reducing patients’ dental anxiety and fear related to the risk of COVID-19 infection within dental clinics.
- Compliance with dentist appointments should be encouraged, helping patients rediscover the confidential relationship of trust with their dentist and return to regular dental visits.
- Identifying economic policies to support the current financial pressure due to the high cost of dental treatments may speed up the return to normalcy for dentists and patients.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/encyclopedia2010022/s1. Table S1: Risk of bias-CHERRIES Checklist. Table S2: Risk of bias-SUrge Checklist.
Author Contributions
Conceptualization, S.S. and M.L.G.; methodology, M.L.G. and E.A.; software, M.L.G. and P.B.; validation, S.S., M.L.G., E.A., and M.S.; writing—original draft preparation, M.L.G., E.A., and P.B.; writing—review and editing, S.S. and M.S.; supervision, M.L.G. and E.A.; project administration, M.L.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not Applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| DFS | Dental Fear Survey |
| MDAS | Modified Dental Anxiety Scale |
| MTurk | Mechanical Turk |
| NRS | Numerical Rating Scale |
| PPE | Personal Protective Equipment |
| PVD | Perceived Vulnerability to disease |
| TMD | Temporomandibular Disorders |
References
- American Dental Association. ADA Recommending Dentists Postpone Elective Procedures. Available online: https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-recommending-dentists-postpone-elective-procedures (accessed on 29 October 2021).
- Center for Disease Control and Prevention, SARS-CoV-2 and Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html (accessed on 29 October 2021).
- Bakaeen, L.G.; Masri, R.; AlTarawneh, S.; Garcia, L.T.; AlHadidi, A.; Khamis, A.H.; Hamdan, A.M.; Baqain, Z.H. Dentists’ knowledge, attitudes, and professional behavior toward the COVID-19 pandemic: A multisite survey of dentists’ perspectives. J. Am. Dent. Assoc. 2021, 152, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Beltran-Aguilar, E.; Benzian, H.; Niederman, R. Rational perspectives on risk and certainty for dentistry during the COVID-19 pandemic. Am. J. Infect. Control. 2021, 49, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Salgarello, S.; Salvadori, M.; Mazzoleni, F.; Salvalai, V.; Francinelli, J.; Bertoletti, P.; Lorenzi, D.; Audino, E.; Garo, M.L. Urgent Dental Care During Italian Lockdown: A Cross-sectional Survey. J. Endod. 2021, 47, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Ball, M.; Akintola, D.; Harrington, Z.; Djemal, S. Emergency dental care triage during the COVID-19 pandemic. Br. Dent. J. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Eggmann, F.; Haschemi, A.A.; Doukoudis, D.; Filippi, A.; Verna, C.; Walter, C.; Weiger, R.; Zitzmann, N.U.; Bornstein, M.M. Impact of the COVID-19 pandemic on urgent dental care delivery in a Swiss university center for dental medicine. Clin. Oral Investig. 2021, 25, 5711–5721. [Google Scholar] [CrossRef] [PubMed]
- Ostrc, T.; Pavlovic, K.; Fidler, A. Urgent dental care on a national level during the COVID-19 epidemic. Clin. Exp. Dent. Res. 2021, 7, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Pajpani, M.; Patel, K.; Bendkowski, A.; Stenhouse, P. Rapid response: Activity from a hospital based Urgent Dental Care Centre during the COVID-19 pandemic. Br. J. Oral Maxillofac. Surg. 2020, 58, e98–e103. [Google Scholar] [CrossRef]
- Walter, E.; von Bronk, L.; Hickel, R.; Huth, K.C. Impact of COVID-19 on Dental Care during a National Lockdown: A Retrospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 7963. [Google Scholar] [CrossRef]
- Salgarello, S.; Salvadori, M.; Mazzoleni, F.; Francinelli, J.; Bertoletti, P.; Audino, E.; Garo, M.L. The New Normalcy in Dentistry after the COVID-19 Pandemic: An Italian Cross-Sectional Survey. Dent. J. 2021, 9, 86. [Google Scholar] [CrossRef]
- American Dental Association. ADA ‘Strongly’ Encouraging Dental Professionals to be Vaccinated for COVID-19. Available online: https://www.ada.org/en/publications/ada-news/2021-archive/july/ada-strongly-encouraging-dental-professionals-to-be-vaccinated (accessed on 29 October 2021).
- Zigron, A.; Dror, A.A.; Morozov, N.G.; Shani, T.; Haj Khalil, T.; Eisenbach, N.; Rayan, D.; Daoud, A.; Kablan, F.; Marei, H.; et al. COVID-19 Vaccine Acceptance Among Dental Professionals Based on Employment Status During the Pandemic. Front Med. 2021, 8, 618403. [Google Scholar] [CrossRef]
- Menhadji, P.; Patel, R.; Asimakopoulou, K.; Quinn, B.; Khoshkhounejad, G.; Pasha, P.; Garcia Sanchez, R.; Ide, M.; Kalsi, P.; Nibali, L. Patients‘ and dentists’ perceptions of tele-dentistry at the time of COVID-19. A questionnaire-based study. J. Dent. 2021, 113, 103782. [Google Scholar] [CrossRef] [PubMed]
- Yavan, M.A. Effects of the COVID-19 pandemic on new patient visits for orthodontic treatment: A comparison of 2020 and the previous 3 years. J. World Fed. Orthod. 2021, 10, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Zhou, Y.; Liu, X.; Tan, J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J. Dent. Sci. 2020, 15, 564–567. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Huang, X.; Zhang, S.; Yang, J.; Yang, L.; Xu, M. Comparison of Prevalence and Associated Factors of Anxiety and Depression Among People Affected by versus People Unaffected by Quarantine During the COVID-19 Epidemic in Southwestern China. Med. Sci. Monit. 2020, 26, e924609. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Weir, K.R.; Ailabouni, N.J.; Schneider, C.R.; Hilmer, S.N.; Reeve, E. Considerations for systematic reviews of quantitative surveys: Learnings from a systematic review of the patients’ Attitudes Towards Deprescribing questionnaire. Res. Soc. Adm. Pharm. 2021, 18, 2345–2349. [Google Scholar] [CrossRef]
- Gonzalez-Olmo, M.J.; Delgado-Ramos, B.; Ortega-Martinez, A.R.; Romero-Maroto, M.; Carrillo-Diaz, M. Fear of COVID-19 in Madrid. Will patients avoid dental care? Int. Dent. J. 2022, 72, 76–82. [Google Scholar] [CrossRef]
- Moffat, R.C.; Yentes, C.T.; Crookston, B.T.; West, J.H. Patient Perceptions about Professional Dental Services during the COVID-19 Pandemic. JDR Clin. Trans. Res. 2021, 6, 15–23. [Google Scholar] [CrossRef]
- Nazir, M.; Almulhim, K.S.; AlDaamah, Z.; Bubshait, S.; Sallout, M.; AlGhamdi, S.; Alhumaid, J. Dental Fear and Patient Preference for Emergency Dental Treatment Among Adults in COVID-19 Quarantine Centers in Dammam, Saudi Arabia. Patient Prefer. Adherence 2021, 15, 1707–1715. [Google Scholar] [CrossRef]
- Quan, S.; Guo, Y.; Zhou, J.; Zhang, G.; Xing, K.; Mei, H.; Li, J. Orthodontic emergencies and mental state of Chinese orthodontic patients during the COVID-19 pandemic. BMC Oral Health 2021, 21, 477. [Google Scholar] [CrossRef] [PubMed]
- Arqub, S.A.; Voldman, R.; Ahmida, A.; Kuo, C.L.; Godoy, L.D.C.; Nasrawi, Y.; Al-Khateeb, S.N.; Uribe, F. Patients’ perceptions of orthodontic treatment experiences during COVID-19: A cross-sectional study. Prog. Orthod. 2021, 22, 17. [Google Scholar] [CrossRef] [PubMed]
- Cotrin, P.; Peloso, R.M.; Oliveira, R.C.; de Oliveira, R.C.G.; Pini, N.I.P.; Valarelli, F.P.; Freitas, K.M.S. Impact of coronavirus pandemic in appointments and anxiety/concerns of patients regarding orthodontic treatment. Orthod. Craniofac. Res. 2020, 23, 455–461. [Google Scholar] [CrossRef] [PubMed]
- KaragÖZoĞLu, İ.; Parlar ÖZ, Ö. Investigation of the patients’ perception on dental treatment and their anxiety levels during the COVID-19 pandemic process. J. Health Sci. Med. 2021, 4, 710–715. [Google Scholar] [CrossRef]
- Martina, S.; Amato, A.; Faccioni, P.; Iandolo, A.; Amato, M.; Rongo, R. The perception of COVID-19 among Italian dental patients: An orthodontic point of view. Prog. Orthod. 2021, 22, 11. [Google Scholar] [CrossRef]
- Peloso, R.M.; Pini, N.I.P.; Sundfeld Neto, D.; Mori, A.A.; Oliveira, R.C.G.; Valarelli, F.P.; Freitas, K.M.S. How does the quarantine resulting from COVID-19 impact dental appointments and patient anxiety levels? Braz. Oral Res. 2020, 34, e84. [Google Scholar] [CrossRef]
- Umeh, O.D.; Utomi, I.L.; Isiekwe, I.G.; Aladenika, E.T. Impact of the coronavirus disease 2019 pandemic on orthodontic patients and their attitude to orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e399–e409. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for Clinical Dental Care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Lanmark 360. Survey of COVID-19 Dental Patients’ Perceptions and Attitudes Toward Returning to Dental Practices. Available online: https://lanmark360.com/research/Lanmark360-Dental-Patients-COVID-19-Survey-Results.pdf (accessed on 29 October 2021).
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; Kc, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A systematic review of droplet and aerosol generation in dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Zimmermann, M.; Nkenke, E. Approaches to the management of patients in oral and maxillofacial surgery during COVID-19 pandemic. J. Craniomaxillofac. Surg. 2020, 48, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatr. 2020, 51, 102083. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data, Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 15 October 2021).
- Jeddy, N.; Nithya, S.; Radhika, T.; Jeddy, N. Dental anxiety and influencing factors: A cross-sectional questionnaire-based survey. Indian J. Dent. Res. 2018, 29, 10–15. [Google Scholar] [CrossRef]
- Lin, C.S.; Wu, S.Y.; Yi, C.A. Association between Anxiety and Pain in Dental Treatment: A Systematic Review and Meta-analysis. J. Dent. Res. 2017, 96, 153–162. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flow-chart.


{kind=link}
Table 1.
Studies characteristics.
| Study | Country | Study Design | Period | Setting | Sample Size | Gender | Age | Types of Dental Emergency/Urgency | Questionnaire Structure | Main Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Cotrin et al. (2020) [26] | Brasil | Survey | NR * | Private Dental Clinics | 354 | 231 females and 123 males | 35.49 ± 13.93 | Orthodontic treatments |
|
|
| Moffat et al. (2020) [22] | USA | Survey | May 2020 | Web-survey through Amazon Mechanical Turk (MTurk) | 452 | 198 females, 250 males, and 4 NR | 40 years | None |
|
|
| Peloso et al. (2020) [29] | Brazil | Survey | NR * | Private Dental Clinics | 595 | 412 females and 183 males | 38.21 ±13.94 | 74.3% orthodontic18.4% oral rehabilitation7.3% restorative or other |
|
|
| Arqub et al. (2021) [25] | USA | Survey | July–October 2020 | Dental Clinic | 154 | 95 females and 59 males | 29.30 ± 12.01 | Orthodontic treatments |
|
|
| Gonzales-Olmo et al. (2021) [21] | Spain | Survey—Repeated measures design (before and after Spain lockdown) | March–June 2020 | Web-survey addressed to community of Madrid | 961 | 559 females and 402 males | 38.4 ± 16.1 | None |
|
|
| Karagözoğlu et al. (2021) [27] | Turkey | Survey | NR | Dentistry Faculty | 300 | 145 females and 155 males | 18–38: 53%, 39–59: 31.7%; 60–80: 15.3% | Patients receiving dental treatment |
|
|
| Martina et al. (2021) [28] | Italy | Survey | May–November 2020 | Web Survey | 1566 | 852 females, 698 males, 16 NR | 18–29: 31.3%30–39: 29.8%40–49: 18.3%; 50–59: 10.6%; 60–69: 6.8%; >70.3% | Orthodontic care |
|
|
| Nazir et al. (2021) [23] | Saudi Arabia | Survey | June–July 2020 | Scientific research unit at the College of Dentistry | 606 | 246 females and 360 males | 30.49 ± 12.01 | Patients receiving dental treatment |
|
|
| Quan et al. (2021) [24] | China | Survey | February–March 2020 | Dental Clinic | 1078 | 786 females and 292 males | 22.59 ± 8.28 | Orthodontic patients |
|
|
| Umeh et al. (2021) [30] | Nigeria | Survey | Public and private dental facilities | 304 | 221 females and 83 males | 35.6 | Orthodontic patients receive treatment |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Salgarello, S.; Audino, E.; Bertoletti, P.; Salvadori, M.; Garo, M.L. Dental Patients’ Perspective on COVID-19: A Systematic Review. Encyclopedia 2022, 2, 365-382. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010022
AMA Style
Salgarello S, Audino E, Bertoletti P, Salvadori M, Garo ML. Dental Patients’ Perspective on COVID-19: A Systematic Review. Encyclopedia. 2022; 2(1):365-382. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010022
Chicago/Turabian StyleSalgarello, Stefano, Elisabetta Audino, Paolo Bertoletti, Matteo Salvadori, and Maria Luisa Garo. 2022. "Dental Patients’ Perspective on COVID-19: A Systematic Review" Encyclopedia 2, no. 1: 365-382. https://0-doi-org.brum.beds.ac.uk/10.3390/encyclopedia2010022