Ovarian Rejuvenation Using Autologous Platelet-Rich Plasma


1
Department of Obstetrics and Gynecology, School of Medicine, International University of Health and Welfare, Narita, Chiba 286-8686, Japan
2
Phoenix ART Clinic, Shibuya, Tokyo 151-0051, Japan
*
Author to whom correspondence should be addressed.
Endocrines 2021, 2(1), 15-27; https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2010002
Submission received: 20 November 2020
/
Revised: 29 December 2020
/
Accepted: 5 January 2021
/
Published: 7 January 2021
Abstract
:Advanced maternal age is associated with the natural oocyte depletion, leading to low oocyte yield, high infertility treatment cancellation rates, and eventual decreases in pregnancy rates. Various innovative interventions have been introduced to improve the outcome of infertility treatment for aging patients. Numerous published data demonstrated that early follicle development was regulated by intraovarian growth factors through autocrine or paracrine mechanisms. Platelet-rich plasma (PRP), a plasma fraction of peripheral blood with a high concentration of platelets, has been implemented in regenerative medicine in the last decade. The plasma contains a variety of growth factors that were suggested to be able to enhance angiogenesis regeneration and the cell proliferation process. The initial report showed that an intraovarian injection of PRP improved the hormonal profile and increased the number of retrieved oocytes in patients with diminished ovarian reserve. Subsequently, several studies with larger sample sizes have reported that this approach resulted in several healthy live births with no apparent complications. However, the use of ovarian PRP treatment needs to be fully investigated, because no randomized controlled trial has yet been performed to confirm its efficacy.
1. Introduction
Along with the global modernization, women tend to delay their childbearing due to professional investment and seeking better living conditions. Recent data revealed a significant rise in the mean age of first-time mothers, ranging between the third and fourth decade [1,2]. This is associated with ovarian aging, which is a physiological process characterized by declining oocyte quantity and quality—an unsolved problem in reproductive medicine. Premature ovarian insufficiency (POI), a condition characterized by a premature decline of ovarian function occurring before the age of 40, has risen from 1% to nearly 2% in the last few decades [3,4]. These changes placed a requirement of implementation therapeutic strategies for these low prognostic infertile women. Indeed, many innovative approaches have been proposed to fulfill the desire of aforementioned patients to have genetically related offspring.
Platelet-rich plasma (PRP), derived from peripheral blood, consists of a high number of platelets (about 1,000,000 of platelets/μL in 5 mL of plasma) [5,6]. The alpha granules of activated platelets release a variety of growth factors including platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β), vascular endothelial growth factor (VEGF), insulin-like growth factor-1 (IGF-I), basic fibroblast growth factor (bFGF), epidermal growth factor (EGF), and pro-inflammatory cytokines (IL-1β and IL-6) [5,7]. PRP has been shown to enhance effectively the regeneration and healing of human tissue [8,9,10,11].
In reproductive medicine, PRP was first used to enhance endometrial thickness in patients attempting in vitro fertilization (IVF) treatment [12]. Several subsequent reports revealed that that intraovarian injection of PRP promoted the follicle growth and improved the treatment outcome in poor prognostic infertile women, resulting in several live births without complications.
In this article, we comprehensively summarized the hypothesis and reported clinical results involving the autologous PRP intraovarian injections to “rejuvenate” ovaries.
2. Bioactive Factors in PRP and their Role in Folliculogenesis
PRP is a biological product defined as a portion of the plasma with highly concentrated platelets after the centrifugation of peripherally collected blood [5]. Upon the activation of platelets, the alpha granules release several biologically active factors, including PDGF, TGF-β, IGF-I, VEGF, EGF, bFGF, and pro-inflammatory cytokines [5,7,13,14,15]. Moreover, several other factors consisting of hepatocyte growth factor (HGF), stem cell factor (SCF), connective tissue growth factor (CTGF), neurotrophins, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), and growth hormone (GH) were demonstrated to be present in PRP [5,16] and act synergistically to induce accelerated angiogenesis, cell migration, differentiation, and proliferation [17].
In ovary, these growth factors are demonstrated to play crucial roles in modulating the folliculogenesis (Table 1 and Figure 1). TGF-β family members in PRP including bone morphogenetic proteins (BMPs), growth and differentiation factors (GDFs), and activins regulate several ovarian functions [18]. At the early stage of folliculogenesis, activins promote the survival of oocytes and the formation of primordial follicles via smad2/smad3 signaling by the kit ligand/c-Kit pathway [19]. BMP7 and BMP4 regulate the recruitment of primordial follicles to promote primordial to primary follicle transition [20,21]. Later on, GDF-9, BMPs, and activins are responsible for the development from primary follicles to the early antral stage. GDF-9, a proliferation factor for granulosa cells, is essential for the growth of follicles after the primary stage [22,23]. The deficiency of GDF-9 in mice led to the blockage of follicular development beyond the primary stage and results in infertility [24]. In humans, the altered GDF-9 function was detected in POI women and mothers of dizygotic twins [25]. Furthermore, GDF-9 supports follicular survival by suppressing granulosa cell apoptosis and follicular atresia [26]. Meanwhile, BMPs play critical roles in preantral follicle activation and maintenance [27]. Subsequently, the antral follicle growth and the dominant follicle selection are modulated by GDF-9, several BMPs, and the inhibin–activin system. GDF-9 enhances glycolysis and sterol biosynthesis in cumulus cells prior to the luteinizing hormone (LH) surge [25]. BMPs are essential for the cumulus cell expansion and stabilization, ovulation, embryonic development, and corpus luteum activity [18]. The levels of GDF9 and BMP15 in the follicular fluid were significantly correlated with oocyte nuclear maturation and embryo quality [28]. Activins modulate oocyte maturation; meanwhile, inhibin upregulates LH-induced androgen secretion to sustain estradiol biosynthesis during the pre-ovulatory phase [29,30,31]. In addition, studies have shown that GDF9, activins, and several BMPs stimulate the expression of follicle stimulating hormone (FSH) receptors as well as increase the stability of FSH receptor mRNA [18]. Smad proteins, downstream molecules for intracellular TGF-β signaling, regulate the apoptosis of follicles [32,33].
Other various growth factors contained in PRP are also important for follicular growth and maturation. At the early stage of folliculogenesis, bFGF, HGF, and SCF induce primordial follicle activation, initiating the folliculogenesis [34,35,36,37]. In mice model experiments, the bFGF-treated ovaries had a higher percentage of developing follicles compared to the control ovaries [34]. Similarly, HGF takes part in the initiation of the primordial follicle development by interacting with kit ligand [35]; meanwhile, SCF upregulates kit ligand mRNA expression and stimulates the phosphatidylinositol 3-kinase/AKT pathway [36,37]. IL-1β promotes the development of primordial follicles [38]. CTGF is necessary for normal primordial follicle assembly, primary follicle development, and ovulation [39,40,41,42]. Loss of CTGF in granulosa cells results in arrested granulosa cell growth, early differentiation of granulosa cells, and retarded follicle development, resulting in subfertility [39]. Neurotrophins nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT-3), neurotrophin-4 (NT-4), and glial cell line-derived neurotrophic factor (GDNF) also play crucial roles in female fertile function. Upon binding to specific receptors, they stimulate a variety of signal pathways involving many phenomena during folliculogenesis, including ovarian follicle assembly, primordial follicle activation, follicular development, steroidogenesis, oocyte maturation, ovulation, and corpus luteum formation [43,44,45]. Dysregulation of these factors is associated with infertility or ovarian diseases including diminished ovarian reserve, PCOS, endometriosis, and even ovarian cancer [44]. PDGF, secreted by the oocyte and granulosa cells with receptors located in granulosa cells, takes part in the activation of primordial follicle [46]. During folliculogenesis, there is a significant increase the number of blood vessels stimulated by different angiogenic modulating factors. Several factors available in PRP such as VEGFs, FGF2, and IGF can activate ovarian neovascularization, improving follicle growth and oocyte quality [47,48,49,50,51,52]. The inhibition of VEGF is linked to the deficiency of angiogenesis, altering of follicular growth, and viability [51]. IGF, released from the granulosa cells, is indispensable in granulosa cell replication. The depletion of this factor leads to the dysfunction and apoptosis of the granulosa cells [53]. Moreover, IGF-I and GH collaborate with FSH to enhance the steroidogenesis and follicle growth in rats as well as human granulosa cells [54,55,56]. GM-CSF has a part in the follicle development, as its treatment in rat ovary was revealed to increase significantly the number of small preantral and large preantral follicles compared with the control group [57]. SCF and HGF regulate the interplay between theca and granulosa cells by promoting cell proliferation and steroidogenesis [58].
At the later phase of folliculogenesis, IL-1β facilitates ovulation by activating the production of prostaglandins, collagenases, hyaluronic acid, and proteoglycans. IL-6 coordinates with IL-8 to assist follicle rupture and neovascularization during the subsequent formation of the corpus luteum [59]. EGF transfers the LH signal from the periphery of the follicle to the cumulus-oocyte complex (COC) to expand COC and result in ovulation [60]. Another study suggested that GM-CSF also increases cumulus cell expansion of in vitro matured bovine COC [61]. G-CSF, whose concentration in follicular fluid was significantly higher than in serum, especially at the ovulation stage, was also suggested to have an important role in ovulation [62,63]. G-CSF treatment increased the competence of oocytes and the embryo’s viability in in vitro culture porcine follicles [64]. In women with the luteinized unruptured follicle syndrome, G-CSF could enhance oocyte release from the follicle [65].
3. The Hypothesized Mechanism of PRP in Ovarian “Rejuvenation”
Given the roles of the bioactive factors presented in PRP in folliculogenesis, the intraovarian injection of PRP is supposed to improve follicular growth. Thus, it is rational to hypothesize that autologous PRP intraovarian infusion treatment could “rejuvenate” the dysfunctional ovarian tissue.
In cyclophosphamide-induced ovarian failure rats, PRP treatment increased the ovarian cortex volume, pre-antral follicles number, and antral follicle diameter [67]. In another study, histopathological studies presented that receiving PRP treatments improved not only the quantity but also quality of follicles in all stages in mice ovaries. In comparison to the control group, the PRP-treated group had an evidently lower number of atretic follicles [68]. In bovine ovaries, a study presented that the serum progesterone concentrations were increased in four of the five cows treated with PRP, followed by four pregnancies after artificial insemination. Meanwhile, there were no recorded variation in progesterone concentration and pregnancies in the control group [69]. Another study suggested that latent follicles and in vivo embryo production could be stimulated by PRP treatment [70]. In an in vitro study, PRP culture could increase the viability and the development of isolated human primordial and primary follicles [71].
Considering the angiogenic features of platelet-derived cytokines, PRP is also expected to ameliorate the aging ovaries by increasing the neovascularization. Studies reported that the molecular network promoting angiogenesis was significantly disrupted in patients presenting with ovarian dysfunction [72,73]. An increase of vascularization in ovary enhances its blood nourishment, contributing to the follicular growth and oocyte quality, resulting in higher fertilization and developmental potentials [74]. Moreover, enhancing oxygen perfusion improves intrafollicular oxygen and better ooplasm quality, leading to the recovery of mitochondrial function that drives a higher possibility to produce an ongoing pregnancy [75]. Numerous publications reported that PRP could improve neoangiogenesis in different clinical situations, especially in regenerative medicine [76,77,78]. At the level of ovary, PRP was revealed to prevent effectively of ischemia and reperfusion damage by studying ovarian torsion in a rat model. PRP decreased the mean total oxidant status, oxidative stress index, and histopathological scores [79]. In POI rats’ ovaries, the PRP injection induced ovarian tissue vascularization via an increase of alpha-smooth muscle actin in the small arteries [68].
4. Clinical Outcomes of Intraovarian PRP Injection
Based on the putative mechanisms of PRP treatment in recovering ovarian dysfunction, several clinics have initiated PRP therapy as an adjuvant treatment. There have been several recorded positive outcomes in both case studies and comparative studies.
4.1. Case Report and Case Series Studies
In the first study describing the benefit of PRP on ovarian function, a patient without ovaries obtained a healthy baby in the first cycle of stimulation after ovarian tissue grafting. Instead of a normal grafting procedure, the frozen-thawed ovarian cubes of this patient were impregnated with a gel preparation of PRP [80]. However, it was difficult to determine whether this positive result is the contribution of PRP, since this study did not have the control tissue grafting without PRP treatment. Subsequently, many case reports and case series studies showed some favorable outcomes in low prognostic infertile women including POI patients and poor responders with diminished ovarian reserve (DOR) (Table 2).
In a case report study, a significant decline in FSH levels and elevation of AMH levels from 0.02 to 0.08 ng/mL were observed in a POI patient at 40 years of age with 19 months amenorrhea after 4 mL per ovary injection of PRP prepared from 30 mL of peripheral blood. The pregnancy was obtained after natural IVF at after 8 weeks of PRP treatment, although it ended in a biochemical loss miscarriage [81]. Another case report showed the outcome of PRP treatment in a POI patient who used to be an extremely poor responder with an undetectable serum level of AMH (<0.02 ng/mL) and 6 months amenorrhea. After the intraovarian injection of 3 mL of autologous PRP in combination with gonadotropin prepared from 40 mL of peripheral blood, this patient received controlled ovarian stimulation and IVF. The patient’s menstrual periods resumed, and good antral follicles were observed in two successive cycles after PRP treatment. After the transferring of three cleavage-stage embryos, a successful pregnancy was obtained, which eventually resulted in live birth of twins [82].
The first case series study reported intraovarian PRP injection in a group of eight infertile women aged 45.13 ± 4.42 years, having the absence of menstrual cycle for 4.88 ± 1.13 months. Autologous PRP was infused into each ovary using a transvaginal ultrasound guided injection under natural IVF cycle. The menstrual cycle was restored 1–3 months after the ovarian PRP treatment. The subsequent oocyte retrievals were successful in all cases, resulting in 1.50 ± 0.71 cryopreserved embryos. However, the result about the outcome of embryos transferring was not included [83].
Subsequently, a second case series study described the PRP effectiveness in four DOR patients. The mean (±SD) patient age was 42 ± 4 years with long infertility duration. They injected 5 mL of autologous PRP to each ovary under transvaginal ultrasound guidance. After an IVF program, 5.3 ± 1.3 of mature oocytes per ovarian stimulation were obtained. All patients could have at least one blastocyst suitable for cryopreservation and an obvious reduction of serum follicle stimulating hormone (FSH) levels. Nevertheless, their AMH levels were not significantly changed, and the number of retrieved oocytes before PRP treatment and the outcome of embryo transfer was not described in this study [84].
Another study in two POI patients with 27 and 40 years of age and one menopausal woman aged 46 years using same transvaginal approach to both ovaries revealed a decrease of a previously high FSH level and a concurrent increase of AMH levels after 4 mL of autologous injection of PRP prepared from 30 mL of peripheral blood to each ovary. Each of three patients obtained a healthy, ongoing complication-free clinical pregnancy spontaneously in less than half a year following PRP treatment. In this study, the duration of amenorrhea in three patients ranged from 12 to 26 months. In contrast, their AMH levels were relatively high ranging from 0.06 to 0.17 ng/mL [85] as compared to POI patients, suggesting a potential of natural conception without PRP intervention.
Another study reported the improved outcome of intraovarian injection of PRP in three poor responders with multiple previous failed IVF cycles. The FSH and AMH levels in these three patients were ranging from 18.3 to 27.8 mIU/mL and 0.44 to 0.65 ng/mL, respectively. Within a 3-month interval, FSH decreased by 67.33%, while AMH level increased by 75.18%, although the numbers of retrieved oocytes were not increased after PRP treatment. An uncomplicated healthy pregnancy at 17 weeks and a successful live birth were achieved through IVF, while one pregnancy was spontaneous 3 months after injection [86].
A case series study described the outcome of PRP injection in 19 POR patients undergoing double stimulation during the follicular and luteal phases. The intraovarian perfusion with 2 mL of PRP was conducted immediately after the first follicular puncture. One day after the first puncture and PRP injection, the second stimulation was initiated. The mean number of oocytes after PRP perfusion was higher than that before PRP (2.1 versus 0.64). Three pregnancies after spontaneous conception or intracytoplasmic sperm injection (ICSI) and three healthy living births were recorded in three cases [87].
Another case series study reported 311 women diagnosed with POI according to the criteria with oligo/amenorrhea for at least 4 months, an elevated serum FSH > 25 IU/l on two occasions 4 weeks apart, and onset before the age of 40 years. These patients were injected with 2–4 mL of autologous injection of PRP prepared from 20 mL of peripheral blood. Although the numbers of retrieved oocyte before and after PRP injection were not shown, PRP treatment increased antral follicle count (AFC) and AMH. There were 23 patients who achieved spontaneous pregnancies, leading to 16 live births. For patients attempting IVF, thirteen pregnancies and nine live births were recorded. In total, twenty-five (8.0%) women achieved live birth, while another 25 (8.0%) had cryopreserved embryos. Of note, the enrolled POI patients might be at an early stage, because the mean AMH level before PRP treatment was relatively high at 0.13 ± 0.16 ng/mL [88].
A case series study was conducted in four different groups of women. Each group reported on thirty patients with low prognostic infertile women including poor ovarian response (POR), POI, perimenopause, and menopause patients. Four ml of autologous PRP prepared from 30 mL of peripheral blood was administrated to each ovary. In POR women diagnosed by Bologna criteria [89], an evident amelioration on the hormonal profile, the number of retrieved oocytes, and the intracytoplasmic sperm injection (ICSI) cycle performance was noted. Fourteen participants achieved clinical pregnancies after ICSI cycles followed by twelve live births. Menstruation recovery as well as the significant improvement in levels of AMH, FSH, and AFC were observed in 18 out of 30 POI patients. Three POI participants achieved spontaneous conceptions and healthy live births. For perimenopausal participants, four women achieved natural conceptions, resulting eventually in three healthy live births. Regarding the menopausal participants, thirteen women (43.3%) had menstrual cycle restoration and FSH levels reduction. One participant achieved a live birth after conceiving naturally [90]. Since the mean AMH levels before PRP treatment in POI, perimenopausal, and menopausal participants were 0.18 ± 0.04, 0.96 ± 0.28, 0.13 ± 0.03 ng/mL, respectively, this study enrolled patients with a relatively high ovarian reserve as a menopausal state.
In a recently case series study, thirty-eight infertile women with low ovarian reserve and at least two unsuccessful IVF cycles received a PRP intraovarian injection through an ultrasound-guided procedure or a laparoscopic-assisted approach. There was a significant decline of FSH and LH levels after the procedure. Meanwhile, the level of AMH rose from 0.08 to 1.1 ng/mL. Four out of thirty-eight women conceived naturally and gave birth to healthy children. Twenty women underwent IVF with a successful retrieval of one to three eggs in fifteen of them. The embryos were transferred in the same menstrual cycle in eight participants. Another seven cases could achieve the frozen embryos for subsequent transfer because of the poor quality of endometrium or other reasons. After both fresh and frozen embryo transfers, there were two live healthy births and four ongoing pregnancies, leading to a 26% (10/38) of success rate of pregnancy in total patients after PRP treatment. Nevertheless, two case of genetic abnormalities in seven frozen nuclei were reported [91].
4.2. Comparative Studies
There have been two prospective controlled, non-randomized comparative studies presented the outcomes of intraovarian PRP injection (Table 3). The first one compared the live birth rate (LBR) between 20 poor responders injected with 3–5 mL autologous PRP under transvaginal ultrasound guidance and 20 control patients. Other basic characteristics such as age, body mass index, partner’s age, and baseline FSH were balanced in both groups, and multivariate analysis found no statistical difference in regard to all known confounders. In both groups, the same protocol of a low dose stimulation using GnRH antagonist was used after 61 ± 18 days at the time of PRP application. The result of baseline characteristics and the IVF outcome are summarized in Table 3. According to the result, a statistical significance in clinical pregnancies and LBR was not found [92]. Of note, the rates of clinical pregnancy and live birth were presented as mean ± standard deviation, and no information about the number of clinical or live birth cases and embryo transfer attempts in each patient was available in the original paper. The second study included 83 women low ovarian reserve. There were 46 women undergoing the PRP treatment; meanwhile, 37 women were allocated to the control group. The baseline FSH levels at day 3, AMH, and antral follicle count (AFC) in the PRP group and control group were not statistic different (13.6 versus 14.9, 0.62 versus 0.68, and 4 versus 5, respectively). The women in the PRP group were injected with 200 µL of PRP derived from 36 mL of peripheral blood into the cortex of each ovary under transvaginal ultrasound guidance. As their first menstrual restarted, these patients were consulted to undergo timed intercourse, IUI or IVF/ICSI. The result noted a remarkable amelioration in AMH and FSH levels as well as AFC during the first three months in the PRP group. In the participants undergoing IVF, the number of retrieved oocytes in the PRP group was statistically higher than the control group (five versus three), and there was no statistical difference in fertilization rate. Overall, rates of biochemical (26.1% versus 5.4%) and clinical pregnancy (23.9% versus 5.4%) in the PRP group were higher than those of the control group, while there was no difference in the rates of first trimester miscarriage and live birth between groups (Table 3) [93].
4.3. Clinical Practice and Future Perspective of Intraovarian PRP Injection
Overall, the published papers revealed that the intraovarian PRP injection (Figure 2) improved the ovarian function and provided better fertility outcome. However, the literature has many case reports treating patients with relatively high ovarian reserve, suggesting a potential of pregnancy without PRP intervention. In two prospective controlled, non-randomized comparative studies, there was no statistical difference of the LBR in patients treated with PRP relative to control group. In addition, based on the recent review, approximately 2.2 to 14.2% of POI women conceive without PRP treatment [94]. Furthermore, the publication bias needs to be considered due to the presence of negative reports on ovarian rejuvenation by PRP injection in the proceedings of some domestic and international congresses. Consequently, it is difficult to attribute the reported live births to the PRP, especially in the context of lacking randomized trial studies. Moreover, in a recently published study, there were two cases of genetic abnormalities after PRP treatment that need to be noted. From the biochemical view point, PRP could contain some growth factors to stimulate follicle growth, but those concentrations in PRP are different among patients [16], resulting in different activities of autologous PRP. The concentrations of bioactive factors in PRP are also various depending on the preparation methods and protocols [5,95]. Since the half-life of growth factors in PRP is very short, the duration of the PRP effect is limited. Therefore, other aspects of clinical practice such as the most appropriate amount of PRP and method of PRP preparation, as well as the duration of its effect, also need to be fully investigated.
5. Conclusions
In conclusion, published literature presented that PRP intraovarian infusion could be a beneficial add-on treatment in the reproductive field. However, the current understanding of the autologous PRP activities in the ovaries, as well as long-term effectiveness of this approach are at an incipient stage. The extension of this novel intervention in clinical practice requires more serious evaluations with better designed studies.
Funding
This research received no external funding.
Acknowledgments
We thank Aaron J.W. Hsueh (Stanford University School of Medicine, Stanford, CA, USA) for critical reading and editing of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Drake, P. Births: Final Data for 2016. Natl. Vital Stat. Rep. 2018, 67, 1–55. [Google Scholar]
- Mathews, T.J.; Hamilton, B.E. Mean Age of Mothers is on the Rise: United States, 2000–2014. NCHS Data Brief. 2016, 232, 1–8. [Google Scholar]
- Coulam, C.B.; Adamson, S.C.; Annegers, J.F. Incidence of premature ovarian failure. Obstet. Gynecol. 1986, 67, 604–606. [Google Scholar] [CrossRef]
- Lagergren, K.; Hammar, M.; Nedstrand, E.; Bladh, M.; Sydsjö, G. The prevalence of primary ovarian insufficiency in Sweden: A national register study. BMC Womens Health 2018, 18, 175. [Google Scholar] [CrossRef] [Green Version]
- Sundman, E.A.; Cole, B.J.; Fortier, L.A. Growth factor and catabolic cytokine concentrations are influenced by the cellular composition of platelet-rich plasma. Am. J. Sports Med. 2011, 39, 2135–2140. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant. Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikolidakis, D.; Jansen, J.A. The biology of platelet-rich plasma and its application in oral surgery: Literature review. Tissue Eng. Part B Rev. 2008, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Alsousou, J.; Ali, A.; Willett, K.; Harrison, P. The role of platelet-rich plasma in tissue regeneration. Platelets 2013, 24, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.T.; James, I.B.; Marra, K.G.; Rubin, J.P. The Effects of Platelet-Rich Plasma on Cell Proliferation and Adipogenic Potential of Adipose-Derived Stem Cells. Tissue Eng. Part A 2015, 21, 2714–2722. [Google Scholar] [CrossRef] [Green Version]
- Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Weir, A.; Verhaar, J.A.; Bierma-Zeinstra, S.M.; Maas, M.; Tol, J.L. Platelet-rich plasma injections in acute muscle injury. N. Engl. J. Med. 2014, 370, 2546–2547. [Google Scholar] [CrossRef]
- Leo, M.S.; Kumar, A.S.; Kirit, R.; Konathan, R.; Sivamani, R.K. Systematic review of the use of platelet-rich plasma in aesthetic dermatology. J. Cosmet. Dermatol. 2015, 14, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Li, J.; Chen, Y.; Wei, L.; Yang, X.; Shi, Y.; Liang, X. Autologous platelet-rich plasma promotes endometrial growth and improves pregnancy outcome during in vitro fertilization. Int. J. Clin. Exp. Med. 2015, 8, 1286–1290. [Google Scholar] [PubMed]
- Noh, K.C.; Liu, X.N.; Zhuan, Z.; Yang, C.J.; Kim, Y.T.; Lee, G.W.; Choi, K.H.; Kim, K.O. Leukocyte-Poor Platelet-Rich Plasma-Derived Growth Factors Enhance Human Fibroblast Proliferation In Vitro. Clin. Orthop. Surg. 2018, 10, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Dolegowska, B.; Banfi, G. Growth factor content in PRP and their applicability in medicine. J. Biol. Regul. Homeost. Agents 2012, 26, 3s–22s. [Google Scholar]
- Mussano, F.; Genova, T.; Munaron, L.; Petrillo, S.; Erovigni, F.; Carossa, S. Cytokine, chemokine, and growth factor profile of platelet-rich plasma. Platelets 2016, 27, 467–471. [Google Scholar] [CrossRef]
- Krüger, J.P.; Freymannx, U.; Vetterlein, S.; Neumann, K.; Endres, M.; Kaps, C. Bioactive factors in platelet-rich plasma obtained by apheresis. Transfus. Med. Hemother. 2013, 40, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Schär, M.O.; Diaz-Romero, J.; Kohl, S.; Zumstein, M.A.; Nesic, D. Platelet-rich concentrates differentially release growth factors and induce cell migration in vitro. Clin. Orthop. Relat. Res. 2015, 473, 1635–1643. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.L.; Xu, Y.R.; Yang, W.X.; Sun, Y. The role of FSH and TGF-β superfamily in follicle atresia. Aging 2018, 10, 305–321. [Google Scholar] [CrossRef]
- Coutts, S.M.; Childs, A.J.; Fulton, N.; Collins, C.; Bayne, R.A.; McNeilly, A.S.; Anderson, R.A. Activin signals via SMAD2/3 between germ and somatic cells in the human fetal ovary and regulates kit ligand expression. Dev. Biol. 2008, 314, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Durlinger, A.L.; Visser, J.A.; Themmen, A.P. Regulation of ovarian function: The role of anti-Müllerian hormone. Reproduction 2002, 124, 601–609. [Google Scholar] [CrossRef]
- Nilsson, E.E.; Skinner, M.K. Bone morphogenetic protein-4 acts as an ovarian follicle survival factor and promotes primordial follicle development. Biol. Reprod. 2003, 69, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Vitt, U.A.; Hsueh, A.J. Stage-dependent role of growth differentiation factor-9 in ovarian follicle development. Mol. Cell. Endocrinol. 2001, 183, 171–177. [Google Scholar] [CrossRef]
- Vitt, U.A.; Hayashi, M.; Klein, C.; Hsueh, A.J. Growth differentiation factor-9 stimulates proliferation but suppresses the follicle-stimulating hormone-induced differentiation of cultured granulosa cells from small antral and preovulatory rat follicles. Biol. Reprod. 2000, 62, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, J.; Albertini, D.F.; Nishimori, K.; Kumar, T.R.; Lu, N.; Matzuk, M.M. Growth differentiation factor-9 is required during early ovarian folliculogenesis. Nature 1996, 383, 531–535. [Google Scholar] [CrossRef]
- Otsuka, F.; McTavish, K.J.; Shimasaki, S. Integral role of GDF-9 and BMP-15 in ovarian function. Mol. Reprod. Dev. 2011, 78, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orisaka, M.; Orisaka, S.; Jiang, J.Y.; Craig, J.; Wang, Y.; Kotsuji, F.; Tsang, B.K. Growth differentiation factor 9 is antiapoptotic during follicular development from preantral to early antral stage. Mol. Endocrinol. 2006, 20, 2456–2468. [Google Scholar] [CrossRef] [Green Version]
- Sanfins, A.; Rodrigues, P.; Albertini, D.F. GDF-9 and BMP-15 direct the follicle symphony. J. Assist. Reprod. Genet. 2018, 35, 1741–1750. [Google Scholar] [CrossRef]
- Gode, F.; Gulekli, B.; Dogan, E.; Korhan, P.; Dogan, S.; Bige, O.; Cimrin, D.; Atabey, N. Influence of follicular fluid GDF9 and BMP15 on embryo quality. Fertil. Steril. 2011, 95, 2274–2278. [Google Scholar] [CrossRef]
- Knight, P.G.; Glister, C. TGF-beta superfamily members and ovarian follicle development. Reproduction 2006, 132, 191–206. [Google Scholar] [CrossRef] [Green Version]
- Findlay, J.K.; Drummond, A.E.; Dyson, M.; Baillie, A.J.; Robertson, D.M.; Ethier, J.F. Production and actions of inhibin and activin during folliculogenesis in the rat. Mol. Cell. Endocrinol. 2001, 180, 139–144. [Google Scholar] [CrossRef]
- Namwanje, M.; Brown, C.W. Activins and Inhibins: Roles in Development, Physiology, and Disease. Cold Spring Harb. Perspect. Biol. 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Quezada, M.; Wang, J.; Hoang, V.; McGee, E.A. Smad7 is a transforming growth factor-beta-inducible mediator of apoptosis in granulosa cells. Fertil. Steril. 2012, 97, 1452–1459.e6. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Zhang, Y.L.; Fan, H.Y. Selective Smad4 knockout in ovarian preovulatory follicles results in multiple defects in ovulation. Mol. Endocrinol. 2013, 27, 966–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, E.; Parrott, J.A.; Skinner, M.K. Basic fibroblast growth factor induces primordial follicle development and initiates folliculogenesis. Mol. Cell. Endocrinol. 2001, 175, 123–130. [Google Scholar] [CrossRef]
- Guglielmo, M.C.; Ricci, G.; Catizone, A.; Barberi, M.; Galdieri, M.; Stefanini, M.; Canipari, R. The effect of hepatocyte growth factor on the initial stages of mouse follicle development. J. Cell. Physiol. 2011, 226, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Thuwanut, P.; Comizzoli, P.; Wildt, D.E.; Keefer, C.L.; Songsasen, N. Stem cell factor promotes in vitro ovarian follicle development in the domestic cat by upregulating c-kit mRNA expression and stimulating the phosphatidylinositol 3-kinase/AKT pathway. Reprod. Fertil. Dev. 2017, 29, 1356–1368. [Google Scholar] [CrossRef]
- Liu, K.; Rajareddy, S.; Liu, L.; Jagarlamudi, K.; Boman, K.; Selstam, G.; Reddy, P. Control of mammalian oocyte growth and early follicular development by the oocyte PI3 kinase pathway: New roles for an old timer. Dev. Biol. 2006, 299, 1–11. [Google Scholar] [CrossRef]
- Passos, J.R.; Costa, J.J.; da Cunha, E.V.; Silva, A.W.; Ribeiro, R.P.; de Souza, G.B.; Barroso, P.A.; Dau, A.M.; Saraiva, M.V.; Gonçalves, P.B.; et al. Protein and messenger RNA expression of interleukin 1 system members in bovine ovarian follicles and effects of interleukin 1β on primordial follicle activation and survival in vitro. Domest. Anim. Endocrinol. 2016, 54, 48–59. [Google Scholar] [CrossRef]
- Nagashima, T.; Kim, J.; Li, Q.; Lydon, J.P.; DeMayo, F.J.; Lyons, K.M.; Matzuk, M.M. Connective tissue growth factor is required for normal follicle development and ovulation. Mol. Endocrinol. 2011, 25, 1740–1759. [Google Scholar] [CrossRef] [Green Version]
- Schindler, R.; Nilsson, E.; Skinner, M.K. Induction of ovarian primordial follicle assembly by connective tissue growth factor CTGF. PLoS ONE 2010, 5, e12979. [Google Scholar] [CrossRef] [Green Version]
- Harlow, C.R.; Hillier, S.G. Connective tissue growth factor in the ovarian paracrine system. Mol. Cell. Endocrinol. 2002, 187, 23–27. [Google Scholar] [CrossRef]
- Hsueh, A.J.; Kawamura, K.; Cheng, Y.; Fauser, B.C. Intraovarian control of early folliculogenesis. Endocr. Rev. 2015, 36, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamura, K.; Kawamura, N.; Mulders, S.M.; Sollewijn Gelpke, M.D.; Hsueh, A.J. Ovarian brain-derived neurotrophic factor (BDNF) promotes the development of oocytes into preimplantation embryos. Proc. Natl. Acad. Sci. USA 2005, 102, 9206–9211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.M.; Wu, H.C.; Sun, Z.G.; Lian, F.; Leung, P.C.K. Neurotrophins and glial cell line-derived neurotrophic factor in the ovary: Physiological and pathophysiological implications. Hum. Reprod. Update 2019, 25, 224–242. [Google Scholar] [CrossRef]
- Cui, L.; Fang, L.; Mao, X.; Chang, H.M.; Leung, P.C.K.; Ye, Y. GDNF-Induced Downregulation of miR-145-5p Enhances Human Oocyte Maturation and Cumulus Cell Viability. J. Clin. Endocrinol. Metab. 2018, 103, 2510–2521. [Google Scholar] [CrossRef]
- Pinkas, H.; Fisch, B.; Rozansky, G.; Felz, C.; Kessler-Icekson, G.; Krissi, H.; Nitke, S.; Ao, A.; Abir, R. Platelet-derived growth factors (PDGF-A and -B) and their receptors in human fetal and adult ovaries. Mol. Hum. Reprod. 2008, 14, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.O.; Trau, H.A.; Duffy, D.M. Vascular endothelial growth factors C and D may promote angiogenesis in the primate ovulatory follicle. Biol. Reprod. 2017, 96, 389–400. [Google Scholar] [CrossRef] [Green Version]
- Li, S.H.; Hwu, Y.M.; Lu, C.H.; Chang, H.H.; Hsieh, C.E.; Lee, R.K. VEGF and FGF2 Improve Revascularization, Survival, and Oocyte Quality of Cryopreserved, Subcutaneously-Transplanted Mouse Ovarian Tissues. Int. J. Mol. Sci. 2016, 17, 1237. [Google Scholar] [CrossRef] [Green Version]
- Mattioli, M.; Barboni, B.; Turriani, M.; Galeati, G.; Zannoni, A.; Castellani, G.; Berardinelli, P.; Scapolo, P.A. Follicle activation involves vascular endothelial growth factor production and increased blood vessel extension. Biol. Reprod. 2001, 65, 1014–1019. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, S.; Konishi, I.; Tsuruta, Y.; Nanbu, K.; Mandai, M.; Kuroda, H.; Matsushita, K.; Hamid, A.A.; Yura, Y.; Mori, T. Expression of vascular endothelial growth factor (VEGF) during folliculogenesis and corpus luteum formation in the human ovary. Gynecol. Endocrinol. 1997, 11, 371–381. [Google Scholar] [CrossRef]
- Fraser, H.M. Regulation of the ovarian follicular vasculature. Reprod. Biol. Endocrinol. 2006, 4, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plendl, J. Angiogenesis and vascular regression in the ovary. Anat. Histol. Embryol. 2000, 29, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Kumar, T.R.; Matzuk, M.M.; Bondy, C. Insulin-like growth factor I regulates gonadotropin responsiveness in the murine ovary. Mol. Endocrinol. 1997, 11, 1924–1933. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Baumgarten, S.C.; Wu, Y.; Bennett, J.; Winston, N.; Hirshfeld-Cytron, J.; Stocco, C. IGF-I signaling is essential for FSH stimulation of AKT and steroidogenic genes in granulosa cells. Mol. Endocrinol. 2013, 27, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, S.C.; Armouti, M.; Ko, C.; Stocco, C. IGF1R Expression in Ovarian Granulosa Cells Is Essential for Steroidogenesis, Follicle Survival, and Fertility in Female Mice. Endocrinology 2017, 158, 2309–2318. [Google Scholar] [CrossRef] [Green Version]
- Serafim, M.K.; Duarte, A.B.; Silva, G.M.; Souza, C.E.; Magalhães-Padilha, D.M.; Moura, A.A.; Silva, L.D.; Campello, C.C.; Figueiredo, J.R. Impact of growth hormone (GH) and follicle stimulating hormone (FSH) on in vitro canine preantral follicle development and estradiol production. Growth Horm. IGF Res. 2015, 25, 85–89. [Google Scholar] [CrossRef]
- Wang, H.; Wen, Y.; Polan, M.L.; Boostanfar, R.; Feinman, M.; Behr, B. Exogenous granulocyte-macrophage colony-stimulating factor promotes follicular development in the newborn rat in vivo. Hum. Reprod. 2005, 20, 2749–2756. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Harada, T.; Tanikawa, M.; Fujii, A.; Shiota, G.; Terakawa, N. Hepatocyte growth factor and stem cell factor involvement in paracrine interplays of theca and granulosa cells in the human ovary. Fertil. Steril. 2001, 75, 973–979. [Google Scholar] [CrossRef]
- Baskind, N.E.; Orsi, N.M.; Sharma, V. Follicular-phase ovarian follicular fluid and plasma cytokine profiling of natural cycle in vitro fertilization patients. Fertil. Steril. 2014, 102, 410–418. [Google Scholar] [CrossRef]
- Richani, D.; Gilchrist, R.B. The epidermal growth factor network: Role in oocyte growth, maturation and developmental competence. Hum. Reprod. Update 2018, 24, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Peralta, O.A.; Bucher, D.; Fernandez, A.; Berland, M.; Strobel, P.; Ramirez, A.; Ratto, M.H.; Concha, I. Granulocyte-macrophage colony stimulating factor (GM-CSF) enhances cumulus cell expansion in bovine oocytes. Reprod. Biol. Endocrinol. 2013, 11, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmassi, A.; Schmutzler, A.G.; Huang, L.; Hedderich, J.; Jonat, W.; Mettler, L. Detection of granulocyte colony-stimulating factor and its receptor in human follicular luteinized granulosa cells. Fertil. Steril. 2004, 81 (Suppl. 1), 786–791. [Google Scholar] [CrossRef] [PubMed]
- Yanagi, K.; Makinoda, S.; Fujii, R.; Miyazaki, S.; Fujita, S.; Tomizawa, H.; Yoshida, K.; Iura, T.; Takegami, T.; Nojima, T. Cyclic changes of granulocyte colony-stimulating factor (G-CSF) mRNA in the human follicle during the normal menstrual cycle and immunolocalization of G-CSF protein. Hum. Reprod. 2002, 17, 3046–3052. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Jeon, Y.; Yoon, J.D.; Hwang, S.U.; Kim, E.; Park, K.M.; Kim, K.J.; Jin, M.H.; Lee, E.; Kim, H.; et al. The effects of human recombinant granulocyte-colony stimulating factor treatment during in vitro maturation of porcine oocyte on subsequent embryonic development. Theriogenology 2015, 84, 1075–1087. [Google Scholar] [CrossRef]
- Check, J.H.; Vaniver, J.; Senft, D.; DiAntonio, G.; Summers, D. The use of granulocyte colony stimulating factor to enhance oocyte release in women with the luteinized unruptured follicle syndrome. Clin. Exp. Obstet. Gynecol. 2016, 43, 178–180. [Google Scholar] [CrossRef]
- Hou, H.Y.; Wang, X.; Yu, Q.; Li, H.Y.; Li, S.J.; Tang, R.Y.; Guo, Z.X.; Chen, Y.Q.; Hu, C.X.; Yang, Z.J.; et al. Evidence that growth hormone can improve mitochondrial function in oocytes from aged mice. Reproduction 2018, 157, 345–358. [Google Scholar] [CrossRef]
- Dehghani, F.; Aboutalebi, H.; Esmaeilpour, T.; Panjehshahin, M.R.; Bordbar, H. Effect of platelet-rich plasma (PRP) on ovarian structures in cyclophosphamide-induced ovarian failure in female rats: A stereological study. Toxicol. Mech. Methods 2018, 28, 653–659. [Google Scholar] [CrossRef]
- Ahmadian, S.; Sheshpari, S.; Pazhang, M.; Bedate, A.M.; Beheshti, R.; Abbasi, M.M.; Nouri, M.; Rahbarghazi, R.; Mahdipour, M. Intra-ovarian injection of platelet-rich plasma into ovarian tissue promoted rejuvenation in the rat model of premature ovarian insufficiency and restored ovulation rate via angiogenesis modulation. Reprod. Biol. Endocrinol. 2020, 18, 78. [Google Scholar] [CrossRef]
- Cremonesi, F.; Bonfanti, S.; Idda, A.; Lange-Consiglio, A. Platelet Rich Plasma for Regenerative Medicine Treatment of Bovine Ovarian Hypofunction. Front. Vet. Sci. 2020, 7, 517. [Google Scholar] [CrossRef]
- Cremonesi, F.; Bonfanti, S.; Idda, A.; Anna, L.C. Improvement of Embryo Recovery in Holstein Cows Treated by Intra-Ovarian Platelet Rich Plasma before Superovulation. Vet. Sci. 2020, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, L.; Shirazi, A.; Naderi, M.M.; Shams-Esfandabadi, N.; Borjian Boroujeni, S.; Sarvari, A.; Sadeghnia, S.; Behzadi, B.; Akhondi, M.M. Platelet-rich plasma promotes the development of isolated human primordial and primary follicles to the preantral stage. Reprod. Biomed. Online 2017, 35, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younis, J.S.; Haddad, S.; Matilsky, M.; Radin, O.; Ben-Ami, M. Undetectable basal ovarian stromal blood flow in infertile women is related to low ovarian reserve. Gynecol. Endocrinol. 2007, 23, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Fenton, A.J. Premature ovarian insufficiency: Pathogenesis and management. J. Midlife Health 2015, 6, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Oh, D.S.; Jeong, J.H.; Shin, B.S.; Joo, B.S.; Lee, K.S. Follicular blood flow is a better predictor of the outcome of in vitro fertilization-embryo transfer than follicular fluid vascular endothelial growth factor and nitric oxide concentrations. Fertil. Steril. 2004, 82, 586–592. [Google Scholar] [CrossRef]
- Wood, S.H.; Sills, E.S. Intraovarian vascular enhancement via stromal injection of platelet-derived growth factors: Exploring subsequent oocyte chromosomal status and in vitro fertilization outcomes. Clin. Exp. Reprod. Med. 2020, 47, 94–100. [Google Scholar] [CrossRef]
- Etulain, J.; Mena, H.A.; Meiss, R.P.; Frechtel, G.; Gutt, S.; Negrotto, S.; Schattner, M. An optimised protocol for platelet-rich plasma preparation to improve its angiogenic and regenerative properties. Sci. Rep. 2018, 8, 1513. [Google Scholar] [CrossRef]
- Samadi, P.; Sheykhhasan, M.; Khoshinani, H.M. The Use of Platelet-Rich Plasma in Aesthetic and Regenerative Medicine: A Comprehensive Review. Aesthetic Plast. Surg. 2019, 43, 803–814. [Google Scholar] [CrossRef]
- Mohamadi, S.; Norooznezhad, A.H.; Mostafaei, S.; Nikbakht, M.; Nassiri, S.; Safar, H.; Moghaddam, K.A.; Ghavamzadeh, A.; Kazemnejad, A. A randomized controlled trial of effectiveness of platelet-rich plasma gel and regular dressing on wound healing time in pilonidal sinus surgery: Role of different affecting factors. Biomed. J. 2019, 42, 403–410. [Google Scholar] [CrossRef]
- Bakacak, M.; Bostanci, M.S.; İnanc, F.; Yaylali, A.; Serin, S.; Attar, R.; Yildirim, G.; Yildirim, O.K. Protective Effect of Platelet Rich Plasma on Experimental Ischemia/Reperfusion Injury in Rat Ovary. Gynecol. Obstet. Investig. 2016, 81, 225–231. [Google Scholar] [CrossRef]
- Callejo, J.; Salvador, C.; González-Nuñez, S.; Almeida, L.; Rodriguez, L.; Marqués, L.; Valls, A.; Lailla, J.M. Live birth in a woman without ovaries after autograft of frozen-thawed ovarian tissue combined with growth factors. J. Ovarian Res. 2013, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Nitsos, N.; Rapani, A.; Pappas, A.; Pantou, A.; Chronopoulou, M.; Deligeoroglou, E.; Koutsilieris, M.; Pantos, K. Autologous Platelet-Rich Plasma Treatment Enables Pregnancy for a Woman in Premature Menopause. J. Clin. Med. 2018, 8, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.C.; Hsu, L.; Hsu, I.; Chiu, Y.J.; Dorjee, S. Live Birth in Woman With Premature Ovarian Insufficiency Receiving Ovarian Administration of Platelet-Rich Plasma (PRP) in Combination With Gonadotropin: A Case Report. Front. Endocrinol. (Lausanne) 2020, 11, 50. [Google Scholar] [CrossRef] [PubMed]
- Pantos, K.; Nitsos, N.; Kokkali, G.; Vaxevanoglou, T.; Markomichali, C.; Pantou, A.; Grammatis, M.; Lazaros, L.; Sfakianoudis, K. Ovarian rejuvenation and folliculogenesis reactivation in peri-menopausal women after autologous platelet-rich plasma treatment. In Proceedings of the ESHRE 32nd Annual Meeting, Helsinki, Finland, 3–6 July 2016. [Google Scholar]
- Sills, E.S.; Rickers, N.S.; Li, X.; Palermo, G.D. First data on in vitro fertilization and blastocyst formation after intraovarian injection of calcium gluconate-activated autologous platelet rich plasma. Gynecol. Endocrinol. 2018, 34, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Pantos, K.; Simopoulou, M.; Pantou, A.; Rapani, A.; Tsioulou, P.; Nitsos, N.; Syrkos, S.; Pappas, A.; Koutsilieris, M.; Sfakianoudis, K. A Case Series on Natural Conceptions Resulting in Ongoing Pregnancies in Menopausal and Prematurely Menopausal Women Following Platelet-Rich Plasma Treatment. Cell Transplant. 2019, 28, 1333–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Nitsos, N.; Rapani, A.; Pantou, A.; Vaxevanoglou, T.; Kokkali, G.; Koutsilieris, M.; Pantos, K. A Case Series on Platelet-Rich Plasma Revolutionary Management of Poor Responder Patients. Gynecol. Obstet. Investig. 2019, 84, 99–106. [Google Scholar] [CrossRef]
- Farimani, M.; Heshmati, S.; Poorolajal, J.; Bahmanzadeh, M. A report on three live births in women with poor ovarian response following intra-ovarian injection of platelet-rich plasma (PRP). Mol. Biol. Rep. 2019, 46, 1611–1616. [Google Scholar] [CrossRef]
- Cakiroglu, Y.; Saltik, A.; Yuceturk, A.; Karaosmanoglu, O.; Kopuk, S.Y.; Scott, R.T.; Tiras, B.; Seli, E. Effects of intraovarian injection of autologous platelet rich plasma on ovarian reserve and IVF outcome parameters in women with primary ovarian insufficiency. Aging 2020, 12, 10211–10222. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Grigoriadis, S.; Pantou, A.; Tsioulou, P.; Maziotis, E.; Rapani, A.; Giannelou, P.; Nitsos, N.; Kokkali, G.; et al. Reactivating Ovarian Function through Autologous Platelet-Rich Plasma Intraovarian Infusion: Pilot Data on Premature Ovarian Insufficiency, Perimenopausal, Menopausal, and Poor Responder Women. J. Clin. Med. 2020, 9, 1809. [Google Scholar] [CrossRef]
- Petryk, N.; Petryk, M. Ovarian Rejuvenation Through Platelet-Rich Autologous Plasma (PRP)-a Chance to Have a Baby Without Donor Eggs, Improving the Life Quality of Women Suffering from Early Menopause Without Synthetic Hormonal Treatment. Reprod. Sci. 2020, 27, 1975–1982. [Google Scholar] [CrossRef]
- Stojkovska, S.; Dimitrov, G.; Stamenkovska, N.; Hadzi-Lega, M.; Petanovski, Z. Live Birth Rates in Poor Responders’ Group after Previous Treatment with Autologous Platelet-Rich Plasma and Low Dose Ovarian Stimulation Compared with Poor Responders Used Only Low Dose Ovarian Stimulation Before in Vitro Fertilization. J. Med. Sci. 2019, 7, 3184–3188. [Google Scholar] [CrossRef] [Green Version]
- Melo, P.; Navarro, C.; Jones, C.; Coward, K.; Coleman, L. The use of autologous platelet-rich plasma (PRP) versus no intervention in women with low ovarian reserve undergoing fertility treatment: A non-randomized interventional study. J. Assist. Reprod. Genet. 2020, 37, 855–863. [Google Scholar] [CrossRef]
- Fraison, E.; Crawford, G.; Casper, G.; Harris, V.; Ledger, W. Pregnancy following diagnosis of premature ovarian insufficiency: A systematic review. Reprod. Biomed. Online 2019, 39, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Fadadu, P.P.; Mazzola, A.J.; Hunter, C.W.; Davis, T.T. Review of concentration yields in commercially available platelet-rich plasma (PRP) systems: A call for PRP standardization. Reg. Anesth. Pain Med. 2019. [Google Scholar] [CrossRef]
Figure 1.
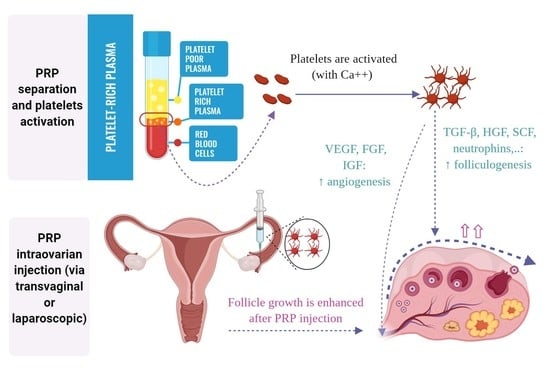
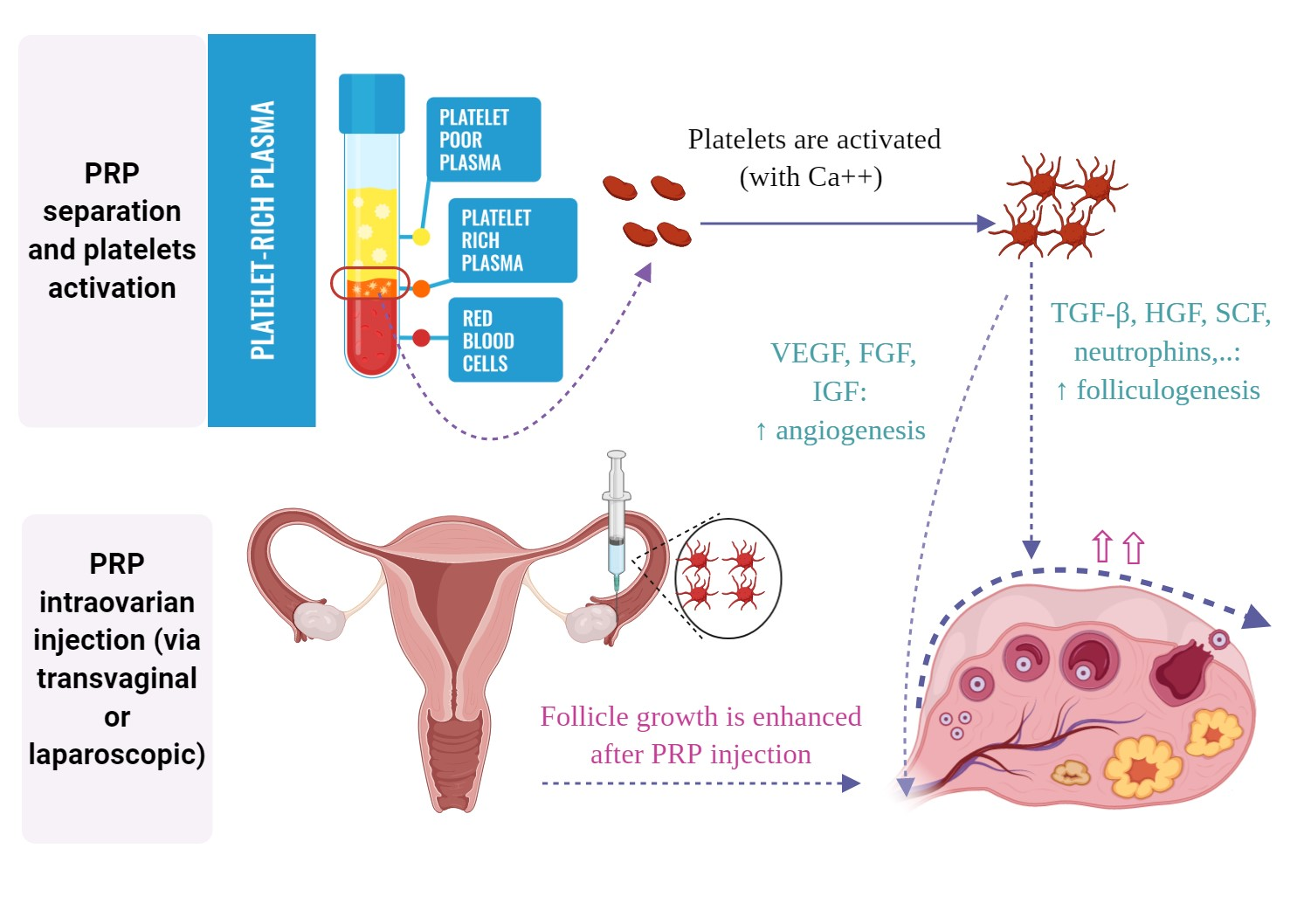
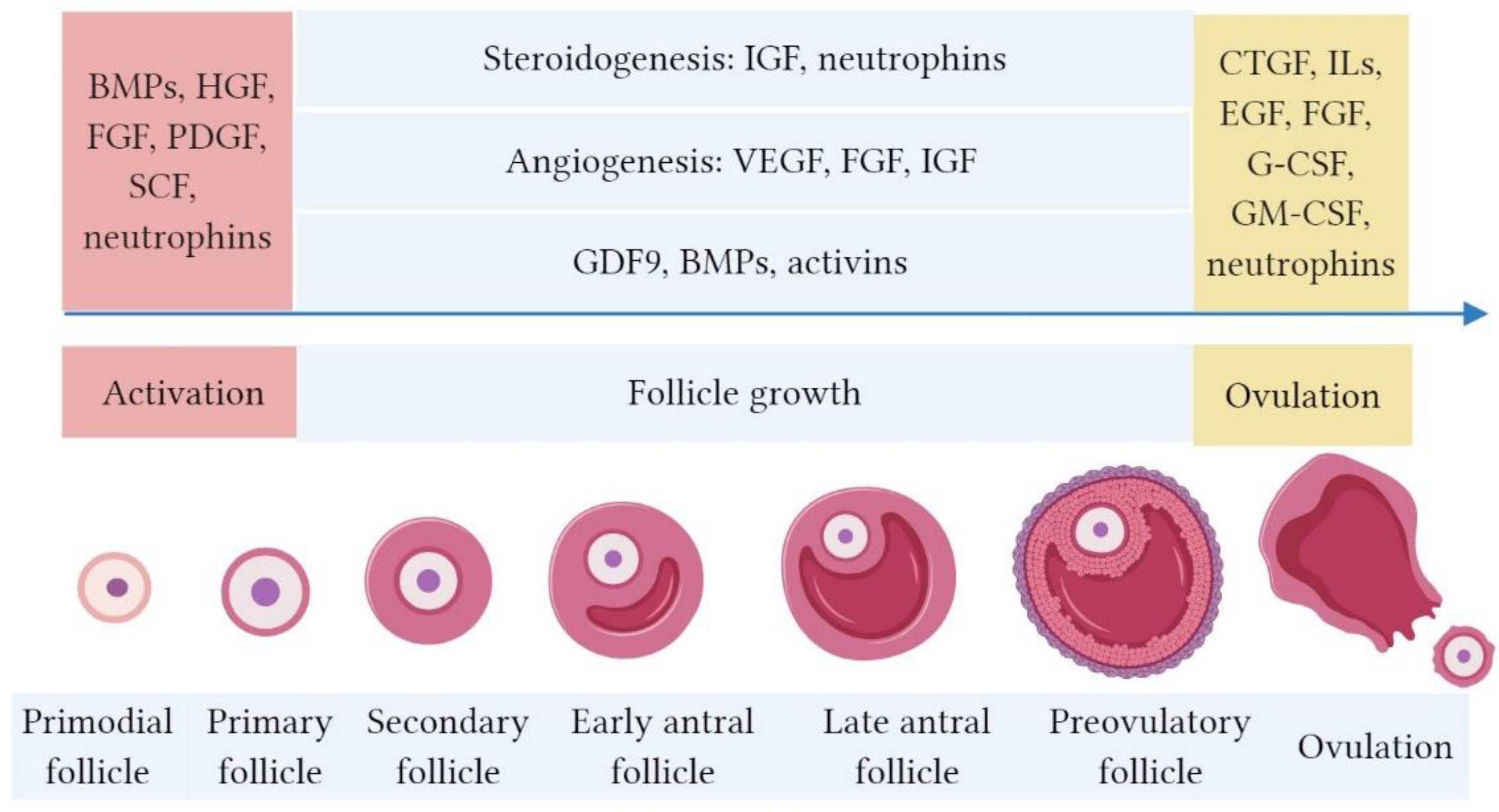
The roles of growth factors involving in PRP in folliculogenesis. At the early stage of folliculogenesis, the activation of primordial follicle is stimulated by bone morphogenetic proteins (BMPs), platelet-derived growth factor (PDGF), hepatocyte growth factor (HGF), fibroblast growth factor (FGF), stem cell factor (SCF) and neutrophins. Growth and differentiation factor (GDF)9, BMPs, and activins regulate the follicle growth from primary to antral stages. During folliculogenesis, neovascularization is enhanced by vascular endothelial growth factor (VEGF), FGF, and insulin-like growth factor (IGF), whereas steroidogenesis is modulated by IGF and neutrophins. Other several factors including connective tissue growth factor (CTGF), interleukins, epidermal growth factor (EGF), FGF, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), and neutrophins assist ovulation.
Figure 1.
The roles of growth factors involving in PRP in folliculogenesis. At the early stage of folliculogenesis, the activation of primordial follicle is stimulated by bone morphogenetic proteins (BMPs), platelet-derived growth factor (PDGF), hepatocyte growth factor (HGF), fibroblast growth factor (FGF), stem cell factor (SCF) and neutrophins. Growth and differentiation factor (GDF)9, BMPs, and activins regulate the follicle growth from primary to antral stages. During folliculogenesis, neovascularization is enhanced by vascular endothelial growth factor (VEGF), FGF, and insulin-like growth factor (IGF), whereas steroidogenesis is modulated by IGF and neutrophins. Other several factors including connective tissue growth factor (CTGF), interleukins, epidermal growth factor (EGF), FGF, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), and neutrophins assist ovulation.

Figure 2.
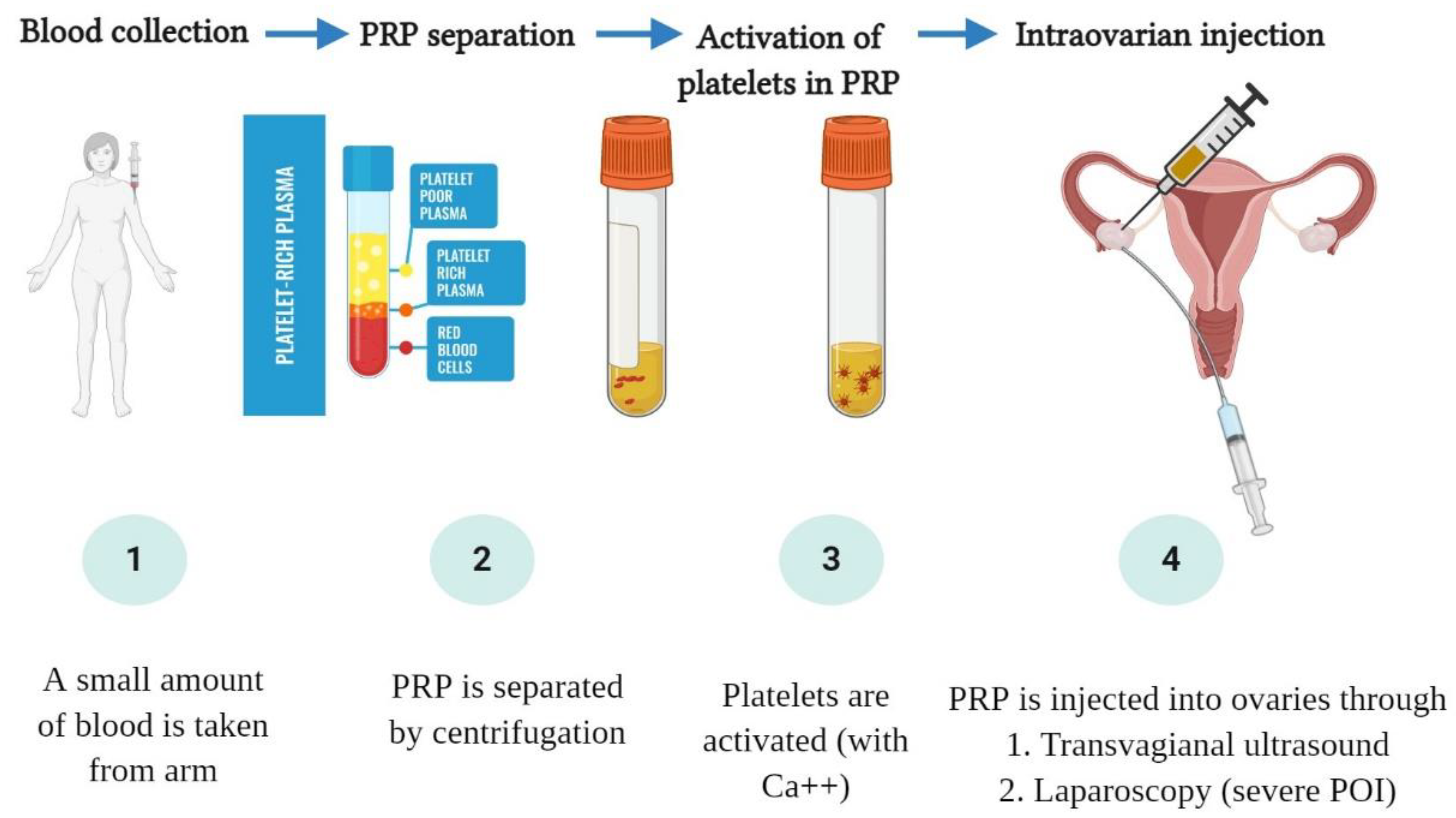
The procedure of PRP preparation and intraovarian injection. Firstly, peripheral blood is harvested from an arm of the patient. The collected blood is centrifugated to separate the PRP. Then, the platelets in PRP are activated for releasing the growth factors. The intraovarian PRP injection is usually conducted under transvaginal ultrasound, whereas the laparoscopic approach is required in severe cases of POI due to difficult detection of ovaries without growing follicles under ultrasound.
Figure 2.
The procedure of PRP preparation and intraovarian injection. Firstly, peripheral blood is harvested from an arm of the patient. The collected blood is centrifugated to separate the PRP. Then, the platelets in PRP are activated for releasing the growth factors. The intraovarian PRP injection is usually conducted under transvaginal ultrasound, whereas the laparoscopic approach is required in severe cases of POI due to difficult detection of ovaries without growing follicles under ultrasound.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Growth factors in platelet-rich plasma (PRP) and their role in folliculogenesis.
| Growth Factors | Roles in Folliculogenesis | References |
|---|---|---|
| Activins | Primordial follicle formation | [19] |
| BDNF | Primordial follicle activation, follicular growth, ovulation | [43,44,45] |
| BMPs | Follicular growth, preantral follicle maintenance, COC expansion | [18,20,21,27] |
| CTGF | Primordial follicle assembly, ovulation | [39,40,41] |
| EGF | COC expansion | [60] |
| FGF | Primordial follicle activation | [34] |
| G-CSF | Ovulation | [62,63,64,65] |
| GDF | Follicles growth after the primary stage, FSH expression | [18,22,23,24,25,26,27] |
| GH | Steroidogenesis in granulosa cells, mitochondrial function | [56,66] |
| GM-CSF | Follicles growth, COC expansion | [57,61] |
| GDNF | Primordial follicle activation, follicular growth, ovulation | [44] |
| HGF | Primordial follicle activation | [35] |
| IGF | Steroidogenesis in granulosa cells | [53,54,55] |
| IL-1 β | Primordial follicle development, ovulation | [38,59] |
| NT-3 | Primordial follicle activation, follicular growth, ovulation | [44] |
| NT-4 | Primordial follicle activation, follicular growth, ovulation | [44] |
| PDGF | Primordial follicle activation | [46] |
| SCF | Primordial follicle activation | [36,37] |
| VEGF | Angiogenesis | [51] |
Table 2.
Summary of published clinical case studies of PRP.
| Authors | Enrolled Case Number | Age | PRP (ml) /Blood (ml)/Ovary * | Follow Up Duration (Months) | AMH (mIU/L) | FSH (mIU/L) | AFC (n) | Number of Oocytes ** | Pregnancy Outcome | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prior PRP | Post PRP | Prior PRP | Post PRP | Prior PRP | Post PRP | Prior PRP | Post PRP | Mode of Conception | ||||||
| Natural | IVF | |||||||||||||
| Sills E.S (2018) [84] | 4 | 42 ± 4 | 5/N/A | 5 | 0.38 | 0.61 | 13.6 | 7.7 | N/A *** | N/A | N/A | 4–7 | 0 | N/A |
| Sfakianoudis K. (2018) [81] | 1 | 40 | 4/30 | 2 | 0.02 | 0.08 | 149 | 27 | N/A | N/A | N/A | N/A | 0 | 1 |
| Pantos K. (2019) [85] | 3 | 46 40 27 (POI) | 4/30 4/30 4/30 | 1 3 5 | 0.16 0.06 0.17 | 0.22 0.2 0.3 | 119 65 46.5 | 27 10 15.1 | 0 0 0 | 4 2 1 | N/A N/A N/A | N/A N/A N/A | 1 1 1 | N/A N/A N/A |
| Sfakianoudis K. (2019) [86] | 3 | 40 37 37 | 5/35 5/35 5/35 | N/A N/A N/A | 0.65 0.54 0.44 | 1.1 0.93 0.81 | 27.8 18.3 24.1 | 11.1 4.1 8.6 | N/A N/A N/A | N/A N/A N/A | 0/4 10/12 2/4 | 5/6 2/2 2/4 | 000 | 111 |
| Farimani M. (2019) [87] | 19 | 35.57± 3.80 | 2/N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | 0.64 ± 0.92 | 2.1 ± 2.5 | 2 | 1 |
| Hsu C.C (2020) [82] | 1 | 37 | 3/20 | N/A | 0.02 | 63.65 | 17.84 | N/A | N/A | 0 | 6/2 | 0 | 1 | |
| Cakiroglu Y. (2020) [88] | 311 | 34.8 ± 4.3 | 2-4/20 | N/A | 0.13 ± 0.16 | 0.18 ± 0.18 | 41.9 ± 24.7 | 41.6 ± 24.7 | 0.5 ± 0.5 | 1.7 ± 1.4 | N/A | N/A | 23 | 13 |
| Sfakianoudis K. (2020) **** (POR) [90] | 30 | 38.40 ± 2.01 | 4/30 | 3 | 0.66 ± 0.20 | 1.14 ± 0.26 | 10.71 ± 1.62 | 8.95 ± 1.40 | 2.63 ± 0.93 | 5.20 ± 1.35 | 1.20 ± 0.76 | N/A | 0 | 14 |
| Petryk N. (2020) [91] | 38 | 31–45 | 0.7/8.5 | 12 | p < 0.05 | p < 0.05 | N/A | N/A | N/A | N/A | 4 | 6 | ||
* The volume of PRP and required peripheral blood for each ovary; ** The total number of oocytes/oocytes pick-up attempts; *** N/A: not applicable or available; **** Poor ovarian response (POR).
Table 3.
Characteristics and in vitro fertilization (IVF) outcome between groups in prospective controlled studies.
Table 3.
Characteristics and in vitro fertilization (IVF) outcome between groups in prospective controlled studies.
| Author | Characteristics | PRP Group | Without PRP Group | p Value |
|---|---|---|---|---|
| Stojkovska S. (2019) [92] | N = 20 | N = 20 | ||
| Age | 37.47 ± 3.87 | 37.64 ± 3.20 | 0.99 | |
| Baseline FSH (mIU/mL) | 19.27 ± 2.29 | 19.22 ± 4.05 | 0.97 | |
| Baseline AMH (ng/mL) | 0.35 ± 0.19 | 0.72 ± 0.42 | 0.03 | |
| Number of oocytes | 1.87 ± 1.13 | 3.71 ± 2.40 | 0.20 | |
| Fertilization rate (%) | 80.67 ± 25.42 | 65.60 ± 25.35 | 0.44 | |
| Implantation rate (%) | 33.33 ± 44.99 | 10.71 ± 28.95 | 0.70 | |
| Clinical pregnancy rate (%) | 33.33 ± 44.99 | 10.71 ± 28.95 | 0.69 | |
| Live birth rate (%) | 40.00 ± 50.71 | 14.29 ± 36.31 | 0.71 | |
| Melo P. (2020) [93] | N = 46 | N = 37 | ||
| Age | 41 (39–44) | 41 (39–44) | 0.78 | |
| Baseline FSH (mIU/mL) | 13.6 (12.9–17.5) | 14.9 (13.1–17.8) | 0.26 | |
| Post PRP FSH (mIU/mL) | 9.07 (8.3–10.5) | 15.0 (13.4–17.9) | N/A * | |
| Baseline AMH (ng/mL) | 0.62 (0.47–0.76) | 0.68 (0.41–0.78) | 0.65 | |
| Post PRP AMH (ng/mL) | 1.01 (0.9–1.3) | 0.58 (0.39–0.76) | N/A | |
| Oocyte number | 5.0 (2.0-9.0) | 3.0 (0.0-6.0) | <0.001 | |
| Biochemical pregnancy rate | 12/46 (26.1) | 2/37 (5.4) | 0.02 | |
| Clinical pregnancy rate | 11/46 (23.9) | 2/37 (5.4) | 0.03 | |
| 1st trimester miscarriages | 6/46 (13.0) ** | 1/37 (2.7) | 0.13 | |
| Live births | 4/46 (8.7) | 1/37 (2.7) | 0.38 |
* N/A: not available; ** Of the six participants who sustained a first trimester miscarriage, three had a history of previous miscarriage.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Vo, T.K.C.; Tanaka, Y.; Kawamura, K. Ovarian Rejuvenation Using Autologous Platelet-Rich Plasma. Endocrines 2021, 2, 15-27. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2010002
AMA Style
Vo TKC, Tanaka Y, Kawamura K. Ovarian Rejuvenation Using Autologous Platelet-Rich Plasma. Endocrines. 2021; 2(1):15-27. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2010002
Chicago/Turabian StyleVo, Tuyen Kim Cat, Yuka Tanaka, and Kazuhiro Kawamura. 2021. "Ovarian Rejuvenation Using Autologous Platelet-Rich Plasma" Endocrines 2, no. 1: 15-27. https://0-doi-org.brum.beds.ac.uk/10.3390/endocrines2010002