
Commercial Baby Foods Aimed at Children up to 36 Months: Are They a Matter of Concern?

 , ,
, ,  ,
,
Abstract
:1. Introduction
- (1)
- Agreement with the compositional criteria and labelling requirements of the Nutrient Profile Model (NPM) for commercial baby foods aimed at children up 36 months;
- (2)
- Level of processing as defined by the NOVA classification system.
2. Materials and Methods
2.1. Data Collection
2.2. Product Categorization
2.3. Nutritional Composition and Labelling Requirements Evaluation
2.4. CACFs Classification into Target Age Groups
2.5. Data Analysis
3. Results
3.1. General Characteristics
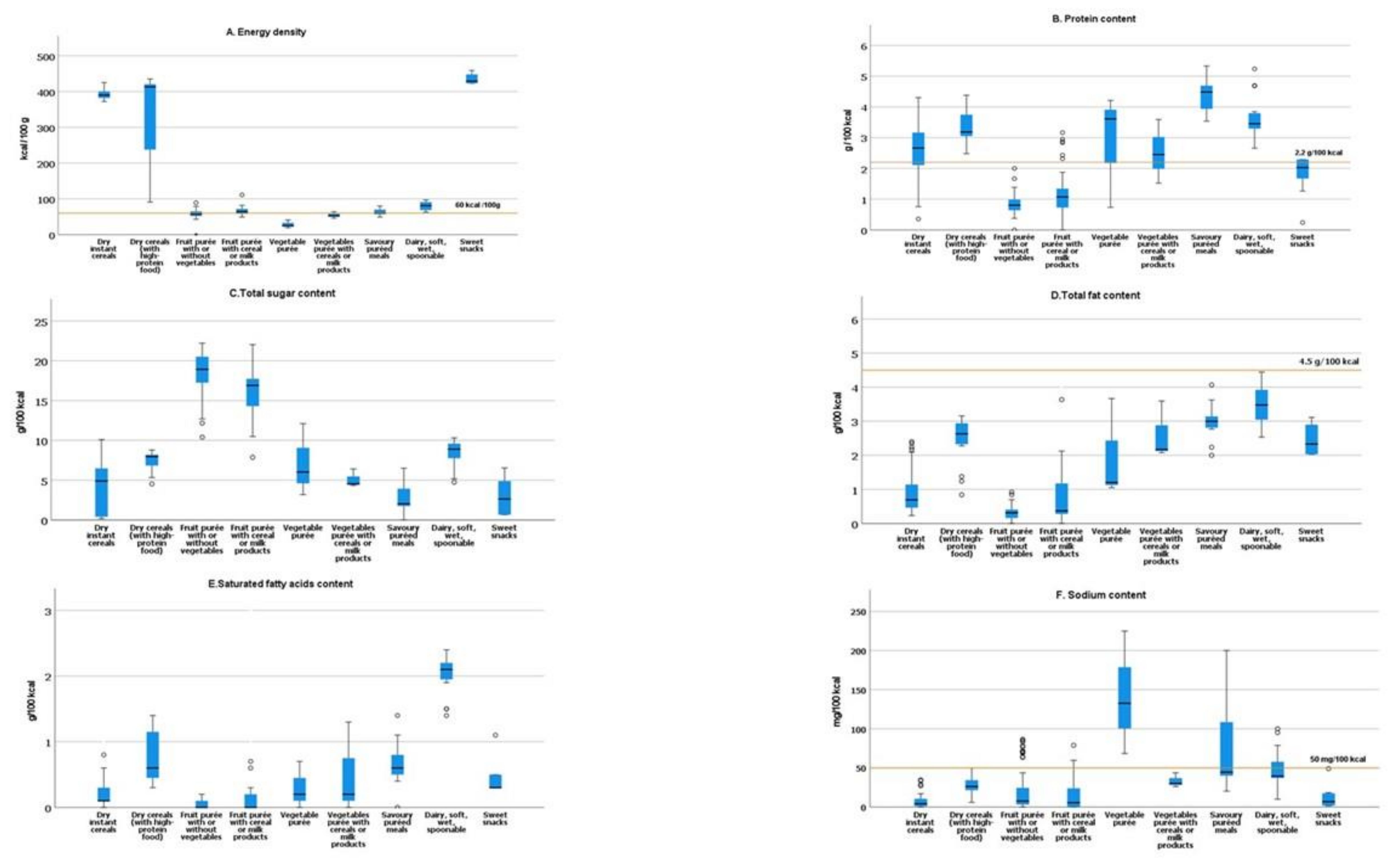
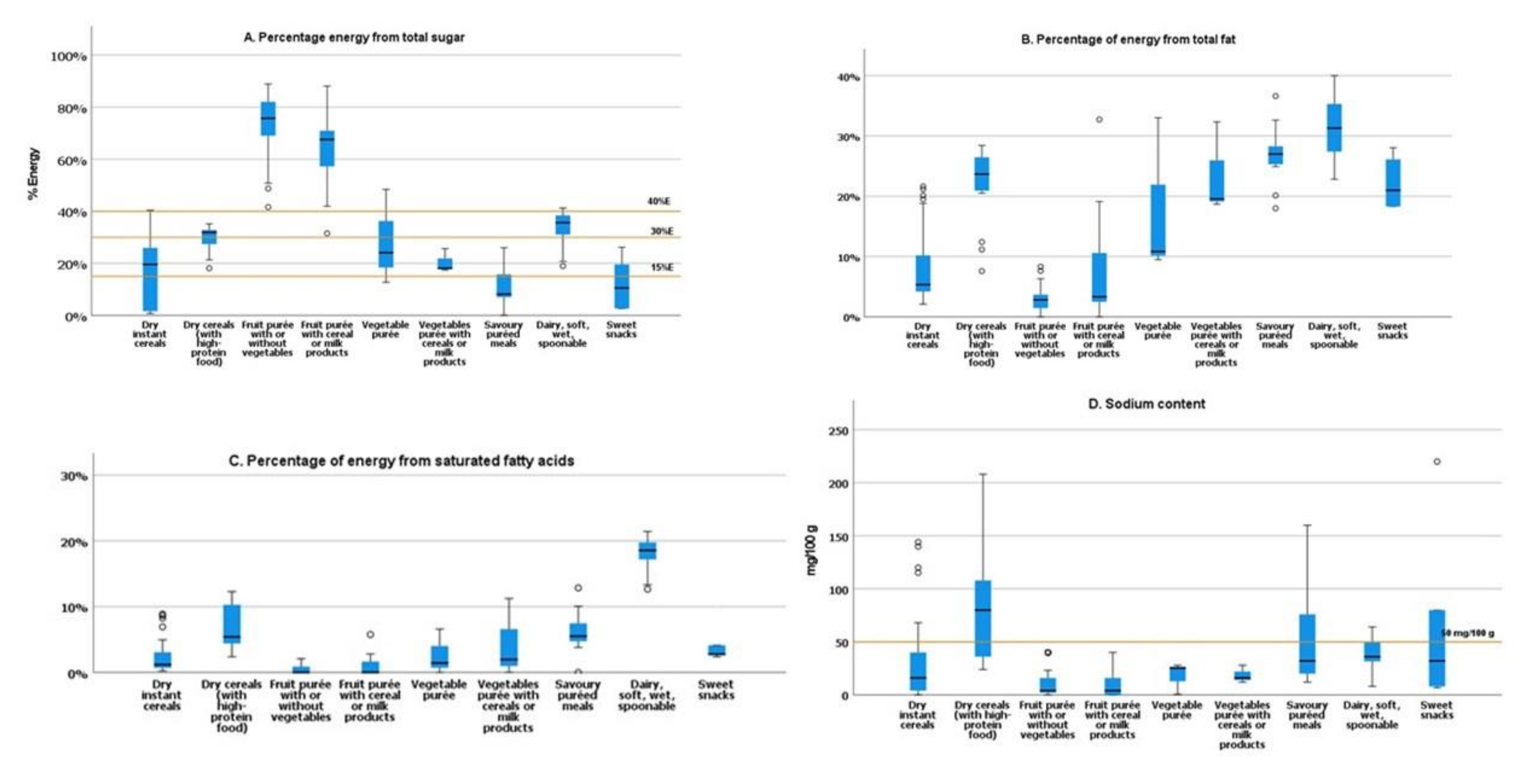
3.2. Nutritional Composition
3.3. Compliance with the NPM Criteria
3.3.1. Compositional Criteria
3.3.2. Labelling Requirements
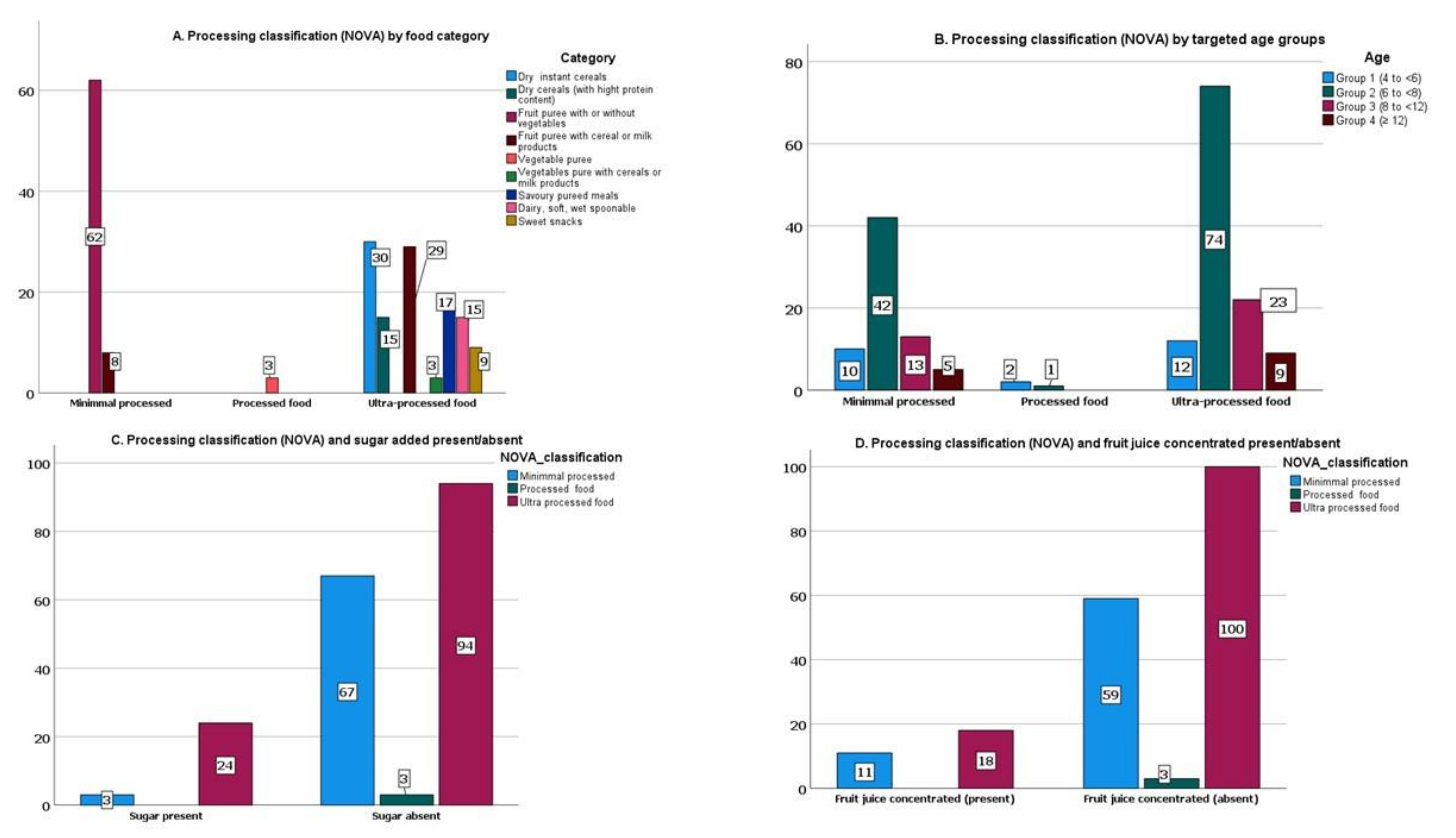
3.4. Processing Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coded Variables | Description |
|---|---|
| Basic information | Brand name, product name, food type, ingredients, recommend age, serving size |
| Product category | Products were classified according to the NPM proposed by WHO/Europe: Dry instant cereals; dry cereals (with high-protein food (added)-powder milk or whey); fruit purée (with/without vegetables); vegetable purées; fruit purée with cereal/milk; vegetables with cereal, soft, wet, spoonable; savoury puréed meals; dairy, soft, wet, spoonable; sweet snacks. |
| Nutritional information | Nutritional content (total energy (kJ/kcal), protein (g), carbohydrates (g), total sugars (g), fat (g), saturated fatty acids (g), and sodium (mg). All the nutritional analysis was per 100 g product. |
| Details on the presence of added sugars | For these analyses, added sugars were classified as fruit juice whether whole, concentrated, or powdered; sugar; sucrose; dextrose; fructose; maltose; any syrup; honey; barley malt/malted barley/malt extract; molasses; and artificial or natural zero/low-calorie sweeteners. |
| Composition, nutrition, and health claims | Composition claim: No added preservatives, organic food, egg-free, dairy-claims free, gluten-free. Nutrition claim: Contains calcium, contains iron, contains vitamin C, contains dietary fiber, contains multiple vitamins, no added sugar, no added salt, contains vitamin E, contains multiple minerals. Health claims: Provides good nutrition to children, nutritionally balanced, cognitive ability. |
| Visual information | Presence of cartoons, pictures of infants/young children, pictures of mothers, pictures of bottles/teats. |
References
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mennella, J.A. Development of food preferences: Lessons learned from longitudinal and experimental studies. Food Qual. Prefer. 2006, 17, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Optimal Duration of Exclusive Breastfeeding: Report of an Expert Consultation. Joint WHO/NHD Expert Consultation. In WHO Technical Report No. 01.09.; WHO: Geneva, Switzerland, 2002; Volume 65. [Google Scholar]
- World Health Organization; United Nations Children’s Fund (UNICEF). Global Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Maslin, K.; Venter, C. Nutritional aspects of commercially prepared infant foods in developed countries: A narrative review. Nutr. Res. Rev. 2017, 30, 138–148. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Resolution WHA69.9. Ending Inappropriate Promotion of Foods for Infants and Young Children, Proceedings of the Sixty-Ninth World Health Assembly, Geneva, Switzerland, 23–28 May 2016; WHO: Geneva, Switzerland, 2016; pp. 23–28.
- World Health Organization. Guidance on Ending the Inappropriate Promotion of Foods for Infants and Young Children: Implementation manual; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- WHO Regional Office for Europe. Ending Inappropriate Promotion of Commercially Available Complementary Foods for Infants and Young Children between 6 and 36 Months in Europe; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- European Commission. Commission Directive 2006/125/EC on processed cereal-based foods and baby foods for infants and young children. Off. J. Eur. Union 2006, 339, 16–35. [Google Scholar]
- UNICEF. The State of the World’s Children 2019. Children, Food and Nutrition. Growing Well in a Changing World; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- World Health Organization. Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015; Volume 57. [Google Scholar]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A review of total & added sugar intakes and dietary sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinho, A.R.; Severo, M.; Correia, D.; Lobato, L.; Vilela, S.; Oliveira, A.; Ramos, E.; Torres, D.; Lopes, C. Total, added and free sugar intakes, dietary sources and determinants of consumption in Portugal: The National Food, Nutrition and Physical Activity Survey (IAN-AF 2015-2016). Public Health Nutr. 2020, 23, 869–881. [Google Scholar] [CrossRef]
- Garcia, A.L.; McLean, K.; Wright, C.M. Types of fruits and vegetables used in commercial baby foods and their contribution to sugar content. Matern. Child Nutr. 2016, 12, 838–847. [Google Scholar] [CrossRef]
- Hutchinson, J.; Rippin, H.; Threapleton, D.; Jewell, J.; Kanamäe, H.; Salupuu, K.; Caroli, M.; Antignani, A.; Pace, L.; Vassallo, C.; et al. High sugar content of European commercial baby foods and proposed updates to existing recommendations. Matern. Child Nutr. 2020, 17, e13020. [Google Scholar] [CrossRef]
- Da Rocha, K.F.; De Araújo, C.R.B.; De Morais, I.L.; Padrão, P.; Moreira, P.; Ribeiro, K.D.D.S. Commercial foods for infants under the age of 36 months: An assessment of the availability and nutrient profile of ultra-processed foods. Public Health Nutr. 2021, 24, 3179–3186. [Google Scholar] [CrossRef]
- McCann, J.; Russell, G.; Campbell, K.; Woods, J. Nutrition and packaging characteristics of toddler foods and milks in Australia. Public Health Nutr. 2021, 24, 1153–1165. [Google Scholar] [CrossRef]
- Grammatikaki, E.; Wollgast, J.; Caldeira, S. High levels of nutrients of concern in baby foods available in Europe that contain sugar-contributing ingredients or are ultra-processed. Nutrients 2021, 13, 3105. [Google Scholar] [CrossRef] [PubMed]
- Spaniol, A.M.; Da Costa, T.H.M.; Souza, A.D.M.; Gubert, M.B. Early consumption of ultra-processed foods among children under 2 years old in Brazil. Public Health Nutr. 2021, 24, 3341–3351. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.C.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: What they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; De Ridder, K.; Fiolet, T.; Bel, S.; Tafforeau, J. Consumption of ultra-processed food products and diet quality among children, adolescents and adults in Belgium. Eur. J. Nutr. 2019, 58, 3267–3278. [Google Scholar] [CrossRef]
- Neri, D.; Martinez-Steele, E.; Monteiro, C.A.; Levy, R.B. Consumption of ultra-processed foods and its association with added sugar content in the diets of US children, NHANES 2009-2014. Pediatr. Obes. 2019, 14, e12563. [Google Scholar] [CrossRef]
- Moubarac, J.C.; Batal, M.; Louzada, M.L.; Martinez Steele, E.; Monteiro, C.A. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Augustin, M.A.; Riley, M.; Stockmann, R.; Bennett, L.; Kahl, A.; Lockett, T.; Osmond, M.; Sanguansri, P.; Stonehouse, W.; Zajac, I.; et al. Role of food processing in food and nutrition security. Trends Food Sci. Technol. 2016, 56, 115–125. [Google Scholar] [CrossRef]
- Costa, C.S.; Del-Ponte, B.; Assunção, M.C.F.; Santos, I.S. Consumption of ultra-processed foods and body fat during childhood and adolescence: A systematic review. Public Health Nutr. 2018, 21, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Askari, M.; Heshmati, J.; Shahinfar, H.; Tripathi, N.; Daneshzad, E. Ultra-processed food and the risk of overweight and obesity: A systematic review and meta-analysis of observational studies. Int. J. Obes. 2020, 44, 2080–2091. [Google Scholar] [CrossRef]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-processed food intake and risk of cardiovascular disease: Prospective cohort study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef] [Green Version]
- Schnabel, L.; Kesse-Guyot, E.; Allès, B.; Touvier, M.; Srour, B.; Hercberg, S.; Buscail, C.; Julia, C. Association between Ultraprocessed Food Consumption and Risk of Mortality among Middle-aged Adults in France. JAMA Intern. Med. 2019, 179, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Sadler, C.R.; Grassby, T.; Hart, K.; Raats, M.; Sokolović, M.; Timotijevic, L. Processed food classification: Conceptualisation and challenges. Trends Food Sci. Technol. 2021, 112, 149–162. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.L.; Machado, P.P. The NOVA Food Classification System and Its Four Food Groups; FAO: Rome, Italy, 2019; ISBN 9789251317013. [Google Scholar]
- Khandpur, N.; Neri, D.A.; Monteiro, C.; Mazur, A.; Frelut, M.L.; Boyland, E.; Weghuber, D.; Thivel, D. Ultra-Processed Food Consumption among the Paediatric Population: An Overview and Call to Action from the European Childhood Obesity Group. Ann. Nutr. Metab. 2020, 76, 109–113. [Google Scholar] [CrossRef]
- De Araújo, C.R.B.; Ribeiro, K.D.D.S.; De Oliveira, A.F.; De Morais, I.L.; Breda, J.; Padrão, P.; Moreira, P. Degree of processing and nutritional value of children’s food products. Public Health Nutr. 2021, 24, 5977–5984. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. Perfil Nutricional—Restrições à Publicidade Alimentar Dirigida a Crianças; Ministério da Saúde: Lisbon, Portugal, 2019.
- Graça, P.; Gregório, M.J. Strategy for the promotion of healthy eating in Portugal. Health Numbers Port. 2015, 4, 36–40. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on Dietary Reference Values for carbohydrates and dietary fibre. EFSA J. 2010, 8, 1462. [Google Scholar] [CrossRef] [Green Version]
- Dodrill, P. Typical Feeding and Swallowing Development in Infants and Children. In Dysphagia; Elsevier: Amsterdam, The Netherlands, 2016; pp. 253–269. ISBN 9780323187015. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 26.0; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Gómez-Martín, M.; Arboleya, S.; Gueimonde, M.; González, S. Nutritional composition of processed baby foods targeted at infants from 0–12 months. J. Food Compos. Anal. 2019, 79, 55–62. [Google Scholar] [CrossRef]
- Azzopardi, D.J.; Lacy, K.E.; Woods, J.L. Energy density of new food products targeted to children. Nutrients 2020, 12, 2242. [Google Scholar] [CrossRef]
- FAO; WHO. Codex Alimentarius: International Food Sandards. Guidelines on Formulated Complementary Foods for Older Infants and Young; FAO: Rome, Italy, 2017. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on Dietary Reference Values for energy. EFSA J. 2013, 11, 3005. [Google Scholar] [CrossRef] [Green Version]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in Infants, Children and Adolescents: A Position Paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, M.B.; Kaar, J.L.; Welsh, J.A.; Van Horn, L.V.; Feig, D.I.; Anderson, C.A.M.; Patel, M.J.; Cruz Munos, J.; Krebs, N.F.; Xanthakos, S.A.; et al. Added Sugars and Cardiovascular Disease Risk in Children: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e1017–e1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012; pp. 1–56. [Google Scholar]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary feeding: A position paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.-I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; et al. Dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maalouf, J.; Cogswell, M.E.; Bates, M.; Yuan, K.; Scanlon, K.S.; Pehrsson, P.; Gunn, J.P.; Merritt, R.K. Sodium, sugar, and fat content of complementary infant and toddler foods sold in the United States, 2015. Am. J. Clin. Nutr. 2017, 105, 1443–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padarath, S.; Gerritsen, S.; Mackay, S. Nutritional aspects of commercially available complementary foods in New Zealand supermarkets. Nutrients 2020, 12, 2980. [Google Scholar] [CrossRef]
- Pace, L.; Bica, M.; Williams, J.; Hutchinson, J.; Cade, J.E.; Wickramasinghe, K.; Vassallo, C.; Breda, J. High levels of sugar and salt in commercial baby foods in Malta: Results from a pilot study using the world health organization draft nutrient profile model. Malta Med. J. 2020, 32, 59–76. [Google Scholar]
- CODEX Alimentarius. Guidelines for the Use of Nutrition and Health Claims. (CAC/GL 23-1997); Joint FAO/WHO Codex Alimentarius Commission; Codex Alimentarius Commission: Rome, Italy, 1997. [Google Scholar]
- WHO Regional Office for Europe. Commercial Foods for Infants and Young Children in the WHO European Region: A Study of the Availability, Composition and Marketing of Baby Foods in Four European Countries; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- European Food Safety Authority. Scientific Opinion on Establishing Food-Based Dietary Guidelines; EFSA: Parma, Italy, 2010; Volume 8. [Google Scholar]
- Lanigan, J. Prevention of overweight and obesity in early life. Proc. Nutr. Soc. 2018, 77, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Doub, A.E. Learning to eat: Birth to age 2 y. Am. J. Clin. Nutr. 2014, 99, 723S–728S. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Martínez Steele, E.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in Consumption of Ultraprocessed Foods among US Youths Aged 2–19 Years, 1999–2018. JAMA J. Am. Med. Assoc. 2021, 326, 519–530. [Google Scholar] [CrossRef]
- Fardet, A.; Thivel, D.; Gerbaud, L.; Rock, E. A Sustainable and Global Health Perspective of the Dietary Pattern of French Population during the 1998–2015 Period from INCA Surveys. Sustainability 2021, 13, 7433. [Google Scholar] [CrossRef]
- Costa, C.S.; Rauber, F.; Leffa, P.S.; Sangalli, C.N.; Campagnolo, P.D.B.; Vitolo, M.R. Ultra-processed food consumption and its effects on anthropometric and glucose profile: A longitudinal study during childhood. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Araújo, C.; Ribeiro, K.D.; Padrão, P.; Moreira, P. Industrialized foods in early infancy: A growing need of nutritional research. Porto Biomed. J. 2019, 4, e47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Regional Office for Europe. Improving Dietary Intake and Achieving Food Product Improvement. Policy Opportunities and Challenges for the WHO European Region in Reducing Salt and Sugar in the Diet; WHO: Geneva, Switzerland, 2020. [Google Scholar]




| Characteristic | Classification | Number (n) | Percentage (%) |
|---|---|---|---|
| Product/Food category | Dry instant cereals | 30 | 15.7 |
| Dry cereals (with high-protein food (added)-powder milk or whey) | 15 | 7.9 | |
| Fruit purée (with/without vegetables) | 62 | 32.5 | |
| Fruit purée with cereal/milk | 37 | 19.4 | |
| Vegetable purée | 3 | 1.6 | |
| Vegetables purée with cereal, soft, wet, spoonable | 3 | 1.6 | |
| Savoury puréed meals | 17 | 8.9 | |
| Dairy, soft, wet, spoonable | 15 | 7.9 | |
| Sweet snacks | 9 | 4.7 | |
| Processing level (NOVA) | Minimally processed | 70 | 36.6 |
| Processed | 3 | 1.6 | |
| Ultra-processed | 118 | 61.8 | |
| Age group (months) | Group 1 (4 to <6) | 24 | 12.6 |
| Group 2 (6 to <8) | 117 | 61.3 | |
| Group 3 (8 to <12) | 36 | 18.8 | |
| Group 4 (≥ 12) | 14 | 7.3 |
| Dry Instant Cereals | Dry Cereals (with High-Protein Food) | Fruit Purée (with/without Vegetables); | Fruit Purée with Cereal/Milk | Vegetable Purees | Vegetables with Cereal, Soft, Wet Spoonable | Savoury Puréed Meals | Dairy, Soft, Wet, Spoonable | Sweet Snacks | p * | |
|---|---|---|---|---|---|---|---|---|---|---|
| Energy (kJ) | 1651 (1617–1696) | 1739 (398–1781) | 243 (220–274) | 271 (244–305) | 105 (81.0–†) | 223 (195–†) | 254 (236–296) | 339 (276–383) | 1810 (1787–1903) | <0.001 |
| SD | 57 | 624 | 41 | 49 | 47 | 38 | 39 | 50 | 60 | |
| Protein (g) | 10.0 (7.9–12.0) | 13.6 (2.9–16.5) | 0.4 (0.3–0.7) | 0.7 (0.4–1.0) | 0.8 (0.3–†) | 1.3 (0.7–†) | 2.7 (2.4–2.9) | 3.0 (2.7–3.1) | 8.7 (6.7–9.7) | <0.001 |
| SD | 3.8 | 5.8 | 0.2 | 0.7 | 0.3 | 0.8 | 0.4 | 0.5 | 2.8 | |
| Total fat (g) | 2.3 (1.8–4.6) | 9.5 (3.0–11.0) | 0.2 (0.1–0.2) | 0.3 (0.2–1.0) | 0.3 (0.2–†) | 1.1 (1.0–†) | 1.8 (1.7–2.2) | 2.8 (2.3–3.2) | 10.0 (8.6–13.5) | <0.001 |
| SD | 2.8 | 3.9 | 0.2 | 1.4 | 0.7 | 0.7 | 0.4 | 0.6 | 2.4 | |
| Saturated fatty acids (g) | 0.5 (0.3–1.5) | 1.8 (1.3–2.5) | 0.0 (0.0–0.6) | 0.0 (0.0–0.3) | 0.0 (0.0–†) | 0.1 (0.0–†) | 0.4 (0.3–0.6) | 1.5 (1.3–2.0) | 1.3 (1.3–3.3) | <0.001 |
| SD | 1.2 | 1.3 | 0.2 | 0.7 | 0.2 | 0.4 | 0.2 | 0.4 | 1.9 | |
| Carbohydrate (g) | 76.7 (75.0–82.0) | 63.0 (14.0–66.4) | 12.9 (11.3–14.1) | 13.0 (12.0–15.0) | 4.1 (3.5–†) | 8.0 (8.0–†) | 7.60 (6.6–9.3) | 11.5 (8.8–12.2) | 76.0 (75.0–76.0) | <0.001 |
| SD | 7.3 | 24.8 | 2.3 | 1.9 | 1.2 | 0.3 | 1.6 | 2.3 | 1.9 | |
| Total sugars (g) | 20.0 (1.5–26,2) | 27.2(8.0–31.1) | 11.0 (9.1–12.1) | 10.7 (9,6–12.0) | 1.5 (1.3–†) | 2.9 (2.0–†) | 1.3 (1.2–2.4) | 7.2 (5.0–8.1) | 12.0 (2.8–24.0) | <0.001 |
| SD | 12.7 | 10.7 | 2.2 | 1.7 | 0.5 | 0.7 | 0.9 | 2.0 | 11.0 | |
| Sodium (mg) | 16.0 (4.0–45.0) | 80.0 (36.0–108) | 4.00 (2.0–16.0) | 4.00 (0.0–16.5) | 28.0 (25.2–†) | 16.0 (12.0–†) | 32.0 (20.0–78.0) | 36.0 (30.0–52.0) | 32.0 (8.0–80.0) | <0.001 |
| SD | 54.0 | 49.9 | 14.4 | 11.6 | 17.0 | 8.3 | 40.0 | 14.7 | 68.9 |
| Characteristic | Sub-Category or Classification | Number (n) | Percentage (%) |
|---|---|---|---|
| Nutrition/Composition Claim | Yes | 185 | 96.9 |
| No | 6 | 3.1 | |
| Health Claim | Yes | 17 | 9.0 |
| No | 174 | 91.0 | |
| Claim type | Composition claim | ||
| No added preservatives | 57 | 29.8 | |
| Gluten-free | 64 | 33.5 | |
| Organic food | 47 | 24.6 | |
| Egg-free | 15 | 7.9 | |
| Dairy-free | 18 | 9.4 | |
| Nutrition claim | |||
| No added sugar | 133 | 69.6 | |
| No added salt | 52 | 27.2 | |
| Contains vitamin C | 26 | 13.6 | |
| Contains iron | 19 | 9.9 | |
| Contains calcium | 27 | 14.1 | |
| Contains vitamin E | 3 | 1.6 | |
| Contains multiple vitamins | 16 | 8.4 | |
| Contains multiple minerals | 13 | 6.8 | |
| Contains dietary fiber | 8 | 4.2 | |
| Health claim | |||
| Nutritionally balanced/provides good nutrition to children | 15 | 7.9 | |
| Cognitive ability | 2 | 1.0 | |
| Visual Information (cartons, pictures) | Yes | 74 | 39.0 |
| No | 117 | 61.0 |
| Dry Instant Cereals | Dry Cereals (with High-Protein Food) | Fruit Purée (with/without Vegetables) | Fruit Purée with Cereal/Milk | Vegetable Purée | Vegetables Purée with Cereal, Soft, Wet, Spoonable | Savoury Puréed Meals | Dairy, Soft, Wet, Spoonable | Sweet Snacks | Total 1 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 30 (15.7%) | 15 (7.9%) | 62 (32.5%) | 37 (19.4%) | 3 (1.6%) | 3 (1.6%) | 17 (8.9%) | 15 (7.9%) | 9 (4.7%) | 193 (100%) |
| Composition Claim No added preservatives (a) | 2 (6.7%) | 1 (6.7%) | 28 (45.2%) | 7 (19.9%) | 0 (0.0%) | 0 (0.0%) | 12 (70.6%) | 7 (46.7%) | 0 (0.0%) | 57 (29.8%) |
| Gluten-free (b) | 6 (20.0%) | 3 (20.0%) | 29 (46.8%) | 10 (27.0%) | 3 (100.0%) | 1 (33.3%) | 4 (23.5%) | 7 (46.7%) | 1 (11.1%) | 64 (33.5%) |
| Organic food (a) | 1 (3.3%) | 0 (0.0%) | 17 (27.4%) | 16 (43.2%) | 0 (0.0%) | 3 (100.0%) | 5 (29.4%) | 4 (26.7%) | 1 (11.1%) | 47 (24.6%) |
| Nutrition Claim No added sugar (a) | 16 (53.3%) | 5 (33.3%) | 59 (95.2%) | 34 (91.9%) | 0 (0.0%) | 0 (0.0%) | 5 (29.4%) | 10 (66.7%) | 4 (44.4%) | 133 (69.6%) |
| No added salt (a) | 13 (43.3%) | 5 (33.3%) | 10 (16.1%) | 3 (8.1%) | 3 (100.0%) | 2 (66.7%) | 12 (70.6%) | 1 (6.7%) | 3 (33.3%) | 52 (27.2%) |
| Health Claim Nutritionally balanced/provides good nutrition to children | 0 (0.0%) | 1 (6.7)% | 0 (0.0%) | 3 (8.1%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 10 (66.7%) | 1 (11.1%) | 15 (7.9%) |
| Ingredients (added sugars) Sugar (a) | 9 (30.0%) | 5 (33.0%) | 3 (4.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 5 (33.0%) | 5 (55.6%) | 27 (13.9%) |
| Fruit juice concentrated (c) | 2 (6.7%) | 3 (20.0%) | 11 (17.7%) | 11 (29.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 2 (13.3%) | 0 (0.0%) | 29 (15.0%) |
| Other added sugars (d), (e), (f) | 5 (16.6%) | 0 (0.0%) | 0 (0.0%) | 3 (8.1%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (11.1%) | 9 (4.7%) |
| Minimally Processed | Processed | Ultra-Processed | p * | |
|---|---|---|---|---|
| Energy (kJ) | 245 (222–272) a,c | 105 (81.0–†) a | 383 (276–1681) b | <0.001 |
| SD | 39 | 47 | 708 | |
| Energy (kcal) | 58.0 (52.5–64.5) a,c | 24.9 (19.0–†) a | 91.0 (66.0–397.3) b | <0.001 |
| SD | 9.0 | 11.3 | 167.4 | |
| Protein (g) | 0.4 (0.3–0.7) a | 0.8 (0.3–†) a,c | 3.0 (1.9–10.0) b,c | <0.001 |
| SD | 0.2 | 0.3 | 5.0 | |
| Total fat (g) | 0.2 (0.1–0.2) a | 0.3 (0.2–†) a,c | 2.3 (1.1–4.0) b,c | <0.001 |
| SD | 0.2 | 0.7 | 3.6 | |
| Saturated fatty acids (g) | 0.0 (0.0–0.0) a | 0.0 (0.0–†) a,c | 0.7(2.9–1.8) b,c | <0.001 |
| SD | 0.2 | 0.2 | 1.2 | |
| Carbohydrate (g) | 12.9 (11.4–14.0) b | 4.1 (3.5–†) a | 15.0 (11.2–75.0) c | <0.001 |
| SD | 2.2 | 1.2 | 32.0 | |
| Total sugars (g) | 11.0 (9.5–12.1) b,c | 1.5 (1.3–†) a | 9.0 (2.9–19.0) a,c | 0.040 |
| SD | 2.1 | 0.5 | 10.4 | |
| Sodium (mg) | 4.0 (0.4–12.0) a | 25.2 (0.56–†) a,c | 24.6 (8.0–52.0) b,c | <0.001 |
| SD | 14.0 | 15.0 | 46.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.; Matias, F.; Loureiro, I.; Rito, A.I.; Castanheira, I.; Bento, A.; Assunção, R. Commercial Baby Foods Aimed at Children up to 36 Months: Are They a Matter of Concern? Foods 2022, 11, 1424. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101424
Santos M, Matias F, Loureiro I, Rito AI, Castanheira I, Bento A, Assunção R. Commercial Baby Foods Aimed at Children up to 36 Months: Are They a Matter of Concern? Foods. 2022; 11(10):1424. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101424
Chicago/Turabian StyleSantos, Mariana, Filipa Matias, Isabel Loureiro, Ana Isabel Rito, Isabel Castanheira, Alexandra Bento, and Ricardo Assunção. 2022. "Commercial Baby Foods Aimed at Children up to 36 Months: Are They a Matter of Concern?" Foods 11, no. 10: 1424. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101424