
Decompensated Cirrhosis as Presentation of LKM1/LC1 Positive Type 2 Autoimmune Hepatitis in Adulthood. A Rare Clinical Entity of Difficult Management

 , , ,
, , ,
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zachou, K.; Muratori, P.; Koukoulis, G.K.; Granito, A.; Gatselis, N.; Fabbri, A.; Dalekos, G.N. Review article: Autoimmune hepatitis—current management and challenges. Aliment. Pharmacol. Ther. 2013, 38, 887–913. [Google Scholar] [CrossRef] [PubMed]
- Muratori, P.; Granito, A.; Quarneti, C.; Ferri, S.; Menichella, R.; Cassani, F.; Pappas, G.; Bianchi, F.B.; Lenzi, M.; Muratori, L. Autoimmune hepatitis in Italy: The Bologna experience. J. Hepatol. 2009, 50, 1210–1218. [Google Scholar] [CrossRef]
- Czaja, A.J. Review article: The management of autoimmune hepatitis beyond consensus guidelines. Aliment. Pharmacol. Ther. 2013, 38, 343–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muratori, L.; Muratori, P.; Granito, A.; Pappas, G.; Cassani, F.; Lenzi, M. Current topics in autoimmune hepatitis. Dig Liver Dis. 2010, 42, 757–764. [Google Scholar] [CrossRef]
- McFarlane, I.G. The relationship between autoimmune markers and different clinical syndromes in autoimmune hepatitis. Gut 1998, 42, 599–602. [Google Scholar] [CrossRef]
- Czaja, A.J. Autoantibody-negative autoimmune hepatitis. Dig. Dis Sci. 2012, 57, 610–624. [Google Scholar] [CrossRef]
- Maggiore, G.; Bernard, O.; Homberg, J.-C.; Hadchouel, M.; Alvarez, F.; Hadchouel, P.; Odièvre, M.; Alagille, D. Liver disease associated with anti-liver-kidney microsome antibody in children. J. Pediatr. 1986, 108, 399–404. [Google Scholar] [CrossRef]
- Muratori, P.; Granito, A.; Pappas, G.; Muratori, L.; Lenzi, M.; Bianchi, FB. Autoimmune liver disease 2007. Mol Aspects Med. 2008, 29, 96–102. [Google Scholar] [CrossRef]
- Bogdanos, D.P.; Mieli-Vergani, G.; Vergani, D. Liver-kidney microsomal antibody-positive autoimmune hepatitis in the United States. Am. J. Gastroenterol. 2001, 96, 3447–3448. [Google Scholar] [CrossRef] [PubMed]
- Homberg, J.C.; Abuaf, N.; Bernard, O.; Islam, S.; Alvarez, F.; Khalil, S.H.; Poupon, R.; Darnis, F.; Lévy, V.G.; Grippon, P.; et al. Chronic active hepatitis associated with antiliver/kidney microsome antibody type 1: A second type of "autoimmune" hepatitis. Hepatology 1987, 7, 1333–1339. [Google Scholar] [CrossRef]
- Duchini, A.; McHutchison, J.G.; Pockros, P.J. LKM-positive autoimmune hepatitis in the western United States: A case series. Am. J. Gastroenterol. 2000, 95, 3238–3241. [Google Scholar] [CrossRef]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines from the American Association for the Study of Liver Diseases. Hepatology 2020, 72, 671–722. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Muratori, P.; Quarneti, C.; Pappas, G.; Cicola, R.; Muratori, L. Antinuclear antibodies as ancillary markers in primary biliary cirrhosis. Expert Rev. Mol. Diagn. 2012, 12, 65–74. [Google Scholar] [CrossRef]
- Granito, A.; Muratori, P.; Ferri, S.; Pappas, G.; Quarneti, C.; Lenzi, M.; Bianchi, F.B.; Muratori, L. Diagnosis and therapy of autoimmune hepatitis. Mini Rev. Med. Chem. 2009, 9, 847–860. [Google Scholar] [CrossRef]
- Muratori, L.; Cassani, F.; Pappas, G.; Guidi, M.; Mele, L.; Lorenza, V.; Lenzi, M.; Bianchi, F.B.; Muratori, P. The hepatitic/cholestatic "overlap" syndrome: An Italian experience. Autoimmunity 2002, 35, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Vergani, D.; Alvarez, F.; Bianchi, F.B.; Cançado, E.L.; Mackay, I.R.; Manns, M.P.; Nishioka, M.; Penner, E. International Autoimmune Hepatitis Group. Liver autoimmune serology: A consensus statement from the committee for autoimmune serology of the International Autoimmune Hepatitis Group. J. Hepatol. 2004, 41, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Terziroli Beretta-Piccoli, B.; Mieli-Vergani, G.; Vergani, D. The clinical usage and definition of autoantibodies in immune-mediated liver disease: A comprehensive overview. J. Autoimmun. 2018, 95, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Mieli-Vergani, G.; Vergani, D.; Czaja, A.J.; Manns, M.P.; Krawitt, E.L.; Vierling, J.M.; Lohse, A.W.; Montano-Loza, A.J. Autoimmune hepatitis. Nat. Rev. Dis Primers 2018, 4, 18017. [Google Scholar] [CrossRef]
- Gregorio, G.V.; Portmann, B.; Reid, F.; Donaldson, P.T.; Doherty, D.G.; McCartney, M.; Mowat, A.P.; Vergani, D.; Mieli-Vergani, G. Autoimmune hepatitis in childhood: A 20-year experience. Hepatology 1997, 25, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Sheng, L.; Yang, Y.; Yang, F.; Xiao, X.; Hua, J.; Guo, C.; Wei, Y.; Tang, R.; Miao, Q.; et al. The Management of Autoimmune Hepatitis Patients with Decompensated Cirrhosis: Real-World Experience and a Comprehensive Review. Clin. Rev. Allergy Immunol. 2017, 52, 424–435. [Google Scholar] [CrossRef]
- Carpenter, H.A.; Czaja, A.J. The role of histologic evaluation in the diagnosis and management of autoimmune hepatitis and its variants. Clin. Liver Dis. 2002, 6, 685–705. [Google Scholar] [CrossRef]
- Tiniakos, D.G.; Brain, J.G.; Bury, Y.A. Role of Histopathology in Autoimmune Hepatitis. Dig. Dis. 2015, 33 (Suppl. 2), 53–64. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.J.; Dinh, H.; Arenovich, T.; Marcus, V.A.; Wanless, I.R.; Heathcote, E.J. Autoimmune hepatitis: Effect of symptoms and cirrhosis on natural history and outcome. Hepatology 2005, 42, 53–62. [Google Scholar] [CrossRef]
- Czaja, A.J. Difficult treatment decisions in autoimmune hepatitis. World J. Gastroenterol. 2010, 16, 934–947. [Google Scholar] [CrossRef]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M.; American Association for the Study of Liver Diseases. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Metzler, F.; Geiger, E.; Heinrich, E.; Hallensleben, M.; Manns, M.P.; Vogel, A. Prediction of short- and long-term outcome in patients with autoimmune hepatitis. Hepatology 2015, 62, 1524–1535. [Google Scholar] [CrossRef]
- Dhaliwal, H.K.; Hoeroldt, B.S.; Dube, A.K.; McFarlane, E.; Underwood, J.C.; Karajeh, M.A.; Gleeson, D. Long-Term Prognostic Significance of Persisting Histological Activity Despite Biochemical Remission in Autoimmune Hepatitis. Am. J. Gastroenterol. 2015, 110, 993–999. [Google Scholar] [CrossRef]
- Roberts, S.K.; Therneau, T.M.; Czaja, A.J. Prognosis of histological cirrhosis in type 1 autoimmune hepatitis. Gastroenterology 1996, 110, 848–857. [Google Scholar] [CrossRef]
- Uribe, M.; Go, V.L.; Kluge, D. Prednisone for chronic active hepatitis: Pharmacokinetics and serum binding in patients with chronic active hepatitis and steroid major side effects. J. Clin. Gastroenterol. 1984, 6, 331–335. [Google Scholar] [PubMed]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Autoimmune hepatitis. J. Hepatol. 2015, 63, 971–1004. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Patient Value | Reference Values |
|---|---|---|
| AST | 81 | <40 |
| ALT | 125 | <40 |
| Total Bilirubin (mg/dl) | 2.9 | <1.2 |
| ALP | 131 | <120 |
| γGT | 321 | <38 |
| Total protein/γ-globulin (g/L/%) | 5.8/26% | 6.6–8.3/11–18.8% |
| Albumin serum level (g/L) | 26 | 35–50 |
| IgG serum level (mg/dL) | 3213 | 700–1600 |
| IgM serum level (mg/dL) | 155 | 40–230 |
| IgA serum level (mg/dL) | 7 | 70–400 |
| ANA | Negative | Negative |
| SMA | Negative | Negative |
| LKM1 | 1:1280 ^ +++ * | Negative |
| LC1 | +++ * | Negative |
| SLA | Negative | Negative |
| AMA | Negative | Negative |
| Anti-Sp100 | Negative | Negative |
| Anti-gp210 | Negative | Negative |
| pANCA | Negative | Negative |
| Anti-tTG IgA/IgG | Negative | Negative |
| AIH revised score | 23 | Definite AIH: >15 Probable: 10–15 |
| AIH simplified score | 8 | Definite: AIH: ≥7 Probable: AIH: ≥6 |
| Time | Event | Findings |
|---|---|---|
| July 2018 | Admitted to the Internal Medicine Unit of the local hospital due to progressive abdominal distension associated with liver enzymes (3–4× UNL) and bilirubin (2.8 mg/dL) elevation | Laboratory and imaging features suggestive for decompensated cirrhosis with abundant ascites |
| Laboratory workup for liver function assessment | Child–Pugh B9 MELD 12 | |
| Laboratory workup for cirrhosis etiology | HBV and HCV negative viral markers | |
| Albumin infusion and diuretic therapy | Improvement of ascites | |
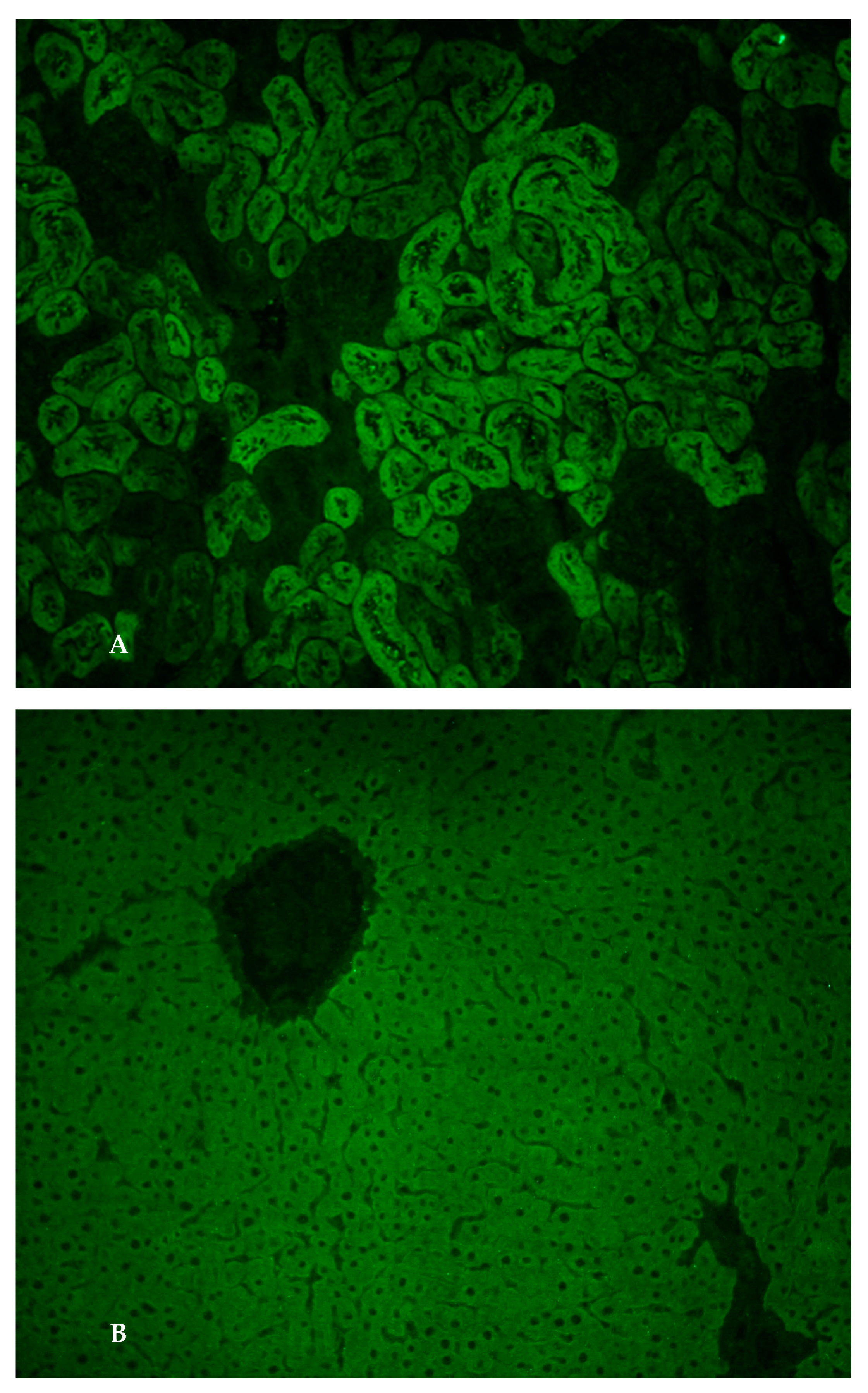
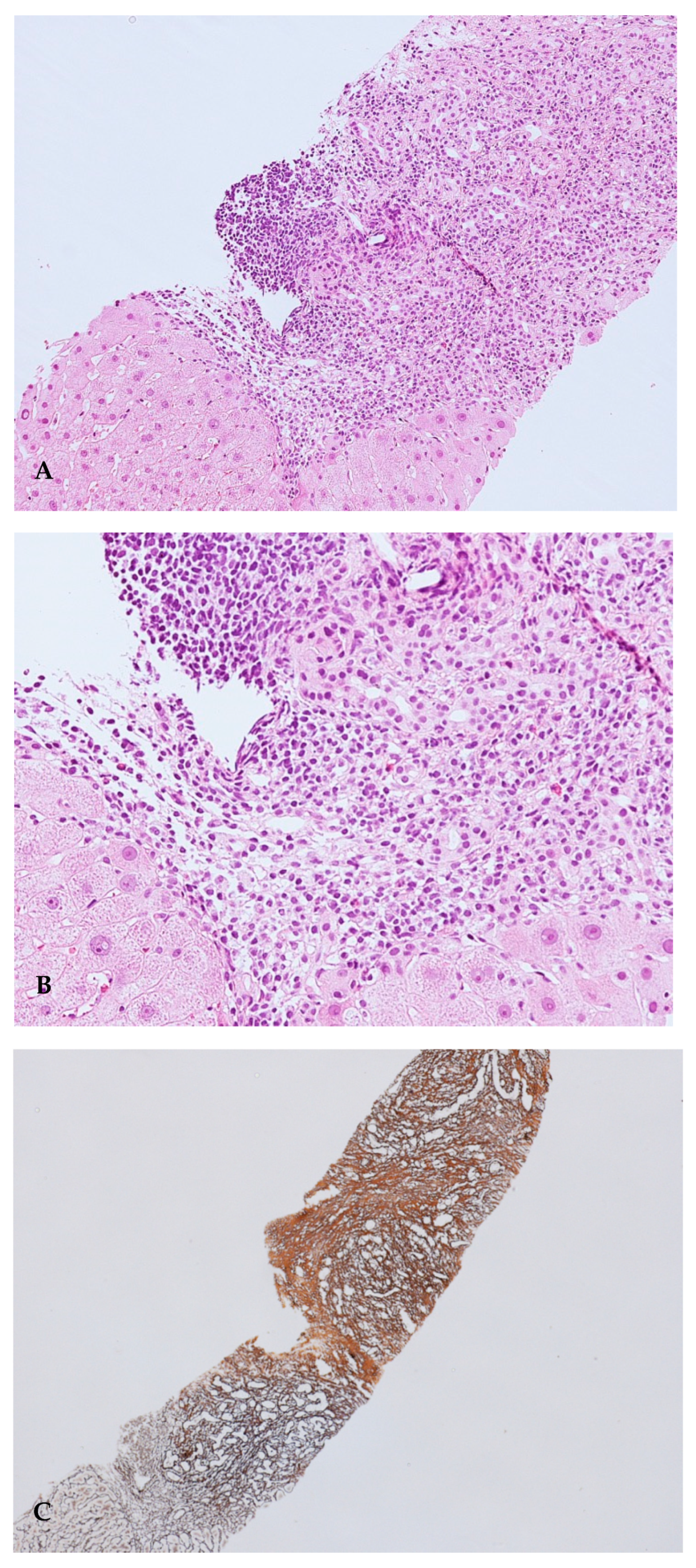
| September 2018 | Admitted to the Center for the Study and Treatment of Autoimmune Diseases of the Liver and Biliary System for suspected autoimmune liver diseases due to the raised serum IgG level | LKM1 and LC1 autoantibody positivity by IIF, confirmed by a second level immunoblot assay; liver histology with typical AIH features; revised and simplified AIH scores indicating definite AIH |
| October 2018 | Ascites resolution. Starting corticosteroid treatment (prednisone 15 mg/day) | Improved but still elevated transaminases after 2 w (3× → 1.8× UNL) and gammaGT (8.5 → 7) |
| December 2018 | Progressive corticosteroid tapering Addition of azathioprine 50 mg/day | Stable liver enzymes (ALT 1.6× UNL: gammaGT 6.5×) |
| April 2019 | Stable disease with prednisone 7.5 mg/day and azathioprine increased to 100 mg/day | ALT 1.3× UNL GammaGT 8× UNL Liver stiffness of 22.8 kPa |
| June 2019 | Magnetic resonance cholangiography because of persistent gammaGT elevation | no bile duct stones or biliary obstruction |
| December 2019 | Urinary sepsis due to Streptococcus Pneumoniae | Immunosuppressive treatment withdrawal |
| January 2020 | ALT 3x UNL; gammaGT 9.9× UNL Total bilirubin 2.5 mg/dl IgG 1.8× UNL Child-Pugh B7; MELD 13 | Resumption of prednisone 10 mg/day and azathioprine 100 mg/day |
| June 2020 | Sepsis due to Streptococcus Pneumoniae | Immunosuppressive treatment withdrawal Child–Pugh C12 |
| November 2020 | Clinical and biochemical re-evaluation prednisone 5 mg/day and azathioprine 50 mg/day | Child–Pugh B8; MELD 14 Transaminases 1.6× UNL gammaGT 6.8× UNL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granito, A.; Pascolini, S.; Ricci, C.; Ferronato, M.; Muratori, L.; Vasuri, F.; Franceschini, T.; Lenzi, M.; Muratori, P. Decompensated Cirrhosis as Presentation of LKM1/LC1 Positive Type 2 Autoimmune Hepatitis in Adulthood. A Rare Clinical Entity of Difficult Management. Gastroenterol. Insights 2021, 12, 67-75. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010007
Granito A, Pascolini S, Ricci C, Ferronato M, Muratori L, Vasuri F, Franceschini T, Lenzi M, Muratori P. Decompensated Cirrhosis as Presentation of LKM1/LC1 Positive Type 2 Autoimmune Hepatitis in Adulthood. A Rare Clinical Entity of Difficult Management. Gastroenterology Insights. 2021; 12(1):67-75. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010007
Chicago/Turabian StyleGranito, Alessandro, Simona Pascolini, Chiara Ricci, Marco Ferronato, Luigi Muratori, Francesco Vasuri, Tania Franceschini, Marco Lenzi, and Paolo Muratori. 2021. "Decompensated Cirrhosis as Presentation of LKM1/LC1 Positive Type 2 Autoimmune Hepatitis in Adulthood. A Rare Clinical Entity of Difficult Management" Gastroenterology Insights 12, no. 1: 67-75. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12010007