
Patient-Reported Outcomes in Inflammatory Bowel Disease: A Measurement of Effect in Research and Clinical Care


Abstract
:1. Introduction
2. Materials and Methods
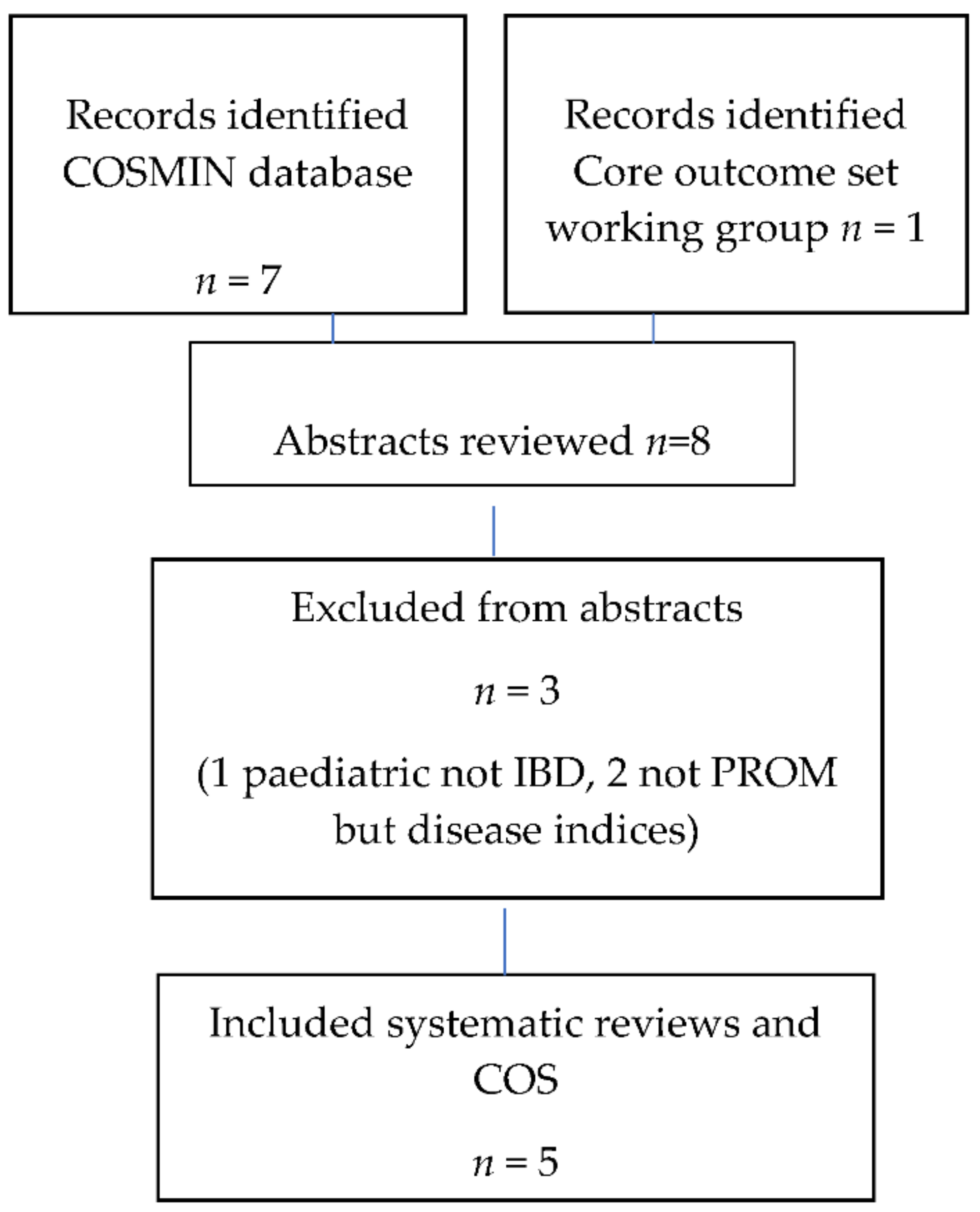
2.1. Search Strategy
2.2. Data Extraction
2.3. Quality Evaluation
3. Results

{kind=link}
| Outcome Measure | Citation | Disease | Method of Administration | Recall Period | Reported Parametric Properties # | Comments |
|---|---|---|---|---|---|---|
| The 32-item Inflammatory Bowel Disease Questionnaire (IBDQ-32) [15] | [11] [10] [12] [5,13] | IBD | Self-report | Past 2 weeks | Consistency 3* Reliability 3* Validity 4* | Versions for patients with or without a stoma. Extensively validated. License required for use. |
| The Short Inflammatory Bowel Disease Questionnaire (SIBDQ) [16] | [11] [10] [5] | IBD | Self-report | Past 2 weeks | Consistency 2* Reliability 2* Validity 3* | 10 questions selected from the IBDQ-32 for community use in general practice. License required for use |
| The 36-item Inflammatory Bowel Disease Questionnaire (IBDQ-36) [17] | [11] | IBD | Self-report | Past 2 weeks | Consistency 2* Reliability NA Validity 2* | IBDQ-32 but with an additional functional element. Less well validated in comparison to the IBDQ-32 [11]. |
| The 9-item Inflammatory Bowel Disease Questionnaire (IBDQ-9) [18] | [11] [10] [5] | IBD | Self-report (9 questions derived from the IBDQ-36) | Past 2 weeks | Consistency 2* Reliability 2* Validity 3* | Further shortened version of IBDQ-32. |
| The Rating Form of IBD Patient Concerns(RFIPC) [19] | [11] [10] [12] [13] | IBD | Self-report (25 questions) | Today | Consistency 4* Reliability 2* Validity 4* | Aim is to elicit patient concerns rather than to determine disease impact on their quality of life. |
| The Cleveland Clinic Questionnaire for Inflammatory Bowel Disease(CCQIBD) [20] | [11] [12] | IBD | Self-report and interview (47 questions) | Past 2 months | Consistency NA Reliability 1* Validity 3* | Limited evidence available for validity noted by Chen et al. |
| The Padova Inflammatory Bowel Disease Quality of Life (PIBDQL) [21] | [11] [12] [13] | IBD | Self-report | NA | Consistency NA Reliability NA Validity 2* | Limited evidence available for their validity noted by Chen et al. |
| The Cleveland Global Quality of Life (CGQL) [22,23] | [11] [13] | IBD | Self-report (3 questions, scale 0–10) | Today | Consistency 3* Reliability NA Validity 3* | Based on patients having surgery [11]. |
| The Short Health Scale (SHS) [24] | [11] | UC | Self-report (4 questions, visual analogue scale) | No set time scale | Consistency 2* Reliability 2* Validity 2* | Not validated for CD. |
| The Edinburgh Inflammatory Bowel Disease Questionnaire (EIBDQ) [25] | [11] [10] | IBD | Self-report (15 questions) | Past 2 weeks | Consistency 3* Reliability 1* Validity 4* | Clinical focus—first two questions ask if they have been given enough information about their disease and the contact details for a patient support group. Nothing specific regarding those with a stoma. |
| The Crohn’s Life Impact Questionnaire (CLIQ) [26] | [11] | CD | Self-report (27 questions) | Today | Consistency 4* Reliability 3* Validity 4* | Specific to CD. |
| The Crohn’s and ulcerative colitis questionnaire (CUCQ-32) [27] | [11] [5] | IBD | Self-report (32 questions) | Past 2 weeks | Consistency 2* Reliability 3* Validity 3* | Similar to the IBDQ but nonspecific to those with a stoma. |
| The Crohn’s and ulcerative colitis questionnaire (CUCQ-8) [27] | [5] | IBD | Self-report (8 questions) | Past 2 weeks | Consistency, Reliability, Validity—graded ‘high’ in all aspects | Shortened version of CUCQ-32. |
| The UK-IBDQ [28] | [5] | IBD | Self-report (32 questions derived from the IBDQ) | Past 2 weeks | High consistency and validity, medium reliability | Anglicized version of the IBDQ. |
| The IBD disability score [29] | [10] | IBD | Self-report (44 questions) | Past month | Consistency 1* Reliability 1* Validity 4* | Section related to stoma included within the main questionnaire. |
| The IBD disability index [30] | [10] | IBD | Interviewer reads aloud to the patient (19 questions plus clinical parameters) | Past week | Consistency NA Reliability NA Validity 4* | Based on the International Classification of Disability, Function and Health. |
| Social Impact of Chronic Conditions– Inflammatory Bowel Disease (SICC-IBD) questionnaire [31] | [10] | UC [31] | Self-report (8 questions) | Ever | Consistency 1* Reliability 1* Validity 4* | Specifically looking at social impact/disability related to work, earnings, family relationship. |
| Crohn’s Disease Perceived Work Disability Questionnaire (CPWDQ) [32] | [10] | CD | Self-report (16 questions) | Past year | Consistency 2* Reliability 2* Validity 4* | Long recall period. |
| Crohn’s disease burden questionnaire [33] | [10] | CD | Self-report (4 questions, responses marked on a ‘feeling thermometer’) | Past 2 weeks then speculative to the future | Consistency 1* Reliability 1* Validity 1* | |
| Ulcerative colitis and Crohn’s disease Health Status Scales [34] | [12] | IBD | Unclear | Unclear | Not described | Authors state it is for research and clinical use [34]. |
| The IBD-Control [35] | [5] | IBD | Self-report 13 questions plus a visual analogue scale | Past 2 weeks then speculating about what they wish to discuss at the next clinical appointment | Graded ‘high’ in all aspects including responsiveness to change | Clinically focused. |
| Study | Content Validity | Internal Consistency | Structural Validity | Cross-Cultural Validity | Measurement Error | Construct Validity | Reliability | Hypothesis Testing for Construct Validity | Criterion Validity | Responsiveness | Establishment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chen et al. [11] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No |
| Dhruva et al. [13] UK | Yes | No | No | No | No | Yes | No | No | Yes | No | No |
| Kim et al. [5] UK | No | No | No | No | No | No | No | No | No | No | No |
| Alrubaiy et al. [10] UK | Yes | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Pallis [12] | No | No | No | No | No | Yes | Yes | No | No | Yes | No |
| Outcome Measure | Domains | |||
|---|---|---|---|---|
| IBD Symptoms/Disease Control | Physical or General Well-Being | Emotional | Social/Work | |
| The 32-item Inflammatory Bowel Disease Questionnaire (IBDQ-32) [15] | IBD and systemic symptoms [15] | General well-being, energy levels, weight [15] | Worry, irritable, happiness [15] | Impacting social interaction; work/school, sports and leisure [15] |
| The Short Inflammatory Bowel Disease Questionnaire (SIBDQ) [16] | IBD and systemic symptoms | - | Worry, irritable, happiness [15] | Impacting social interaction; work/school, sports and leisure [15] |
| The 36-item Inflammatory Bowel Disease Questionnaire (IBDQ-36) [17] | IBD and systemic symptoms | General well-being, energy levels, weight, functional element [15] | Worry, irritable, happiness [15] | Impacting social interaction; work/school, sports and leisure [15] |
| The 9-item Inflammatory Bowel Disease Questionnaire (IBDQ-9) [18] | IBD and systemic symptoms | Energy, unwell/general well-being | Satisfied, happy | Delaying social engagements |
| The Rating Form of IBD Patient Concerns (RFIPC) [19] | Impact and complications of IBD such as developing cancer, having surgery or a stoma | Loss of bowel control, pain | Attractiveness, loneliness | Financial difficulties |
| The Cleveland Clinic Questionnaire for Inflammatory Bowel Disease (CCQIBD) [20] | Medical/symptoms | Affect/life in general | Social/recreational | Functional/economic and social/recreational |
| The Padova Inflammatory Bowel Disease Quality of Life (PIBDQL) [21] | Intestinal and systemic symptoms [11] | - | Emotional [11] | Social [11] |
| The Cleveland Global Quality of Life (CGQL) [22,23] | - | Quality of life and health, energy level [11] | - | - |
| The Short Health Scale (SHS) [24] | Bowel problems interfering with activities, severity of symptoms | General feeling of well-being | Worry over bowel disease | - |
| The Edinburgh Inflammatory Bowel Disease Questionnaire (EIBDQ) [25] | IBD symptoms | Overall quality of life | Enough information received | Bowel functions affect social life or home life |
| The Crohn’s Life Impact Questionnaire (CLIQ) [26] | Impact of the disease e.g., fear of incontinence. Not specific to symptom control | Impact of the disease e.g., hygiene | Esteem, affection | Social needs, cognitive |
| The Crohn’s and ulcerative colitis questionnaire (CUCQ-32) [27] | IBD symptoms | General well-being | Anger, depression, frustration | Bowel problems affecting social interaction |
| The Crohn’s and ulcerative colitis questionnaire (CUCQ-8) [27] | IBD symptoms | General well-being | Feeling upset | Prevented from going out socially |
| The UK-IBDQ [28] | IBD symptoms | General well-being, energy levels | Upset, unhappy, irritable | Affected leisure and sport, work |
| The IBD disability score [29] | IBD symptoms | General well-being, weight | Mental function—anxiety, depression | Problems with mobility, travel |
| The IBD disability index [30] | IBD symptoms—medication effect | General well-being | Depression, anxiety | Household activities, work/school |
| Social Impact of Chronic Conditions–Inflammatory Bowel Disease (SICC-IBD) questionnaire [31] | - | Help with physical activities | Relationship problems | Education, employment, earning capacity |
| Crohn’s Disease Perceived Work Disability Questionnaire (CPWDQ) [32] | CD symptoms impacting capacity to work | CD symptoms and issues impacting capacity to work, e.g., fatigue, anal fissures, incontinence | Capacity to work affected by feeling forced to hide your condition, personal problems, anxiety or depression | CD symptoms impacting capacity to work |
| Crohn’s disease burden questionnaire [33] | Feelings about how CD affects their health, perception of how health might be if they did not need CD treatment | Current health, perception of how health might be without CD | - | - |
| Ulcerative colitis and Crohn’s disease Health Status Scales [34] | IBD symptoms | Perceived wellbeing, dependence on analgesia | - | - |
| The IBD-Control [35] | Control of IBD symptoms, getting better or worse, current treatment; what would you like to discuss at your next IBD appointment? | Pain, lethargy | Feeling anxious or depressed | Missed activities |
4. Discussion
4.1. IBDQ-32
4.2. IBD-Control
4.3. Disability Versus Quality of Life
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perler, B.K.; Ungaro, R.; Baird, G.; Mallette, M.; Bright, R.; Shah, S.; Shapiro, J.; Sands, B.E. Presenting symptoms in inflammatory bowel disease: Descriptive analysis of a community-based inception cohort. BMC Gastroenterol. 2019, 19, 47. [Google Scholar] [CrossRef] [Green Version]
- Conley, S.; Proctor, D.D.; Jeon, S.; Sandler, R.S.; Redeker, N.S. Symptom clusters in adults with inflammatory bowel disease. Res. Nurs. Health 2017, 40, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.V.; Winer, S.; Travis, S.P.; Riddell, R.H. Systematic review: Histological remission in inflammatory bowel disease. Is ‘complete’ remission the new treatment paradigm? An IOIBD initiative. J. Crohn’s Colitis 2014, 8, 1582–1597. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; de Vet, H.C.W. COSMIN: Consensus-Based Standards for the Selection of Health Status Measurement Instruments. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 1309–1312. [Google Scholar] [CrossRef]
- Kim, A.H.; Roberts, C.; Feagan, B.G.; Banerjee, R.; Bemelman, W.; Bodger, K.; Derieppe, M.; Dignass, A.; Driscoll, R.; Fitzpatrick, R.; et al. Developing a Standard Set of Patient-Centred Outcomes for Inflammatory Bowel Disease—an International, Cross-disciplinary Consensus. J. Crohn’s Colitis 2017, 12, 408–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Food & Drug Administration. Guidance for Industry. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims; Department of Health and Human Services (US) FDA Center for Drug Evaluation and Research: Washington, DC, USA, 2009.
- Bojic, D.; Bodger, K.; Travis, S. Patient Reported Outcome Measures (PROMs) in Inflammatory Bowel Disease: New Data. J. Crohn’s Colitis 2016, 11, S576–S585. [Google Scholar] [CrossRef]
- Prinsen, C.A.; Vohra, S.; Rose, M.R.; Boers, M.; Tugwell, P.; Clarke, M.; Williamson, P.R.; Terwee, C.B. How to select outcome measurement instruments for outcomes included in a “Core Outcome Set”—A practical guideline. Trials 2016, 17, 449. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP Checklists. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 23 March 2021).
- Alrubaiy, L.; Rikaby, I.; Dodds, P.; Hutchings, H.A.; Williams, J.G. Systematic Review of Health-related Quality of Life Measures for Inflammatory Bowel Disease. J. Crohn’s Colitis 2015, 9, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.-L.; Zhong, L.-H.; Wen, Y.; Liu, T.-W.; Li, X.-Y.; Hou, Z.-K.; Hu, Y.; Mo, C.-W.; Liu, F.-B. Inflammatory bowel disease-specific health-related quality of life instruments: A systematic review of measurement properties. Health Qual. Life Outcomes 2017, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Pallis, A.G.; Mouzas, I.A. Instruments for quality of life assessment in patients with inflammatory bowel disease. Dig. Liver Dis. 2000, 32, 682–688. [Google Scholar] [CrossRef]
- Dhruva Rao, P.K.; Davies, M.; Price, P.E.; Torkington, J. Crohn’s disease: Systematic review of assessment of disease severity and its relevance to surgery. Colorectal Dis. 2007, 9, 678–685. [Google Scholar] [CrossRef]
- David, L.; Streiner, G.R.N.; Cairney, J. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 1995. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Mitchell, A.; Irvine, E.; Singer, J.; Williams, N.; Goodacre, R.; Tompkins, C. A new measure of health status for clinical trials in inflammatory bowel disease. Gastroenterology 1989, 96, 804–810. [Google Scholar] [CrossRef]
- Irvine, E.J.; Zhou, Q.; Thompson, A.K. The Short Inflammatory Bowel Disease Questionnaire: A quality of life instrument for community physicians managing inflammatory bowel disease. CCRPT Investigators. Canadian Crohn’s Relapse Prevention Trial. Am. J. Gastroenterol. 1996, 91, 1571–1578. [Google Scholar]
- Love, J.R.; Irvine, E.J.; Fedorak, R.N. Quality of life in inflammatory bowel disease. J. Clin. Gastroenterol. 1992, 14, 15–19. [Google Scholar] [CrossRef]
- Alcalá, M.J.; Casellas, F.; Fontanet, G.; Prieto, L.; Malagelada, J.-R. Shortened Questionnaire on Quality of Life for Inflammatory Bowel Disease. Inflamm. Bowel. Dis. 2004, 10, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Drossman, D.A.; Leserman, J.; Li, Z.M.; Mitchell, C.M.; Zagami, E.A.; Patrick, D.L. The rating form of IBD patient concerns: A new measure of health status. Psychosom. Med. 1991, 53, 701–712. [Google Scholar] [CrossRef]
- Farmer, R.G.; Easley, K.A.; Farmer, J.M. Quality of life assessment by patients with inflammatory bowel disease. Clevel. Clin. J. Med. 1992, 59, 35–42. [Google Scholar] [CrossRef]
- Martin, A.; Leone, L.; Fries, W.; Naccarato, R. Quality of life in inflammatory bowel disease. Ital. J. Gastroenterol. 1995, 27, 450. [Google Scholar]
- Fazio, V.W.; O’Riordain, M.G.; Lavery, I.C.; Church, J.M.; Lau, P.; Strong, S.A.; Hull, T. Long-term functional outcome and quality of life after stapled restorative proctocolectomy. Ann. Surg. 1999, 230, 575–584; discussion 584–586. [Google Scholar] [CrossRef] [PubMed]
- Kiran, R.P.; Delaney, C.P.; Senagore, A.J.; O’Brien-Ermlich, B.; Mascha, E.; Thornton, J.; Fazio, V.W. Prospective assessment of Cleveland Global Quality of Life (CGQL) as a novel marker of quality of life and disease activity in Crohn’s disease. Am. J. Gastroenterol. 2003, 98, 1783–1789. [Google Scholar] [CrossRef] [PubMed]
- Hjortswang, H.; Järnerot, G.; Curman, B.; Sandberg-Gertzén, H.; Tysk, C.; Blomberg, B.; Almer, S.; Ström, M. The Short Health Scale: A valid measure of subjective health in ulcerative colitis. Scand. J. Gastroenterol. 2006, 41, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.D.; Watson, R.; Palmer, K.R. Inflammatory bowel disease: Developing a short disease specific scale to measure health related quality of life. Int. J. Nurs. Stud. 2002, 39, 583–590. [Google Scholar] [CrossRef]
- Wilburn, J.; McKenna, S.P.; Twiss, J.; Kemp, K.; Campbell, S. Assessing quality of life in Crohn’s disease: Development and validation of the Crohn’s Life Impact Questionnaire (CLIQ). Qual. Life Res. 2015, 24, 2279–2288. [Google Scholar] [CrossRef]
- Alrubaiy, L.; Cheung, W.-Y.; Dodds, P.; Hutchings, H.A.; Russell, I.T.; Watkins, A.; Williams, J.G. Development of a Short Questionnaire to Assess the Quality of Life in Crohn’s Disease and Ulcerative Colitis. J. Crohn’s Colitis 2015, 9, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.-y.; Garratt, A.M.; Russell, I.T.; Williams, J.G. The UK IBDQ—A British version of the inflammatory bowel disease questionnaire: Development and validation. J. Clin. Epidemiol. 2000, 53, 297–306. [Google Scholar] [CrossRef]
- Allen, P.B.; Kamm, M.A.; Peyrin-Biroulet, L.; Studd, C.; Mc Dowell, C.; Allen, B.C.M.; Connell, W.R.; De Cruz, P.P.; Bell, S.J.; Elliot, R.P.; et al. Development and validation of a patient-reported disability measurement tool for patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 37, 438–444. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Cieza, A.; Sandborn, W.J.; Coenen, M.; Chowers, Y.; Hibi, T.; Kostanjsek, N.; Stucki, G.; Colombel, J.F. Development of the first disability index for inflammatory bowel disease based on the international classification of functioning, disability and health. Gut 2012, 61, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.J.; Netuveli, G.; Sleight, S.P.; Das, P.; Tekkis, P.P.; Gabe, S.M.; Clark, S.K.; Nicholls, R.J. Development of a social morbidity score in patients with chronic ulcerative colitis as a potential guide to treatment. Colorectal. Dis. 2012, 14, e250–e257. [Google Scholar] [CrossRef] [PubMed]
- Vergara, M.; Montserrat, A.; Casellas, F.; Gallardo, O.; Suarez, D.; Motos, J.; Villoria, A.; Miquel, M.; Martinez-Bauer, E.; Calvet, X. Development and validation of the Crohn’s disease perceived work disability questionnaire. Inflamm. Bowel. Dis. 2011, 17, 2350–2357. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, A.R.; Dragnev, M.C.C.; Darcey, C.J.; Siegel, C.A. A new tool to measure the burden of Crohn’s disease and its treatment: Do patient and physician perceptions match? Inflamm. Bowel. Dis. 2010, 16, 645–650. [Google Scholar] [CrossRef] [Green Version]
- Drossman, D.A.; Li, Z.; Leserman, J.; Patrick, D.L. Ulcerative colitis and Crohn’s disease health status scales for research and clinical practice. J. Clin. Gastroenterol. 1992, 15, 104–112. [Google Scholar] [CrossRef]
- Bodger, K.; Ormerod, C.; Shackcloth, D.; Harrison, M. Development and validation of a rapid, generic measure of disease control from the patient’s perspective: The IBD-control questionnaire. Gut 2014, 63, 1092–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mokkink, L.B.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de VEt, H.C.W.; Terwee, C.B. COSMIN Methodology for Systematic Reviews of Patient-Reported Outcome Measures (PROMS) User Manual; COSMIN: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [Green Version]
- International Consortium for Health Outcomes Measurement. Standard Sets. 2021. Available online: https://www.ichom.org/standard-sets/ (accessed on 24 March 2021).
- Irvine, E.J. Development and subsequent refinement of the inflammatory bowel disease questionnaire: A quality-of-life instrument for adult patients with inflammatory bowel disease. J. Pediatric Gastroenterol. Nutr. 1999, 28, S23–S27. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Louis, E.; Beaugerie, L.; Bossuyt, P.; Bouguen, G.; Bourreille, A.; Ferrante, M.; Franchimont, D.; Frost, K.; Hebuterne, X.; et al. Development of the IBD Disk: A Visual Self-administered Tool for Assessing Disability in Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2017, 23, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le Berre, C.; Flamant, M.; Bouguen, G.; Siproudhis, L.; Dewitte, M.; Dib, N.; Cesbron-Metivier, E.; Goronflot, T.; Hanf, M.; Gourraud, P.A.; et al. VALIDation of the IBD-Disk Instrument for Assessing Disability in Inflammatory Bowel Diseases in a French Cohort: The VALIDate Study. J. Crohn’s Colitis 2020, 14, 1512–1523. [Google Scholar] [CrossRef] [PubMed]
- van Andel, E.M.; Koopmann, B.D.M.; Crouwel, F.; Noomen, C.G.; de Boer, N.K.H.; van Asseldonk, D.P.; Mokkink, L.B. Systematic Review of Development and Content Validity of Patient-reported Outcome Measures in Inflammatory Bowel Disease: Do We Measure What We Measure? J. Crohn’s Colitis 2020, 14, 1299–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fletcher, J.; Cooper, S.C.; Swift, A. Patient-Reported Outcomes in Inflammatory Bowel Disease: A Measurement of Effect in Research and Clinical Care. Gastroenterol. Insights 2021, 12, 225-237. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12020020
Fletcher J, Cooper SC, Swift A. Patient-Reported Outcomes in Inflammatory Bowel Disease: A Measurement of Effect in Research and Clinical Care. Gastroenterology Insights. 2021; 12(2):225-237. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12020020
Chicago/Turabian StyleFletcher, Jane, Sheldon C. Cooper, and Amelia Swift. 2021. "Patient-Reported Outcomes in Inflammatory Bowel Disease: A Measurement of Effect in Research and Clinical Care" Gastroenterology Insights 12, no. 2: 225-237. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent12020020