
No Association of Early-Onset Breast or Ovarian Cancer with Early-Onset Cancer in Relatives in BRCA1 or BRCA2 Mutation Families


 , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Calculation of Number of BRCAm Carrier Women
2.4. Outcome Measures and Statistical Analysis
2.4.1. Families According to VEO Cancer
2.4.2. Cumulative VEO-BC and VEO-OC Risk
2.4.3. Mean Age at BC and OC Diagnosis in Relatives
2.4.4. Distribution of Age at BC and OC Diagnosis in Relatives
2.4.5. Relation between VEO-BC Occurrence and EO-BC in Relatives
3. Results
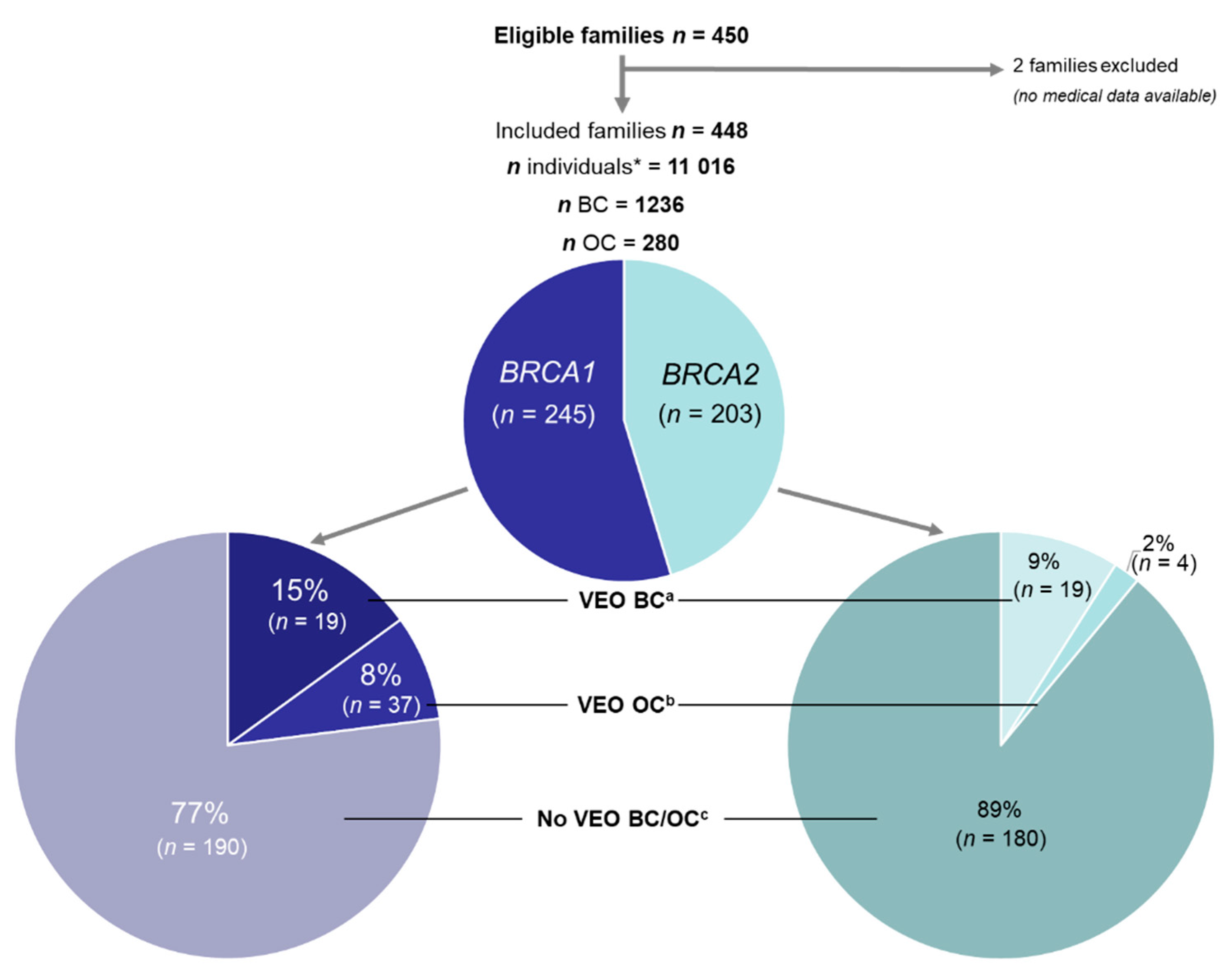
3.1. Study Population
3.2. VEO-BC and VEO-OC Families
3.3. Cumulative Risk of VEO-BC and VEO-OC
3.4. Age at BC and OC Diagnosis in Relatives of BRCAm Carrier Women with VEO-BC or VEO-OC
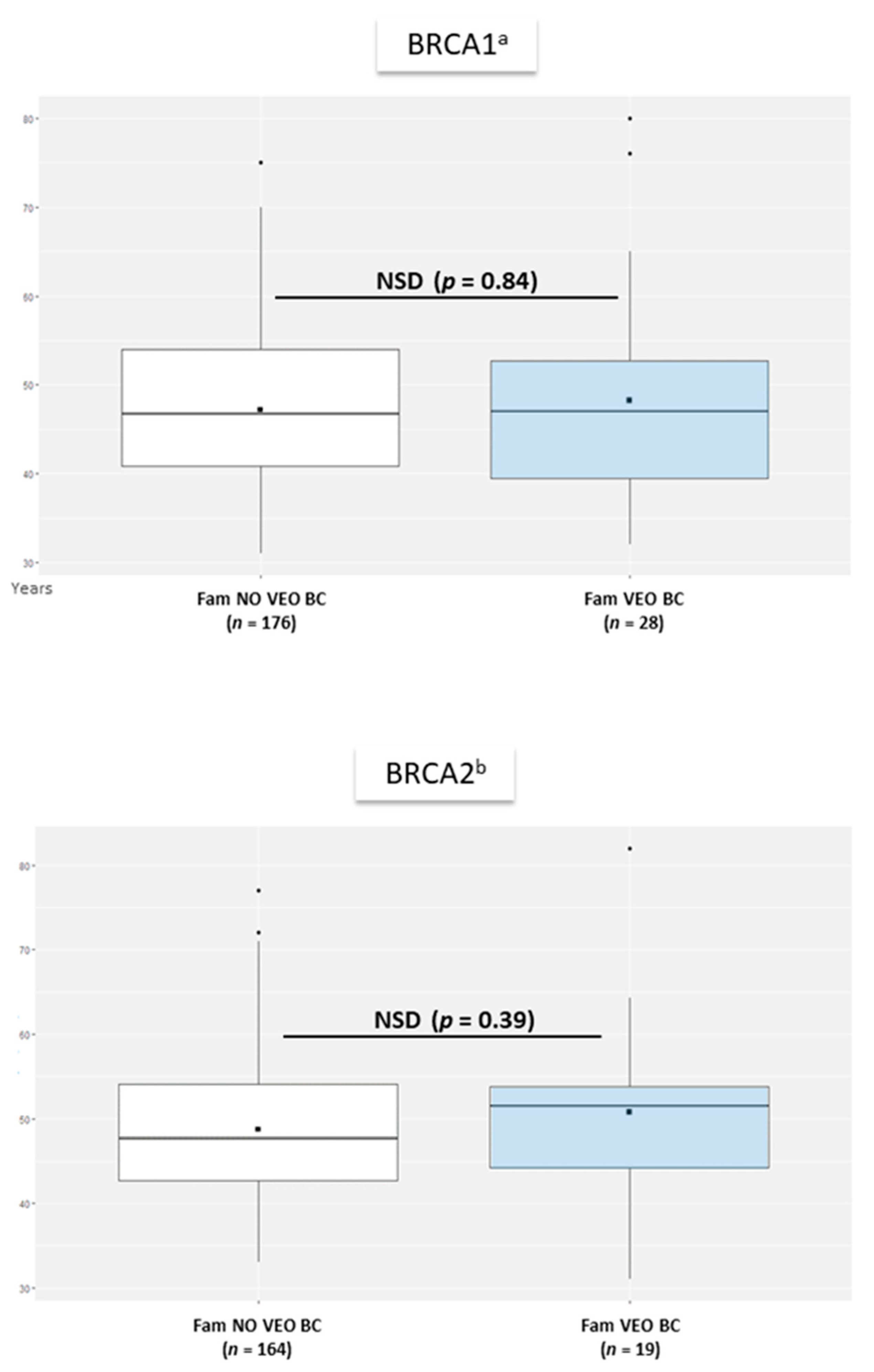
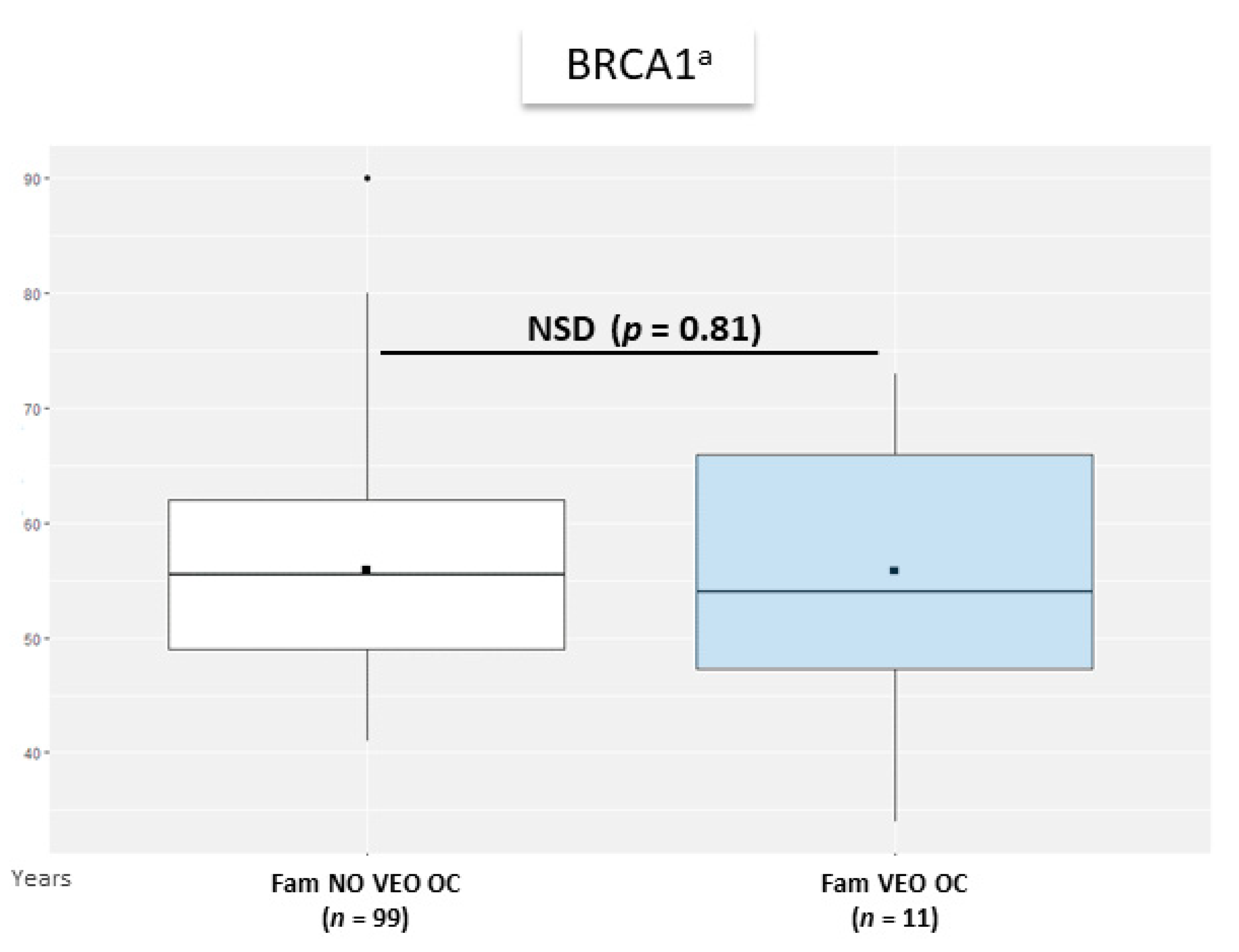
3.4.1. Mean Age at BC and OC Diagnosis in Relatives
3.4.2. Mixed-Effects Model
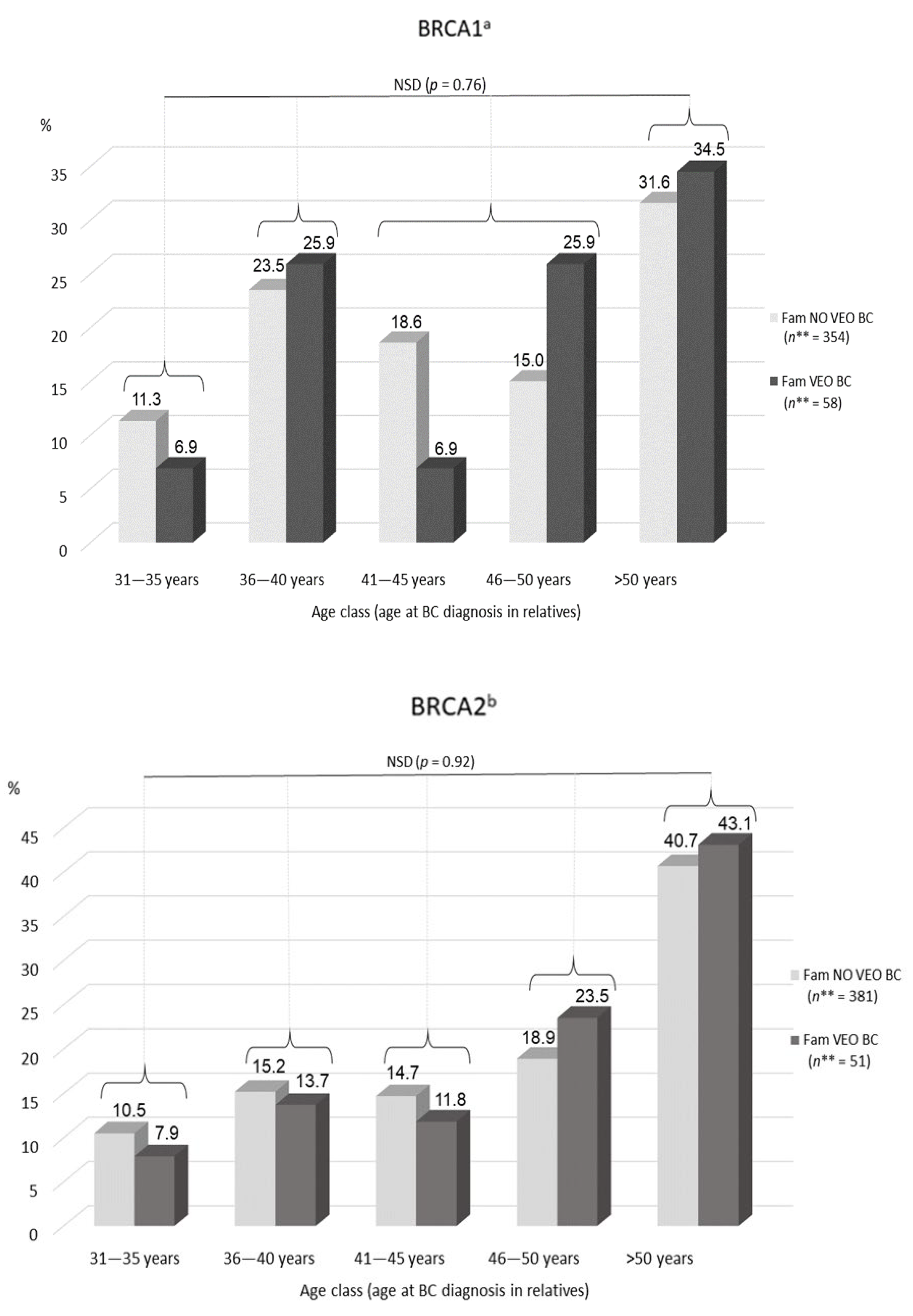
3.4.3. Distribution of Ages at BC and OC Diagnosis in Relatives
3.5. Relation between VEO-BC Occurrence and Early-Onset BC (EO-BC) in Relatives
3.5.1. Conditional Probability of VEO-BC by Occurrence of EO-BC
3.5.2. Association between EO Cancer Occurrence and Number of VEO Cancer Cases in the Family (Cochran–Mantel–Haenszel Model)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Women with BRCAm | women carrying a germline BRCA1 or BRCA2 pathogenic variant |
| BC | breast cancer |
| CI | confidence interval |
| EO | early-onset |
| ESMO | European Society for Medical Oncology |
| HR | hazard ratio |
| INCa | National Institute of Cancer (France) |
| NCCN | National Comprehensive Cancer Network (USA) |
| NICE | National Institute for Health and Care Excellence (UK) |
| OC | ovarian cancer |
| RR | relative risk |
| RRSO | risk-reducing salpingo-oophorectomy |
| VEO | very early-onset |
References
- Ford, D.; Easton, D.F.; Bishop, D.T.; Narod, S.A.; Goldgar, D.E. Risks of cancer in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Lancet 1994, 343, 692–695. [Google Scholar] [CrossRef]
- Ford, D.; Easton, D.F.; Stratton, M.; Narod, S.; Goldgar, D.; Devilee, P.; Bishop, D.T.; Weber, B.; Lenoir, G.; Chang-Claude, J.; et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. The Breast Cancer Linkage Consortium. Am. J. Hum. Genet. 1998, 62, 676–689. [Google Scholar] [CrossRef] [Green Version]
- Tavtigian, S.V.; Simard, J.; Rommens, J.; Couch, F.; Shattuck-Eidens, D.; Neuhausen, S.; Merajver, S.; Thorlacius, S.; Offit, K.; Stoppa-Lyonnet, D.; et al. The complete BRCA2 gene and mutations in chromosome 13q-linked kindreds. Nat. Genet. 1996, 12, 333–337. [Google Scholar] [CrossRef]
- Wooster, R.; Bignell, G.; Lancaster, J.; Swift, S.; Seal, S.; Mangion, J.; Collins, N.; Gregory, S.; Gumbs, C.; Micklem, G. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995, 378, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Eccles, D.; Marlow, A.; Royle, G.; Collins, A.; Morton, N.E. Genetic epidemiology of early onset breast cancer. J. Med. Genet. 1994, 31, 944–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, J.F.; Thompson, D.; Bobrow, L.; Dalal, N.; Gore, M.; Bishop, D.T.; Scott, I.; Evans, G.; Daly, P.; Easton, D.F.; et al. The genetic epidemiology of early-onset epithelial ovarian cancer: A population-based study. Am. J. Hum. Genet. 1999, 65, 1725–1732. [Google Scholar] [CrossRef] [Green Version]
- Easton, D.F.; Ford, D.; Bishop, D.T. Breast and ovarian cancer incidence in BRCA1-mutation carriers. Breast Cancer Linkage Consortium. Am. J. Hum. Genet. 1995, 56, 265–271. [Google Scholar]
- Antoniou, A.; Pharoah, P.D.P.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: A combined analysis of 22 studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Parmigiani, G. Meta-analysis of BRCA1 and BRCA2 penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.-A.; Mooij, T.M.; Roos-Blom, M.-J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavaddat, N.; Peock, S.; Frost, D.; Ellis, S.; Platte, R.; Fineberg, E.; Evans, D.G.; Izatt, L.; Eeles, R.A.; Adlard, J.; et al. Cancer risks for BRCA1 and BRCA2 mutation carriers: Results from prospective analysis of EMBRACE. J. Natl. Cancer Inst. 2013, 105, 812–822. [Google Scholar] [CrossRef] [Green Version]
- Doutriaux-Dumoulin, I. Suivi des patientes porteuses d’une mutation des gènes BRCA1 et 2: Recommandations de l’InCa 2017. Imagerie de la Femme 2018, 28, 6–18. [Google Scholar] [CrossRef]
- Daly, M.B.; Pilarski, R.; Axilbund, J.E.; Buys, S.S.; Crawford, B.; Friedman, S.; Garber, J.E.; Horton, C.; Kaklamani, V.; Klein, C.; et al. Genetic/familial high-risk assessment: Breast and ovarian, version 1.2014. J. Natl. Compr. Cancer Netw. 2014, 12, 1326–1338. [Google Scholar] [CrossRef] [PubMed]
- Paluch-Shimon, S.; Cardoso, F.; Sessa, C.; Balmana, J.; Cardoso, M.J.; Gilbert, F.; Senkus, E.; ESMO Guidelines Committee. Prevention and screening in BRCA mutation carriers and other breast/ovarian hereditary cancer syndromes: ESMO Clinical Practice Guidelines for cancer prevention and screening. Ann. Oncol. 2016, 27, v103–v110. [Google Scholar] [CrossRef]
- Tools and Resources. In Familial Breast Cancer: Classification, Care and Managing Breast Cancer and Related Risks in People with a Family History of Breast Cancer; Guidance, NICE; National Institute for Health and Care Excellence: London, UK, 2019.
- Corso, G.; Magnoni, F. Hereditary Breast Cancer: Translation into Clinical Practice of Recent American Society of Clinical Oncology, American Society of Radiation Oncology, and Society of Surgical Oncology Recommendations. Eur. J. Cancer Prev. 2021, 30, 311–314. [Google Scholar] [CrossRef]
- Tung, N.M.; Boughey, J.C.; Pierce, L.J.; Robson, M.E.; Bedrosian, I.; Dietz, J.R.; Dragun, A.; Gelpi, J.B.; Hofstatter, E.W.; Isaacs, C.J.; et al. Management of Hereditary Breast Cancer: American Society of Clinical Oncology, American Society for Radiation Oncology, and Society of Surgical Oncology Guideline. J. Clin. Oncol. 2020, 38, 2080–2106. [Google Scholar] [CrossRef]
- Metcalfe, K.; Lubinski, J.; Lynch, H.T.; Ghadirian, P.; Foulkes, W.D.; Kim-Sing, C.; Neuhausen, S.; Tung, N.; Rosen, B.; Gronwald, J.; et al. Family History of Cancer and Cancer Risks in Women with BRCA1 or BRCA2 Mutations. J. Natl. Cancer Inst. 2010, 102, 1874–1878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semple, J.; Metcalfe, K.A.; Lubinski, J.; Huzarski, T.; Gronwald, J.; Armel, S.; Lynch, H.T.; Karlan, B.; Foulkes, W.; Singer, C.F.; et al. Does the age of breast cancer diagnosis in first-degree relatives impact on the risk of breast cancer in BRCA1 and BRCA2 mutation carriers? Breast Cancer Res. Treat. 2015, 154, 163–169. [Google Scholar] [CrossRef]
- Tilanus-Linthorst, M.M.A.; Lingsma, H.F.; Gareth Evans, D.; Thompson, D.; Kaas, R.; Manders, P.; van Asperen, C.J.; Adank, M.; Hooning, M.J.; Kwan Lim, G.E.; et al. Optimal age to start preventive measures in women with BRCA1/2 mutations or high familial breast cancer risk. Int. J. Cancer 2013, 133, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Panchal, S.; Bordeleau, L.; Poll, A.; Llacuachaqui, M.; Shachar, O.; Ainsworth, P.; Armel, S.; Eisen, A.; Sun, P.; Narod, S.A. Does family history predict the age at onset of new breast cancers in BRCA1 and BRCA2 mutation-positive families? Clin. Genet. 2010, 77, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.M. Factors Associated with Early Versus Late Development of Breast and Ovarian Cancer in BRCA1 and BRCA2 Positive Women; The Texas Medical Center Library: Houston, TX, USA, 2010. [Google Scholar]
- Soegaard, M.; Frederiksen, K.; Jensen, A.; Høgdall, E.; Høgdall, C.; Blaakaer, J.; Ramus, S.J.; Gayther, S.A.; Kjaer, S.K. Risk of ovarian cancer in women with first-degree relatives with cancer. Acta Obstet. Gynecol. Scand. 2009, 88, 449–456. [Google Scholar] [CrossRef]
- Stratton, J.F.; Pharoah, P.; Smith, S.K.; Easton, D.; Ponder, B.A. A systematic review and meta-analysis of family history and risk of ovarian cancer. Br. J. Obstet. Gynaecol. 1998, 105, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Pharoah, P.D.; Day, N.E.; Duffy, S.; Easton, D.F.; Ponder, B.A. Family history and the risk of breast cancer: A systematic review and meta-analysis. Int. J. Cancer 1997, 71, 800–809. [Google Scholar] [CrossRef]
- Begg, C.B.; Haile, R.W.; Borg, Å.; Malone, K.E.; Concannon, P.; Thomas, D.C.; Langholz, B.; Bernstein, L.; Olsen, J.H.; Lynch, C.F.; et al. Variation of Breast Cancer Risk Among BRCA1/2 Carriers. JAMA 2008, 299, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, D.; Easton, D.; Breast Cancer Linkage Consortium. Variation in BRCA1 cancer risks by mutation position. Cancer Epidemiol. Biomark. Prev. 2002, 11, 329–336. [Google Scholar]
- Thompson, D.; Easton, D.F. Cancer Incidence in BRCA1 Mutation Carriers. Obstet. Gynecol. Surv. 2003, 58, 27–28. [Google Scholar] [CrossRef] [Green Version]
- Rebbeck, T.R.; Mitra, N.; Wan, F.; Sinilnikova, O.M.; Healey, S.; McGuffog, L.; Mazoyer, S.; Chenevix-Trench, G.; Easton, D.F.; Antoniou, A.C.; et al. Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. JAMA 2015, 313, 1347–1361. [Google Scholar] [CrossRef] [Green Version]
- Lesueur, F.; Mebirouk, N.; Jiao, Y.; Barjhoux, L.; Belotti, M.; Laurent, M.; Léone, M.; Houdayer, C.; Paillerets, B.B.; Vaur, D.; et al. GEMO, a National Resource to Study Genetic Modifiers of Breast and Ovarian Cancer Risk in BRCA1 and BRCA2 Pathogenic Variant Carriers. Front. Oncol. 2018, 8, 490. [Google Scholar] [CrossRef]
- Pujol, P.; Lyonnet, D.S.; Frebourg, T.; Blin, J.; Picot, M.C.; Lasset, C.; Dugast, C.; Berthet, P.; de Paillerets, B.B.; Sobol, H.; et al. Lack of referral for genetic counseling and testing in BRCA1/2 and Lynch syndromes: A nationwide study based on 240,134 consultations and 134,652 genetic tests. Breast Cancer Res. Treat. 2013, 141, 135–144. [Google Scholar] [CrossRef]
- Thompson, D.; Easton, D.; Breast Cancer Linkage Consortium. Variation in cancer risks, by mutation position, in BRCA2 mutation carriers. Am. J. Hum. Genet. 2001, 68, 410–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, R. Hereditary Breast and Ovarian Cancer (HBOC): Review of Its Molecular Characteristics, Screening, Treatment, and Prognosis. Breast Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Angulo, A.M.; Timms, K.M.; Liu, S.; Chen, H.; Litton, J.K.; Potter, J.; Lanchbury, J.S.; Stemke-Hale, K.; Hennessy, B.T.; Arun, B.K.; et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin. Cancer Res. 2011, 17, 1082–1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubalek, M.; Czech, T.; Müller, H. Biological Subtypes of Triple-Negative Breast Cancer. Breast Care 2017, 12, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fackenthal, J.D.; Olopade, O.I. Breast cancer risk associated with BRCA1 and BRCA2 in diverse populations. Nat. Rev. Cancer 2007, 7, 937–948. [Google Scholar] [CrossRef]
- Tun, N.M.; Villani, G.; Ong, K.; Yoe, L.; Bo, Z.M. Risk of having BRCA1 mutation in high-risk women with triple-negative breast cancer: A meta-analysis. Clin. Genet. 2014, 85, 43–48. [Google Scholar] [CrossRef]
- Podo, F.; Santoro, F.; Di Leo, G.; Manoukian, S.; de Giacomi, C.; Corcione, S.; Cortesi, L.; Carbonaro, L.A.; Trimboli, R.M.; Cilotti, A.; et al. Triple-Negative versus Non-Triple-Negative Breast Cancers in High-Risk Women: Phenotype Features and Survival from the HIBCRIT-1 MRI-Including Screening Study. Clin. Cancer Res. 2016, 22, 895–904. [Google Scholar] [CrossRef] [Green Version]
- Dogan, B.E.; Turnbull, L.W. Imaging of triple-negative breast cancer. Ann. Oncol. 2012, 23 (Suppl. S6), vi23–vi29. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-negative breast cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [Green Version]
- Dawson, S.J.; Provenzano, E.; Caldas, C. Triple negative breast cancers: Clinical and prognostic implications. Eur. J. Cancer 2009, 45, 27–40. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef] [Green Version]
- Noda, S.; Onoda, N.; Morisaki, T.; Kashiwagi, S.; Takashima, T.; Hirakawa, K. The significance and the predictive factors of microscopic lymph node metastasis in patients with clinically node negative papillary thyroid cancer: A retrospective cohort study. Int. J. Surg. 2015, 20, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Phi, X.-A.; Houssami, N.; Obdeijn, I.-M.; Warner, E.; Sardanelli, F.; Leach, M.O.; Riedl, C.C.; Trop, I.; Tilanus-Linthorst, M.M.A.; Mandel, R.; et al. Magnetic Resonance Imaging Improves Breast Screening Sensitivity in BRCA Mutation Carriers Age ≥ 50 Years: Evidence From an Individual Patient Data Meta-Analysis. J. Clin. Oncol. 2015, 33, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Phi, X.-A.; Saadatmand, S.; De Bock, G.H.; Warner, E.; Sardanelli, F.; Leach, M.O.; Riedl, C.C.; Trop, I.; Hooning, M.J.; Mandel, R.; et al. Contribution of mammography to MRI screening in BRCA mutation carriers by BRCA status and age: Individual patient data meta-analysis. Br. J. Cancer 2016, 114, 631–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riedl, C.C.; Luft, N.; Bernhart, C.; Weber, M.; Bernathova, M.; Tea, M.-K.M.; Rudas, M.; Singer, C.F.; Helbich, T.H. Triple-modality screening trial for familial breast cancer underlines the importance of magnetic resonance imaging and questions the role of mammography and ultrasound regardless of patient mutation status, age, and breast density. J. Clin. Oncol. 2015, 33, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.; Eisen, A.; Senter, L.; Armel, S.; Bordeleau, L.; Meschino, W.S.; Pal, T.; Lynch, H.T.; Tung, N.M.; Kwong, A.; et al. International trends in the uptake of cancer risk reduction strategies in women with a BRCA1 or BRCA2 mutation. Br. J. Cancer 2019. [Google Scholar] [CrossRef] [Green Version]
- Julian-Reynier, C.; Mancini, J.; Mouret-Fourme, E.; Gauthier-Villars, M.; Bonadona, V.; Berthet, P.; Fricker, J.-P.; Caron, O.; Luporsi, E.; Noguès, C. Cancer risk management strategies and perceptions of unaffected women 5 years after predictive genetic testing for BRCA1/2 mutations. Eur. J. Hum. Genet. 2011, 19, 500–506. [Google Scholar] [CrossRef]
- Metcalfe, K.A.; Birenbaum-Carmeli, D.; Lubinski, J.; Gronwald, J.; Lynch, H.; Moller, P.; Ghadirian, P.; Foulkes, W.D.; Klijn, J.; Friedman, E.; et al. International variation in rates of uptake of preventive options in BRCA1 and BRCA2 mutation carriers. Int. J. Cancer 2008, 122, 2017–2022. [Google Scholar] [CrossRef] [Green Version]
- de Bock, G.H.; Vermeulen, K.M.; Jansen, L.; Oosterwijk, J.C.; Siesling, S.; Dorrius, M.D.; Feenstra, T.; Houssami, N.; Greuter, M.J.W. Which screening strategy should be offered to women with BRCA1 or BRCA2 mutations? A simulation of comparative cost-effectiveness. Br. J. Cancer 2013, 108, 1579–1586. [Google Scholar] [CrossRef] [Green Version]
- Pataky, R.; Armstrong, L.; Chia, S.; Coldman, A.J.; Kim-Sing, C.; McGillivray, B.; Scott, J.; Wilson, C.M.; Peacock, S. Cost-effectiveness of MRI for breast cancer screening in BRCA1/2 mutation carriers. BMC Cancer 2013, 13, 339. [Google Scholar] [CrossRef] [Green Version]
- Petelin, L.; Trainer, A.H.; Mitchell, G.; Liew, D.; James, P.A. Cost-effectiveness and comparative effectiveness of cancer risk management strategies in BRCA1/2 mutation carriers: A systematic review. Genet. Med. 2018, 20, 1145–1156. [Google Scholar] [CrossRef] [Green Version]
- Finch, A.P.M.; Lubinski, J.; Møller, P.; Singer, C.F.; Karlan, B.; Senter, L.; Rosen, B.; Maehle, L.; Ghadirian, P.; Cybulski, C.; et al. Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J. Clin. Oncol. 2014, 32, 1547–1553. [Google Scholar] [CrossRef] [Green Version]
- Podfigurna-Stopa, A.; Czyzyk, A.; Grymowicz, M.; Smolarczyk, R.; Katulski, K.; Czajkowski, K.; Meczekalski, B. Premature ovarian insufficiency: The context of long-term effects. J. Endocrinol. Investig. 2016, 39, 983–990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchetti, C.; De Felice, F.; Palaia, I.; Perniola, G.; Musella, A.; Musio, D.; Muzii, L.; Tombolini, V.; Panici, P.B. Risk-reducing salpingo-oophorectomy: A meta-analysis on impact on ovarian cancer risk and all cause mortality in BRCA 1 and BRCA 2 mutation carriers. BMC Women’s Health 2014, 14, 150. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Kauff, N.D.; Domchek, S.M. Meta-analysis of Risk Reduction Estimates Associated with Risk-Reducing Salpingo-oophorectomy in BRCA1 or BRCA2 Mutation Carriers. J. Natl. Cancer Inst. 2009, 101, 80–87. [Google Scholar] [CrossRef]
- Singer, C.F.; Tea, M.K.; Pristauz, G.; Hubalek, M.; Rappaport, C.; Riedl, C.C.; Helbich, T.H. Clinical Practice Guideline for the prevention and early detection of breast and ovarian cancer in women from HBOC (hereditary breast and ovarian cancer) families. Wien. Klin. Wochenschr. 2015, 127, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Mancini, J.; Mouret-Fourme, E.; Noguès, C.; Julian-Reynier, C. Impact of BRCA1/2 mutation on young women’s 5-year parenthood rates: A prospective comparative study (GENEPSO-PS cohort). Fam. Cancer 2015, 14, 273–279. [Google Scholar] [CrossRef]
- Chan, J.; Johnson, L.N.; DiGiovanni, L.; Voong, C.; Sammel, M.D.; Domchek, S.M.; Gracia, C. Reproductive decision-making in patients diagnosed with BRCA mutations. Fertil. Steril. 2015, 104, e76. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Mangili, G.; Bergamini, A.; Filippi, F.; Martinelli, F.; Ferrari, F.; Noli, S.; Rabaiotti, E.; Candiani, M.; Somigliana, E. Fertility preservation in women harboring deleterious BRCA mutations: Ready for prime time? Hum. Reprod. 2018, 33, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Gammon, M.D.; Skrzynia, C.; Mersereau, J.E. BRCA mutation carriers: A new target population for fertility preservation consultation and treatment. Fertil. Steril. 2013, 100, S190. [Google Scholar] [CrossRef]
- Gunnala, V.; Fields, J.; Irani, M.; D’Angelo, D.; Xu, K.; Schattman, G.; Rosenwaks, Z. BRCA carriers have similar reproductive potential at baseline to noncarriers: Comparisons in cancer and cancer-free cohorts undergoing fertility preservation. Fertil. Steril. 2019, 111, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Grynberg, M.; Raad, J.; Comtet, M.; Vinolas, C.; Cédrin-Durnerin, I.; Sonigo, C. Fertility preservation in BRCA-mutated women: When and how? Future Oncol. 2018, 14, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Milne, R.L.; Antoniou, A.C. Modifiers of breast and ovarian cancer risks for BRCA1 and BRCA2 mutation carriers. Endocr. Relat. Cancer 2016, 23, T69–T84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osorio, A.; Milne, R.L.; Pita, G.; Peterlongo, P.; Heikkinen, T.; Simard, J.; Chenevix-Trench, G.; Spurdle, A.B.; Beesley, J.; Chen, X.; et al. Evaluation of a candidate breast cancer associated SNP in ERCC4 as a risk modifier in BRCA1 and BRCA2 mutation carriers. Results from the Consortium of Investigators of Modifiers of BRCA1/BRCA2 (CIMBA). Br. J. Cancer 2009, 101, 2048–2054. [Google Scholar] [CrossRef] [Green Version]
- Mulligan, A.M.; Couch, F.J.; Barrowdale, D.; Domchek, S.M.; Eccles, D.; Nevanlinna, H.; Ramus, S.J.; Robson, M.; Sherman, M.; Spurdle, A.B.; et al. Common breast cancer susceptibility alleles are associated with tumour subtypes in BRCA1 and BRCA2 mutation carriers: Results from the Consortium of Investigators of Modifiers of BRCA1/2. Breast Cancer Res. 2011, 13, R110. [Google Scholar] [CrossRef] [Green Version]
- Antoniou, A.C.; Kartsonaki, C.; Sinilnikova, O.M.; Soucy, P.; McGuffog, L.; Healey, S.; Lee, A.; Peterlongo, P.; Manoukian, S.; Peissel, B.; et al. Common alleles at 6q25.1 and 1p11.2 are associated with breast cancer risk for BRCA1 and BRCA2 mutation carriers. Hum. Mol. Genet. 2011, 20, 3304–3321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bugrein, H. Genotype and phenotype correlation of breast cancer in BRCA carriers and non-carriers. J. Cancer Sci. Ther. 2015, 07, HBPP1674. [Google Scholar] [CrossRef]
- Bujassoum, S.M.; Bugrein, H.A.; Al Sulaiman, R. Genotype and Phenotype Correlation of Breast Cancer in BRCA Mutation Carriers and Non-Carriers. J. Cancer Sci. Ther. 2017, 9. [Google Scholar] [CrossRef]
- Lecarpentier, J.; Noguès, C.; Mouret-Fourme, E.; Buecher, B.; Gauthier-Villars, M.; Stoppa-Lyonnet, D.; Bonadona, V.; Fricker, J.-P.; Berthet, P.; Caron, O.; et al. Breast Cancer Risk Associated with Estrogen Exposure and Truncating Mutation Location in BRCA1/2 Carriers. Cancer Epidemiol. Biomark. Prev. 2015, 24, 698–707. [Google Scholar] [CrossRef] [Green Version]
- Andrieu, N.; Easton, D.F.; Chang-Claude, J.; Rookus, M.A.; Brohet, R.; Cardis, E.; Antoniou, A.C.; Wagner, T.; Simard, J.; Evans, G.; et al. Effect of chest X-rays on the risk of breast cancer among BRCA1/2 mutation carriers in the international BRCA1/2 carrier cohort study: A report from the EMBRACE, GENEPSO, GEO-HEBON, and IBCCS Collaborators’ Group. J. Clin. Oncol. 2006, 24, 3361–3366. [Google Scholar] [CrossRef] [Green Version]
- Narod, S.A. Modifiers of risk of hereditary breast cancer. Oncogene 2006, 25, 5832–5836. [Google Scholar] [CrossRef] [Green Version]
- Friebel, T.M.; Domchek, S.M.; Rebbeck, T.R. Modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers: Systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju091. [Google Scholar] [CrossRef] [Green Version]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.-H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, D.R.; Rookus, M.A.; McGuffog, L.; Leslie, G.; Mooij, T.M.; Dennis, J.; Mavaddat, N.; Adlard, J.; Ahmed, M.; Aittomäki, K.; et al. Polygenic risk scores and breast and epithelial ovarian cancer risks for carriers of BRCA1 and BRCA2 pathogenic variants. Genet. Med. 2020, 22, 1653–1666. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.; Hughes, E.; Wagner, S.; Tshiaba, P.; Rosenthal, E.; Roa, B.B.; Kurian, A.W.; Domchek, S.M.; Garber, J.; Lancaster, J.; et al. Association of a Polygenic Risk Score with Breast Cancer Among Women Carriers of High- and Moderate-Risk Breast Cancer Genes. JAMA Netw. Open 2020, 3, e208501. [Google Scholar] [CrossRef] [PubMed]
- Mars, N.; Koskela, J.T.; Ripatti, P.; Kiiskinen, T.T.J.; Havulinna, A.S.; Lindbohm, J.V.; Ahola-Olli, A.; Kurki, M.; Karjalainen, J.; Palta, P.; et al. Polygenic and clinical risk scores and their impact on age at onset and prediction of cardiometabolic diseases and common cancers. Nat. Med. 2020, 26, 549–557. [Google Scholar] [CrossRef]
- Levy, D.E.; Garber, J.E.; Shields, A.E. Guidelines for genetic risk assessment of hereditary breast and ovarian cancer: Early disagreements and low utilization. J. Gen. Intern. Med. 2009, 24, 822–828. [Google Scholar] [CrossRef] [Green Version]
- George, A.; Kaye, S.; Banerjee, S. Delivering widespread BRCA testing and PARP inhibition to patients with ovarian cancer. Nat. Rev. Clin. Oncol. 2017, 14, 284–296. [Google Scholar] [CrossRef]
- U.S. Breast Cancer Statistics. Breastcancer.org. Available online: https://www.breastcancer.org/symptoms/understand_bc/statistics (accessed on 11 May 2019).
- Institut National Du Cancer Epidémiologie des Cancers—Les chiffres du Cancer en France. Available online: https://www.e-cancer.fr/Professionnels-de-sante/Les-chiffres-du-cancer-en-France/Epidemiologie-des-cancers (accessed on 11 May 2019).
- Pearce, N. Classification of epidemiological study designs. Int. J. Epidemiol. 2012, 41, 393–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kass, P.H. Modern Epidemiological Study Designs. In Handbook of Epidemiology; Springer: Berlin/Heidelberg, Germany, 2014; pp. 325–363. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cumulative Prevalence (95% CI) | Comparative Data from Literature: Range of Previously Published Cumulative Incidence of VEO Cancer | |
|---|---|---|
| VEO BC | ||
| BRCA1 a | 5.1% (3.6–6.6) | 0.7–8.7% * |
| BRCA2 b | 2.5% (2.4–3.6) | 0.0–4.8% * |
| VEO OC | ||
| BRCA1 a | 2.7% (1.6–3.8) | 1.1–2.3% * |
| BRCA2 b | 0.5% (0.01–1.0) | 0.1–1.7% * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imbert-Bouteille, M.; Corsini, C.; Picot, M.-C.; Mizrahy, L.; Akouete, S.; Huguet, H.; Thomas, F.; Geneviève, D.; Taourel, P.; Ychou, M.; et al. No Association of Early-Onset Breast or Ovarian Cancer with Early-Onset Cancer in Relatives in BRCA1 or BRCA2 Mutation Families. Genes 2021, 12, 1100. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071100
Imbert-Bouteille M, Corsini C, Picot M-C, Mizrahy L, Akouete S, Huguet H, Thomas F, Geneviève D, Taourel P, Ychou M, et al. No Association of Early-Onset Breast or Ovarian Cancer with Early-Onset Cancer in Relatives in BRCA1 or BRCA2 Mutation Families. Genes. 2021; 12(7):1100. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071100
Chicago/Turabian StyleImbert-Bouteille, Marion, Carole Corsini, Marie-Christine Picot, Lucas Mizrahy, Sandrine Akouete, Helena Huguet, Frédéric Thomas, David Geneviève, Patrice Taourel, Marc Ychou, and et al. 2021. "No Association of Early-Onset Breast or Ovarian Cancer with Early-Onset Cancer in Relatives in BRCA1 or BRCA2 Mutation Families" Genes 12, no. 7: 1100. https://0-doi-org.brum.beds.ac.uk/10.3390/genes12071100