Effect of Exercise Training on Body Temperature in the Elderly: A Retrospective Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Evaluation of Body Temperature and Body Composition
2.3. Exercise Protocol
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Body Temperature Variation
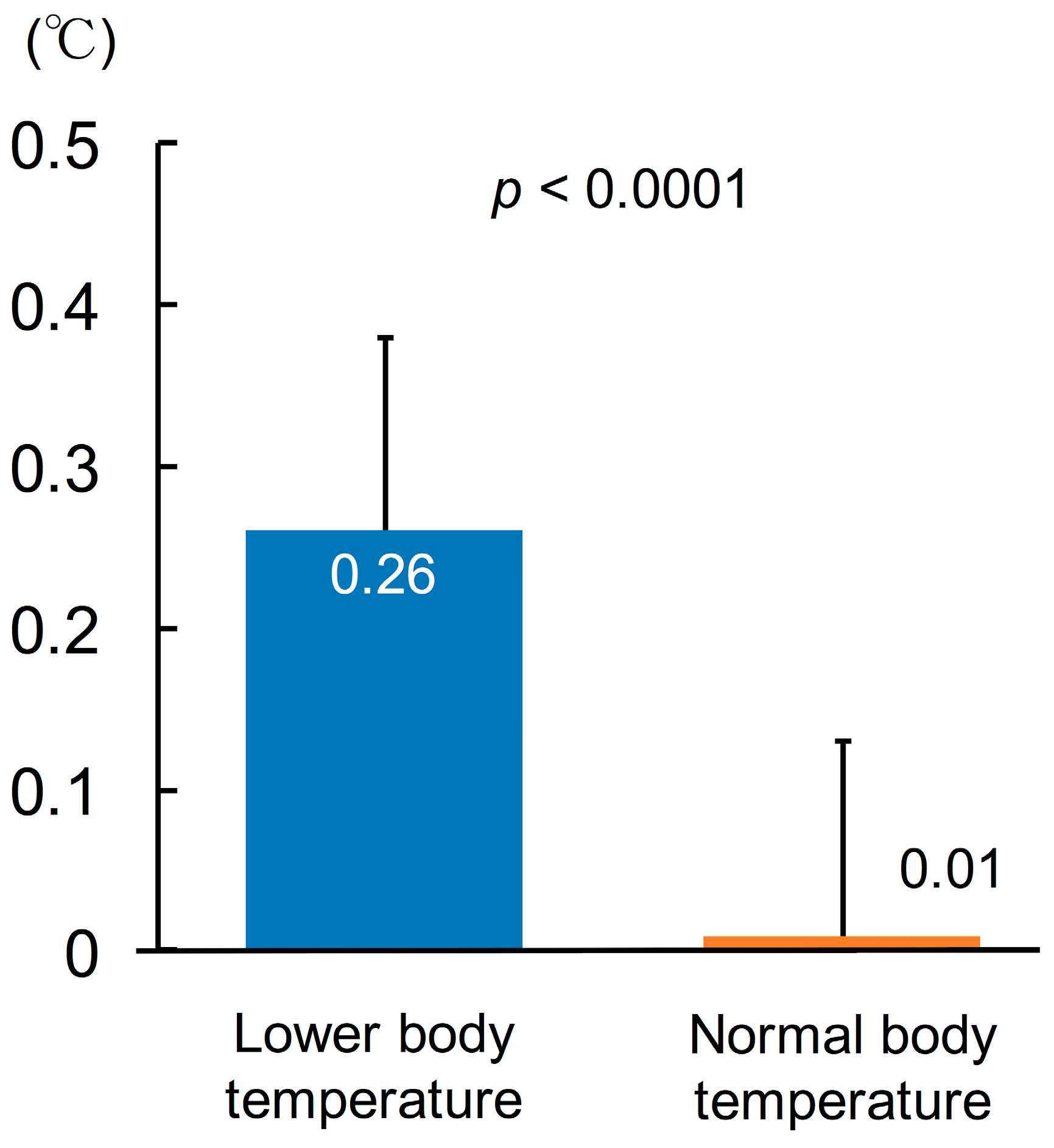
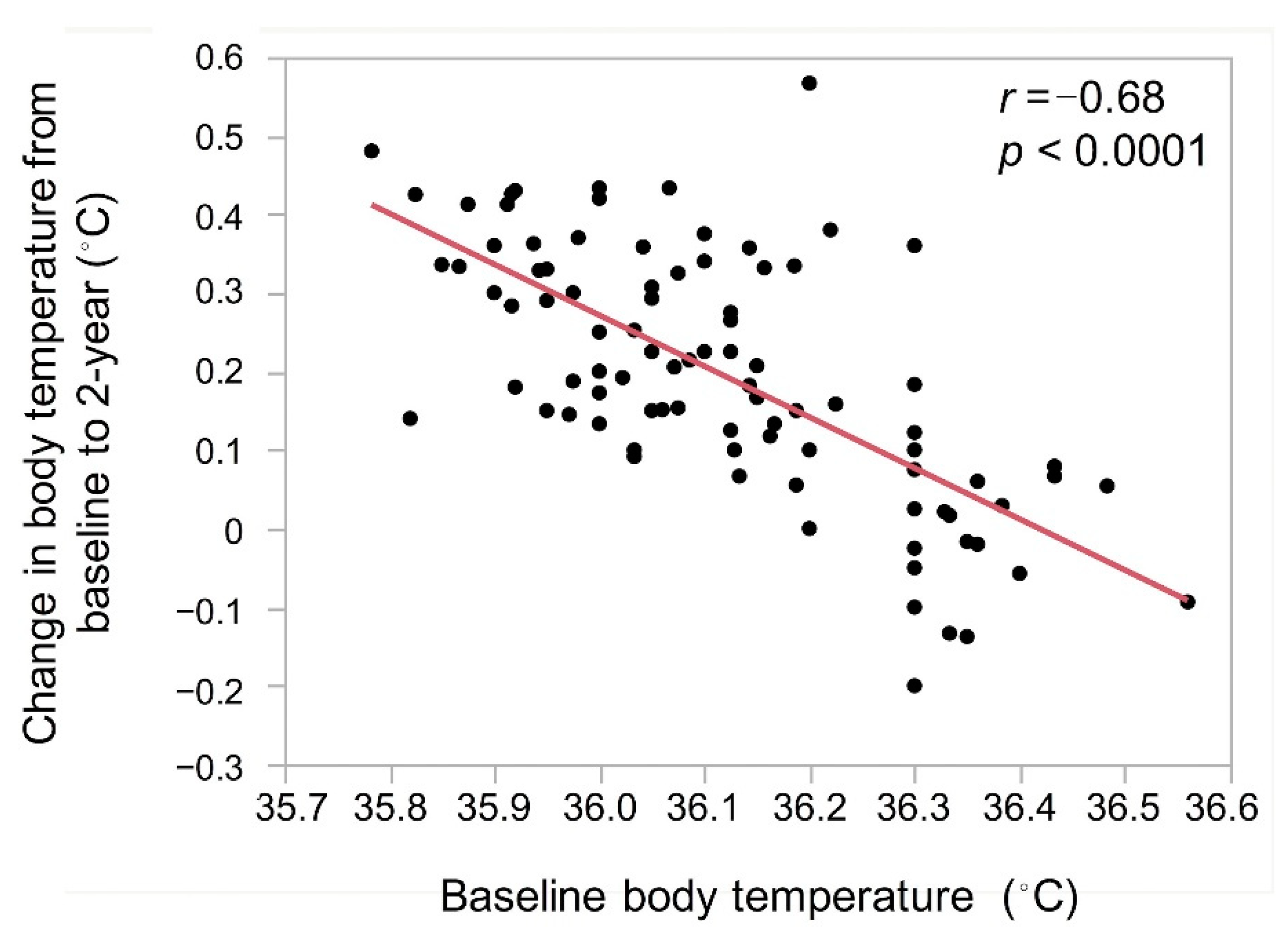
3.3. Change in Body Temperature
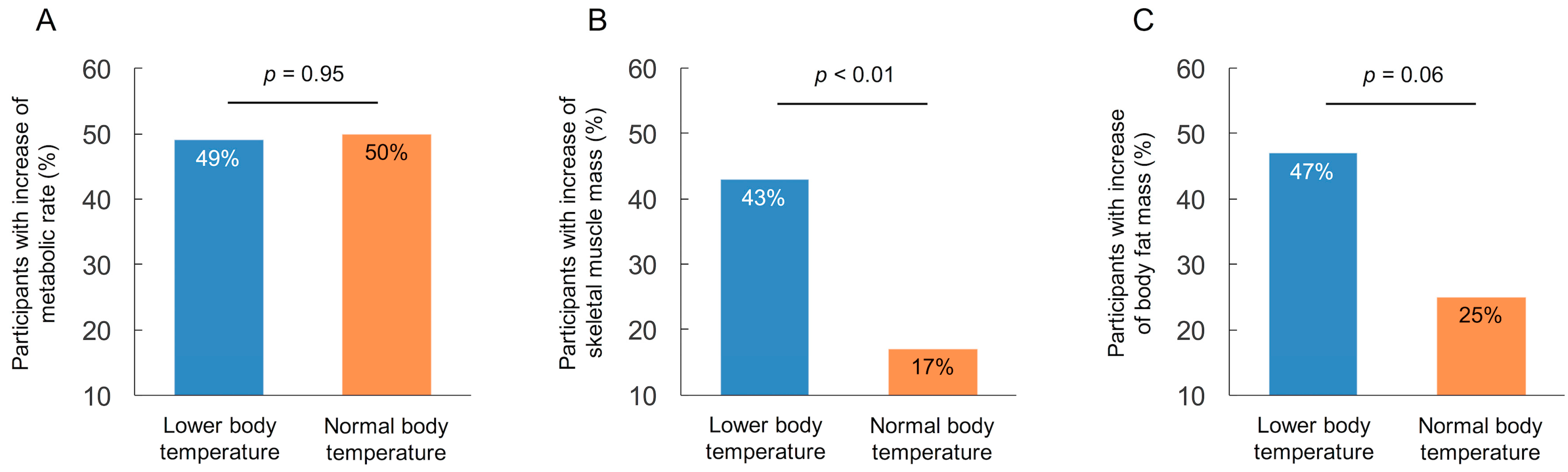
3.4. Relationship between Body Temperature and Change in Body Composition
3.5. Relationship between Status of Activity of Daily Living and Body Composition and Body Temperature
3.6. Variable Related to the Rise in Body Temperature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waalen, J.; Buxbaum, J.N. Is older colder or colder older? The association of age with body temperature in 18,630 individuals. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66A, 487–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rising, R.; Keys, A.; Ravussin, E.; Bogardus, C. Concomitant interindividual variation in body temperature and metabolic rate. Am. J. Physiol. 1992, 263, E730–E734. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Verdejo, R.; Marlatt, K.L.; Ravussin, E.; Galgani, J.E. Contribution of brown adipose tissue to human energy metabolism. Mol. Asp. Med. 2019, 68, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, M.; Okazaki, K.; Inoue, Y. Aging and thermoregulation. J. Phys. Fit. Sports Med. 2013, 2, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Mace, T.A.; Zhong, L.; Kilpatrick, C.; Zynda, E.; Lee, C.T.; Capitano, M.; Minderman, H.; Repasky, E.A. Differentiation of CD8+ T cells into effector cells is enhanced by physiological range hyperthermia. J. Leukoc. Biol. 2011, 90, 951–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foxman, E.F.; Storer, J.A.; Fitzgerald, M.E.; Wasik, B.R.; Hou, L.; Zhao, H.; Turner, P.E.; Pyle, A.M.; Iwasaki, A. Temperature-dependent innate defense against the common cold virus limits viral replication at warm temperature in mouse airway cells. Proc. Natl. Acad. Sci. USA 2015, 112, 827–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foxman, E.F.; Storer, J.A.; Vanaja, K. Two interferon-independent double-stranded RNA-induced host defense strategies suppress the common cold virus at warm temperature. Proc. Natl. Acad. Sci. USA 2016, 113, 8496–8501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagawa, Y.; Tanigawa, K.; Kobayashi, Y.; Yamamoto, M. Cancer immunity and therapy using hyperthermia with immunotherapy, radiotherapy, chemotherapy, and surgery. J. Cancer Metastasis Treat. 2017, 3, 218–230. [Google Scholar] [CrossRef]
- Harper, C.V.; Woodcock, D.J.; Lam, C.; Garcia-Albornoz, M.; Adamson, A.; Ashall, L.; Rowe, W.; Downton, P.; Schmidt, L.; West, S.; et al. Temperature regulates NF-kappaB dynamics and function through timing of A20 transcription. Proc. Natl. Acad. Sci. USA 2018, 115, E5243–E5249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between dual-energy x-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conraads, V.M.; Vanderheyden, M.; Paelinck, B.; Verstreken, S.; Blankoff, I.; Miljoen, H.; De Sutter, J.; Beckers, P. The effect of endurance training on exercise capacity following cardiac resynchronization therapy in chronic heart failure patients: A pilot trial. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Conraads, V.; Corrà, U.; Dickstein, K.; Francis, D.P.; Jaarsma, T.; McMurray, J.; Pieske, B.; Piotrowicz, E.; Schmid, J.P.; et al. Exercise training in heart failure: From theory to practice. A consensus document of the Heart Failure Association and the European Association for Cardiovascular Prevention and Rehabilitation. Eur. J. Heart Fail. 2011, 4, 347–357. [Google Scholar] [CrossRef]
- Lim, C.L.; Byrne, C.; Lee, J.K. Human thermoregulation and measurement of body temperature in exercise and clinical settings. Ann. Acad. Med. Singap. 2008, 37, 347–353. [Google Scholar] [PubMed]
- Poehlman, E.T.; Berke, E.M.; Joseph, J.R.; Gardner, A.W.; Katzman-Rooks, S.M.; Goran, M.I. Influence of aerobic capacity, body composition, and thyroid hormones on the age-related decline in resting metabolic rate. Metab. Clin. Exp. 1992, 41, 915–921. [Google Scholar] [CrossRef]
- Atkinson, G.; Coldwells, A.; Reilly, T.; Waterhouse, J. A comparison of circadian rhythms in work performance between physically active and inactive subjects. Ergonomics 1993, 36, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2 (2019) Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower Body Temperature (n = 67) | Normal Body Temperature (n = 24) | p Value | |
|---|---|---|---|
| Age (years) | 81.3 ± 4.5 | 80.5 ± 3.6 | 0.49 |
| Male | 24 (36) | 8 (33) | 0.83 |
| Body temperature (°C) | 36.0 ± 0.1 | 36.4 ± 0.1 | <0.0001 |
| Comorbidity | |||
| Hypertension | 18 (27) | 5 (21) | 0.56 |
| Diabetes mellitus | 9 (13) | 2 (8) | 0.51 |
| Orthopedic disease | 35 (52) | 14 (58) | 0.61 |
| Previous cerebral infarction | 5 (7) | 1 (4) | 0.58 |
| Activity of daily living | 0.70 | ||
| Independent outdoor walking | 37 (55) | 13 (54) | |
| Independent indoor walking | 12 (18) | 6 (25) | |
| Indoor walking with assistance | 18 (27) | 5 (21) | |
| Body composition | |||
| Body mass index (kg/m2) | 23.3 ± 3.8 | 25.6 ± 5.4 | 0.03 |
| Metabolic rate (kcal) | 1159 ± 135 | 1182 ± 138 | 0.48 |
| Skeletal muscle mass (kg) | 19.2 ± 3.8 | 19.8 ± 3.8 | 0.49 |
| Body fat mass (kg) | 17.5 ± 6.3 | 21.3 ± 8.5 | 0.02 |
| Odds Ratio | 95% CI | p Value | |
|---|---|---|---|
| Age (years) | 0.94 | 0.84–1.04 | 0.23 |
| Male | 0.99 | 0.38–2.63 | 0.99 |
| Baseline BMI ≥ 25 kg/m2 | 0.49 | 0.18–1.35 | 0.17 |
| Increase of metabolic rate | 0.33 | 0.09–1.17 | 0.09 |
| Increase of skeletal muscle mass | 4.73 | 1.29–17.26 | 0.02 |
| Increase of body fat mass | 1.15 | 0.44–2.97 | 0.78 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumura, K.; Iwasaka, T.; Mizuno, S.; Mizuno, I.; Hayanami, H.; Sawada, K.; Iwasaka, J.; Takeuchi, K.; Suga, T.; Sugiura, T.; et al. Effect of Exercise Training on Body Temperature in the Elderly: A Retrospective Cohort Study. Geriatrics 2021, 6, 3. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010003
Matsumura K, Iwasaka T, Mizuno S, Mizuno I, Hayanami H, Sawada K, Iwasaka J, Takeuchi K, Suga T, Sugiura T, et al. Effect of Exercise Training on Body Temperature in the Elderly: A Retrospective Cohort Study. Geriatrics. 2021; 6(1):3. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010003
Chicago/Turabian StyleMatsumura, Koichiro, Toshiji Iwasaka, Satoshi Mizuno, Ikuko Mizuno, Hikaru Hayanami, Kiyoshi Sawada, Junji Iwasaka, Kotaro Takeuchi, Toshimitsu Suga, Tetsuro Sugiura, and et al. 2021. "Effect of Exercise Training on Body Temperature in the Elderly: A Retrospective Cohort Study" Geriatrics 6, no. 1: 3. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010003