The Effect of High-Intensity Power Training on Habitual, Intervention and Total Physical Activity Levels in Older Adults with Type 2 Diabetes: Secondary Outcomes of the GREAT2DO Randomized Controlled Trial

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
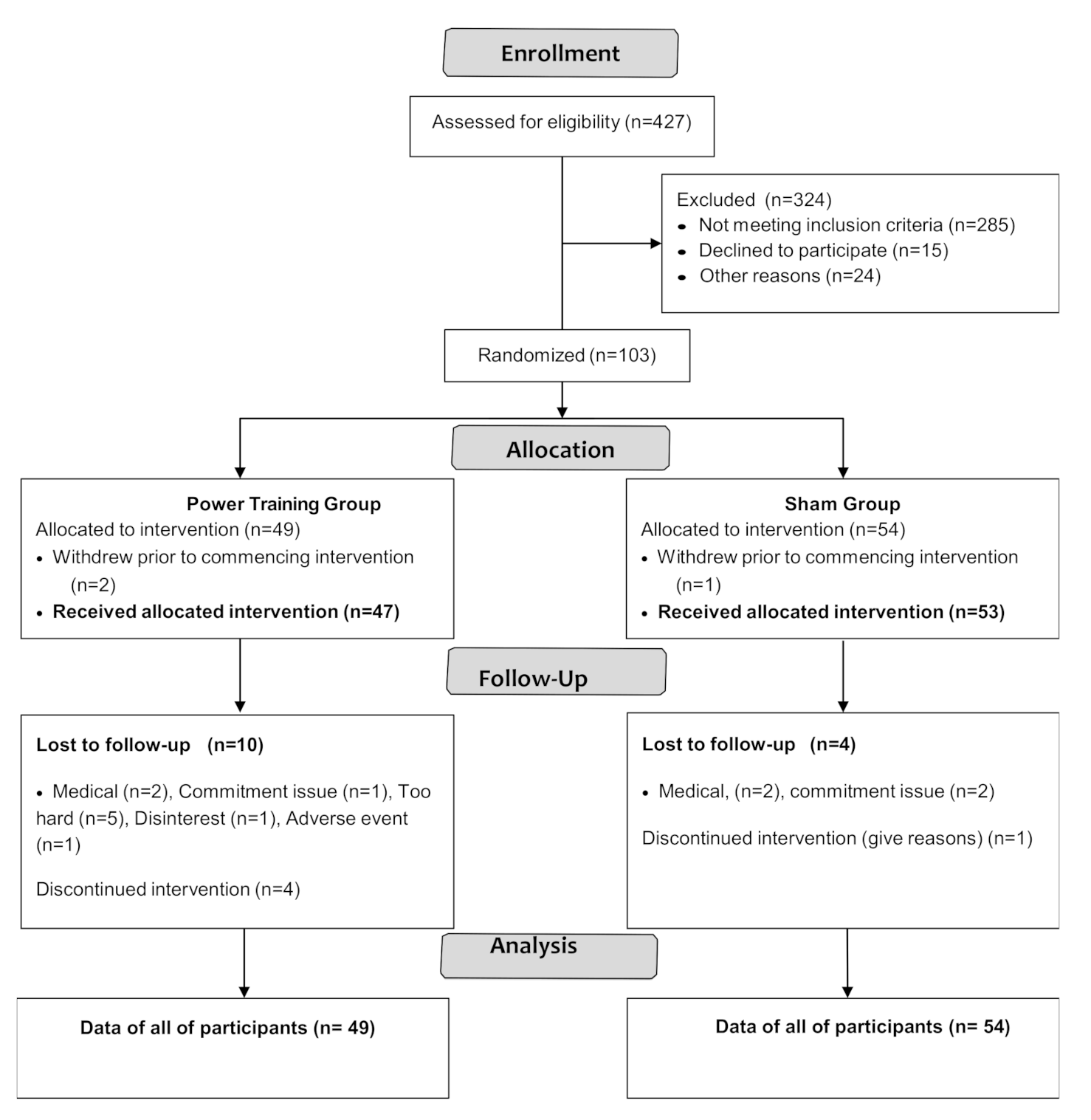
2.1. Study Subjects
2.2. Training Protocol
2.3. Habitual Physical Activity Level
Physical Activity Level Definitions
- 1.
- Habitual PA = any activity performed outside intervention sessions.
- 2.
- 3.
- Total PA = [average number of intervention sessions attended over the previous 6-months (% attendance) × 3 d/week × duration of session (h/day) × weighting factor (30 for power sessions and 21 for sham sessions)] + habitual PA.
- % attendance at 6 months = average attendance over the first 6 months of intervention.
- % attendance at 12 months = average attendance over months 6–12.
2.4. Measures of Insulin Resistance and Glucose Homeostasis
2.5. Anthropometrics
3. Statistical Analyses
4. Results
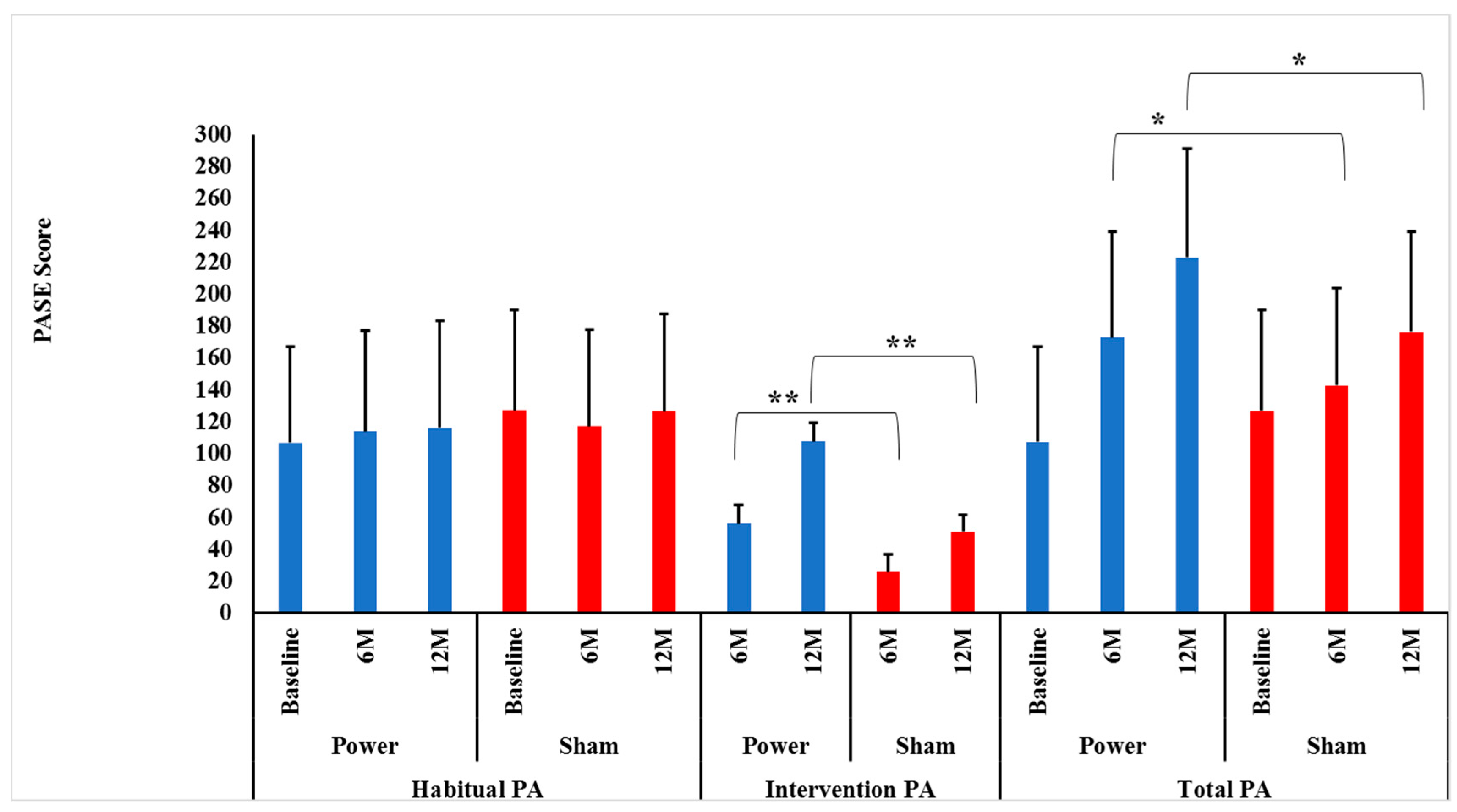
4.1. Changes in PA Level
4.1.1. Habitual PA Score
4.1.2. Intervention PA/Tonnage Score
4.1.3. Total PA Score
5. Discussion
5.1. Habitual PA Level
5.1.1. Why Habitual PA Did Not Increase over Time
5.1.2. Why Habitual PA Did not Decrease over Time
5.1.3. Intervention PA and Feasibility of High-Intensity Power Training
5.2. Total PA Level
Associations among PA Levels and Metabolic Profile
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Febbraio, M.A. Exercise metabolism in 2016: Health benefits of exercise—More than meets the eye! Nat. Rev. Endocrinol. 2017, 13, 72. [Google Scholar] [CrossRef]
- Umpierre, D.; Ribeiro, P.A.; Kramer, C.K.; Leitao, C.B.; Zucatti, A.T.; Azevedo, M.J.; Gross, J.L.; Ribeiro, J.P.; Schaan, B.D. Physical activity advice only or structured exercise training and association with HbA1c levels in type 2 diabetes: A systematic review and meta-analysis. JAMA 2011, 305, 1790–1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, S.J.; Connell, C.M.; Janevic, M.R. Gender Differences in Trajectories of Physical Activity Among Older Americans With Diabetes. J. Aging Health 2015, 28, 460–480. [Google Scholar] [CrossRef] [PubMed]
- Balducci, S.; D’Errico, V.; Haxhi, J.; Sacchetti, M.; Orlando, G.; Cardelli, P.; Vitale, M.; Bollanti, L.; Conti, F.; Zanuso, S.; et al. Effect of a Behavioral Intervention Strategy on Sustained Change in Physical Activity and Sedentary Behavior in Patients with Type 2 Diabetes: The IDES_2 Randomized Clinical Trial. JAMA 2019, 321, 880–890. [Google Scholar] [CrossRef] [Green Version]
- Morio, B.; Montaurier, C.; Pickering, G.; Ritz, P.; Fellmann, N.; Coudert, J.; Beaufrère, B.; Vermorel, M. Effects of 14 weeks of progressive endurance training on energy expenditure in elderly people. Br. J. Nutr. 1998, 80, 511–519. [Google Scholar] [CrossRef]
- Goran, M.I.; Poehlman, E.T. Endurance training does not enhance total energy expenditure in healthy elderly persons. Am. J. Physiol. Metab. 1992, 263, E950–E957. [Google Scholar] [CrossRef] [Green Version]
- King, N.A.; Caudwell, P.; Hopkins, M.; Byrne, N.M.; Colley, R.; Hills, A.P.; Stubbs, J.R.; Blundell, J.E. Metabolic and Behavioral Compensatory Responses to Exercise Interventions: Barriers to Weight Loss. Obesity 2007, 15, 1373–1383. [Google Scholar] [CrossRef]
- Manthou, E.; Gill, J.M.R.; Wright, A.; Malkova, D. Behavioural Compensatory Adjustments to Exercise Training in Overweight Women. Med. Sci. Sports Exerc. 2009, 42, 1. [Google Scholar] [CrossRef] [Green Version]
- Dunstan, D.W.; Daly, R.M.; Owen, N.; Jolley, D.; De Courten, M.; Shaw, J.; Zimmet, P. High-intensity resistance training improves glycemic control in older patients with type 2 diabetes. Diabetes Care 2002, 25, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Church, T.S.; Blair, S.N.; Cocreham, S.; Johannsen, N.; Johnson, W.; Kramer, K.; Mikus, C.R.; Myers, V.; Nauta, M.; Rodarte, R.Q.; et al. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: A randomized controlled trial. JAMA 2010, 304, 2253–2262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castaneda, C.; Layne, J.E.; Munoz-Orians, L.; Gordon, P.L.; Walsmith, J.; Foldvari, M.; Roubenoff, R.; Tucker, K.L.; Nelson, M.E. A Randomized Controlled Trial of Resistance Exercise Training to Improve Glycemic Control in Older Adults with Type 2 Diabetes. Diabetes Care 2002, 25, 2335–2341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balducci, S.; Zanuso, S.; Nicolucci, A.; de Feo, P.; Cavallo, S.; Cardelli, P.; Fallucca, S.; Alessi, E.; Fallucca, F.; Pugliese, G.; et al. Effect of an intensive exercise intervention strategy on modifiable cardiovascular risk factors in subjects with type 2 diabetes mellitus: A randomized controlled trial: The Italian Diabetes and Exercise Study (IDES). Arch. Intern. Med. 2010, 170, 1794–1803. [Google Scholar] [CrossRef] [Green Version]
- Korkiakangas, E.E.G.; Alahuhta, M.A.; Laitinen, J.H. Barriers to regular exercise among adults at high risk or diagnosed with type 2 diabetes: A systematic review. Health Promot. Int. 2009, 24, 416–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Heijden, M.M.P.; Van Dooren, F.E.P.; Pop, V.J.M.; Pouwer, F. Effects of exercise training on quality of life, symptoms of depression, symptoms of anxiety and emotional well-being in type 2 diabetes mellitus: A systematic review. Diabetologia 2013, 56, 1210–1225. [Google Scholar] [CrossRef] [Green Version]
- Lysy, Z.; Da Costa, D.; Dasgupta, K. The association of physical activity and depression in Type 2 diabetes. Diabet. Med. 2008, 25, 1133–1141. [Google Scholar] [CrossRef]
- Henwood, T.R.; Taaffe, D.R. Improved Physical Performance in Older Adults Undertaking a Short-Term Programme of High-Velocity Resistance Training. Gerontology 2005, 51, 108–115. [Google Scholar] [CrossRef]
- Rice, J.; Keogh, J. Power training: Can it improve functional performance in older adults? A systematic review. Int. J. Exerc. Sci. 2009, 2, 6. [Google Scholar]
- Orr, R.; De Vos, N.J.; Singh, N.A.; Ross, D.A.; Stavrinos, T.M.; Fiatarone-Singh, M.A. Power Training Improves Balance in Healthy Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Fielding, R.A.; Lebrasseur, N.K.; Cuoco, A.; Bean, J.; Mizer, K.; Singh, M.A.F. High-Velocity Resistance Training Increases Skeletal Muscle Peak Power in Older Women. J. Am. Geriatr. Soc. 2002, 50, 655–662. [Google Scholar] [CrossRef]
- De Vos, N.J.; Singh, N.A.; Ross, D.A.; Stavrinos, T.M.; Orr, R.; Singh, M.A.F. Optimal Load for Increasing Muscle Power During Explosive Resistance Training in Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 638–647. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Pessin, J.E. Mechanisms for fiber-type specificity of skeletal muscle atrophy. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 243–250. [Google Scholar] [CrossRef]
- Perry, B.D.; Caldow, M.K.; Brennan-Speranza, T.C.; Sbaraglia, M.; Jerums, G.; Garnham, A.; Wong, C.; Levinger, P.; Haq, M.A.U.; Hare, D.L.; et al. Muscle atrophy in patients with Type 2 Diabetes Mellitus: Roles of inflammatory pathways, physical activity and exercise. Exerc. Immunol. Rev. 2016, 22, 94–109. [Google Scholar]
- Braith, R.W.; Beck, D.T. Resistance exercise: Training adaptations and developing a safe exercise prescription. Hear. Fail. Rev. 2007, 13, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.A.; Mavros, Y.; Kay, S.; Meiklejohn, J.; De Vos, N.; Wang, Y.; Guo, Q.; Zhao, R.R.; Climstein, M.; Baune, B.T.; et al. Graded Resistance Exercise And Type 2 Diabetes in Older adults (The GREAT2DO study): Methods and baseline cohort characteristics of a randomized controlled trial. Trials 2015, 16, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavros, Y.; Kay, S.; Anderberg, K.A.; Baker, M.K.; Wang, Y.; Zhao, R.; Meiklejohn, J.; Climstein, M.; O’Sullivan, A.; De Vos, N.; et al. Changes in Insulin Resistance and HbA1c Are Related to Exercise-Mediated Changes in Body Composition in Older Adults With Type 2 Diabetes: Interim outcomes from the GREAT2DO trial. Diabetes Care 2013, 36, 2372–2379. [Google Scholar] [CrossRef] [Green Version]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome-a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, A.; Ingemann-Hansen, T.; Schmidt, A.; Halkjaer-Kristensen, J. Exercise-induced asthma after walking, running and cycling. Scand. J. Clin. Lab. Investig. 1982, 42, 15–18. [Google Scholar] [CrossRef]
- Washburn, R.A.; Smith, K.W.; Jette, A.M.; Janney, C.A. The physical activity scale for the elderly (PASE): Development and evaluation. J. Clin. Epidemiol. 1993, 46, 153–162. [Google Scholar] [CrossRef]
- New England Research Institutes. PASE: Physical Activity Scale for the Elderly; New England Research Institutes, Inc.: Watertown, MA, USA, 1991. [Google Scholar]
- Paffenbarger, R.S., Jr.; Hyde, R.T.; Wing, A.L.; Lee, I.M.; Jung, D.L.; Kampert, J.B. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N. Engl. J. Med. 1993, 328, 538–545. [Google Scholar] [CrossRef]
- Cussler, E.C.; Lohman, T.G.; Going, S.B.; Houtkooper, L.B.; Metcalfe, L.L.; Flint-Wagner, H.G.; Harris, R.B.; Teixeira, P.J. Weight Lifted in Strength Training Predicts Bone Change in Postmenopausal Women. Med. Sci. Sports Exerc. 2003, 35, 10–17. [Google Scholar] [CrossRef]
- Levy, J.C.; Matthews, D.R.; Hermans, M.P. Correct Homeostasis Model Assessment (HOMA) Evaluation Uses the Computer Program. Diabetes Care 1998, 21, 2191–2192. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- West, B.T. Analyzing Longitudinal Data with the Linear Mixed Models Procedure in SPSS. Eval. Health Prof. 2009, 32, 207–228. [Google Scholar] [CrossRef]
- Dubowitz, N.; Xue, W.; Long, Q.; Ownby, J.G.; Olson, D.E.; Barb, D.; Rhee, M.K.; Mohan, A.V.; Watson-Williams, P.I.; Jackson, S.L.; et al. Aging is associated with increased HbA1clevels, independently of glucose levels and insulin resistance, and also with decreased HbA1cdiagnostic specificity. Diabet. Med. 2014, 31, 927–935. [Google Scholar] [CrossRef]
- Kumar, A. Prevalence of Glycemic Status, Obesity & Waist Circumference in Punjabi Type 2 Diabetics. J. Exerc. Sci. Physiother. 2013, 9, 1. [Google Scholar] [CrossRef]
- Zazai, R.; Wilms, B.; Ernst, B.; Thurnheer, M.; Schultes, B. Waist Circumference and Related Anthropometric Indices Are Associated with Metabolic Traits in Severely Obese Subjects. Obes. Surg. 2014, 24, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Group, L.A.R. Cardiovascular effects of intensive lifestyle intervention in type 2 diabetes. N. Engl. J. Med. 2013, 2013, 145–154. [Google Scholar]
- Rejeski, W.J.; Bray, G.A.; Chen, S.-H.; Clark, J.M.; Evans, M.; Hill, J.O.; Jakicic, J.M.; Johnson, K.C.; Neiberg, R.; Ip, E.H.; et al. Aging and Physical Function in Type 2 Diabetes: 8 Years of an Intensive Lifestyle Intervention. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 70, 345–353. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.; Durstine, J.L.; Painter, P.; American College of Sports Medicine. ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities, 4E; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Ehlers, D.K.; Fanning, J.; Awick, E.A.; Kramer, A.F.; McAuley, E. Contamination by an Active Control Condition in a Randomized Exercise Trial. PLoS ONE 2016, 11, e0164246. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise Training and Nutritional Supplementation for Physical Frailty in Very Elderly People. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Perri, M.G.; Anton, S.D.; Durning, P.E.; Ketterson, T.U.; Sydeman, S.J.; Berlant, N.E.; Kanasky, W.F., Jr.; Newton, R.L., Jr.; Limacher, M.C.; Martin, A.D. Adherence to exercise prescriptions: Effects of prescribing moderate versus higher levels of intensity and frequency. Health Psychol. 2002, 21, 452. [Google Scholar] [CrossRef] [PubMed]
- Eves, N.D.; Plotnikoff, R.C. Resistance Training and Type 2 Diabetes: Considerations for implementation at the population level. Diabetes Care 2006, 29, 1933–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Boulé, N.G.; Wells, G.A.; Prud’homme, D.; Fortier, M.; Reid, R.D.; Tulloch, H.; Coyle, D.; Phillips, P.; et al. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes: A randomized trial. Ann. Intern. Med. 2007, 147, 357–369. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Pruitt, L.A.; Phillips, W.; Oka, R.; Rodenburg, A.; Haskell, W.L. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, 74–83. [Google Scholar]



{kind=link}
{kind=link}
| PASE Activity | PASE Weight | Activity Frequency | PASE Score = Weight × Frequency |
|---|---|---|---|
| Muscle strength/endurance | 30 | ||
| Strenuous sports | 23 | ||
| Moderate sports | 23 | ||
| Light sports | 21 | ||
| Job involving standing/walking | 21 | ||
| Walk outside | 20 | ||
| Lawn work or yard care | 36 | ||
| Caring for another person | 35 | ||
| Home repairs | 30 | ||
| Heavy housework | 25 | ||
| Light housework | 25 | ||
| Outdoor-gardening | 20 | ||
| PASE Total |
| Demographics and Health Status | Group | Mean ± SD or N, (%) |
|---|---|---|
| Age (years) | Power | 67.0 ± 5.0 |
| SHAM | 69.0 ± 6.0 | |
| Total | 67.9 ± 5.5 | |
| Men, Women (n) | Power | 25, 24 |
| SHAM | 27, 27 | |
| Duration of diabetes (years) | Power | 7 ± 5 |
| SHAM | 9 ± 7 | |
| Total | 8.0 ± 6.0 | |
| Average stretch stature (m) | Power | 1.7 ± 0.1 |
| SHAM | 1.7 ± 0.1 | |
| Total | 1.7 ± 0.1 | |
| Weight (kg) | Power | 90.0 ± 15.3 |
| SHAM | 88.7 ± 18.8 | |
| Total | 89.1 ± 17.1 | |
| BMI (kg/m2) | Power | 31.5 ± 4.6 |
| SHAM | 31.6 ± 6.0 | |
| Total | 31.6 ± 5.4 | |
| Waist circumference (cm) | Power | 110.1 ± 11.9 |
| SHAM | 109.0 ± 12.4 | |
| Total | 109.5 ± 12.1 | |
| Total no. chronic diseases (n) | Power | 5 ± 2 |
| SHAM | 5 ± 2 | |
| Total | 5 ± 2 | |
| Osteoarthritis, n (%) | Power | 35 (71.4) |
| SHAM | 33 (61.1) | |
| Total | 68.0 (66.0) | |
| Diabetic treatment, n (%) | ||
| Diet only | Power | 8 (16) |
| SHAM | 10 (19) | |
| Total | 18 (17) | |
| Oral hypoglycemics only | Power | 34 (69) |
| SHAM | 35(65) | |
| Total | 69 (67) | |
| Oral hypoglycemics + insulin | Power | 4 (8) |
| SHAM | 7 (13) | |
| Total | 11 (11) | |
| Insulin only | Power | 3 (6) |
| SHAM | 2 (4) | |
| Total | 5 (5) | |
| Metabolic profile | ||
| HbA1c (%) | Power | 6.9 ± 0.9 |
| SHAM | 7.3 ± 1.3 | |
| Total | 7.1 ± 1.1 | |
| Fasting serum glucose (mmol/L) | Power | 7.4 ± 2.5 |
| SHAM | 7.1 ± 2.2 | |
| Total | 7.3 ± 2.4 | |
| Fasting serum insulin (mU/L) | Power | 10.1 ± 5.9 |
| SHAM | 11.1 ± 6.7 | |
| Total | 10.6 ± 6.3 | |
| * HOMA2-IR | Power | 2.7 ± 0.96 |
| SHAM | 3.1 ± 1.2 | |
| Total | 2.9 ± 1.1 | |
| Physical activity level | ||
| PASE score | Power | 113.2 ± 61.9 |
| SHAM | 126.2 ± 63.0 | |
| Total | 120.0 ± 62.5 | |
| Physical function | ||
| Habitual gait speed (m/s) | Power | 1.2 ± 0.2 |
| SHAM | 1.2 ± 0.2 | |
| Total | 1.2 ± 0.2 | |
| Maximal gait speed (m/s) | Power | 1.9 ± 0.3 |
| SHAM | 1.9 ± 0.3 | |
| Total | 1.9 ± 0.3 |
| Study | Age (years) | Supervised | PA Assessment | Aerobic Exercise Effect on Habitual PA | Resistance Exercise Effect on Habitual PA | Combined Aerobic and Resistance Exercise Effect on Habitual PA |
|---|---|---|---|---|---|---|
| Dunstan | 60–80 | Y | Subjective | - | No change | - |
| Castaneda | >55 | Y | Subjective | - | Increase | - |
| Church | 30–75 | Y | Objective | No change | No change | No change |
| Balducci | 40–75 | Y | Subjective | - | - | Increase |
| GREAT2DO | 60–83 | Y | Subjective | - | No change | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosalman Haghighi, M.; Mavros, Y.; Kay, S.; Simpson, K.A.; Baker, M.K.; Wang, Y.; Zhao, R.R.; Meiklejohn, J.; Climstein, M.; O’Sullivan, A.J.; et al. The Effect of High-Intensity Power Training on Habitual, Intervention and Total Physical Activity Levels in Older Adults with Type 2 Diabetes: Secondary Outcomes of the GREAT2DO Randomized Controlled Trial. Geriatrics 2021, 6, 15. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010015
Mosalman Haghighi M, Mavros Y, Kay S, Simpson KA, Baker MK, Wang Y, Zhao RR, Meiklejohn J, Climstein M, O’Sullivan AJ, et al. The Effect of High-Intensity Power Training on Habitual, Intervention and Total Physical Activity Levels in Older Adults with Type 2 Diabetes: Secondary Outcomes of the GREAT2DO Randomized Controlled Trial. Geriatrics. 2021; 6(1):15. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010015
Chicago/Turabian StyleMosalman Haghighi, Marjan, Yorgi Mavros, Shelley Kay, Kylie A. Simpson, Michael K. Baker, Yi Wang, Ren Ru Zhao, Jacinda Meiklejohn, Mike Climstein, Anthony J. O’Sullivan, and et al. 2021. "The Effect of High-Intensity Power Training on Habitual, Intervention and Total Physical Activity Levels in Older Adults with Type 2 Diabetes: Secondary Outcomes of the GREAT2DO Randomized Controlled Trial" Geriatrics 6, no. 1: 15. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6010015