
Sustained Crohn’s Disease Remission with an Exclusive Elemental and Exclusion Diet: A Case Report

Johns Hopkins University, Baltimore, MD 21218, USA
Gastrointest. Disord. 2021, 3(3), 129-137; https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3030014
Submission received: 14 July 2021
/
Revised: 5 August 2021
/
Accepted: 9 August 2021
/
Published: 12 August 2021
{kind=link}
{kind=link}
Abstract
:The incidence of inflammatory bowel diseases, such as Crohn’s disease (CD), is increasing worldwide. Despite several new therapeutics to treat CD, many patients fail to respond to their medications and inevitably face surgical resection. While genetics plays a role in CD, environmental factors are potential triggers. Recent research from the past few years suggest that pro-inflammatory foods are associated with an increased risk of CD. Some studies have shown the benefit of including exclusion diets, such as the specific carbohydrate diet (SCD) and exclusive elemental diets, to induce CD remission, but published data is limited. This case study explores how an exclusive elemental and exclusion diet helped induce clinical and biochemical remission and radiologic healing in a young adult male who had failed to achieve remission using standard medical treatment. C-reactive protein (CRP), fecal calprotectin, and magnetic resonance enterography (MRE) served as objective markers of inflammation in this study.
1. Introduction
At the Mount Sinai Hospital in 1932, Dr. Burrill B. Crohn and his colleagues Dr. Leon Ginzburg and Dr. Gordon D. Oppenheimer first described Crohn’s disease (CD), a disease of the terminal ileum mainly affecting young adults [1]. There is now a lot more known about CD, but still a lot unknown. The onset of the disease, for example, occurs between ages 10 to 40, including a small peak between ages 50 to 60 years [2]. CD differs from ulcerative colitis (UC), as inflammation occurs at the terminal ileum and anywhere in the gastrointestinal tract from mouth to rectum [3]. CD is characterized by periods of disease activity (flares) and periods of few to no symptoms (remission). During flares, patients experience gastrointestinal symptoms, such as loose stools, diarrhea, abdominal pain, and rectal bleeding, which may lead to weight loss, anemia, and fatigue [4]. CD can also be complicated by abscesses, fistulas, strictures, bowel obstructions, and surgical resections [3]. The overall mortality rate among patients with CD is slightly higher than the general population due to cancer, gastrointestinal diseases, respiratory diseases, and genitourinary diseases [5]. Patients with UC or CD with colon involvement are six times more likely to develop colon cancer than the general population, which accounts for 10–15% of all deaths among patients with IBD [6]. The overall incidence of IBD is increasing worldwide [7]. In the United States, IBD incidence particularly increased between 2005 and 2015; and in 2019, the overall incidence rate was 37.5/100,000 person-years [7].
Intestinal tuberculosis was once thought to be the cause of CD; however, Dr. Crohn and his colleagues did not find the symptoms of CD to be consistent with tuberculosis or any other known disease [1]. Although the cause of CD is still unclear, it is understood that genetic predisposition, environmental triggers, and immune system dysregulation collectively interact [8]. In 2001, mutations of NOD2/CARD15 were identified as the first susceptibility gene associated with the development of CD [9]. In 2006, IL23R was identified as another IBD gene [10]. In 2012, 163 gene variants were confirmed to be associated with IBD; 110 associated with both UC and CD, 23 as UC-specific, and 30 as CD-specific [11]. Despite discovering many genes associated with IBD, only a small portion of heritability is characterized by genetic variants: 13.1% in CD and 8.2% in UC [12]. Many environmental factors can potentially trigger IBD. Individuals who are smokers, for example, are more likely to develop CD [13]. Antibiotics are also associated with an increased risk of new-onset CD [14].
As various medications to treat Crohn’s disease have met with limited success, diet has shown some promise as a treatment alternative or accompaniment. The gut microbiome and diet are intrinsically linked to the emergence of IBD, thus offering potential targets for therapeutic intervention [14]. In 2014, clinical evidence to support altering diet was deemed scarce [15]. In recent years, however, more data has suggested that diet may impact CD. In 2018, a Cochrane systematic review concluded that there is low-quality evidence suggesting that corticosteroids may be more effective than enteral nutrition, such as exclusive use of elemental (amino-acid based) diets, for inducing clinical remission in adults with active CD [16]. The Cochrane systematic review also suggested that enteral nutrition, such as exclusive elemental diets, should be considered as a therapeutic option for CD; this option should only be considered in specific cases, for instance with pediatric patients or patients who can consume exclusively elemental diet formulations without difficulty [16].
New research has also shown associations between various foods and inflammation. Mediterranean diets, which are rich in monounsaturated fats, fiber, and omega-3 fatty acids, for example, have been associated with a significantly lower risk of later-onset CD [17]. On the other hand, consumption of pro-inflammatory foods high in red meat, high-fat dairy, refined grains, saturated fats, glycemic carbohydrates, and high-energy soft drinks have been associated with an increased risk of CD [18]. The specific carbohydrate diet (SCD), created by Dr. Sidney Haas and Elaine Gloria Gottschall in 1994, which is featured in this study, has also received attention in recent years [19]. The SCD theorizes that microbiome dysbiosis is associated with IBD and that adhering to a low-complex-carbohydrate diet can improve symptoms through restoring balance to gut flora [19]. Unlike the Mediterranean diet, the SCD solely allows carbohydrates that come from monosaccharides (glucose, fructose, galactose) [19]. All grains and most starchy vegetables are prohibited on the SCD, while the consumption of non-starchy vegetables is allowed [19]. Unprocessed meats, poultry, fish, shellfish, lactose-free dairy products, including homemade fermented yogurt, and fresh fruit are allowed [19]. Most nuts, oils, teas, coffee, and juices with no additives are also allowed [19]. The effectiveness of SCD in reducing inflammation and improving symptoms has been shown in pediatric CD studies and case series [20,21,22,23]. This case report explores how clinical and biochemical remission and radiologic healing was achieved in a young adult with ileocolonic and perianal disease, simultaneously using the exclusive use of an elemental diet (amino acid based) formula and an exclusion diet, based on the theories of SCD, while also excluding eggs, all dairy, and alcohol.
2. Case Presentation
A 25-year-old Caucasian male patient first presented in 2012 with a perianal abscess and fistula. He subsequently underwent a fistulotomy and hemorrhoidectomy. The diagnosis/impression biopsy revealed severe acute, chronic granulomatous inflammation with ulceration of the anal canal. He went on to have a colonoscopy, which demonstrated ileocolonic ulceration. His treatment between 2012 and 2013 commenced with corticosteroids (prednisone 20 mg/day) and azathioprine (100 mg orally 1×/day for six months). In late 2013, he initiated treatment with infliximab (100 mg IV/8 weeks). In 2017, however, he developed antibodies against infliximab (2550, high titer) and had evidence of active CD based on elevated fecal calprotectin in May 2017. Subsequently, he began treatment with adalimumab (160 mg at day 0, 80 mg at day 14, and 40 mg at day 28, then 40 mg every other week).
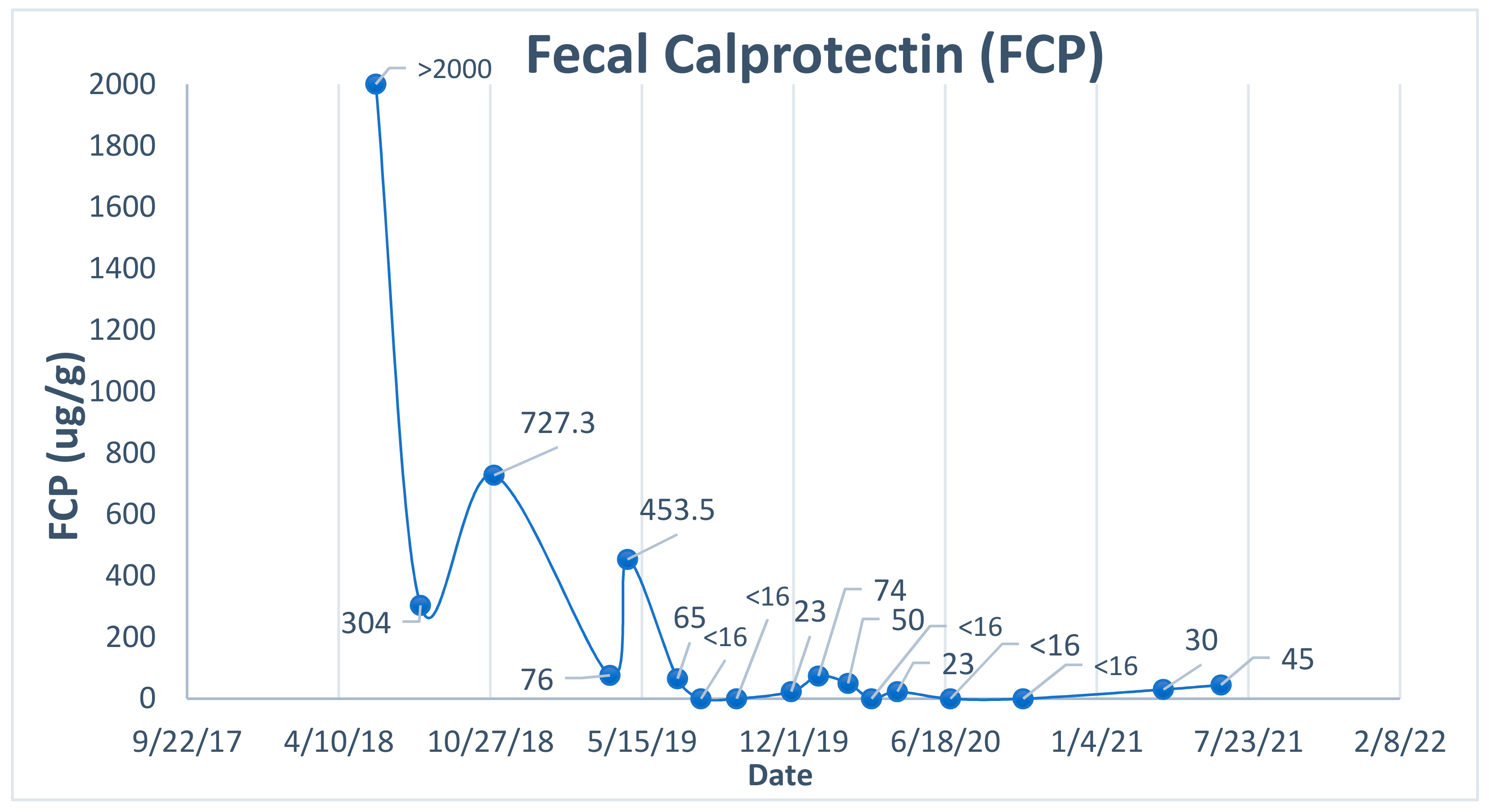
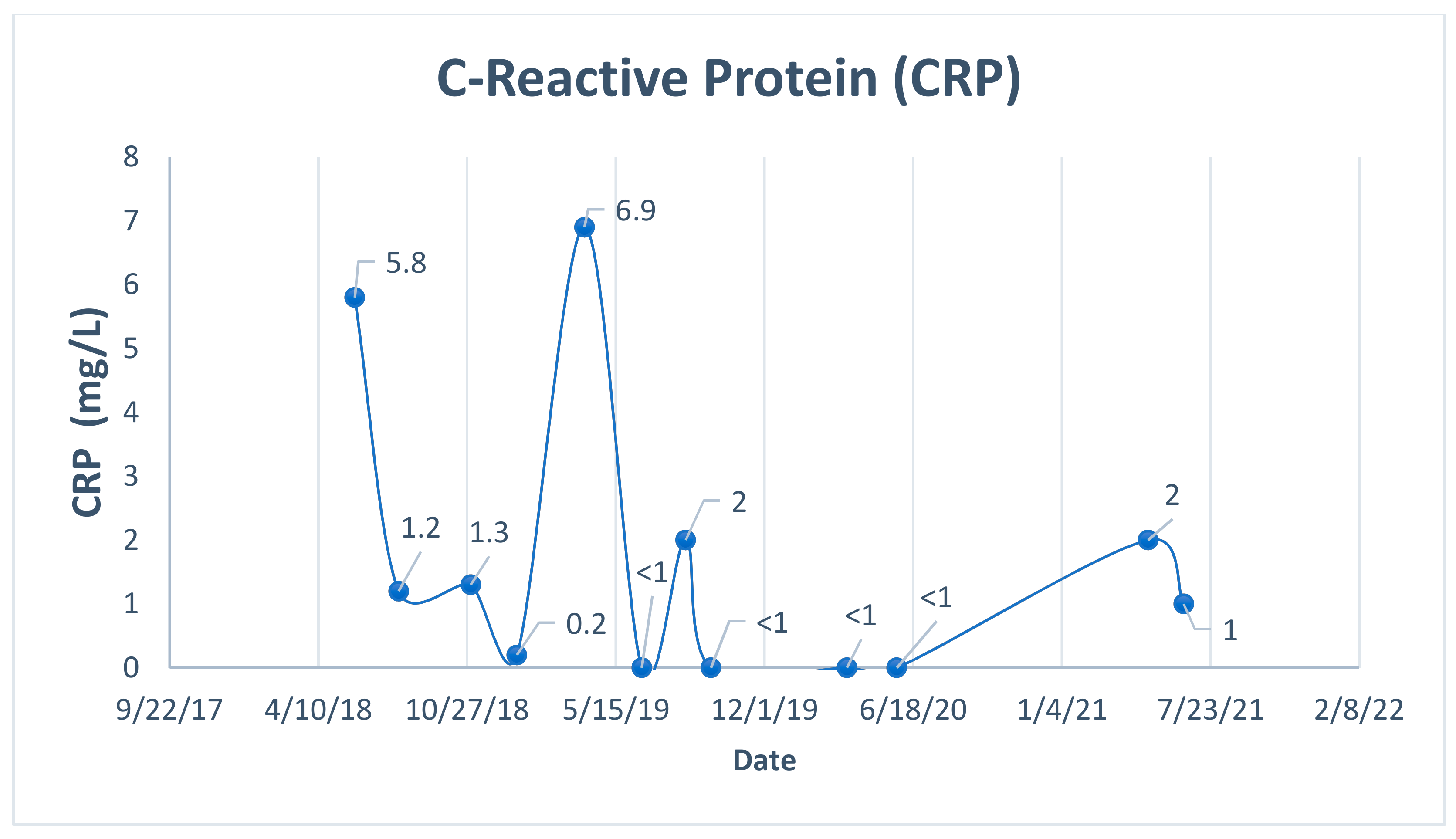
In May 2018, his symptoms, including diarrhea, abdominal pain, and fatigue, returned, his fecal calprotectin was elevated at >2000, and his CRP (C-reactive protein) was elevated at 5.8 (Figure 1 and Figure 2). MRE (magnetic resonance enterography) in June 2018 indicated active ileal disease, without obstruction, but some smooth narrowing of the terminal ileum and the apparent involvement of the cecum. Humira levels were checked and were undetectable, but high antibody levels were present, consistent with active disease. Subsequently, in June 2018, he was treated with ustekinumab (90 mg/mL, 1 mL (90 mg per dose) every eight weeks). In July 2018, his fecal calprotectin dropped from >2000 to 304 (Figure 1). A repeat MRE in December 2018, however, indicated a stable appearance of thickening/enhancement in the distal/terminal ileum without evidence of fistula or abscess. Thus, he began taking Stelara every four weeks and also commenced budesonide (9 mg/day, tapered by 3 mg/month). He stopped budesonide in March 2019. Towards the end of March 2019, his calprotectin was elevated to 453.5 (Figure 1). He repeated an MRE in May 2019, which indicated stable mural thickening and enhancement of the terminal ileum. It appeared that ustekinumab did not work as well for him as the anti-TNFα family of drugs. He continued to report loose bowel movements (Bristol Stool Chart Type 6), abdominal pain, and fatigue.
In early June 2019, the patient decided to begin two weeks of physicians’ elemental diet dextrose free (integrative therapeutics), an exclusive elemental diet (amino-acid sources), followed by a week of a diet in which half the calories came from food (based on the SCD stage one) and half from the exclusive elemental diet, with physician supervision [24]. Biochemical and clinical responses were recorded after three weeks. His CRP dropped from 6.9 in early March 2019 to <1 in mid-June 2019 (Figure 2). His fecal calprotectin dropped from 453.5 in late March 2019 to 65 in July 2019 (Figure 1). Following the exclusive elemental diet, he decided to transition to an exclusion diet similar to SCD by eliminating all grains (wheat, rice, corn, oats, pseudo-grains), disaccharides (lactose, sucrose), polysaccharides (starchy vegetables, cellulose), processed foods (boxed and manufactured foods), additives, stabilizers, and emulsifiers. He also excluded all alcohol, dairy, and eggs.
The patient followed the five stages of the diet based on educational resources provided on NiMBAL (Nutrition in Immune Balance), founded by David L. Suskind, MD, at Seattle Children’s Hospital [24]. In the beginning stages, the foods the patient consumed were meats that were roasted, boiled, or broiled, 100% apple cider juice, gelatin, ripe bananas with spots, applesauce, pear sauce, and carrots and squash that were peeled and pureed [24]. The variation of the foods included in the diet increased as the stages of the diet progressed [24]. Over time, he introduced cooked foods ranging from fish, meats, fruits, non-starchy vegetables, herbs, spices, and legumes. The patient was educated on strictly adhering to making home-cooked meals and learning which foods are “legal and illegal” on the diet, based on the information found in NiMBAL [25]. In this case report, the patient was educated on the risk of deficiencies if his diet remained restricted to only certain foods. Every 2 to 4 weeks, the patient self-reported his food intake to ensure compliance to the diet and a varied and adequate food consumption. The dietary reports were then analyzed to assess nutrient intake by his provider. Thus, the micronutrient and macronutrient content was sufficient in the diet, including calcium, according to blood tests. However, a deficiency in vitamin D was observed; thus, supplementation was provided. Fecal calprotectin (Figure 1) was closely monitored every 1–2 months, and several normal readings were observed throughout the diet, ensuring the patient did not flare. His weight remained stable throughout the diet.
The patient kept track of both his bowel movements and his stool classification with the Bristol Stool Chart daily. Throughout June–September 2019, his stool mainly was Bristol Stool Chart Type 5 (1–3 bowel movements a day). During October 2019–March 2020, his stool was between Bristol Stool Chart Type 4 and Bristol Stool Chart Type 5 (1–3 bowel movements a day), but primarily Bristol Stool Chart Type 4. During April 2020–June 2021, his stool was primarily Bristol Stool Chart Type 4 (1–2 bowel movements a day). He occasionally experienced Bristol Stool Chart Type 6, once every other month, which was assumed to be due to consuming too much fiber on a particular day. The patient then began a moderate consumption of fiber. Before changing his diet, he consumed a standard American diet of daily consumption of dairy products, grains, processed foods, starchy vegetables, and some fruits and vegetables. In April 2020, he repeated an MRE, which indicated no new areas of stricture, no abscess, no fistula, and the previously seen mucosal enhancement and thickening of the terminal ileum appeared to have improved compared to the previous study in May 2019. He has strictly adhered to his exclusion diet, and his fecal calprotectin and CRP markers have been stable for two years (June/July 2019–June 2021) (Figure 1 and Figure 2).
MRE Results
Baseline (14 May 2019): Redemonstration of long-segment mural thickening and enhancement of the terminal ileum, grossly stable.
12 months (16 April 2020): Previously seen mucosal enhancement and thickening of the terminal ileum appears to have improved in the current study. No new areas of stricture are seen. No abscess, fistula is definitively noted.
3. Discussion
The first choice for treatment of IBD is medication [26]. There are five classes of treatment for IBD, ranging from aminosalicylates, corticosteroids, immunomodulators, antibiotics, and most recently, biologic therapies [26]. Despite the effectiveness of recent anti-TNFα medications, they produce numerous side effects, and up to 30% of patients are unresponsive [27]. Among patients who successfully respond to their first anti-TNFα medications, almost 60% experience a secondary loss of response [28]. Patients with IBD inevitably face several additional health complications once medications fail. Nearly 50 percent of patients with CD, for example, require surgical resection within ten years of diagnosis [29]. Surgery, however, does not cure CD, and the likelihood of relapses remains high [30]. Most patients fail to maintain clinical remission [31].
CD also places a significant strain on the healthcare system. In 2004, over 800,000 ambulatory care visits and over 1 million all-listed visits were due to CD, with over 80 percent of visits amongst young and middle-aged adults [32]. There were also 1.8 million prescriptions for medication to treat CD [32]. Hospital stays for CD in 2013 were >196,000 (59.7 per 100,000) [33]. The healthcare burden of IBD ranged anywhere between USD 14 to almost USD 32 billion in 2014 [34]. Around 31% of costs are attributable to hospitalization, 33% to outpatient care, and 35% to pharmaceuticals for CD [35]. Patients with IBD also have higher rates of depression and anxiety than the general population, which is associated with poor treatment compliance [36].
Although anecdotal evidence of active CD and UC treatment with diet may be common, published data with exclusion diets are limited [22,37]. Some studies have shown exclusion diets, such as SCD, to be effective; however, these studies were completed in pediatric patients [21,22,23]. Another case report study, which was the first remission of disease activity with SCD, was completed in a 73-year-old female with UC, not CD [38]. The elderly are also known to have milder disease activity, while stricturing and fistulating disease with ileocolonic involvement is more common in younger individuals [39]. Although another case series showed many patients adhering to SCD while in remission, there were no patients with both ileocolonic and perianal disease [20]. The case series also showed that many patients were still taking either immunosuppressive medications, corticosteroids, nonsteroidal anti-inflammatories, or off-label naltrexone at low doses to manage their disease activity, thus, making it difficult to assess whether remission was achieved through diet or medication [20].
On the other hand, this case shows clinical and biochemical remission and radiologic healing in a 25-year-old male, who is considered to have a moderate-to-severe form of CD due to ileocolonic and perianal disease, without using any medications through an exclusive elemental diet and an exclusion diet. The mechanism of the exclusive elemental diet, which is solely based on amino acids and monosaccharides, is theorized to induce remission through reducing antigen exposure, and alteration of the fecal flora that impacts immunomodulation downscaling, allowing for “bowel rest” as a result [40]. One study has shown a down-regulation of pro-inflammatory cytokine mRNA in both the terminal ileum and colon following an oral polymeric diet [41]. Certain bacteria may have also been starved off. According to Gottschall, polysaccharides, for example, are theorized to be poorly absorbed in the gastrointestinal tract causing bacterial and yeast overgrowth [19]. A clinical trial studying exclusive elemental diets showed that terminal restriction fragments (reflecting bacterial species) were unchanged, whereas Bacteroides fragilis significantly decreased after patients with CD completed an exclusive elemental diet [42]. Strains of enterotoxigenic Bacteroides fragilis can lead to diarrhea and colon cancer, and severe inflammation in patients with CD and UC [43].
Healing continued when the patient transitioned to an exclusion diet, which is theorized to have cumulative anti-inflammatory effects. Continuing to exclude polysaccharides, for example, in this patient’s diet may have contributed to gut healing. The patient cooked all of his foods (including all fruits and vegetables), and because cooking breaks down fibers, it likely made it easier for him to both digest and absorb the nutrients [44]. Although the mechanisms are unclear, dietary fiber has been shown to inhibit inflammation, be favorable for CD, and help maintain remission [45,46]. When fiber reaches the colon to be degraded by the microbiota, it is believed that the short-chain fatty acids (acetate, propionate, butyrate) produced result in an anti-inflammatory, anticarcinogenic immune-regulatory function [44]. The patient substantially increased his fiber intake, but excessive fiber (40 g+ per day) caused an increase in bowel movements. A moderate fiber intake (25–30 g per day) appeared to be more suitable for him. Tolerances of amount of fiber intake are highly individualized. Future studies should evaluate the right amount, or patients may need to investigate through trial and error. The patient also excluded eggs, dairy, and alcohol. However, tolerances of dairy and eggs are highly variable amongst patients. In one study, patients with UC who had a high consumption of eggs were more likely to have a flare-up [47]. High-fat dairy products have also been shown to worsen CD symptoms [48]. Diets high in milk fat have been shown to alter the gut microbiome by increasing the sulfite-reducing pathobiont Bilophilia wadsworthia and inducing inflammation in genetically susceptible mice [49]. Alcohol also has pro-oxidant effects and deleterious effects on the gut, which could trigger flares in patients with IBD [50].
One of the limitations of this case report was that mucosal healing was not assessed with colonoscopy. Other objective measures, such as CRP and fecal calprotectin, however, showed significant decreases in disease activity. Fecal calprotectin has been shown to correlate with disease activity in IBD [51]. Furthermore, calprotectin, CRP, and MRE had all been previously shown to be reliable for detecting the degree of this patient’s inflammation during flares. MRE is safe and non-invasive and has been shown to compare favorably to colonoscopy for characterizing the disease activity of CD [52]. MRE has a sensitivity of 82% and specificity of 80% compared to colonoscopy, with a sensitivity of 85% and a specificity of 85% [53].
Another limitation of this study is its difficulty in implementation without adequate supervision from a physician or dietitian familiar with the intricacies of SCD. Whenever exclusion diets such as SCD are followed, and certain foods are cut out, such as eggs or dairy, they pose concerns for individuals for deficiency in certain nutrients like B vitamins, calcium, potassium, and vitamins A, C, E, and D [54]. While these are concerns, the exclusion diet provides all dietary micro and macronutrients, only if a wide range of foods are incorporated. A study in pediatric patients who adhered to SCD showed that the majority of participants’ daily intakes met or exceeded the recommended dietary allowance (RDA) for B vitamins and vitamins A, C, and E [54]. The study also demonstrated sufficient protein and amino acid intake, as protein intake was three times the RDA [54]. However, all participants’ intakes were below the RDA for vitamin D and seventy-five percent of daily intakes were less than the RDA for calcium [54]. In this case report, as expected, a vitamin D deficiency was observed, so supplementation was provided. Close monitoring of dietary reports by providers is necessary to avoid any nutrient deficiencies.
It is a limitation that there were no objective measures of dietary compliance, but the patient’s stable weight, food intake reports, and fecal calprotectin results completed monthly or bimonthly ensured little-to-no prohibited foods were consumed. Another strategy to ensure compliance is for patients to incorporate their food consumption into a food tracking app. Future studies need to ensure close monitoring with a physician or dietitian trained in SCD to avoid the risk of gastrointestinal complaints, flare-ups, or nutritional deficiencies. To avoid exacerbation of disease activity, noninvasive tests such as fecal calprotectin should also be closely monitored on a monthly or bimonthly basis.
Another limitation of this case report is its inability to generalize certain foods, since triggers may be varied for different patients. For example, in this study, the patient had trouble implementing carrots in the earlier stages of the diet, but did better when consuming butternut squash. To address some of these issues, the patient used an app to track trigger foods and his stool frequency and shape according to the Bristol Stool Chart. Having records using an app about stool frequency and notes on foods consumed daily will ensure that both the patient and provider can quickly identify any issues with foods. Ultimately, implementing dietary changes is individualized, and future studies should be cognizant that patients need to receive a diet that is tailored towards their needs, with the close supervision of a dietitian or physician. For patients and physicians looking to learn more about exclusion diets such as SCD, the book “Breaking the Vicious Cycle” by Elaine Gloria Gottschall, published in 1994, provides more information [19]. There are also a wealth of educational resources, such as handouts on the various stages of the diet, a list of allowed foods, and more, on NiMBAL [24,25].
A final limitation of the study is that it was difficult to measure what specifically decreased the patient’s inflammation. While he made several changes to his diet, it is unclear which exclusion of foods specifically contributed to quelling disease activity, as well as the accuracy of diet reporting. Although this single case report has limitations in the ability to generalize, it warrants a continued approach to promote individualized diets, either as a sole therapeutic option in select patients or in adjunct with medications, to control disease activity and induce sustained remission, with physician supervision. Future studies could explore the mechanisms by which specific foods cause a decrease in inflammation and which foods are generally tolerable for patients with CD. Additionally, more research is needed to better understand what changes occur in the gut microbiome and which microbes are implicated in IBD when dietary modifications, such as exclusive elemental and exclusion diets, are made to address disease activity in patients.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
| CD | Crohn’s disease |
| CRP | C-Reactive protein |
| FCP | Fecal calprotectin |
| IBD | Inflammatory bowel disease |
| MRE | Magnetic resonance enterography |
| mRNA | Messenger ribonucleic acid |
| SCD | Specific carbohydrate diet |
| TNF-α | Tumor necrosis factor-alpha |
| UC | Ulcerative colitis |
References
- Crohn, B.B.; Ginzburg, L.; Oppenheimer, G.D. Regional Ileitis: A pathologic and clinical entity. J. Am. Med. Assoc. 1932, 99, 1323–1329. [Google Scholar] [CrossRef]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing Incidence and Prevalence of the Inflammatory Bowel Diseases with Time, Based on Systematic Review. Gastroenterology 2012, 142, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Wilkins, T.; Jarvis, K.; Patel, J. Diagnosis and Management of Crohn’s Disease. Am. Fam. Physician 2011, 84, 1365–1375. [Google Scholar]
- Duricova, D.; Pedersen, N.; Elkjaer, M.; Gamborg, M.; Munkholm, P.; Jess, T. Overall and Cause-Specific Mortality in Crohn’s Disease: A Meta-Analysis of Population-Based Studies. Inflamm. Bowel Dis. 2010, 16, 347–353. [Google Scholar] [CrossRef]
- Mattar, M.C.; Lough, D.; Pishvaian, M.J.; Charabaty, A. Current Management of Inflammatory Bowel Disease and Colorectal Cancer. Gastrointest. Cancer Res. 2011, 4, 53–61. [Google Scholar] [PubMed]
- Keyashian, K.; Dehghan, M.; Sceats, L.; Kin, C.; Limketkai, B.N.; Park, K.T. Comparative Incidence of Inflammatory Bowel Disease in Different Age Groups in the United States. Inflamm. Bowel Dis. 2019, 25, 1983–1989. [Google Scholar] [CrossRef]
- Ha, F.; Khalil, H. Crohn’s Disease: A Clinical Update. Ther. Adv. Gastroenterol. 2015, 8, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Hugot, J.-P.; Chamaillard, M.; Zouali, H.; Lesage, S.; Cézard, J.-P.; Belaiche, J.; Almer, S.; Tysk, C.; O’Morain, C.A.; Gassull, M.; et al. Association of NOD2 Leucine-Rich Repeat Variants with Susceptibility to Crohn’s Disease. Nature 2001, 411, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Duerr, R.H.; Taylor, K.D.; Brant, S.R.; Rioux, J.D.; Silverberg, M.S.; Daly, M.J.; Steinhart, A.H.; Abraham, C.; Regueiro, M.; Griffiths, A.; et al. A Genome-Wide Association Study Identifies IL23R as an Inflammatory Bowel Disease Gene. Science 2006, 314, 1461–1463. [Google Scholar] [CrossRef] [Green Version]
- Jostins, L.; Ripke, S.; Weersma, R.K.; Duerr, R.H.; McGovern, D.P.; Hui, K.Y.; Lee, J.C.; Schumm, L.P.; Sharma, Y.; Anderson, C.A.; et al. Host-Microbe Interactions Have Shaped the Genetic Architecture of Inflammatory Bowel Disease. Nature 2012, 491, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Ventham, N.T.; Kennedy, N.A.; Adams, A.T.; Kalla, R.; Heath, S.; O’Leary, K.R.; Drummond, H.; Wilson, D.C.; Gut, I.G.; Nimmo, E.R.; et al. Integrative Epigenome-Wide Analysis Demonstrates That DNA Methylation May Mediate Genetic Risk in Inflammatory Bowel Disease. Nat. Commun. 2016, 7, 13507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkes, G.C.; Whelan, K.; Lindsay, J.O. Smoking in Inflammatory Bowel Disease: Impact on Disease Course and Insights into the Aetiology of Its Effect. J. Crohns Colitis 2014, 8, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, C. Inflammatory Bowel Disease Pathogenesis: Where are We? J. Gastroenterol. Hepatol. 2015, 30, 12–18. [Google Scholar] [CrossRef]
- Hou, J.K.; Lee, D.; Lewis, J. Diet and Inflammatory Bowel Disease: Review of Patient-Targeted Recommendations. Clin. Gastroenterol. Hepatol. 2014, 12, 1592–1600. [Google Scholar] [CrossRef] [Green Version]
- Narula, N.; Dhillon, A.; Zhang, D.; Sherlock, M.E.; Tondeur, M.; Zachos, M. Enteral Nutritional Therapy for Induction of Remission in Crohn’s Disease. Cochrane Database Syst. Rev. 2018, 4, 542. [Google Scholar] [CrossRef]
- Khalili, H.; Håkansson, N.; Chan, S.S.; Chen, Y.; Lochhead, P.; Ludvigsson, J.F.; Chan, A.T.; Hart, A.R.; Olén, O.; Wolk, A. Adherence to a Mediterranean Diet is Associated with a Lower Risk of Later-Onset Crohn’s Disease: Results from Two Large Prospective Cohort Studies. Gut 2020, 69, 1637–1644. [Google Scholar] [CrossRef]
- Lo, C.-H.; Lochhead, P.; Khalili, H.; Song, M.; Tabung, F.K.; Burke, K.E.; Richter, J.M.; Giovannucci, E.L.; Chan, A.T.; Ananthakrishnan, A.N. Dietary Inflammatory Potential and Risk of Crohn’s Disease and Ulcerative Colitis. Gastroenterology 2020, 159, 873–883. [Google Scholar] [CrossRef]
- Gottschall, E. Breaking the Vicious Cycle; Kirkton Press: Baltimore, ON, Canada, 1994. [Google Scholar]
- Kakodkar, S.; Farooqui, A.J.; Mikolaitis, S.L.; Mutlu, E.A. The Specific Carbohydrate Diet for Inflammatory Bowel Disease: A Case Series. J. Acad. Nutr. Diet. 2015, 115, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suskind, D.L.; Wahbeh, G.; Gregory, N.; Vendettuoli, H.; Christie, D. Nutritional Therapy in Pediatric Crohn Disease: The Specific Carbohydrate Diet. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Suskind, D.L.; Cohen, S.A.; Brittnacher, M.J.; Wahbeh, G.; Lee, D.; Shaffer, M.L.; Braly, K.; Hayden, H.S.; Klein, J.; Gold, B.; et al. Clinical and Fecal Microbial Changes With Diet Therapy in Active Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2018, 52, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Suskind, D.L.; Lee, D.; Kim, Y.-M.; Wahbeh, G.; Singh, N.; Braly, K.; Nuding, M.; Nicora, C.D.; Purvine, S.O.; Lipton, M.S.; et al. The Specific Carbohydrate Diet and Diet Modification as Induction Therapy for Pediatric Crohn’s Disease: A Randomized Diet Controlled Trial. Nutrients 2020, 12, 3749. [Google Scholar] [CrossRef]
- Suskind, D.L. Downloadable Papers|NIMBAL Therapy|Treat IBD with Diet|NIMBAL Therapy|Treat IBD with Diet. Available online: https://www.nimbal.org/education/implementing-scd-into-your-daily-life/downloadable-papers (accessed on 28 July 2021).
- Suskind, D.L. Specific Carbohydrate Diet (SCD) Legal & Illegal Foods|NiMBAL|NIMBAL Therapy|Treat IBD with Diet. Available online: https://www.nimbal.org/education/implementing-scd-into-your-daily-life/knowing-what-foods-are-legal-and-illegal (accessed on 28 July 2021).
- Kozuch, P.L.; Hanauer, S.B. Treatment of Inflammatory Bowel Disease: A Review of Medical Therapy. World J. Gastroenterol. 2008, 14, 354–377. [Google Scholar] [CrossRef] [PubMed]
- Hazel, K.; O’Connor, A. Emerging Treatments for Inflammatory Bowel Disease. Ther. Adv. Chronic Dis. 2020, 11. [Google Scholar] [CrossRef]
- Lindsay, J.O.; Armuzzi, A.; Gisbert, J.P.; Bokemeyer, B.; Peyrin-Biroulet, L.; Nguyen, G.C.; Smyth, M.; Patel, H. Indicators of Suboptimal Tumor Necrosis Factor Antagonist Therapy in Inflammatory Bowel Disease. Dig. Liver Dis. 2017, 49, 1086–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frolkis, A.D.; Dykeman, J.; Negrón, M.E.; Debruyn, J.; Jette, N.; Fiest, K.M.; Frolkis, T.; Barkema, H.W.; Rioux, K.P.; Panaccione, R.; et al. Risk of Surgery for Inflammatory Bowel Diseases Has Decreased over Time: A Systematic Review and Meta-Analysis of Population-Based Studies. Gastroenterology 2013, 145, 996–1006. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N. Surgery for Crohn’s Disease: Look Harder, Act Faster. Lancet 2015, 385, 1370–1371. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Loftus, E.V.; Colombel, J.-F.; Sandborn, W.J. The Natural History of Adult Crohn’s Disease in Population-Based Cohorts. Am. J. Gastroenterol. 2010, 105, 289–297. [Google Scholar] [CrossRef]
- Everhart, J.E. Burden of Digestive Diseases in the United States Report|NIDDK. Available online: https://www.niddk.nih.gov/about-niddk/strategic-plans-reports/burden-of-digestive-diseases-in-united-states/burden-of-digestive-diseases-in-the-united-states-report (accessed on 3 March 2021).
- Malarcher, C.A.; Wheaton, A.G.; Liu, Y.; Greenlund, S.F.; Greenlund, S.J.; Lu, H.; Croft, J.B. Hospitalizations for Crohn’s Disease—United States, 2003–2013. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Mehta, F. Report: Economic Implications of Inflammatory Bowel Disease and Its Management. Am. J. Manag. Care 2016, 22, s51–s60. [Google Scholar]
- Kappelman, M.D.; Rifas-Shiman, S.L.; Porter, C.Q.; Ollendorf, D.A.; Sandler, R.S.; Galanko, J.A.; Finkelstein, J.A. Direct Health Care Costs of Crohn’s Disease and Ulcerative Colitis in US Children and Adults. Gastroenterology 2008, 135, 1907–1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, G.; Rosenfeld, G.; Leung, Y.; Qian, H.; Raudzus, J.; Nunez, C.; Bressler, B. Prevalence of Anxiety and Depression in Patients with Inflammatory Bowel Disease. Can. J. Gastroenterol. Hepatol. 2017, 2017, 6496727. [Google Scholar] [CrossRef]
- Lee, D.; Albenberg, L.; Compher, C.; Baldassano, R.; Piccoli, D.; Lewis, J.D.; Wu, G.D. Diet in the Pathogenesis and Treatment of Inflammatory Bowel Diseases. Gastroenterology 2015, 148, 1087–1106. [Google Scholar] [CrossRef] [Green Version]
- Khandalavala, B.N.; Nirmalraj, M.C. Resolution of Severe Ulcerative Colitis with the Specific Carbohydrate Diet. Case Rep. Gastroenterol. 2015, 9, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Saygili, F.; Saygili, S.M.; Tenlik, I.; Yuksel, M.; Kilic, Z.M.Y.; Ozin, Y.O.; Kayacetin, E. Crohn’s Disease in the Elderly: Clinical Presentation and Manifestations from a Tertiary Referral Center in Turkey. North. Clin. Istanb. 2017, 3, 183–186. [Google Scholar] [CrossRef] [Green Version]
- Rajendran, N.; Kumar, D. Role of Diet in the Management of Inflammatory Bowel Disease. World J. Gastroenterol. WJG 2010, 16, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Fell, J.M.; Paintin, M.; Arnaud-Battandier, F.; Beattie, R.M.; Hollis, A.; Kitching, P.; Donnet-Hughes, A.; MacDonald, T.T.; Walker-Smith, J.A. Mucosal Healing and a Fall in Mucosal Pro-Inflammatory Cytokine MRNA Induced by a Specific Oral Polymeric Diet in Paediatric Crohn’s Disease. Aliment. Pharmacol. Ther. 2000, 14, 281–289. [Google Scholar] [CrossRef]
- Shiga, H.; Kajiura, T.; Shinozaki, J.; Takagi, S.; Kinouchi, Y.; Takahashi, S.; Negoro, K.; Endo, K.; Kakuta, Y.; Suzuki, M.; et al. Changes of Faecal Microbiota in Patients with Crohn’s Disease Treated with an Elemental Diet and Total Parenteral Nutrition. Dig. Liver Dis. 2012, 44, 736–742. [Google Scholar] [CrossRef]
- Zamani, S.; Hesam Shariati, S.; Zali, M.R.; Asadzadeh Aghdaei, H.; Sarabi Asiabar, A.; Bokaie, S.; Nomanpour, B.; Sechi, L.A.; Feizabadi, M.M. Detection of Enterotoxigenic Bacteroides Fragilis in Patients with Ulcerative Colitis. Gut Pathog. 2017, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ercolini, D.; Fogliano, V. Food Design to Feed the Human Gut Microbiota. J. Agric. Food Chem. 2018, 66, 3754–3758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiba, M.; Tsuji, T.; Nakane, K.; Komatsu, M. High Amount of Dietary Fiber Not Harmful But Favorable for Crohn Disease. Perm. J. 2015, 19, 58–61. [Google Scholar] [CrossRef] [Green Version]
- Pituch-Zdanowska, A.; Banaszkiewicz, A.; Albrecht, P. The Role of Dietary Fibre in Inflammatory Bowel Disease. PRZEGLAD Gastroenterol. 2015, 10, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.D. The Role of Diet in Inflammatory Bowel Disease. Gastroenterol. Hepatol. 2016, 12, 51–53. [Google Scholar]
- Nolan-Clark, D.; Tapsell, L.C.; Hu, R.; Han, D.Y.; Ferguson, L.R. Effects of Dairy Products on Crohn’s Disease Symptoms Are Influenced by Fat Content and Disease Location but Not Lactose Content or Disease Activity Status in a New Zealand Population. J. Am. Diet. Assoc. 2011, 111, 1165–1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakodkar, S.; Mutlu, E.A. Diet as a Therapeutic Option for Adult Inflammatory Bowel Disease. Gastroenterol. Clin. N. Am. 2017, 46, 745–767. [Google Scholar] [CrossRef] [PubMed]
- Swanson, G.R.; Sedghi, S.; Farhadi, A.; Keshavarzian, A. Pattern of Alcohol Consumption and Its Effect on Gastrointestinal Symptoms in Inflammatory Bowel Disease. Alcohol 2010, 44, 223–228. [Google Scholar] [CrossRef] [Green Version]
- D’Haens, G.; Ferrante, M.; Vermeire, S.; Baert, F.; Noman, M.; Moortgat, L.; Geens, P.; Iwens, D.; Aerden, I.; Van Assche, G.; et al. Fecal Calprotectin is a Surrogate Marker for Endoscopic Lesions in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2012, 18, 2218–2224. [Google Scholar] [CrossRef]
- Grand, D.J.; Kampalath, V.; Harris, A.; Patel, A.; Resnick, M.B.; Machan, J.; Beland, M.; Chen, W.T.; Shah, S.A. MR Enterography Correlates Highly with Colonoscopy and Histology for Both Distal Ileal and Colonic Crohn’s Disease in 310 Patients. Eur. J. Radiol. 2012, 81, e763–e769. [Google Scholar] [CrossRef]
- Khater, N.H.; Fahmy, H.S.; Ali, H.I. Value of MR Enterography in Assessment of Crohn’s Disease: Correlation with Capsule Endoscopy and Colonoscopy. Egypt. J. Radiol. Nucl. Med. 2017, 48, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Braly, K.; Williamson, N.; Shaffer, M.L.; Lee, D.; Wahbeh, G.; Klein, J.; Giefer, M.; Suskind, D.L. Nutritional Adequacy of the Specific Carbohydrate Diet in Pediatric Inflammatory Bowel Disease. J. Pediatr Gastroenterol Nutr 2017, 65, 533–538. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Fecal Calprotectin Results (10 April 2018–17 June 21).

Figure 2.
C-reactive protein results (10 April 2018–17 June 21).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mehrtash, F. Sustained Crohn’s Disease Remission with an Exclusive Elemental and Exclusion Diet: A Case Report. Gastrointest. Disord. 2021, 3, 129-137. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3030014
AMA Style
Mehrtash F. Sustained Crohn’s Disease Remission with an Exclusive Elemental and Exclusion Diet: A Case Report. Gastrointestinal Disorders. 2021; 3(3):129-137. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3030014
Chicago/Turabian StyleMehrtash, Farhad. 2021. "Sustained Crohn’s Disease Remission with an Exclusive Elemental and Exclusion Diet: A Case Report" Gastrointestinal Disorders 3, no. 3: 129-137. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord3030014