
Disclosing Critical Voice Features for Discriminating between Depression and Insomnia—A Preliminary Study for Developing a Quantitative Method


Abstract
:1. Introduction
1.1. Depression vs. Insomnia
1.2. Diagnoses of Depression and Insomnia
1.3. Speech Voice May Help Diagnoses
1.4. Research Objective
2. Materials and Methods
2.1. Participants and Clinical Assessment
2.2. Collection and Preprocessing of the Speech Voice
2.3. Voice Features Extraction and Statistical Analysis
3. Results
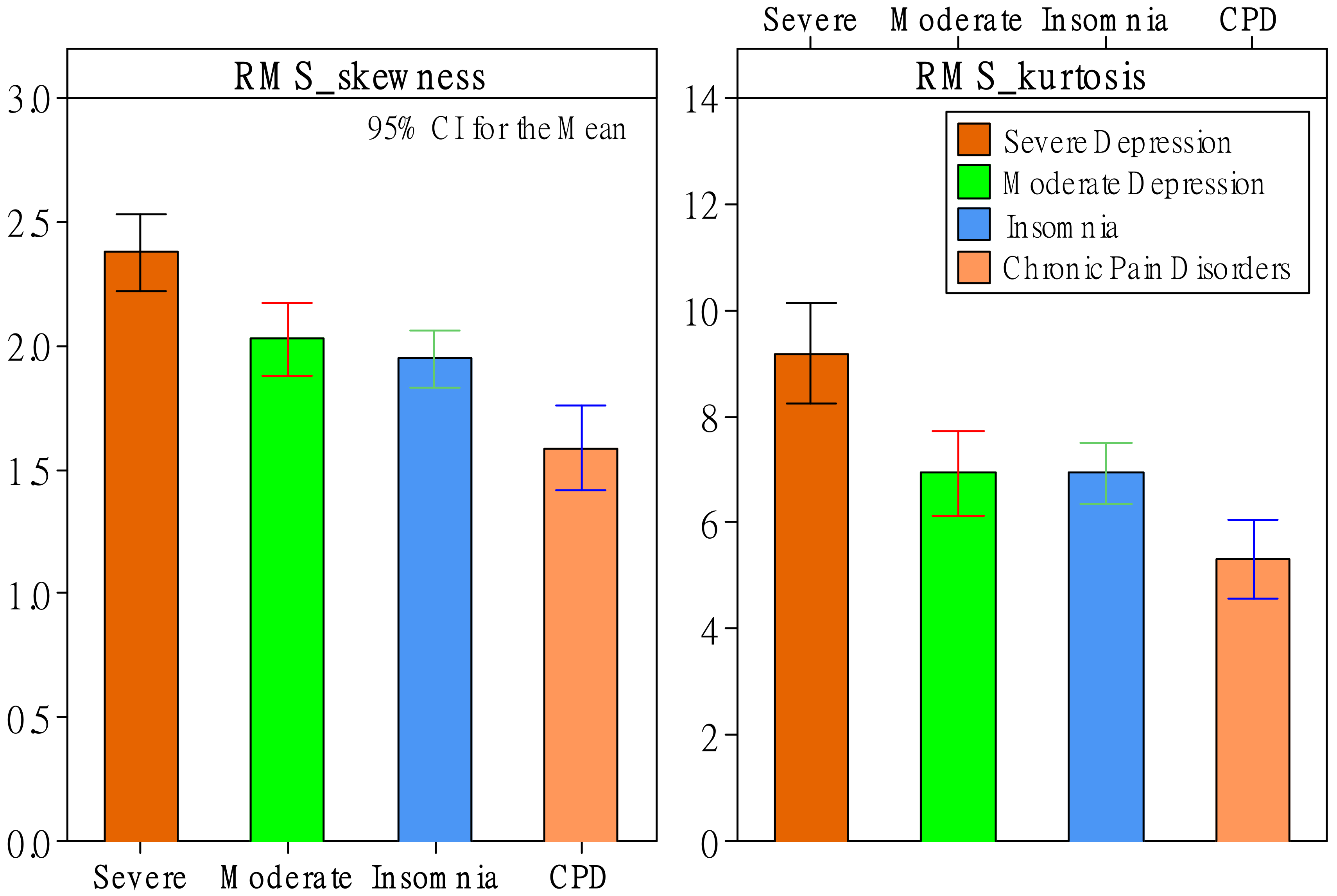
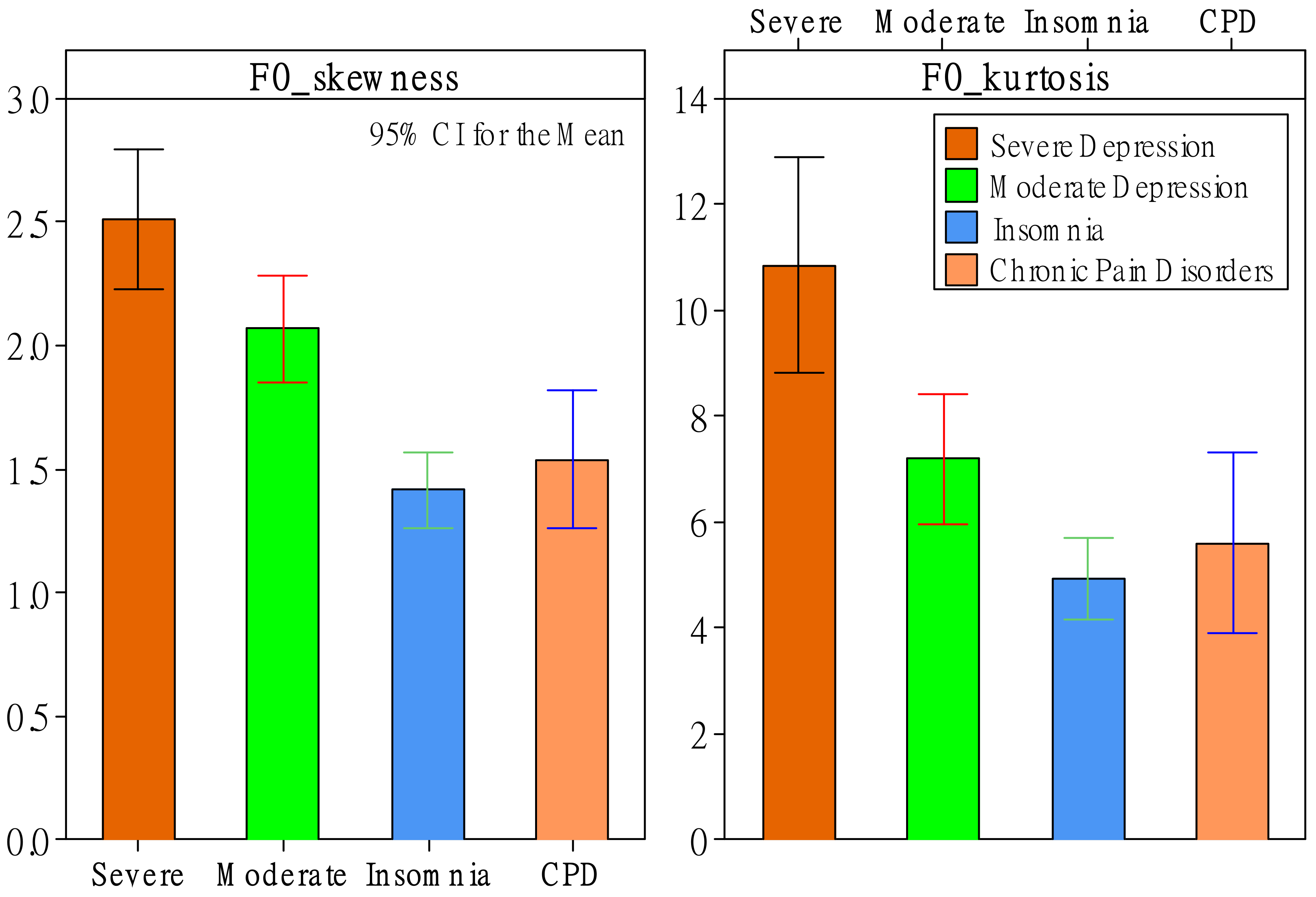
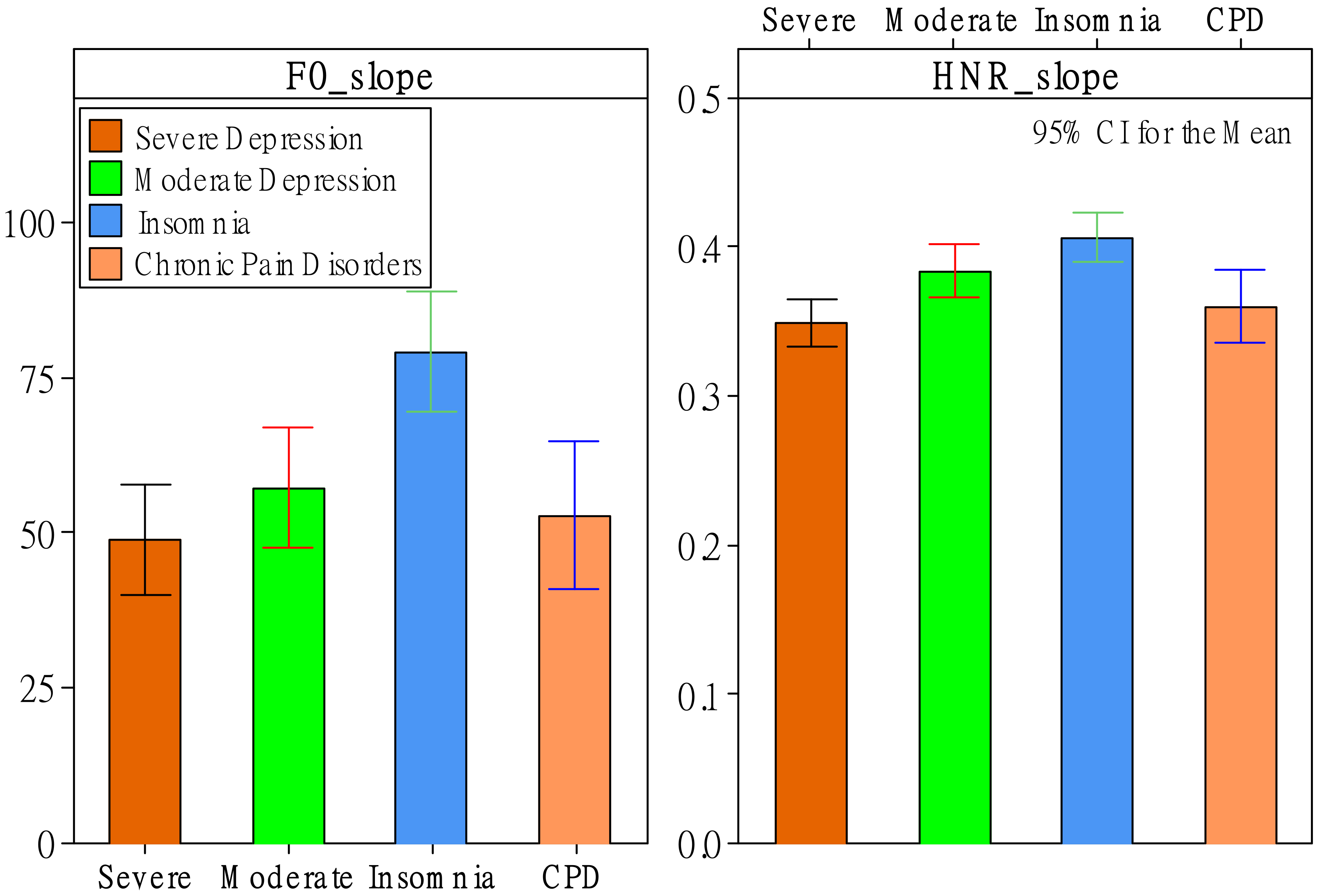
3.1. Effects of Patient Status
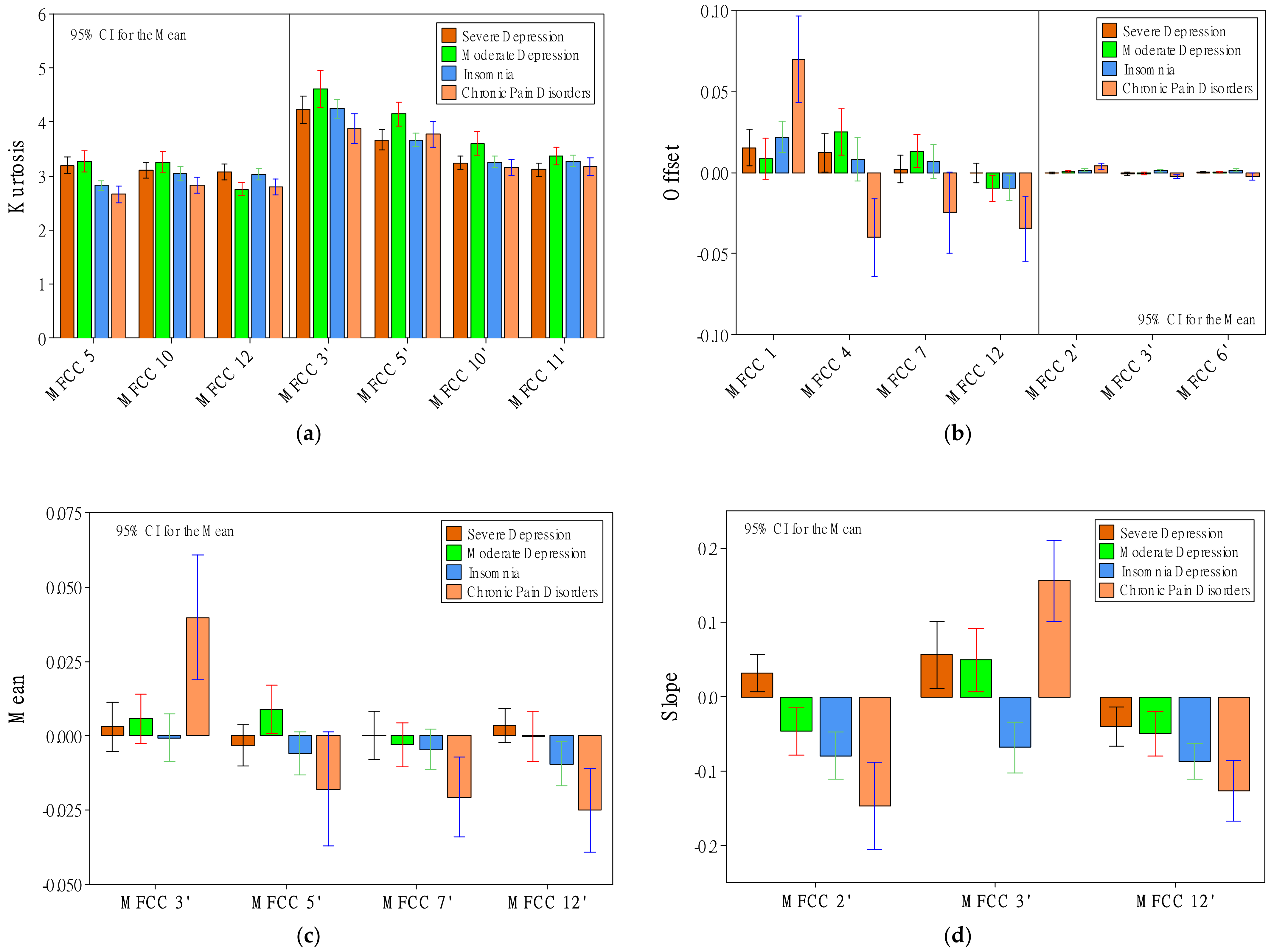
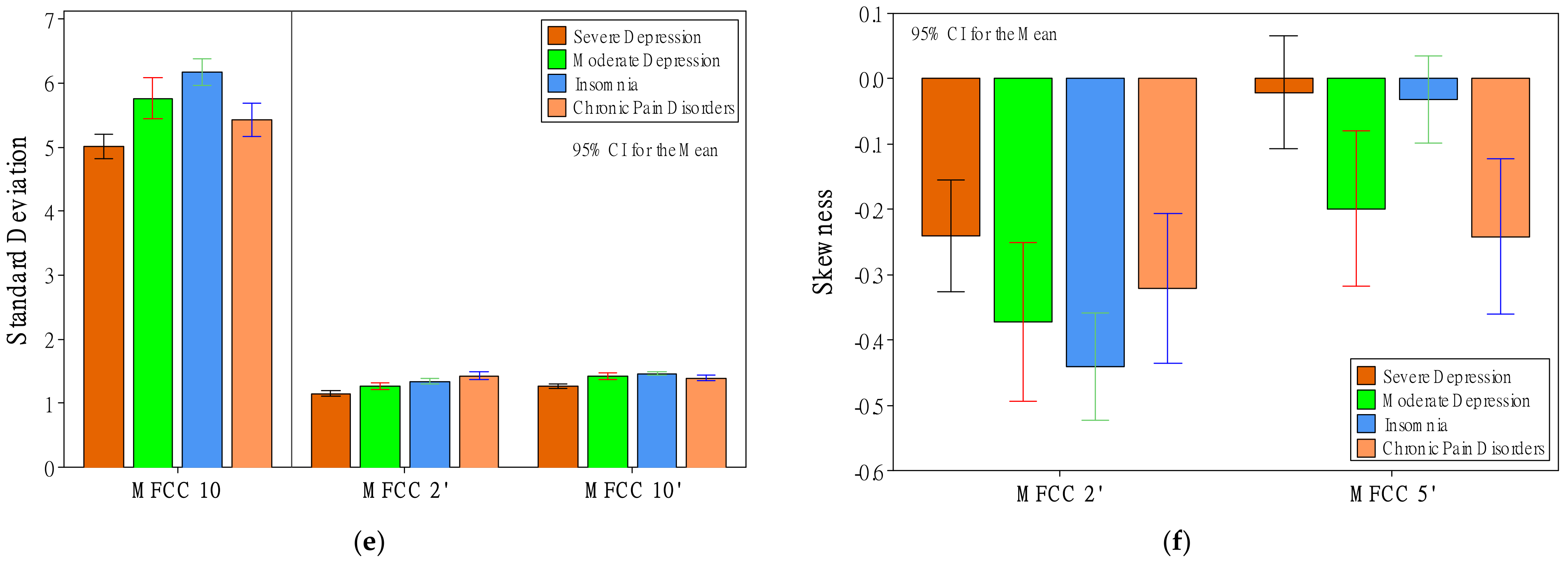
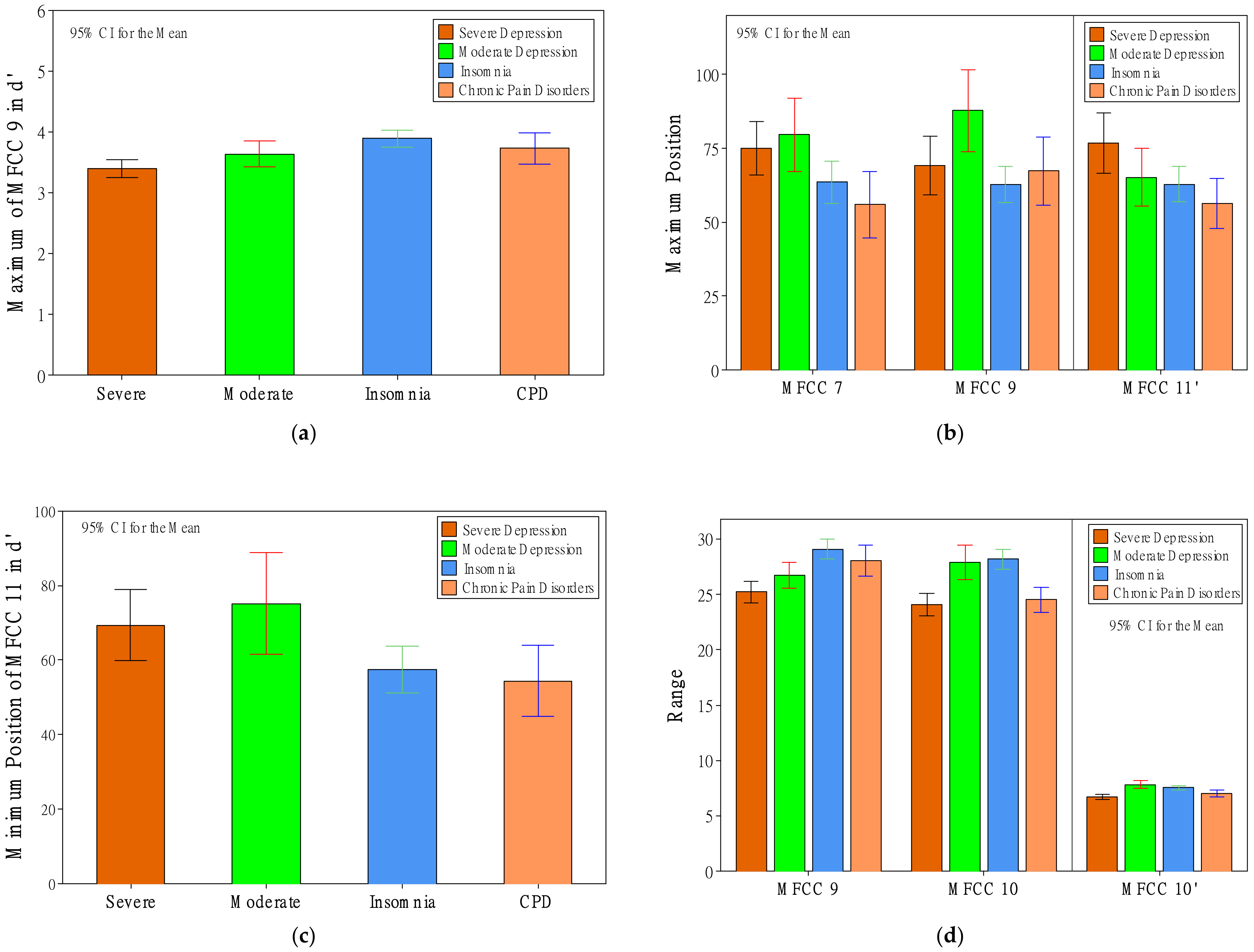
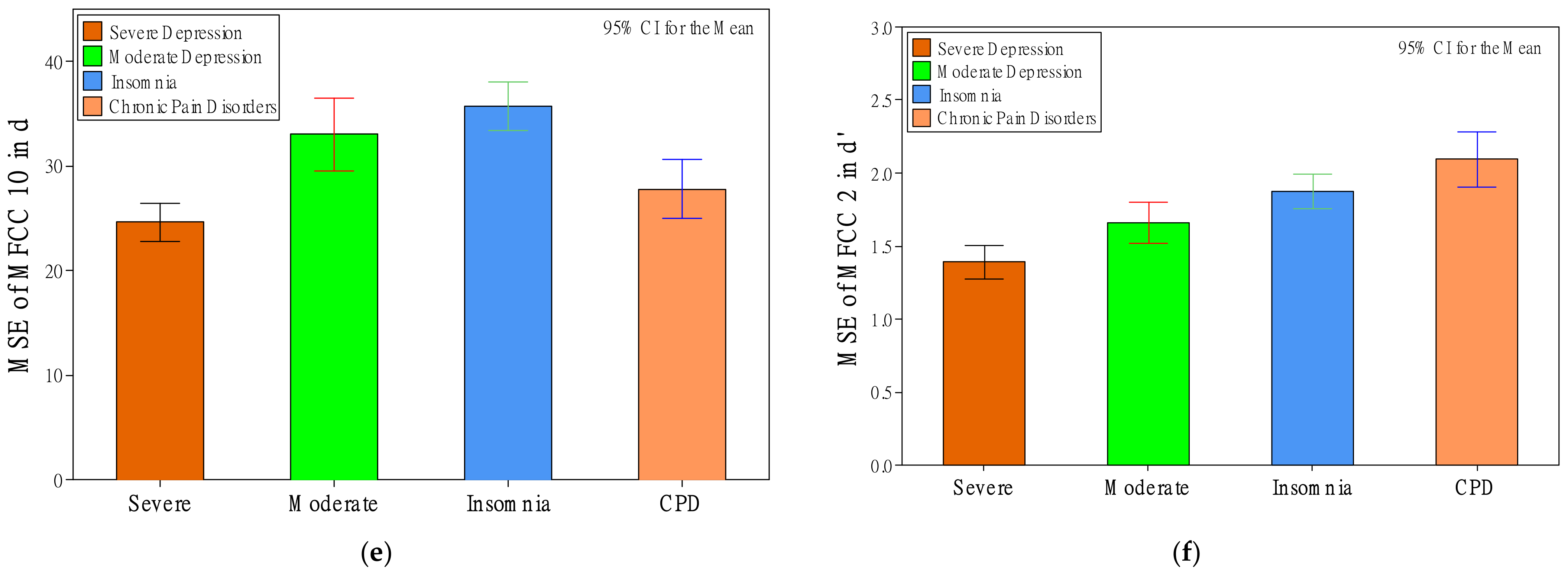
3.2. Effects of Patient Status on MFCC
3.3. Effects of Gender and Interaction Effects of Status and Gender
4. Discussion
4.1. Voice Features Show the Differences among Patient Groups
4.2. Considerations of Gender Effects
4.3. Contributions and Implications
4.4. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Morin, C.M.; LeBlanc, M.; Daley, M.; Gregoire, J.; Merette, C. Epidemiology of insomnia: Prevalence, self-help treatments, consultations, and determinants of help-seeking behaviors. Sleep Med. 2006, 7, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Observation of the natural evolution of insomnia in the American general population cohort. Sleep Med. Clin. 2009, 4, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Pandey, S.; Phillips, B.A. Why is the prevalence of insomnia skyrocketing? And what can be done about it? Sleep Med. 2015, 16, 555–556. [Google Scholar] [CrossRef]
- Theorell-Haglöw, J.; Miller, C.B.; Bartlett, D.J.; Yee, B.J.; Openshaw, H.D.; Grunstein, R.R. Gender differences in obstructive sleep apnoea, insomnia and restless legs syndrome in adults–What do we know? A clinical update. Sleep Med. Rev. 2018, 38, 28–38. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, R.; Lei, F.; Zhou, J.; Zhang, J.; Wing, Y.-K.; Sanford, L.D.; Tang, X. Worldwide and regional prevalence rates of co-occurrence of insomnia and insomnia symptoms with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 45, 1–17. [Google Scholar] [CrossRef]
- Benca, R.M. Diagnosis and treatment of chronic insomnia: A review. Psychiatr. Serv. 2005, 56, 332–343. [Google Scholar] [CrossRef]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H. Insomnia as a health risk factor. Behav. Sleep Med. 2003, 1, 227–247. [Google Scholar] [CrossRef]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H.; Reidel, B.W.; Bush, A.J. Epidemiology of insomnia, depression, and anxiety. Sleep 2005, 28, 1457–1464. [Google Scholar] [CrossRef]
- Irwin, M.R. Depression and insomnia in cancer: Prevalence, risk factors, and effects on cancer outcomes. Curr. Psychiatry Rep. 2013, 15, 404. [Google Scholar] [CrossRef] [Green Version]
- Fiorentino, L.; Rissling, M.; Liu, L.; Ancoli-Israel, S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: Severity of the problem and treatment options. Drug Today Dis. Models 2011, 8, 167–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, A.G. Insomnia: Symptom or diagnosis? Clin. Psychol. Rev. 2001, 21, 1037–1059. [Google Scholar] [CrossRef]
- Taylor, D.; Walters, H.; Krebaum, S.; Kraft, D.; Jarrett, R. Does Residual Insomnia Predict Depressive Relapse and Recurrence in Cognitive Therapy Responders? Sleep 2004, 27, 346–347. [Google Scholar]
- Lichstein, K.L.; Durrence, H.H.; Riedel, B.W.; Taylor, D.J.; Bush, A.J. Epidemiology of Sleep: Age, Gender, and Ethnicity; Psychology Press: Hove, UK, 2013. [Google Scholar]
- DeRubeis, R.J.; Siegle, G.J.; Hollon, S.D. Cognitive therapy versus medication for depression: Treatment outcomes and neural mechanisms. Nat. Rev. Neurosci. 2008, 9, 788–796. [Google Scholar] [CrossRef]
- Mitchell, M.D.; Gehrman, P.; Perlis, M.; Umscheid, C.A. Comparative effectiveness of cognitive behavioral therapy for insomnia: A systematic review. BMC Fam. Pract. 2012, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Okajima, I.; Komada, Y.; Inoue, Y. A meta-analysis on the treatment effectiveness of cognitive behavioral therapy for primary insomnia. Sleep Biol. Rhythm. 2011, 9, 24–34. [Google Scholar] [CrossRef]
- Girard, J.M.; Cohn, J.F. Automated audiovisual depression analysis. Curr. Opin. Psychol. 2015, 4, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Solomon, C.; Valstar, M.F.; Morriss, R.K.; Crowe, J. Objective methods for reliable detection of concealed depression. Front. ICT 2015, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in psychiatric outpatients. J. Personal. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Asgari, M.; Shafran, I.; Sheeber, L.B. Inferring Clinical Depression from Speech and Spoken Utterances. In Proceedings of the MLSP, Reims, France, 21–24 September 2014; pp. 1–5. [Google Scholar]
- Schramm, E.; Hohagen, F.; Grasshoff, U.; Riemann, D.; Hajak, G.; Weess, H.; Berger, M. Test-retest reliability and validity of the Structured Interview for Sleep Disorders According to DSM-III—R. Am. J. Psychiatry 1993, 150, 867–872. [Google Scholar] [PubMed]
- Roth, T. New developments for treating sleep disorders. J. Clin. Psychiatry 2001, 62, 3–4. [Google Scholar] [PubMed]
- Chiu, H.-Y.; Chang, L.-Y.; Hsieh, Y.-J.; Tsai, P.-S. A meta-analysis of diagnostic accuracy of three screening tools for insomnia. J. Psychosom. Res. 2016, 87, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Munson, B.; Babel, M. The phonetics of sex and gender. In The Routledge Handbook of Phonetics; Routledge: London, UK, 2019; pp. 499–525. [Google Scholar]
- Simpson, A.P. Phonetic differences between male and female speech. Lang. Linguist. Compass 2009, 3, 621–640. [Google Scholar] [CrossRef]
- Hancock, A.; Colton, L.; Douglas, F. Intonation and gender perception: Applications for transgender speakers. J. Voice 2014, 28, 203–209. [Google Scholar] [CrossRef]
- Scherer, K.R. Vocal affect expression: A review and a model for future research. Psychol. Bull. 1986, 99, 143–165. [Google Scholar] [CrossRef]
- Williamson, J.R.; Young, D.; Nierenberg, A.A.; Niemi, J.; Helfer, B.S.; Quatieri, T.F. Tracking depression severity from audio and video based on speech articulatory coordination. Comput. Speech Lang. 2018, 55, 40–56. [Google Scholar] [CrossRef]
- Cummins, N.; Scherer, S.; Krajewski, J.; Schnieder, S.; Epps, J.; Quatieri, T.F. A review of depression and suicide risk assessment using speech analysis. Speech Commun. 2015, 71, 10–49. [Google Scholar] [CrossRef]
- Gumelar, A.B.; Kurniawan, A.; Sooai, A.G.; Purnomo, M.H.; Yuniarno, E.M.; Sugiarto, I.; Widodo, A.; Kristanto, A.A.; Fahrudin, T.M. Human Voice Emotion Identification Using Prosodic and Spectral Feature Extraction Based on Deep Neural Networks. In Proceedings of the 2019 IEEE 7th International Conference on Serious Games and Applications for Health (SeGAH), Kyoto, Japan, 5–7 August 2019; pp. 1–8. [Google Scholar]
- Moore II, E.; Clements, M.A.; Peifer, J.W.; Weisser, L. Critical analysis of the impact of glottal features in the classification of clinical depression in speech. IEEE Trans. Biomed. Eng. 2007, 55, 96–107. [Google Scholar] [CrossRef]
- Alghowinem, S.; Goecke, R.; Wagner, M.; Epps, J.; Gedeon, T.; Breakspear, M.; Parker, G. A Comparative Study of Different Classifiers for Detecting Depression from Spontaneous Speech. In Proceedings of the 2013 IEEE International Conference on Acoustics, Speech and Signal Processing, Vancouver, BC, Canada, 26–31 May 2013; pp. 8022–8026. [Google Scholar]
- Cohn, J.F.; Kruez, T.S.; Matthews, I.; Yang, Y.; Nguyen, M.H.; Padilla, M.T.; Zhou, F.; de la Torre, F. Detecting Depression from Facial Actions and Vocal Prosody. In Proceedings of the 2009 3rd International Conference on Affective Computing and Intelligent Interaction and Workshops, Amsterdam, The Netherlands, 10–12 September 2009; pp. 1–7. [Google Scholar]
- Alghowinem, S.; Goecke, R.; Cohn, J.F.; Wagner, M.; Parker, G.; Breakspear, M. Cross-Cultural Detection of Depression from Nonverbal Behaviour. In Proceedings of the 2015 11th IEEE International Conference and Workshops on Automatic Face and Gesture Recognition (FG), Ljubljana, Slovenia, 4–8 May 2015; pp. 1–8. [Google Scholar]
- Heydarifard, Z.; Krasikova, D. Voice and Insomnia: A Daily Study of Underlying Affective and Cognitive Mechanisms. In Proceedings of the Academy of Management Proceedings, Briarcliff Manor, NY, USA, Virtual. 26 July 2021; p. 15460. [Google Scholar]
- Endicott, J.; Cohen, J.; Nee, J.; Fleiss, J.; Sarantakos, S. Hamilton Depression Rating Scale: Extracted from regular and change versions of the Schedule for Affective Disorders and Schizophrenia. Arch. Gen. Psychiatry 1981, 38, 98–103. [Google Scholar] [CrossRef]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity classification on the Hamilton depression rating scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Che, H.H.; Lu, M.L.; Chen, H.C.; Chang, S.W.; Lee, Y.J. Validation of the Chinese version of the Beck Anxiety Inventory. Formos. J. Med. 2006, 10, 451–452. [Google Scholar]
- Schuller, B.; Steidl, S.; Batliner, A. The Interspeech 2009 Emotion Challenge. In Proceedings of the Tenth Annual Conference of the International Speech Communication Association, Brighton, UK, 6–10 September 2009. [Google Scholar]
- Cao, W.-H.; Xu, J.-P.; Liu, Z.-T. Speaker-Independent Speech Emotion Recognition Based on Random Forest Feature Selection Algorithm. In Proceedings of the 36th Chinese Control Conference (CCC), Dalian, China, 26–28 July 2017; pp. 10995–10998. [Google Scholar]
- Gangamohan, P.; Kadiri, S.R.; Yegnanarayana, B. Analysis of Emotional Speech—A Review. In Toward Robotic Socially Believable Behaving Systems—Volume I; Intelligent Systems Reference Library; Springer: Cham, Switzerland, 2016; pp. 205–238. [Google Scholar]
- Murray, I.R.; Arnott, J.L. Toward the simulation of emotion in synthetic speech: A review of the literature on human vocal emotion. J. Acoust. Soc. Am. 1993, 93, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Kiss, G.; Vicsi, K. Seasonal affective disorder speech detection on the base of acoustic phonetic speech parameters. Acta Univ. Sapientiae Electr. Mech. Eng. 2015, 7, 62–79. [Google Scholar]
- Taguchi, T.; Tachikawa, H.; Nemoto, K.; Suzuki, M.; Nagano, T.; Tachibana, R.; Nishimura, M.; Arai, T. Major depressive disorder discrimination using vocal acoustic features. J. Affect. Disord. 2018, 225, 214–220. [Google Scholar] [CrossRef]
- Sardari, S.; Nakisa, B.; Rastgoo, M.N.; Eklund, P. Audio based depression detection using Convolutional Autoencoder. Expert Syst. Appl. 2022, 189, 189–116076. [Google Scholar] [CrossRef]
- Kwon, N.; Kim, S. Depression Severity Detection Using Read Speech with a Divide-and-Conquer Approach. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, (Virtual). 1–5 November 2021; pp. 633–637. [Google Scholar]
- Zhao, Y.; Xie, Y.; Liang, R.; Zhang, L.; Zhao, L.; Liu, C. Detecting Depression from Speech through an Attentive LSTM Network. IEICE Trans. Inf. Syst. 2021, 104, 2019–2023. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Effects | Original Descriptors (d) | De-Differentiated Descriptors (d’) | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | ||
| RMS | * | * | |||||||||||||||||||||||
| ZCR | ^ | ^ | ^ | ^ | |||||||||||||||||||||
| F0 | ^ | ● | * | * | ^ | ||||||||||||||||||||
| HNR | ^ | * | |||||||||||||||||||||||
| MFCC | 1 | * | |||||||||||||||||||||||
| 2 | ^ | * | * | ● | * | * | |||||||||||||||||||
| 3 | * | * | ● | ■ | |||||||||||||||||||||
| 4 | * | ||||||||||||||||||||||||
| 5 | ● | * | * | ||||||||||||||||||||||
| 6 | * | ^ | * | * | ^ | ||||||||||||||||||||
| 7 | * | * | * | ||||||||||||||||||||||
| 8 | |||||||||||||||||||||||||
| 9 | ^ | * | * | ^ | * | ^ | ^ | ^ | |||||||||||||||||
| 10 | * | * | ^ | * | ^ | * | * | ● | ^ | ^ | * | ^ | ^ | ||||||||||||
| 11 | ^ | ^ | * | * | ^ | ||||||||||||||||||||
| 12 | ● | * | ● | ^ | * | ||||||||||||||||||||
| Effects | Original Descriptors (d) | De-Differentiated Descriptors (d’) | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | ||
| RMS | * | ^ | |||||||||||||||||||||||
| ZCR | * | * | * | * | ^ | ^ | ● | ||||||||||||||||||
| F0 | * | ^ | |||||||||||||||||||||||
| HNR | * | ^ | * | ^ | ^ | ||||||||||||||||||||
| MFCC | 1 | ^ | ^ | * | * | ||||||||||||||||||||
| 2 | ^ | ^ | |||||||||||||||||||||||
| 3 | |||||||||||||||||||||||||
| 4 | ^ | ||||||||||||||||||||||||
| 5 | * | ^ | |||||||||||||||||||||||
| 6 | ^ | ^ | ^ | ^ | |||||||||||||||||||||
| 7 | * | ● | * | ^ | ^ | * | ^ | * | * | ||||||||||||||||
| 8 | |||||||||||||||||||||||||
| 9 | * | ^ | * | * | * | * | * | ^ | ● | * | |||||||||||||||
| 10 | * | ^ | ● | ● | ● | ● | ^ | * | * | * | |||||||||||||||
| 11 | * | ● | ● | ● | ^ | ^ | |||||||||||||||||||
| 12 | * | ^ | * | * | ■ | * | ● | ^ | |||||||||||||||||
| Effects | Original Descriptors (d) | De-Differentiated Descriptors (d’) | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | Mean | SD | Skewness | Kurtosis | Max Value | Min Value | Max Position | Min Position | Range | Offset | Slope | MSE | ||
| RMS | |||||||||||||||||||||||||
| ZCR | |||||||||||||||||||||||||
| F0 | |||||||||||||||||||||||||
| HNR | |||||||||||||||||||||||||
| MFCC | 1 | ||||||||||||||||||||||||
| 2 | * | ^ | |||||||||||||||||||||||
| 3 | ^ | * | * | ||||||||||||||||||||||
| 4 | |||||||||||||||||||||||||
| 5 | |||||||||||||||||||||||||
| 6 | |||||||||||||||||||||||||
| 7 | * | ||||||||||||||||||||||||
| 8 | ^ | ^ | |||||||||||||||||||||||
| 9 | * | * | |||||||||||||||||||||||
| 10 | ^ | ^ | ^ | * | ^ | ||||||||||||||||||||
| 11 | ^ | ||||||||||||||||||||||||
| 12 | * | ^ | ● | ||||||||||||||||||||||
| Feature Category | Original Descriptor (d) | De-Differentiated Descriptor (d’) | ||||
|---|---|---|---|---|---|---|
| Emotion Study | Depression Study | This Study | This Study | |||
| RMS | Mean▼ [43,44] Range▼ [43] | – | Skewness▲ |  | – | |
| Kurtosis▲ |  | – | ||||
| ZCR | – | – | – | – | ||
| F0 | Mean▼ [43] Range▼ [43] | Mean▼ [45] | Skewness▲ |  | – | |
| Kurtosis▲ |  | – | ||||
| Slope▼ |  | – | ||||
| HNR | Mean▲ [44] | – | Slope: ▼ |  | – | |
| MFCC 1 | – | – | – | – | ||
| MFCC 2 | – | Mean▲ [46] | – | SD’▼ |  | |
| – | Offset’▼ |  | ||||
| – | Slope’▲ |  | ||||
| – | MSE’▼ |  | ||||
| MFCC 3 | – | – | – | Offset’ |  | |
| – | Slope’ |  | ||||
| MFCC 4 | – | Max? [19] | – | – | ||
| MFCC 5 | – | Mean? [19] Max? [19] Min? [19] | Kurtosis▲ |  | – | |
| MFCC 6 | – | – | – | Offset’ |  | |
| MFCC 7 | – | – | Max P.▲ |  | – | |
| MFCC 8 | – | Max? [19] | – | – | ||
| MFCC 9 | – | – | Range▼ |  | Max’▼ |  |
| MFCC 10 | – | Max? [19] | SD▼ |  | SD’▼ |  |
| MSE▼ |  | Range’▼ |  | |||
| MFCC 11 | – | – | – | Max’▲ |  | |
| – | Min P’▲ |  | ||||
| MFCC 12 | – | – | Offset▲ |  | Slope’▲ |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, R.F.; Leung, T.-K.; Liu, Y.-P.; Hu, K.-R. Disclosing Critical Voice Features for Discriminating between Depression and Insomnia—A Preliminary Study for Developing a Quantitative Method. Healthcare 2022, 10, 935. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050935
Lin RF, Leung T-K, Liu Y-P, Hu K-R. Disclosing Critical Voice Features for Discriminating between Depression and Insomnia—A Preliminary Study for Developing a Quantitative Method. Healthcare. 2022; 10(5):935. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050935
Chicago/Turabian StyleLin, Ray F., Ting-Kai Leung, Yung-Ping Liu, and Kai-Rong Hu. 2022. "Disclosing Critical Voice Features for Discriminating between Depression and Insomnia—A Preliminary Study for Developing a Quantitative Method" Healthcare 10, no. 5: 935. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050935