
Morphological Comparison of the Maxillary Arch in Buccal and Palatal Canine Impaction among Asian Population of Gujarati Origin: A Hospital-Based Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Settings
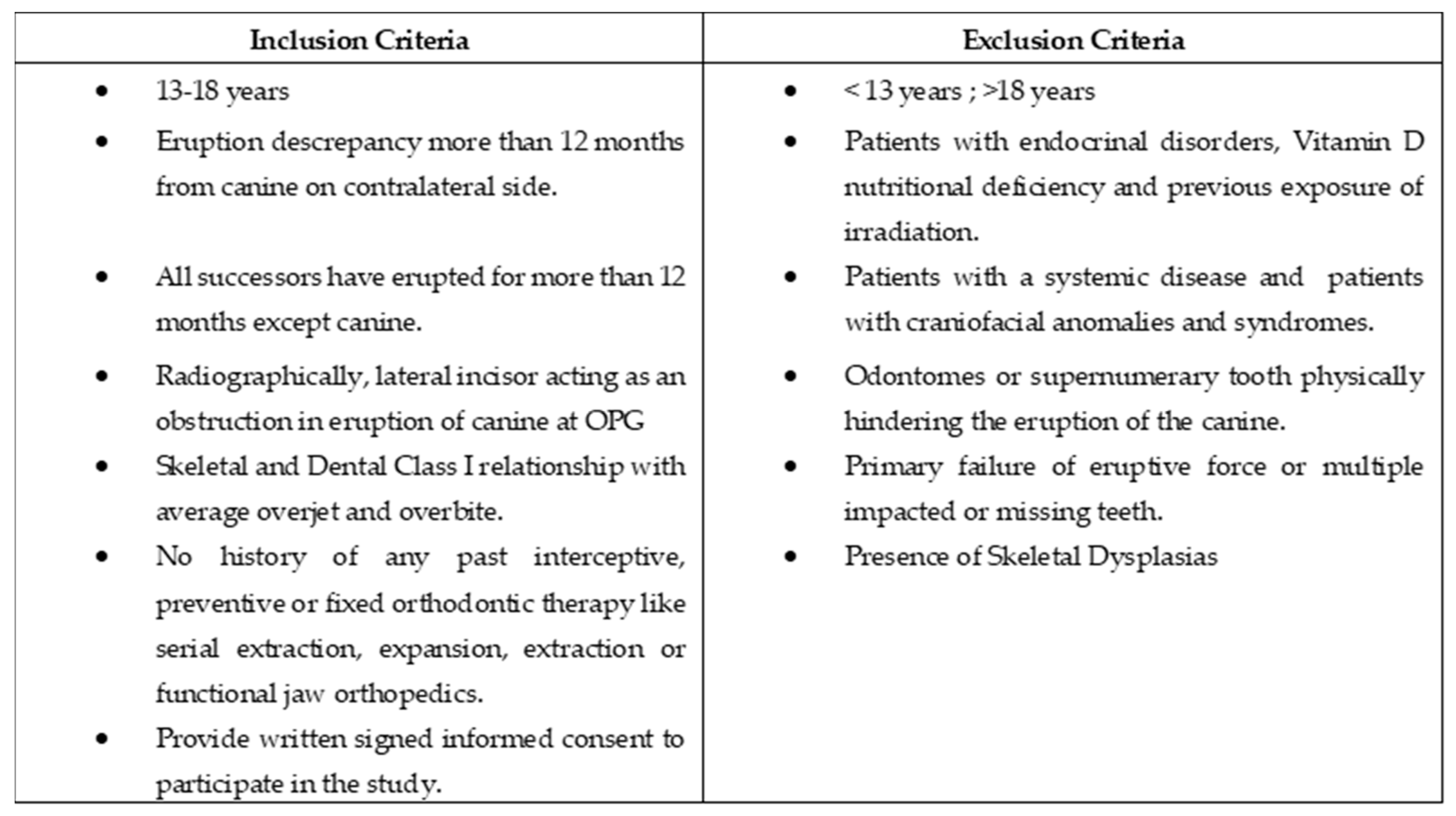
2.2. Participants
2.3. Landmarks and Measurements
2.4. Data Analysis
3. Results
3.1. Sample Demographics of Buccal, Palatal MIC and Controls
3.2. Comparison among Buccal, Palatal MIC and Control Group
4. Discussion
4.1. Clinical Implication
4.2. Limitation
5. Conclusions
- Inadequate arch length (p < 0.0001) and a higher degree of crowding with reduced available arch space (p < 0.0001) may be considered as early risk factors for buccal maxillary canine impaction.
- An inadequate inter-molar width (p < 0.0001), and increased palatal depth (p < 0.0001) with a clinically reduced mesiodistal width of the sum of maxillary incisors, may be considered as a risk factor for palatal maxillary canine impaction in an Asian population of Gujarati origin.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Becker, A. General principles related to the diagnosis and treatment of impacted teeth. In The Orthodontic Treatment of Impacted Teeth, 2nd ed.; Martin Dunitz: London, UK, 2007; pp. 1–11. [Google Scholar]
- Miletich, I.; Sharpe, P.T. Normal and abnormal dental development. Hum. Mol. Genet. 2003, 12, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, A. Radiographic methods related to the diagnosis of impacted teeth. In The Orthodontic Treatment of Impacted Teeth, 2nd ed.; Martin Dunitz: London, UK, 2007; pp. 13–24. [Google Scholar]
- Patil, S.; Maheshwari, S. Prevalence of impacted and supernumerary teeth in the North Indian population. J. Clin. Exp. Dent. 2014, 6, e116–e120. [Google Scholar] [CrossRef] [PubMed]
- Fardi, A.; Kondylidou-Sidira, A.; Bachour, Z.; Parisis, N.; Tsirlis, A. Incidence of impacted and supernumerary teeth-a radiographicStudy in a North Greek population. Oral Surg. 2011, 16, e56–e61. [Google Scholar] [CrossRef] [Green Version]
- Alyami, B.; Braimah, R.; Alharieth, S. Prevalence and pattern of impacted canines in Najran, South Western Saudi Arabian population. Saudi Dent. J. 2020, 32, 300–305. [Google Scholar] [CrossRef]
- Lövgren, M.L.; Dahl, O.; Uribe, P.; Ransjö, M.; Westerlund, A. Prevalence of impacted maxillary canines—An epidemiological study in a region with systematically implemented interceptive treatment. Eur. J. Orthod. 2019, 41, 454–459. [Google Scholar] [CrossRef]
- Celikoglu, M.; Kamak, H.; Oktay, H. Investigation of Transmigrated and Impacted Maxillary and Mandibular Canine Teeth in an Orthodontic Patient Population. J. Oral Maxillofac. Surg. 2010, 68, 1001–1006. [Google Scholar] [CrossRef]
- Thilander, B.; Jakobsson, S.O. Local factors in impaction of maxillary canines. Acta Odontol. Scand. 1968, 26, 145–168. [Google Scholar] [CrossRef]
- Papagiannis, A.; Halazonetis, D.J. Shape variation and covariation of upper and lower dental arches of an orthodontic population. Eur. J. Orthod. 2016, 38, 202–211. [Google Scholar] [CrossRef] [Green Version]
- Ericson, S.; Kurol, J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur. J. Orthod. 1988, 10, 283–295. [Google Scholar] [CrossRef]
- Hou, R.; Kong, L.; Ao, J.; Liu, G.; Zhou, H.; Qin, R.; Hu, K. Investigation of Impacted Permanent Teeth Except the Third Molar in Chinese Patients Through an X-Ray Study. J. Oral Maxillofac. Surg. 2010, 68, 762–767. [Google Scholar] [CrossRef]
- Becker, A.; Smith, P.; Behar, R. The incidence of anomalous maxillary lateral incisors in relation to palatally-displaced cuspids. Angle Orthod. 1981, 51, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.; Peck, S.; Peck, L.; Kataja, M. Palatal canine displacement: Guidance theory or an anomaly of genetic origin? Angle Orthod. 1995, 65, 95–102. [Google Scholar] [PubMed]
- Peck, S.; Peck, L.; Kataja, M. The palatally displaced canine as a dental anomaly of genetic origin The Angle Orthodontist. Angle Orthod. 1994, 64, 249–256. [Google Scholar] [PubMed]
- Brin, I.; Becker, A.; Shalhav, M. Position of the maxillary permanent canine in relation to anomalous or missing lateral incisors: A population study. Eur. J. Orthod. 1986, 8, 12–16. [Google Scholar] [CrossRef]
- Bishara, S. Impacted maxillary canines: A review. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 159–171. [Google Scholar] [CrossRef]
- McConnell, T.L.; Hoffman, D.L.; Forbes, D.P.; Janzen, E.K.; Weintraub, N.H. Maxillary canine impaction in patients with transverse maxillary deficiency. ASDC J. Dent. Child. 1996, 63, 190–195. [Google Scholar]
- Schindel, R.H.; Duffy, S.L. Maxillary Transverse Discrepancies and Potentially Impacted Maxillary Canines in Mixed-dentition Patients. Angle Orthod. 2007, 77, 430–435. [Google Scholar] [CrossRef]
- Langberg, B.J.; Peck, S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 220–223. [Google Scholar] [CrossRef]
- Al-Nimri, K.; Gharaibeh, T. Space conditions and dental and occlusal features in patients with palatally impacted maxillary canines: An aetiological study. Eur. J. Orthod. 2005, 27, 461–465. [Google Scholar] [CrossRef]
- Jain, S.; Debbarma, S. Patterns and prevalence of canine anomalies in orthodontic patients. Med. Pharm. Rep. 2019, 92, 72–78. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Epidemiology 2007, 18, 800–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Hyun, H.K.; Jang, K.T. Interrelationship between the position of impacted maxillary canines and the morphology of the maxilla. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Sun, Z.; Fields, H.; Wang, L.; Luo, L. Etiologic factors for buccal and palatal maxillary canine impaction: A perspective based on cone-beam computed tomography analyses. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Hong, W.-H.; Radfar, R.; Chung, C.-H. Relationship between the maxillary transverse dimension and palatally displaced canines: A cone-beam computed tomographic study. Angle Orthod. 2015, 85, 440–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anic-Milosevic, S.; Varga, S.; Mestrovic, S.; Lapter-Varga, M.; Slaj, M. Dental and occlusal features in patients with palatally displaced maxillary canines. Eur. J. Orthod. 2009, 31, 367–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fattahi, H.; Ghaeed, F.; Alipour, A. Association between maxillary canine impaction and arch dimensions. Aust. Orthod. J. 2012, 28, 56–62. [Google Scholar]
- Leonardi, R.; Barbato, E.; Vichi, M.; Caltabiano, M. A sella turcica bridge in subjects with dental anomalies. Eur. J. Orthod. 2006, 28, 580–585. [Google Scholar] [CrossRef]
- Tepedino, M.; Laurenziello, M.; Guida, L.; Montaruli, G.; Grassia, V.; Chimenti, C.; Campanelli, M.; Ciavarella, D. Sella turcica and craniofacial morphology in patients with palatally displaced canines: A retrospective study. Folia Morphol. 2020, 79, 51–57. [Google Scholar] [CrossRef]
- Kjaer, I.; Fischer-Hansen, B. The adenohypophysis and the cranial base in early human development. J. Craniofacial Genet. Dev. Biol. 1995, 15, 157–161. [Google Scholar]
- Kjaer, I.; Bagheri, A. Prenatal development of the alveolar bone of human deciduous incisors and canines. J. Dent. Res. 1999, 78, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Stellzig, A.; Basdra, E.; Komposch, G. The etiology of canine tooth impaction--a space analysis. Fortschr. Der Kieferorthopadie 1994, 55, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, E.; Cassetta, M.; Cavallini, C.; Vicari, D.; Leonardi, R.; Barbato, E. Dental anomalies and clinical features in patients with maxillary canine impaction: A retrospective study. Angle Orthod. 2013, 83, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Mehrotra, P.; Bhagchandani, J.; Singh, A.; Garg, A.; Kumar, S.; Sharma, A.; Yadav, H. Localization of impacted canines. J. Clin. Diagn. Res. JCDR 2015, 9, ZE11–ZE14. [Google Scholar] [CrossRef] [PubMed]
- Litsas, G. A Review of Early Displaced Maxillary Canines: Etiology, Diagnosis and Interceptive Treatment. Open Dent. J. 2011, 5, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Dental Association Council on Scientific Affairs. The use of cone-beam computed tomography in dentistry: An advisory statement from the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2012, 143, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Abdelkarim, A. Cone-Beam Computed Tomography in Orthodontics. Dent. J. 2019, 7, 89. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Details of Maxillary Impacted Canine Characteristics, Landmarks and Measurements Employed in This Study | |
| Type | Unilateral or Bilateral |
| Side | Right or left |
| Location | Buccal or Palatal |
| Landmarks and Measurements Employed | |
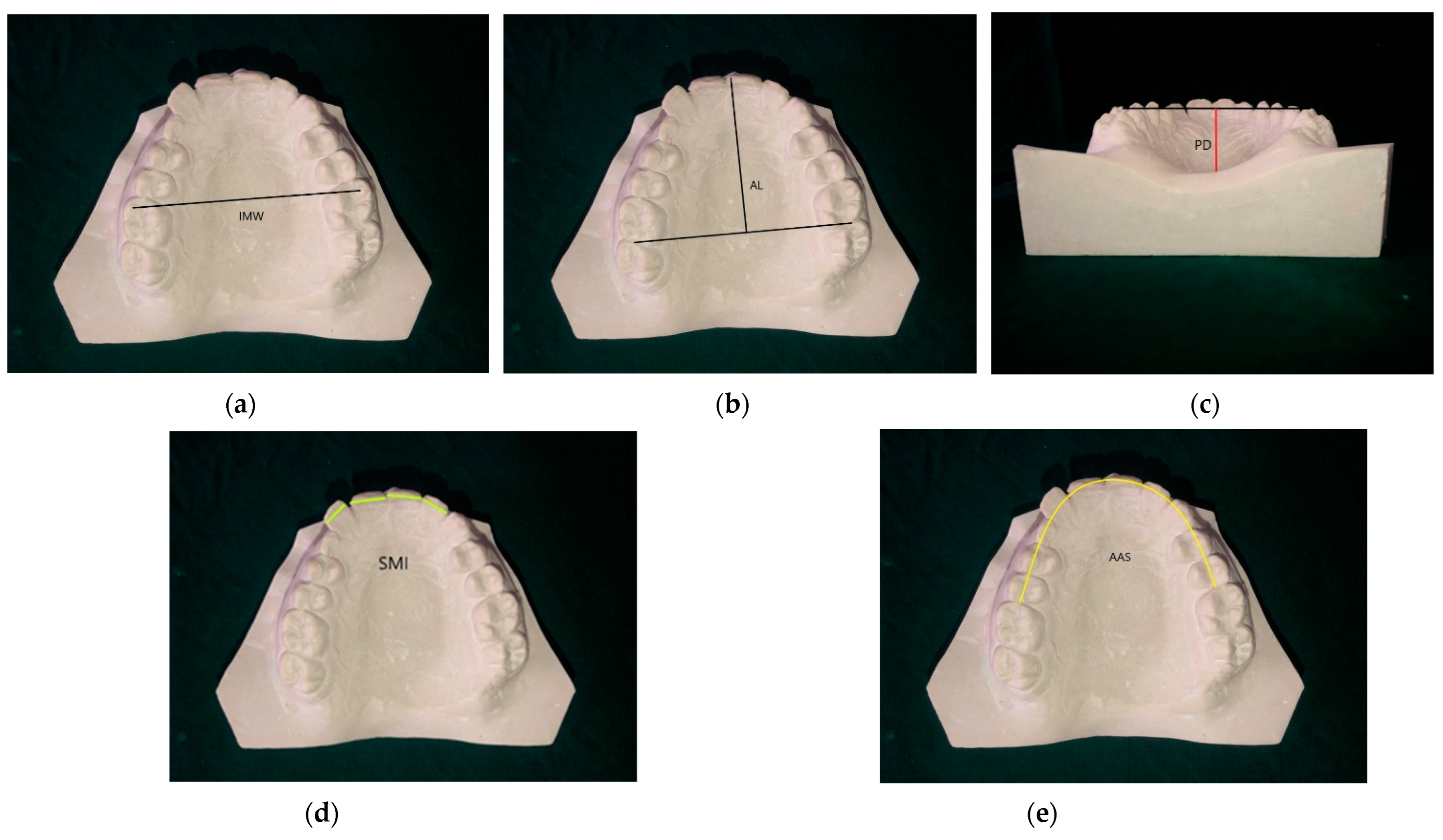
| Inter-molar width; IMW (mm) | The transverse distance between the mesiobuccal cusp tips of both first molars. |
| Palatal depth; PD (mm) | The perpendicular height measured from the line joining the mesiopalatal cusp tips of both first molars to the palatal surface in vertical direction along the midline. |
| Arch Length; AL (mm) | The perpendicular distance, measured from the line joining the distal surface of both first molars to mesial surface incisal edge of either central incisor in saggital direction. |
| Sum of Maxillary incisors; (mm) | The sum of the mesiodistal widths of all four maxillary incisors. |
| Available arch space; AAS (mm) | The space measured through adjoining teeth from the mesial surfaces of the right to the left first molars with the help of brass wire. |
| Ratio 1 AL × 100/IMW | This value signifies Maxillary arch shape. |
| Ratio 2 PD × 100/IMW | This value signifies palatal vault shape. |
| Ratio 3 SMI × 100/AAS | This value indicates whether or not the maxillary permanent dentition had adequate space to erupt. |
| Variables | Maxillary Impacted Canine (MIC) * | Controls (30) | |||
|---|---|---|---|---|---|
| Buccal (12) | Palatal (18) | Total (30) | |||
| Age (Mean ± SD) (Years) | 15.6 ± 1.8 | 15.8 ± 1.6 | 15.7 ± 1.9 | 15.7 ± 2.2 | |
| Sex n (%) | Females Male | 8 (26.66%) 4 (13.33%) | 12 (40%) 6 (20%) | 20 10 | 16 (53.33%) 14 (46.60%) |
| Origin | Gujarati | 12 | 18 | 30 | 30 |
| Bilateral: Unilateral | 4:8 (33.3%:66.6%) | 5:13 (27.7%:72.2%) | 9:21 | ||
| Left: Right | 7:5 (50.8%:41.6%) | 11:7 (61.1%:38.8%) | 18:12 | ||
| Parameters | Group | Mean | SD | Std. Error | Minimum | Maximum | Anova p-Value | Post Hoc |
| IMW | Buccal side | 51.04 | 2.93 | 0.535 | 45.52 | 57.08 | <0.0001 * | 1.3 > 2 |
| Palatal side | 48.22 | 2.65 | 0.484 | 43.75 | 59.07 | |||
| Controls | 50.42 | 2.61 | 0.477 | 46.25 | 57.47 | |||
| PD | Buccal side | 19.32 | 1.86 | 0.340 | 16.12 | 25.03 | <0.0001 * | 1.3 > 2 |
| Palatal side | 21.33 | 2.08 | 0.380 | 15.62 | 25.93 | |||
| Controls | 19.28 | 1.96 | 0.358 | 15.01 | 24.02 | |||
| AL | Buccal side | 35.93 | 1.71 | 0.313 | 30.76 | 39.73 | <0.0001 * | 2.3 > 1 |
| Palatal side | 39.70 | 2.18 | 0.398 | 35.08 | 43.82 | |||
| Controls | 39.62 | 1.98 | 0.361 | 34.53 | 43.37 | |||
| SMI | Buccal side | 30.94 | 2.47 | 0.452 | 26.01 | 36.77 | 0.014 | 1.3 > 2 |
| Palatal side | 29.62 | 2.14 | 0.391 | 26.10 | 33.57 | |||
| Controls | 31.26 | 2.13 | 0.389 | 26.93 | 36.73 | |||
| AAS | Buccal side | 71.73 | 4.11 | 0.750 | 63.94 | 79.55 | <0.0001 * | 3 > 2 > 1 |
| Palatal side | 75.57 | 4.63 | 0.845 | 67.67 | 86.06 | |||
| Controls | 78.36 | 4.15 | 0.758 | 71.67 | 89.69 | |||
| RATIO 1 AL × 100/IMW | Buccal side | 70.85 | 4.41 | 0.804 | 60.98 | 80.92 | <0.0001 * | 2 > 3 > 1 |
| Palatal side | 82.47 | 5.42 | 0.989 | 69.54 | 91.24 | |||
| Controls | 78.71 | 4.88 | 0.892 | 68.71 | 91.84 | |||
| RATIO 2 PD × 100/IMW | Buccal side | 37.90 | 3.11 | 0.568 | 33.34 | 47.25 | <0.0001 * | 2 > 1.3 |
| Palatal side | 44.28 | 4.18 | 0.763 | 33.90 | 53.89 | |||
| Controls | 38.35 | 4.46 | 0.813 | 28.05 | 49.43 | |||
| RATIO 3 SMI ×100/AAS | Buccal side | 43.86 | 3.74 | 0.682 | 38.11 | 51.68 | <0.0001 * | 1 > 2.3 |
| Palatal side | 39.33 | 3.73 | 0.681 | 32.70 | 47.92 | |||
| Controls | 39.89 | 1.87 | 0.341 | 36.01 | 43.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehta, F.; Jain, M.; Verma, S.; Basha, S.; Patel, R.A.; Trivedi, R.; Parekh, H.A.; Ahmed, V.K.S.; Alam, M.K.; Nagarajappa, A.K.; et al. Morphological Comparison of the Maxillary Arch in Buccal and Palatal Canine Impaction among Asian Population of Gujarati Origin: A Hospital-Based Study. Healthcare 2022, 10, 939. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050939
Mehta F, Jain M, Verma S, Basha S, Patel RA, Trivedi R, Parekh HA, Ahmed VKS, Alam MK, Nagarajappa AK, et al. Morphological Comparison of the Maxillary Arch in Buccal and Palatal Canine Impaction among Asian Population of Gujarati Origin: A Hospital-Based Study. Healthcare. 2022; 10(5):939. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050939
Chicago/Turabian StyleMehta, Falguni, Mayank Jain, Swati Verma, Sakeenabi Basha, Renuka A. Patel, Rahul Trivedi, Harshik A. Parekh, Valai Kasim Shakeel Ahmed, Mohammad Khursheed Alam, Anil Kumar Nagarajappa, and et al. 2022. "Morphological Comparison of the Maxillary Arch in Buccal and Palatal Canine Impaction among Asian Population of Gujarati Origin: A Hospital-Based Study" Healthcare 10, no. 5: 939. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050939