Impact of Body Mass Index on the Development of Inflammatory Bowel Disease: A Systematic Review and Dose-Response Analysis of 15.6 Million Participants





Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
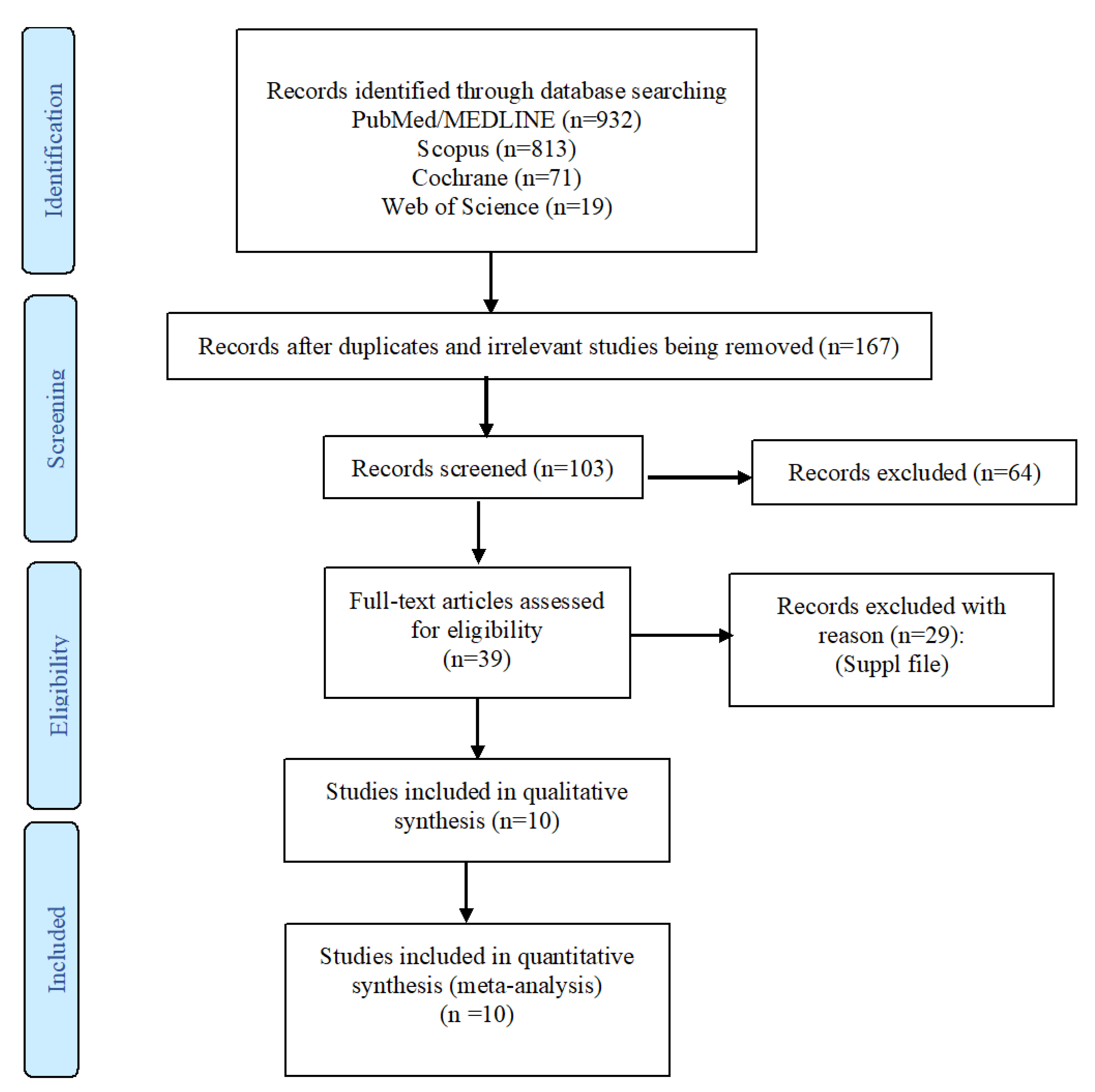
3.1. Study Selection and Characteristics
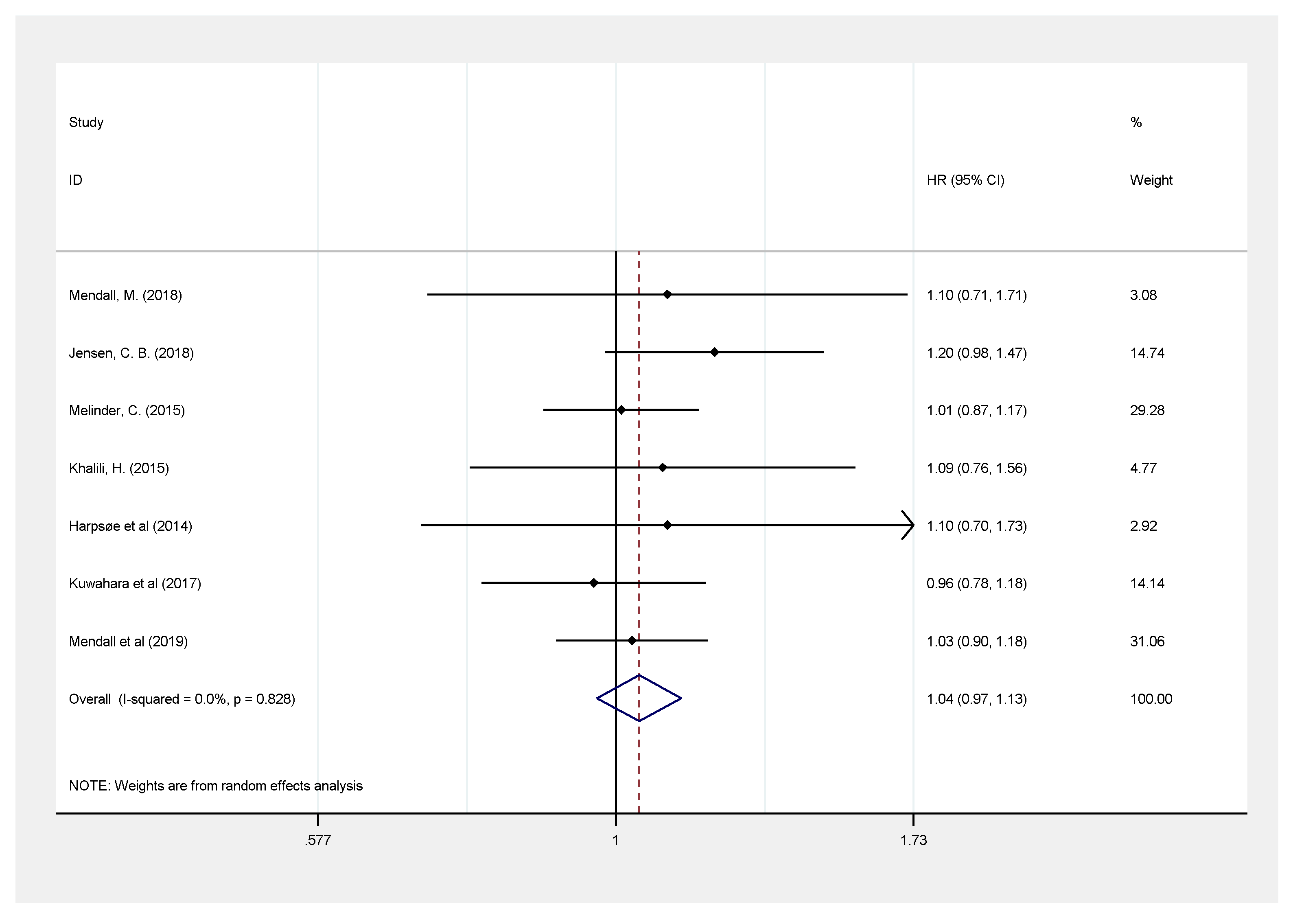
3.2. Primary Meta-Analysis
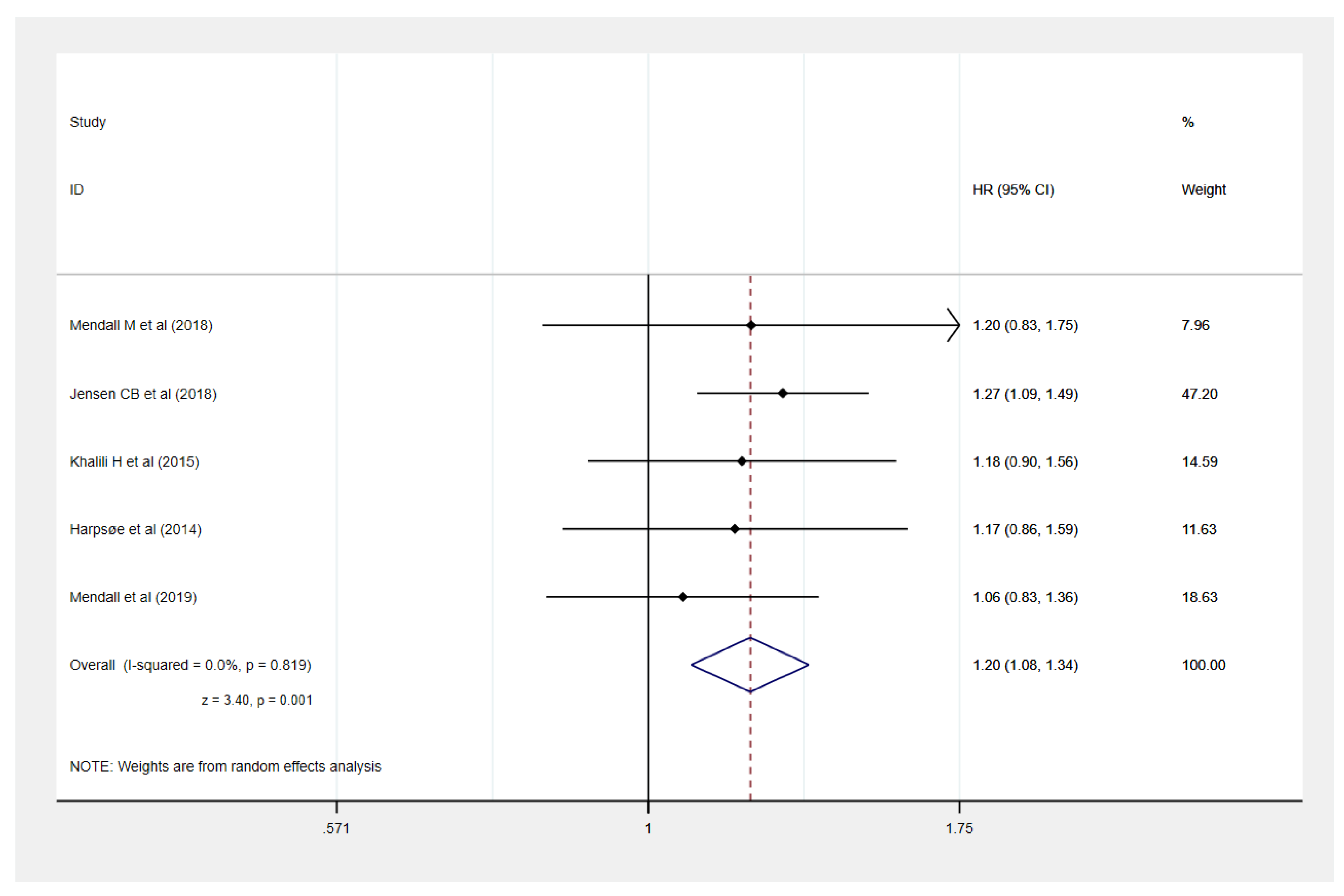
3.2.1. Association Between BMI and Development of IBD
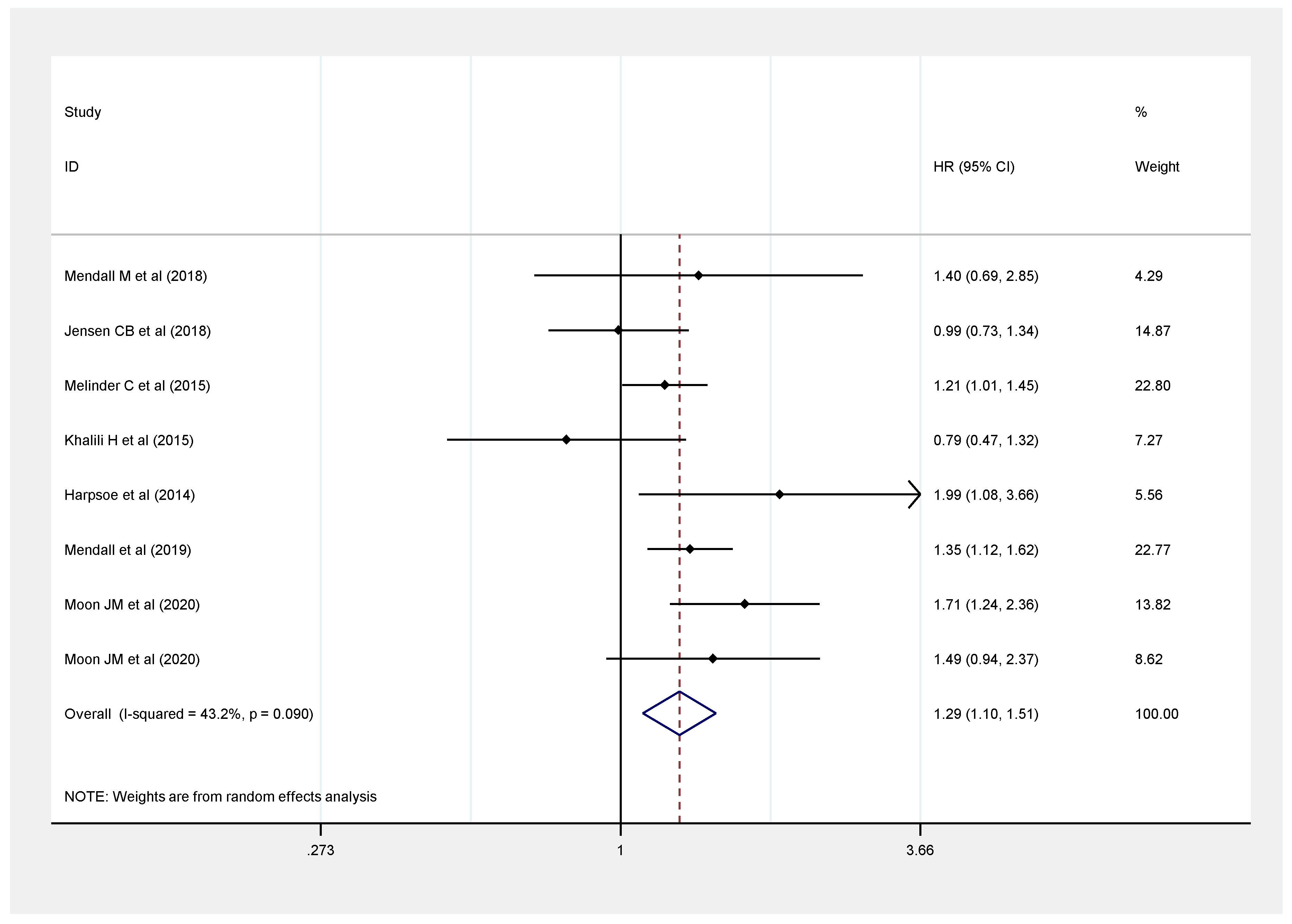
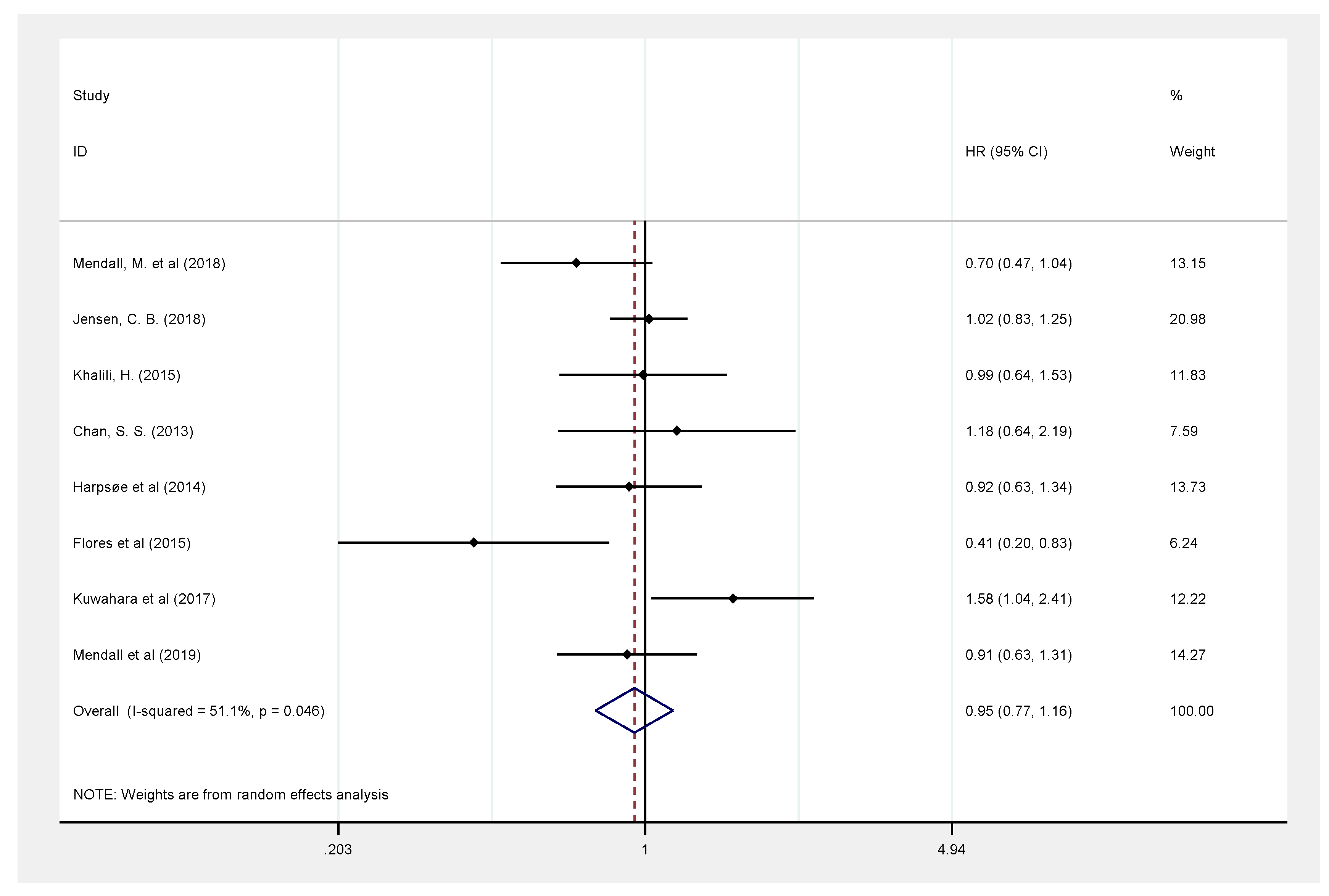
3.2.2. Association Between BMI and Crohn’s Disease
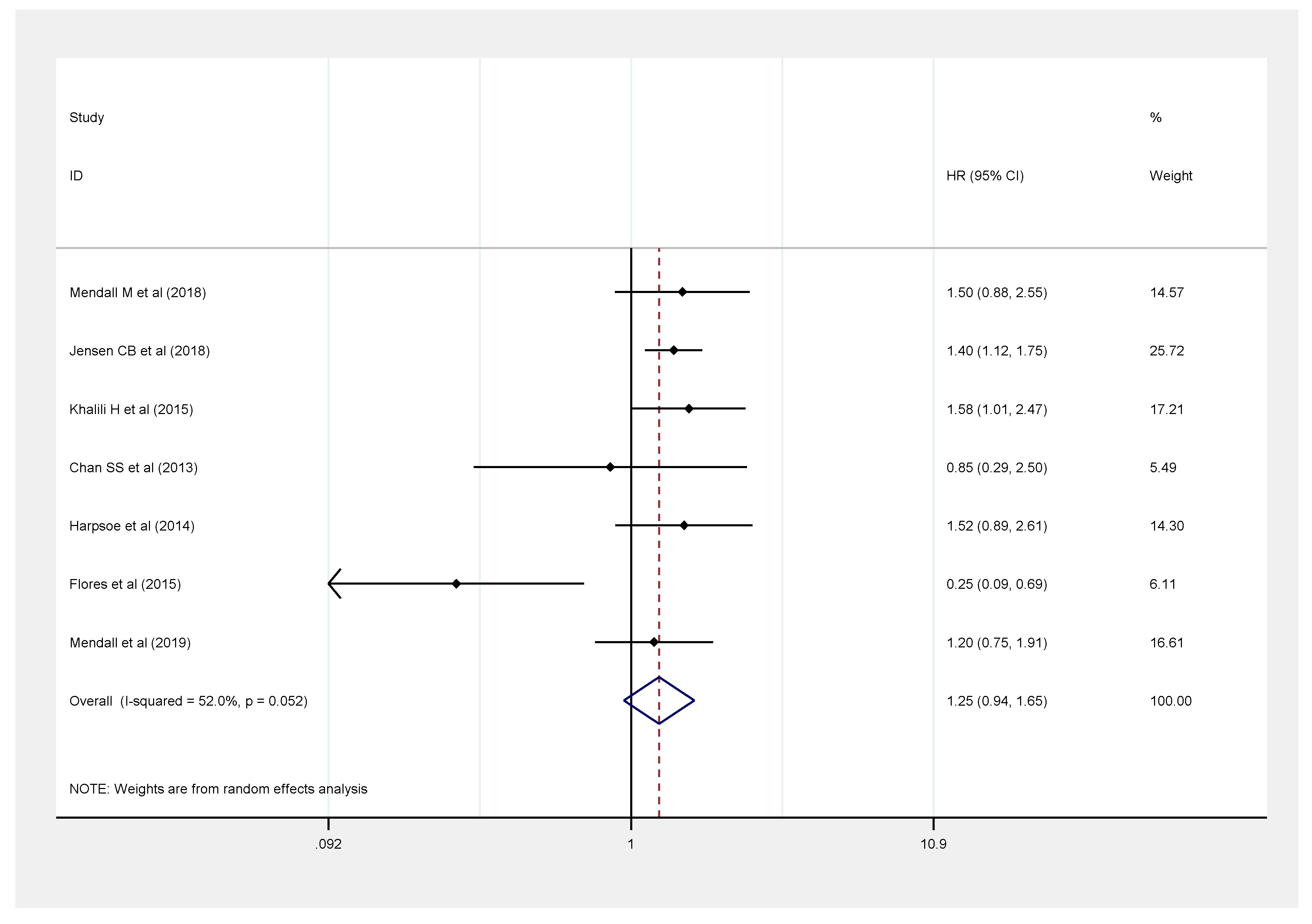
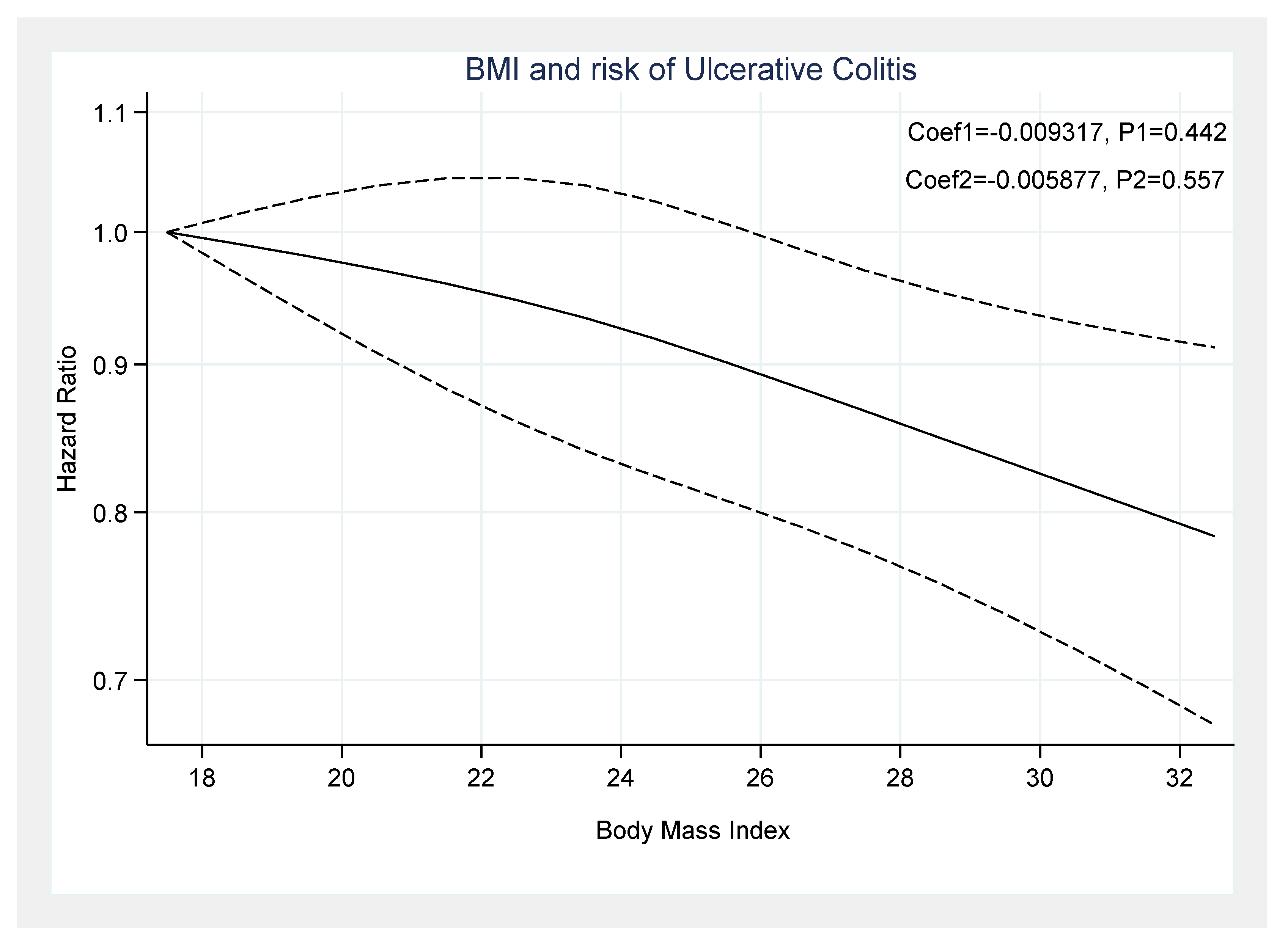
3.2.3. Association Between BMI and Ulcerative Colitis
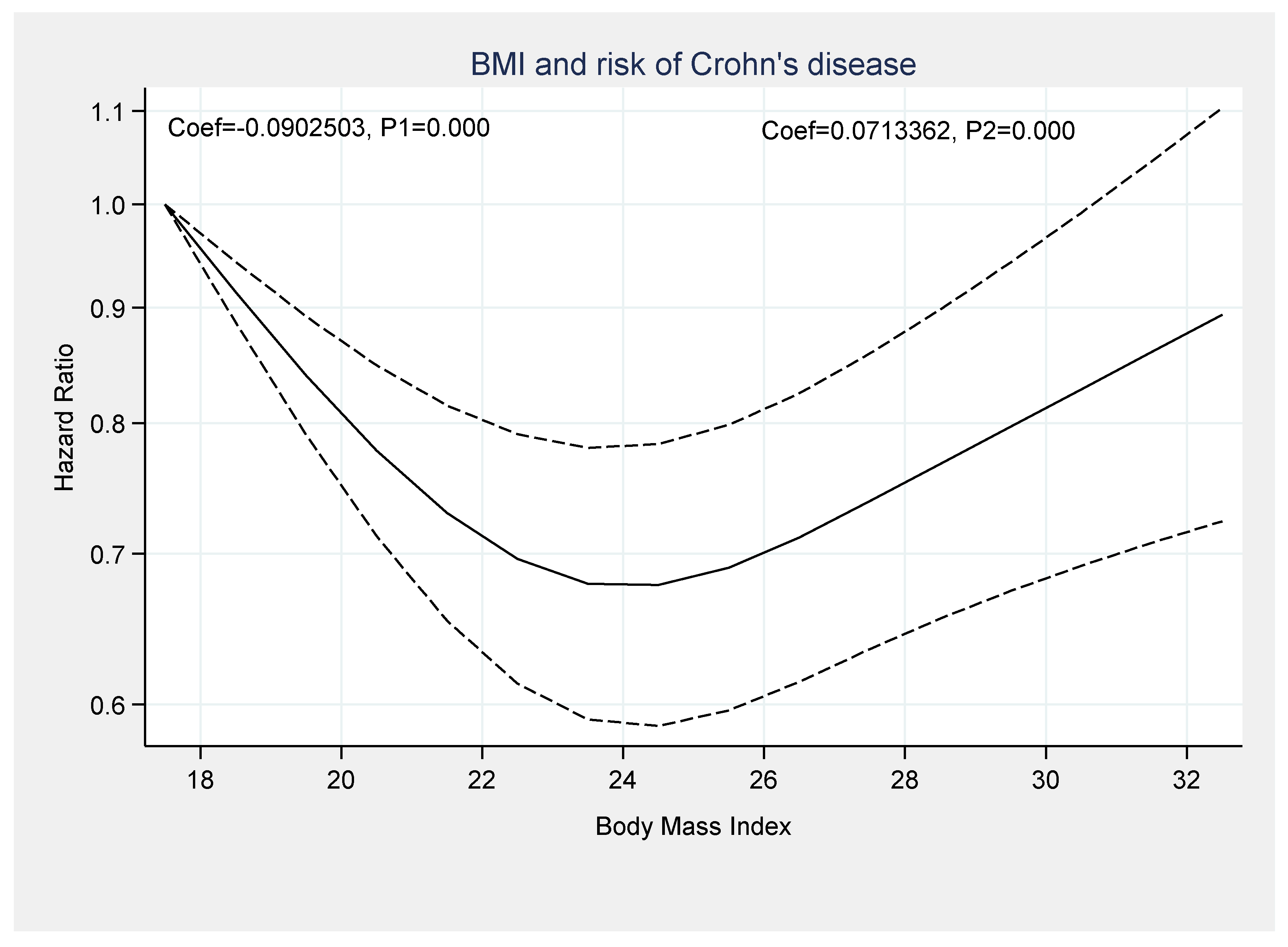
3.3. Dose-Response Analysis
3.4. Quality of Studies
3.5. Publication Bias
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abolhassani, H.; Alipour, V. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar]
- Weimers, P.; Munkholm, P. The natural history of IBD: Lessons learned. Curr. Teat. Options Gastroenterol. 2018, 16, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Pulley, J.; Todd, A.; Flatley, C.; Begun, J. Malnutrition and quality of life among adult inflammatory bowel disease patients. JGH Open 2020, 4, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Scaldaferri, F.; Pizzoferrato, M.; Lopetuso, L.R.; Musca, T.; Ingravalle, F.; Sicignano, L.L.; Mentella, M.; Miggiano, G.; Mele, M.C.; Gaetani, E.; et al. Nutrition and IBD: Malnutrition and/or sarcopenia? A practical guide. Gastroenterol. Res. Pract. 2017, 2017, 8646495. [Google Scholar] [CrossRef]
- Seminerio, J.L.; Koutroubakis, I.E.; Ramos-Rivers, C.; Hashash, J.G.; Dudekula, A.; Regueiro, M.; Baidoo, L.; Barrie, A.; Swoger, J.; Schwartz, M.; et al. Impact of obesity on the management and clinical course of patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2015, 21, 2857–2863. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.V.; Trott, M.J.; Bartholomeusz, F.D.; Andrews, J.M. Systematic review: Body composition in adults with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 38, 213–225. [Google Scholar] [CrossRef]
- Steed, H.; Walsh, S.; Reynolds, N. A brief report of the epidemiology of obesity in the inflammatory bowel disease population of Tayside, Scotland. Obes. Facts 2009, 2, 370–372. [Google Scholar] [CrossRef]
- Singh, S.; Khera, R.; Sandborn, W.J. Obesity Is Associated with Worse Outcomes in Hospitalized Patients with Inflammatory Bowel Diseases: A Nationwide Analysis: 591. Am. J. Gastroenterol. 2016, 111, S271. [Google Scholar] [CrossRef]
- Mendall, M.A.; Jensen, C.B.; Sørensen, T.I.; Ängquist, L.H.; Jess, T. Body mass index in young men and risk of inflammatory bowel disease through adult life: A population-based Danish cohort study. Sci. Rep. 2019, 9, 6360. [Google Scholar] [CrossRef]
- Jensen, C.B.; Ängquist, L.H.; Mendall, M.A.; Sørensen, T.I.; Baker, J.L.; Jess, T. Childhood body mass index and risk of inflammatory bowel disease in adulthood: A population-based cohort study. Am. J. Gastroenterol. 2018, 113, 694–701. [Google Scholar] [CrossRef]
- Mendall, M.; Harpsøe, M.C.; Kumar, D.; Andersson, M.; Jess, T. Relation of body mass index to risk of developing inflammatory bowel disease amongst women in the Danish National Birth Cohort. PLoS ONE 2018, 13, e0190600. [Google Scholar] [CrossRef] [Green Version]
- Khalili, H.; Ananthakrishnan, A.N.; Konijeti, G.G.; Higuchi, L.M.; Fuchs, C.S.; Richter, J.M.; Chan, A.T. Measures of obesity and risk of Crohn’s disease and ulcerative colitis. Inflamm. Bowel Dis. 2015, 21, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harpsøe, M.C.; Basit, S.; Andersson, M.; Nielsen, N.M.; Frisch, M.; Wohlfahrt, J.; Nohr, E.A.; Linneberg, A.; Jess, T. Body mass index and risk of autoimmune diseases: A study within the Danish National Birth Cohort. Int. J. Epidemiol. 2014, 43, 843–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuwahara, E.; Murakami, Y.; Nakamura, T.; Inoue, N.; Nagahori, M.; Matsui, T.; Watanabe, M.; Suzuki, Y.; Nishiwaki, Y. Factors associated with exacerbation of newly diagnosed mild ulcerative colitis based on a nationwide registry in Japan. J. Gastroenterol. 2017, 52, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.; Luben, R.; Olsen, A.; Tjonneland, A.; Kaaks, R.; Teucher, B.; Lindgren, S.; Grip, O.; Key, T.; Crowe, F.L.; et al. Body Mass Index and the Risk for Crohn’s Disease and Ulcerative Colitis: Data from a European Prospective Cohort Study (The IBD in EPIC Study). Am. J. Gastroenterol. 2013, 108, 575–582. [Google Scholar] [CrossRef]
- Flores, A.; Burstein, E.; Cipher, D.J.; Feagins, L.A. Obesity in inflammatory bowel disease: A marker of less severe disease. Dig. Dis. Sci. 2015, 60, 2436–2445. [Google Scholar] [CrossRef] [PubMed]
- Melinder, C.; Hiyoshi, A.; Hussein, O.; Halfvarson, J.; Ekbom, A.; Montgomery, S. Physical fitness in adolescence and subsequent inflammatory bowel disease risk. Clin. Transl. Gastroenterol. 2015, 6, e121. [Google Scholar] [CrossRef]
- Dong, J.; Chen, Y.; Tang, Y.; Xu, F.; Yu, C.; Li, Y.; Pankaj, P.; Dai, N. Body mass index is associated with inflammatory bowel disease: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0144872. [Google Scholar] [CrossRef] [Green Version]
- Rahmani, J.; Kord-Varkaneh, H.; Hekmatdoost, A.; Thompson, J.; Clark, C.; Salehisahlabadi, A.; Day, A.S.; Jacobson, K. Body mass index and risk of inflammatory bowel disease: A systematic review and dose-response meta-analysis of cohort studies of over a million participants. Obes. Rev. 2019, 20, 1312–1320. [Google Scholar] [CrossRef]
- Moon, J.M.; Kang, E.A.; Han, K.; Hong, S.W.; Soh, H.; Park, S.; Lee, J.; Lee, H.J.; Im, J.P.; Kim, J.S. Trends and risk factors of elderly-onset Crohn’s disease: A nationwide cohort study. World J. Gastroenterol. 2020, 26, 404–415. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Br. Med. J. 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, D.; White, I.R.; Thompson, S.G. Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat. Med. 2010, 29, 1282–1297. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-Analysis for linear and non-linear dose-response relations: Examples, an evaluation of approximations, and software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Dulai, P.S.; Zarrinpar, A.; Ramamoorthy, S.; Sandborn, W.J. Obesity in IBD: Epidemiology, pathogenesis, disease course and treatment outcomes. Nat. Rev. Gastroenterol. Hepatol. 2016, 30, 30. [Google Scholar] [CrossRef] [Green Version]
- Karmiris, K.; Koutroubakis, I.; Xidakis, C.; Polychronaki, M.; Voudouri, T.; Kouroumalis, E.A. Circulating levels of leptin, adiponectin, resistin, and ghrelin in inflammatory bowel disease. Inflamm. Bowel Dis. 2006, 12, 100–105. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Gonzales, F.; Dubuquoy, L.; Rousseaux, C.; Dubuquoy, C.; Decourcelle, C.; Saudemont, A.; Tachon, M.; Beclin, E.; Odou, M.-F.; et al. Mesenteric fat as a source of C reactive protein and as a target for bacterial translocation in Crohn’s disease. Gut 2012, 61, 78–85. [Google Scholar] [CrossRef]
- Konrad, A.; Lehrke, M.; Schachinger, V.; Seibold, F.; Stark, R.; Ochsenkuhn, T.; Parhofer, K.G.; Goke, B.; Broedl, U.C. Resistin is an inflammatory marker of inflammatory bowel disease in humans. Eur. J. Gastroenterol. Hepatol. 2007, 19, 1070–1074. [Google Scholar] [CrossRef]
- Bilski, J.; Mazur-Bialy, A.; Wojcik, D.; Surmiak, M.; Magierowski, M.; Sliwowski, Z.; Pajdo, R.; Kwiecien, S.; Danielak, A.; Ptak-Belowska, A.; et al. Role of obesity, mesenteric adipose tissue, and adipokines in inflammatory bowel diseases. Biomolecules 2019, 9, 780. [Google Scholar] [CrossRef] [Green Version]
- Kim, A. Dysbiosis: A review highlighting obesity and inflammatory bowel disease. J. Clin. Gastroenterol. 2015, 49, S20–S24. [Google Scholar] [CrossRef]
- Szilagyi, A. Relationship(s) between obesity and inflammatory bowel diseases: Possible intertwined pathogenic mechanisms. Clin. J. Gastroenterol. 2020, 13, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spooren, C.E.; Wintjens, D.S.; de Jong, M.J.; van der Meulen-de, A.E.; Romberg-Camps, M.J.; Becx, M.C.; Maljaars, J.P.; van Bodegraven, A.A.; Mahmmod, N.; Markus, T.; et al. Risk of impaired nutritional status and flare occurrence in IBD outpatients. Dig. Liver Dis. 2019, 51, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Ciocîrlan, M.; Ciocîrlan, M.; Iacob, R.; Tanțău, A.; Gheorghe, L.; Gheorghe, C.; Dobru, D.; Constantinescu, G.; Cijevschi, C.; Trifan, A.; et al. Malnutrition Prevalence in Newly Diagnosed Patients with Inflammatory Bowel Disease-Data from the National Romanian Database. J. Gastrointestin. Liver Dis. 2019, 28, 163–168. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Year | Country | Baseline | Study Characteristics | IBD Development (Outcomes) | Literature Quality † | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age | Gender | Cohort Design | Follow-Up (Year) | Sample Size | CD | UC | ||||
| Moon, J. M. et al. [20] | 2020 | Korea | 50 | Both | Retrospective | 7.3 | 14,060,821 | 977 | - | 8 |
| Mendall, M. A. et al. [9] | 2019 | Denmark | 19 | Male | Prospective | 38 | 377,957 | 1523 | 3323 | 9 |
| Jensen, C. B. et al. [10] | 2018 | Denmark | 46 | Both | Prospective | 38 | 316,799 | 1500 | 2732 | 7 |
| Mendall, M. et al. [11] | 2018 | Denmark | 30 | Female | Prospective | 6 | 74,512 | 137 | 448 | 8 |
| Kuwahara, E. et al. [14] | 2017 | Japan | 42 | Both | Retrospective | 2 | 39,554 | - | 8120 | 9 |
| Flores, A. et al. [16] | 2015 | U.S.A. | 40 | Both | Retrospective | 5 | 581 | 297 | 284 | 8 |
| Melinder, C. et al. [17] | 2015 | Sweden | 18 | Male | Prospective | 4 | 240,984 | 986 | 1878 | 9 |
| Khalili, H. et al. [12] | 2015 | U.S.A. | 34 | Female | Prospective | 18 | 111,498 | 153 | 229 | 8 |
| Harpsøe, M. C. et al. [13] | 2014 | Denmark | 30 | Female | Retrospective | 11 | 75,008 | 138 | 394 | 8 |
| Chan, S. S. et al. [15] | 2013 | 10 European countries | 52 | Both | Prospective | 5.1 | 300,724 | 75 | 177 | 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhagavathula, A.S.; Clark, C.C.T.; Rahmani, J.; Chattu, V.K. Impact of Body Mass Index on the Development of Inflammatory Bowel Disease: A Systematic Review and Dose-Response Analysis of 15.6 Million Participants. Healthcare 2021, 9, 35. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010035
Bhagavathula AS, Clark CCT, Rahmani J, Chattu VK. Impact of Body Mass Index on the Development of Inflammatory Bowel Disease: A Systematic Review and Dose-Response Analysis of 15.6 Million Participants. Healthcare. 2021; 9(1):35. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010035
Chicago/Turabian StyleBhagavathula, Akshaya Srikanth, Cain C.T. Clark, Jamal Rahmani, and Vijay Kumar Chattu. 2021. "Impact of Body Mass Index on the Development of Inflammatory Bowel Disease: A Systematic Review and Dose-Response Analysis of 15.6 Million Participants" Healthcare 9, no. 1: 35. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010035