
Cost-Effectiveness Analysis of Type 2 Diabetes Mellitus (T2DM) Treatment in Patients with Complications of Kidney and Peripheral Vascular Diseases in Indonesia


Abstract
:1. Introduction
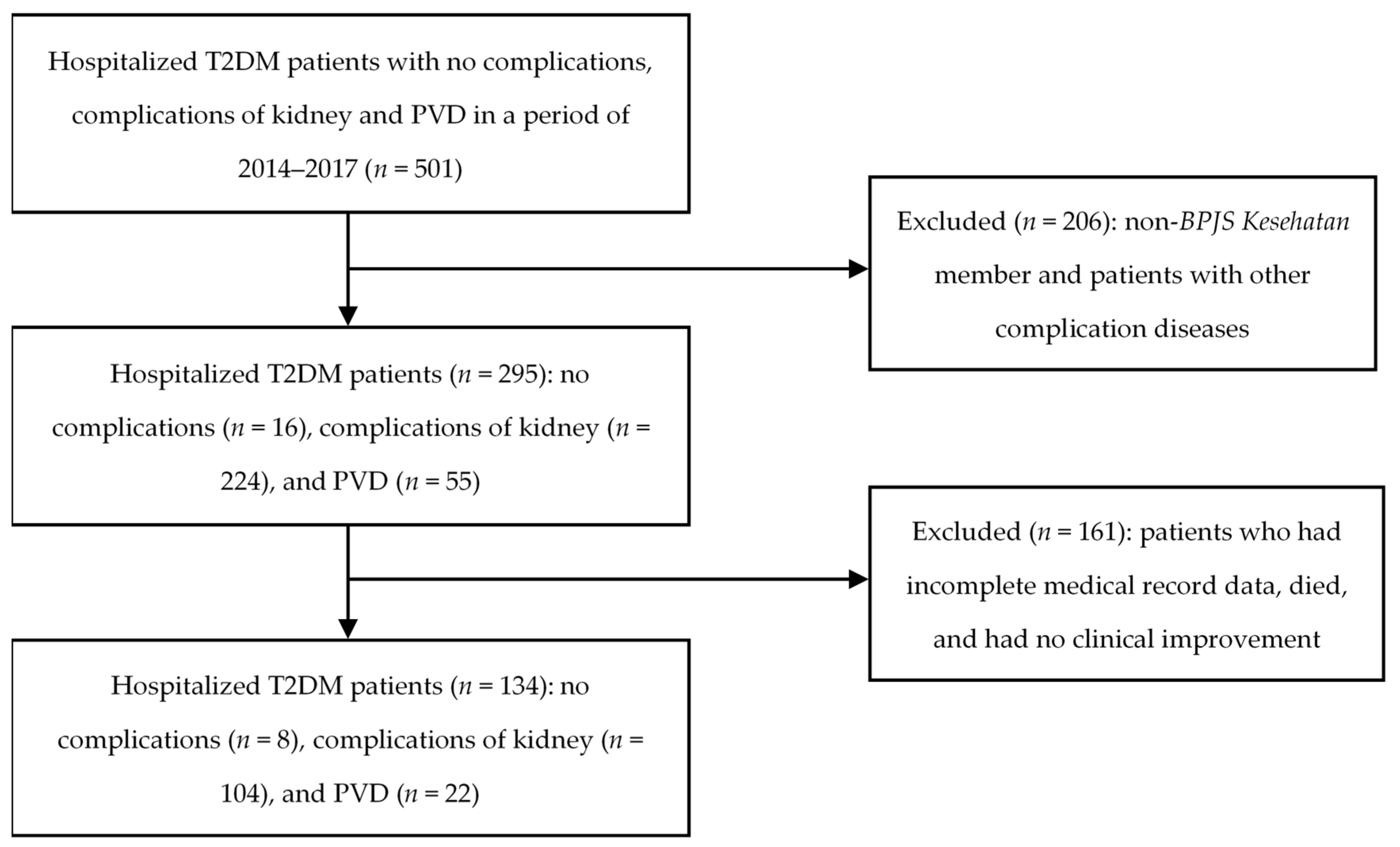
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Soelistijo, S.A.; Novida, H.; Rudijanto, A.; Soewondo, P.; Suastika, K.; Manaf, A. Management and Prevention of Type 2 Diabetes Mellitus in Indonesia 2015; PB Perkeni: Jakarta, Indonesia, 2015. [Google Scholar]
- Sinuraya, R.K.; Oktrina, A.; Handayani, N.K.; Destiani, D.P.; Puspitasari, I.M. Clinical Pharmacy Services Improve Blood Sugar Control of Diabetes Mellitus Patients. Indones. J. Clin. Pharm. 2019, 8, 271–280. [Google Scholar] [CrossRef]
- IDF. IDF Diabetes Atlas Ninth Edition (9th) 2019. Available online: https://www.diabetesatlas.org/upload/resources/2019/IDF_Atlas_9th_Edition_2019.pdf (accessed on 5 September 2020).
- Basic Health Research. Badan Penelitian dan Pengembangan Kesehatan, Kementerian Kesehatan Republik Indonesia; Basic Health Research: Jakarta, Indonesia, 2018. [Google Scholar]
- ADA. Standards of medical care in diabetes-2015 abridged for primary care providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar] [CrossRef] [Green Version]
- ADA. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010, 33 (Suppl. 1), S62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ADA. Diagnosis and classification of diabetes mellitus. Diabetes Care 2013, 36 (Suppl. 1), S67–S74. [Google Scholar] [CrossRef] [Green Version]
- ADA. Diagnosis and classification of diabetes mellitus. Diabetes Care 2013, 36 (Suppl. 1), S8. [Google Scholar]
- Flint, A.; Arslanian, S. Treatment of Type 2 Diabetes in Youth. Diabetes Care 2011, 34, S177–S183. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach: Position Statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [Green Version]
- Roden, M.; Shulman, G.I. The integrative biology of type 2 diabetes. Nat. Cell Biol. 2019, 576, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casqueiro, J.; Casqueiro, J.; Alves, C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J. Endocrinol. Metab. 2012, 16 (Suppl. 1), S27–S36. [Google Scholar]
- Pecoits-Filho, R.; Abensur, H.; Betônico, C.C.R.; Machado, A.D.; Parente, E.B.; Queiroz, M.; Salles, J.E.N.; Titan, S.; Vencio, S. Interactions between kidney disease and diabetes: Dangerous liaisons. Diabetol. Metab. Syndr. 2016, 8, 1–21. [Google Scholar] [CrossRef]
- Vallon, V.; Komers, R. Pathophysiology of the Diabetic Kidney. Compr. Physiol. 2011, 1, 1175–1232. [Google Scholar] [CrossRef] [PubMed]
- Pourghasem, M.; Shafi, H.; Babazadeh, Z. Histological changes of kidney in diabetic nephropathy. Casp. J. Intern. Med. 2015, 6, 120–127. [Google Scholar]
- Hidayati, T.; Adiningrat, A.; Akrom, A. Clinical conditions and history of illness among terminal chronic kidney disease patients. Int. J. Public Health Sci. 2019, 8, 385–390. [Google Scholar] [CrossRef]
- Yazdanpanah, L.; Shahbazian, H.; Nazari, I.; Arti, H.R.; Ahmadi, F.; Mohammadianinejad, S.E.; Cheraghian, B.; Hesam, S. Incidence and Risk Factors of Diabetic Foot Ulcer: A Population-Based Diabetic Foot Cohort (ADFC Study)—Two-Year Follow-Up Study. Int. J. Endocrinol. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Boulton, A.J.M.; Kirsner, R.S.; Vileikyte, L. Neuropathic Diabetic Foot Ulcers. N. Engl. J. Med. 2004, 351, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Pemayun, T.G.D.; Naibaho, R.M. Clinical profile and outcome of diabetic foot ulcer, a view from tertiary care hospital in Semarang, Indonesia. Diabet. Foot Ankle 2017, 8, 1312974. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, E.A.; Chay, J.; Bajpai, S. The Economic Burden of Self-Reported and Undiagnosed Cardiovascular Diseases and Diabetes on Indonesian Households. PLoS ONE 2014, 9, e99572. [Google Scholar] [CrossRef]
- Padmawati, R.S.; Ng, N.; Prabandari, Y.S.; Nichter, M. Smoking among diabetes patients in Yogyakarta, Indonesia: Cessation efforts are urgently needed. Trop. Med. Int. Health 2009, 14, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Ligita, T.; Wicking, K.; Francis, K.; Harvey, N.; Nurjannah, I. How people living with diabetes in Indonesia learn about their disease: A grounded theory study. PLoS ONE 2019, 14, e0212019. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, R.; Dennis, S.; Hasan, I.; Slewa, J.; Chen, W.; Tian, D.; Bobba, S.; Zwar, N. A systematic review of chronic disease management interventions in primary care. BMC Fam. Pr. 2018, 19, 1–13. [Google Scholar] [CrossRef]
- Holdford, D.A. Pharmacoeconomics: From Theory to Practice. Am. J. Pharm. Educ. 2010, 74, 53. [Google Scholar] [CrossRef]
- Bodrogi, J.; Kaló, Z. Principles of pharmacoeconomics and their impact on strategic imperatives of pharmaceutical research and development. Br. J. Pharmacol. 2010, 159, 1367–1373. [Google Scholar] [CrossRef] [Green Version]
- A Suwantika, A.; Postma, M.J. Effect of breastfeeding promotion interventions on cost-effectiveness of rotavirus immunization in Indonesia. BMC Public Health 2013, 13, 1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics of West Java Province, Indonesia. Total Population in West Java Province, Indonesia. Available online: https://jabar.bps.go.id/dynamictable/2020/02/11/212/-jumlah-penduduk-dan-jenis-kelamin-menurut-kabupaten-kota-di-provinsi-jawa-barat-2019.html (accessed on 15 January 2020).
- West Java Province. In 2040, Approximately 642 Million People in the World Will Suffer Diabetes. Available online: https://jabarprov.go.id/index.php/news/26203/2040_Sebanyak_642_Juta_Penduduk_Dunia_Akan_Mengalami_Diabetes (accessed on 15 January 2020).
- Kalyani, R.R.; Egan, J.M. Diabetes and Altered Glucose Metabolism with Aging. Endocrinol. Metab. Clin. N. Am. 2013, 42, 333–347. [Google Scholar] [CrossRef] [Green Version]
- Chia Chee, W.; Egan Josephine, M.; Ferrucci, L. Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circ. Res. 2018, 123, 886–904. [Google Scholar] [CrossRef] [PubMed]
- Comino, E.J.; Harris, M.F.; Islam, M.D.F.; Tran, D.T.; Jalaludin, B.; Jorm, L.; Flack, J.; Haas, M. Impact of diabetes on hospital admission and length of stay among a general population aged 45 year or more: A record linkage study. BMC Health Serv. Res. 2015, 15, 1–13. [Google Scholar] [CrossRef]
- Allende-Vigo, M.Z.; González-Rosario, R.A.; González, L.; Sánchez, V.; Vega, M.A.; Alvarado, M.; Ramón, R.O. Inpatient Management of Diabets Mellitus among Noncritically Ill Patients at the University Hospital of Puerto Rico. Endocr. Pr. 2014, 20, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, H.; Kawai, K.; Kobayashi, M.; on behalf of the Japan Diabetes Clinical Data Management Study Group. Microalbuminuria Is Common in Japanese Type 2 Diabetic Patients: A nationwide survey from the Japan Diabetes Clinical Data Management Study Group (JDDM 10). Diabetes Care 2007, 30, 989–992. [Google Scholar] [CrossRef] [Green Version]
- Retnakaran, R.; Cull, C.A.; Thorne, K.I.; Adler, A.I.; Holman, R.R.; for the UKPDS Study Group. Risk Factors for Renal Dysfunction in Type 2 Diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006, 55, 1832–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andayani, T.M.; Ibrahim, M.I.M.; Asdie, A.H. Assessing the Impact of Complications on the Direct Medical Costs of Type 2 Diabetes Mellitus Outpatients. Int. J. Curr. Pharm. Res. 2010, 2, 32–35. [Google Scholar]
- Soewondo, P.; Ferrario, A.; Tahapary, D.L. Challenges in diabetes management in Indonesia: A literature review. Glob. Health 2013, 9, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwantika, A.A.; Zakiyah, N.; Lestari, K.; Postma, M.J. Accelerating the introduction of rotavirus immunization in Indonesia. Expert Rev. Vaccines 2014, 13, 463–472. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, A.C.O.; Cazarim, M.D.S.; Sanches, C.; Pereira, L.R.L.; Camargos, A.M.T.; Aquino, J.A.; Baldoni, A.O. Cost-effectiveness analysis of a pharmacotherapeutic empowerment strategy for patients with type 2 diabetes mellitus. BMJ Open Diabetes Res. Care 2019, 7, e000647. [Google Scholar] [CrossRef] [Green Version]
- Siegel, K.R.; Ali, M.K.; Zhou, X.; Ng, B.P.; Jawanda, S.; Proia, K.; Zhang, X.; Gregg, E.W.; Albright, A.L.; Zhang, P. Cost-effectiveness of Interventions to Manage Diabetes: Has the Evidence Changed Since 2008? Diabetes Care 2020, 43, 1557–1592. [Google Scholar] [CrossRef]
- Najafi, B.; Farzadfar, F.; Ghaderi, H.; Hadian, M. Cost effectiveness of type 2 diabetes screening: A systematic review. Med. J. Islam. Repub. Iran 2016, 30, 326. [Google Scholar]
- Piatt, G.; Ye, W.; Kuo, S.; Sinco, B.R.; Herman, W.H.; Spencer, M.S.; Palmisano, G.; Heisler, M.; Kieffer, E.C. Cost-Effectiveness of Diabetes Self-Management Education and Support in the Community—Projections from a Randomized Controlled Trial. Diabetes 2018, 67, 703. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.C.; Driver, V.R.; Wrobel, J.S.; Armstrong, D.G. Foot ulcers in the diabetic patient, prevention and treatment. Vasc. Health Risk Manag. 2007, 3, 65–76. [Google Scholar]


{kind=link}
| Category | Sub-Category | Total | % |
|---|---|---|---|
| Gender | Male | 58 | 43.28% |
| Female | 76 | 56.72% | |
| Ages (years) | 18–44 | 10 | 7.46% |
| 45–64 | 93 | 69.40% | |
| ≥65 | 31 | 23.14% | |
| Length of stay (days) | 1–3 | 14 | 10.45% |
| 4–10 | 73 | 54.48% | |
| >10 | 47 | 35.07% | |
| Types of T2DM complications | Without complication | 8 | 5.97% |
| Kidney disease | 104 | 77.61% | |
| PVD | 22 | 16.42% |
| Types of T2DM Complication | Year | Cost * | ||||||
|---|---|---|---|---|---|---|---|---|
| Hospital Room | Doctors’ Fee | Medicines | Laboratory Tests | Blood Transfusion | Medical Services | Total Cost | ||
| Without complication | 2014 | 2,647,000 | 500,000 | 2,456,500 | 1,439,500 | - | 345,940 | 7,388,940 |
| 2015 | 2,864,887 | 486,812 | 547,225 | 880,825 | - | 1,315,689 | 6,095,439 | |
| 2016 | 4,825,000 | 800,000 | 843,000 | 680,376 | - | 1,983,500 | 9,131,876 | |
| 2017 | 7,711,548 | 1,076,358 | 1,192,141 | 754,391 | 297,056 | 871,972 | 11,903,465 | |
| Average | 4,512,109 | 715,792 | 1,258,716 | 938,773 | 74,264 | 1,129,275 | 8,629,930 | |
| Complication of kidney disease | 2014 | 1,606,250 | 237,813 | 1,657,331 | 1,634,793 | 223,750 | 2,577,721 | 7,937,657 |
| 2015 | 1,948,082 | 288,436 | 2,047,165 | 1,834,698 | 151,364 | 2,277,201 | 8,546,946 | |
| 2016 | 2,424,766 | 509,571 | 2,716,532 | 2,651,687 | 856,325 | 3,364,893 | 12,523,774 | |
| 2017 | 4,048,111 | 451,043 | 3,106,726 | 2,556,657 | 455,057 | 3,873,361 | 14,490,955 | |
| Average | 2,506,802 | 371,716 | 2,381,939 | 2,169,459 | 421,624 | 3,023,294 | 10,874,833 | |
| Complication of PVD | 2014 | 7,055,200 | 1,427,500 | 10,563,515 | 3,629,325 | 618,300 | 9,194,600 | 32,488,440 |
| 2015 | 9,746,297 | 1,888,830 | 11,592,904 | 3,214,702 | 1,301,086 | 10,942,231 | 38,686,049 | |
| 2016 | 4,576,995 | 792,428 | 5,751,749 | 3,781,058 | 407,443 | 7,439,602 | 22,749,276 | |
| 2017 | 5,180,618 | 878,947 | 13,208,775 | 3,846,804 | 1,148,742 | 7,700,424 | 31,964,311 | |
| Average | 6,639,778 | 1,246,926 | 10,279,236 | 3,617,972 | 868,893 | 8,819,214 | 31,472,019 | |
| Types of T2DM Complication | Year | Cost * | ||||||
|---|---|---|---|---|---|---|---|---|
| Hospital Room | Doctors’ Fee | Medicines | Laboratory Tests | Blood Transfusion | Medical Services | Total Cost | ||
| Without complication | 2014 | 35.82% | 6.77% | 33.25% | 19.48% | 0.00% | 4.68% | 100.00% |
| 2015 | 47.00% | 7.99% | 8.98% | 14.45% | 0.00% | 21.58% | 100.00% | |
| 2016 | 52.84% | 8.76% | 9.23% | 7.45% | 0.00% | 21.72% | 100.00% | |
| 2017 | 64.78% | 9.04% | 10.02% | 6.34% | 2.50% | 7.33% | 100.00% | |
| Average | 50.11% | 8.14% | 15.37% | 11.93% | 0.62% | 13.83% | 100.00% | |
| Complication of kidney disease | 2014 | 20.24% | 3.00% | 20.88% | 20.60% | 2.82% | 32.47% | 100.00% |
| 2015 | 22.79% | 3.37% | 23.95% | 21.47% | 1.77% | 26.64% | 100.00% | |
| 2016 | 19.36% | 4.07% | 21.69% | 21.17% | 6.84% | 26.87% | 100.00% | |
| 2017 | 27.94% | 3.11% | 21.44% | 17.64% | 3.14% | 26.73% | 100.00% | |
| Average | 22.58% | 3.39% | 21.99% | 20.22% | 3.64% | 28.18% | 100.00% | |
| Complication of PVD | 2014 | 21.72% | 4.39% | 32.51% | 11.17% | 1.90% | 28.30% | 100.00% |
| 2015 | 25.19% | 4.88% | 29.97% | 8.31% | 3.36% | 28.28% | 100.00% | |
| 2016 | 20.12% | 3.48% | 25.28% | 16.62% | 1.79% | 32.70% | 100.00% | |
| 2017 | 16.21% | 2.75% | 41.32% | 12.03% | 3.59% | 24.09% | 100.00% | |
| Average | 20.81% | 3.88% | 32.27% | 12.03% | 2.66% | 28.34% | 100.00% | |
| Year | Types of T2DM Complication | Total Cost (IDR) | Blood Glucose Reduction (mg/dL) | p-Value |
|---|---|---|---|---|
| 2014 | Without complication | 11,330,400 | 95 | 0.01639 * |
| Complication of kidney disease | 15,064,238 | 98 | ||
| Complication of PVD | 21,475,940 | 65 | ||
| 2015 | Without complication | 11,031,545 | 121 | 0.01747 * |
| Complication of kidney disease | 14,813,909 | 84 | ||
| Complication of PVD | 21,377,659 | 169 | ||
| 2016 | Without complication | 6,094,319 | 54 | 0.02735 * |
| Complication of kidney disease | 9,663,898 | 93 | ||
| Complication of PVD | 14,614,062 | 87 | ||
| 2017 | Without complication | 9,832,741 | 15 | 0.00227 * |
| Complication of kidney disease | 10,396,008 | 64 | ||
| Complication of PVD | 12,256,473 | 98 | ||
| Average | Without complication | 9,572,251 | 71 | 0.01453 * |
| Complication of kidney disease | 12,484,513 | 85 | ||
| Complication of PVD | 17,431,034 | 105 | ||
| ICER ** | Complication of kidney disease | IDR 215,723 | ||
| per 1 mg/dL blood glucose reduction | ||||
| Complication of PVD | IDR 234,591 | |||
| per 1 mg/dL blood glucose reduction | ||||
| Year | Types of T2DM Complication | Total Cost (IDR) | Blood Glucose Reduction (mg/dL) | p-Value |
|---|---|---|---|---|
| 2014 | Without complication | 7,388,940 | 95 | 0.097 |
| Complication of kidney disease | 7,937,657 | 98 | ||
| Complication of PVD | 32,488,440 | 65 | ||
| 2015 | Without complication | 6,095,439 | 121 | 0.11595 |
| Complication of kidney disease | 8,546,946 | 84 | ||
| Complication of PVD | 38,686,049 | 169 | ||
| 2016 | Without complication | 9,131,875 | 54 | 0.03434 * |
| Complication of kidney disease | 12,523,774 | 93 | ||
| Complication of PVD | 22,749,276 | 87 | ||
| 2017 | Without complication | 11,903,465 | 15 | 0.04541 * |
| Complication of kidney disease | 14,490,955 | 64 | ||
| Complication of PVD | 31,964,311 | 98 | ||
| Average | Without complication | 8,629,930 | 71 | 0.07219 |
| Complication of kidney disease | 10,874,833 | 85 | ||
| Complication of PVD | 31,472,019 | 105 | ||
| ICER ** | Complication of kidney disease | IDR 166,289 | ||
| per 1 mg/dL blood glucose reduction | ||||
| Complication of PVD | IDR 681,853 | |||
| per 1 mg/dL blood glucose reduction | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priyadi, A.; Permana, H.; Muhtadi, A.; Sumiwi, S.A.; Sinuraya, R.K.; Suwantika, A.A. Cost-Effectiveness Analysis of Type 2 Diabetes Mellitus (T2DM) Treatment in Patients with Complications of Kidney and Peripheral Vascular Diseases in Indonesia. Healthcare 2021, 9, 211. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020211
Priyadi A, Permana H, Muhtadi A, Sumiwi SA, Sinuraya RK, Suwantika AA. Cost-Effectiveness Analysis of Type 2 Diabetes Mellitus (T2DM) Treatment in Patients with Complications of Kidney and Peripheral Vascular Diseases in Indonesia. Healthcare. 2021; 9(2):211. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020211
Chicago/Turabian StylePriyadi, Akhmad, Hikmat Permana, Ahmad Muhtadi, Sri A. Sumiwi, Rano K. Sinuraya, and Auliya A. Suwantika. 2021. "Cost-Effectiveness Analysis of Type 2 Diabetes Mellitus (T2DM) Treatment in Patients with Complications of Kidney and Peripheral Vascular Diseases in Indonesia" Healthcare 9, no. 2: 211. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9020211