
Relationship between Training Load Management and Immunoglobulin A to Avoid Immunosuppression after Soccer Training and Competition: A Theoretical Framework Based on COVID-19 for Athletes’ Healthcare

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Screening Strategy and Study Selection
2.3. Data Analysis
3. Results
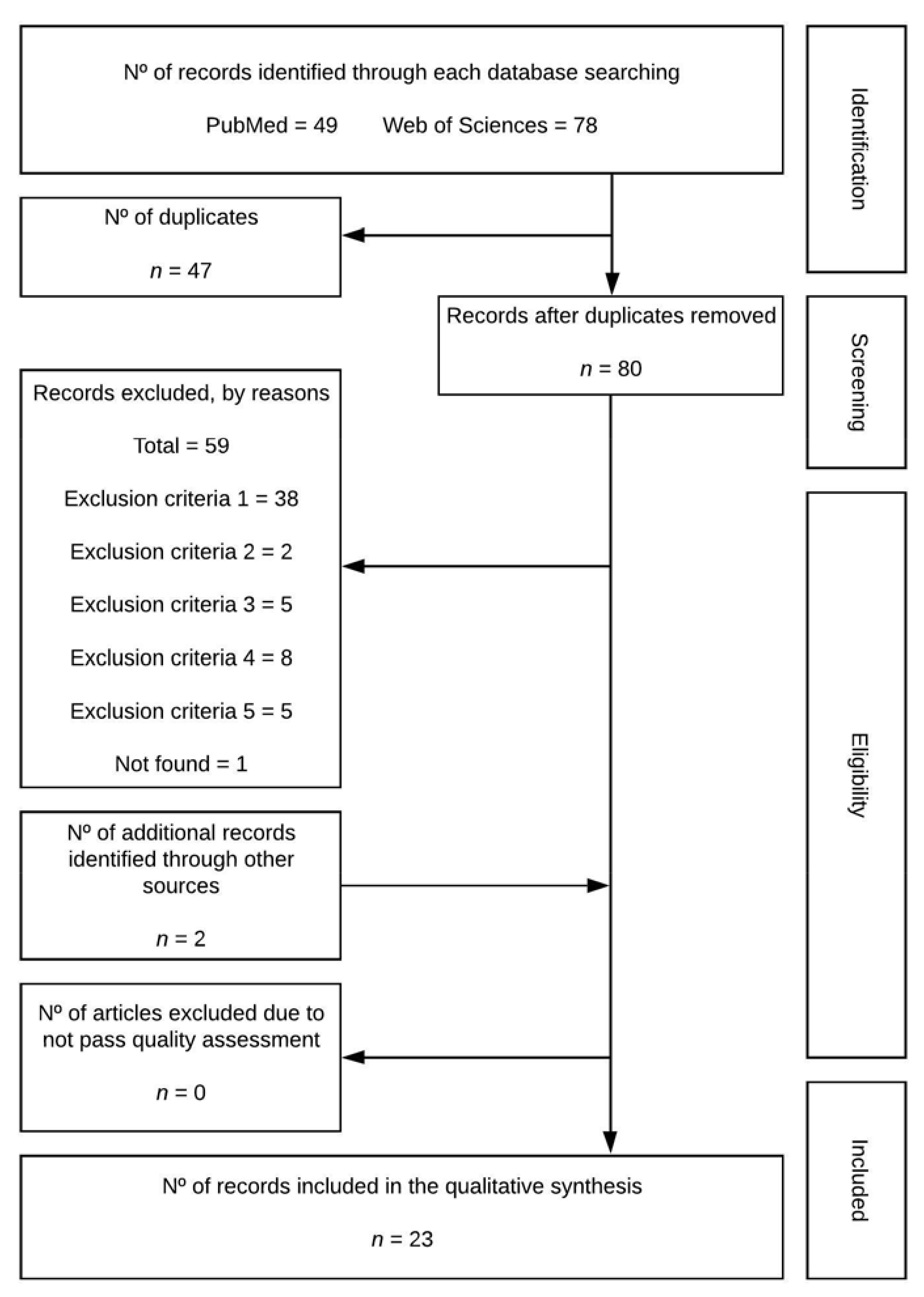
3.1. Identification and Selection of Studies
3.2. Study Characteristics
3.2.1. Repeated Sprint Ability and Treadmill Exercises
3.2.2. Matches during Intensive and Non-Intensive Fixture Schedules
3.2.3. Preparation Periods (Matches/Training or Training) during Intensive and Non-Intensive Fixture Schedules
4. Discussion
4.1. Repeated Sprint Ability and Treadmill Exercises
4.2. Matches during Intensive and Non-Intensive Fixture Schedules
4.3. Preparation Periods (Matches/Training or Training) during Intensive and Non-Intensive Fixture Schedules
5. Study Limitations
6. Conclusions
7. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Rico-González, M.; Mendez-Villanueva, A.; Los Arcos, A. Training load periodization in soccer with one official match a week: A systematic review. In An Essential Guide to Sports Performance; NOVA Science Publisher: New York, NY, USA, 2020; pp. 123–166. ISBN 978-1-5361-7608-7. [Google Scholar]
- Figueiredo, P.; Nassis, G.P.; Brito, J. Within-Subject Correlation Between Salivary IgA and Measures of Training Load in Elite Football Players. Int. J. Sports Physiol. Perform. 2019, 14, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.L.; Wong, D.P.; Dunlop, G.; Groussard, C.; Kebsi, W.; Dellal, A.; Morgans, R.; Zouhal, H. High-Intensity Training and Salivary Immunoglobulin A Responses in Professional Top-Level Soccer Players: Effect of Training Intensity. J. Strength. Cond. Res. 2016, 30, 2460–2469. [Google Scholar] [CrossRef] [PubMed]
- Keaney, L.C.; Kilding, A.E.; Merien, F.; Dulson, D.K. The Impact of Sport Related Stressors on Immunity and Illness Risk in Team-Sport Athletes. J. Sci. Med. Sport. 2018, 21, 1192–1199. [Google Scholar] [CrossRef] [PubMed]
- Freitas, C.G.; Aoki, M.S.; Arruda, A.F.S.; Franciscon, C.; Moreira, A. Monitoring Salivary Immunoglobulin A Responses to Official and Simulated Matches In Elite Young Soccer Players. J. Hum. Kinet. 2016, 53, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M. Immune Function and Exercise. Eur. J. Sport Sci. 2004, 4, 52–66. [Google Scholar] [CrossRef]
- Fahlman, M.M.; Engels, H.-J. Mucosal IgA and URTI in American College Football Players: A Year Longitudinal Study. Med. Sci. Sports Exerc. 2005, 37, 374–380. [Google Scholar] [CrossRef]
- Moreira, A.; Mortatti, A.L.; Arruda, A.F.S.; Freitas, C.G.; de Arruda, M.; Aoki, M.S. Salivary IgA Response and Upper Respiratory Tract Infection Symptoms During a 21-Week Competitive Season in Young Soccer Players. J. Strength. Cond. Res. 2014, 28, 467–473. [Google Scholar] [CrossRef]
- Mortatti, A.L.; Moreira, A.; Aoki, M.S.; Crewther, B.T.; Castagna, C.; de Arruda, A.F.S.; Filho, J.M. Effect of Competition on Salivary Cortisol, Immunoglobulin A, and Upper Respiratory Tract Infections in Elite Young Soccer Players. J. Strength. Cond. Res. 2012, 26, 1396–1401. [Google Scholar] [CrossRef]
- Lopes, R.F.; Minuzzi, L.G.; Figueiredo, A.J.; Gonçalves, C.; Tessitore, A.; Capranica, L.; Teixeira, A.M.; Rama, L. Upper Respiratory Symptoms (URS) and Salivary Responses across a Season in Youth Soccer Players: A Useful and Non-Invasive Approach Associated to URS Susceptibility and Occurrence in Young Athletes. PLoS ONE 2020, 15, e0236669. [Google Scholar] [CrossRef]
- Bisciotti, G.N.; Eirale, C.; Corsini, A.; Baudot, C.; Saillant, G.; Chalabi, H. Return to Football Training and Competition after Lockdown Caused by the COVID-19 Pandemic: Medical Recommendations. Biol. Sport. 2020, 37, 313. [Google Scholar] [CrossRef] [PubMed]
- Primorac, D.; Matišić, V.; Molnar, V.; Bahtijarević, Z.; Polašek, O. Pre-Season Football Preparation in the Era of COVID-19: Croatian Football Association Model. J. Glob. Health 2020, 10, 010352. [Google Scholar] [CrossRef]
- Putlur, P.; Foster, C.; Miskowski, J.A.; Kane, M.K.; Burton, S.E.; Scheett, T.P.; McGuigan, M.R. Alteration of Immune Function in Women Collegiate Soccer Players and College Student. J. Sports Sci. Med. 2004, 3, 234. [Google Scholar] [PubMed]
- Milanez, V.F.; Ramos, S.P.; Okuno, N.M.; Boullosa, D.A. Evidence of a Non-Linear Dose-Response Relationship between Training Load and Stress Markers in Elite Female Futsal Players. J. Sports Sci. Med. 2014, 13, 22. [Google Scholar] [PubMed]
- Padoin, S. Effects of Futsal Demands on Serum and Salivary Levels of Trace Elements and Minerals Detected by Total Reflection X-ray Fluorescence. Biol. Trace Elem. Res. 2019, 193, 73–80. [Google Scholar] [CrossRef]
- Vardiman, J.P.; Riggs, C.E.; Galloway, D.L.; Waxman, M.B.; Touchberry, C.D.; Gallagher, P.M. Salivary IgA Is Not a Reliable Indicator of Upper Respiratory Infection in Collegiate Female Soccer Athletes. J. Strength. Cond. Res. 2011, 25, 1937–1942. [Google Scholar] [CrossRef]
- Padoan, A.; Sciacovelli, L.; Basso, D.; Negrini, D.; Zuin, S.; Cosma, C.; Faggian, D.; Matricardi, P.; Plebani, M. IgA-Ab Response to Spike Glycoprotein of SARS-CoV-2 in Patients with COVID-19: A Longitudinal Study. Clin. Chim. Acta 2019, 507, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B.; Anderson, L.; Anglem, N.; Armstrong, S.; Baker, S.; Beable, S.; Burt, P.; Coleman, L.; Doughty, R.; Edwards, T.; et al. Medical Considerations for Supporting Elite Athletes during the Post-Peak Phase of the New Zealand COVID-19 Pandemic: A New Zealand Sporting Code Consensus. N. Z. Med. J. 2020, 133, 10. [Google Scholar]
- Impellizzeri, F.M.; Franchi, M.V.; Sarto, F.; Meyer, T.; Coutts, A.J. Sharing Information Is Probably More Helpful than Providing Generic Training Recommendations on Return to Play after COVID-19 Home Confinement. Sci. Med. Footb. 2020, 4, 169–170. [Google Scholar] [CrossRef]
- Rico-González, M.; Clemente, F.M.; Oliveira, R.; Bustamante, N.; Pino, J. Part I: Relationship among Training Load Management, Salivary Immunoglobulin A, and Upper Respiratory Tract Infection in Team Sport: A Systematic Review. Healthcare 2021, 9, 366. [Google Scholar] [CrossRef] [PubMed]
- Rico-González, M.; Pino-Ortega, J.; Clemente, F.; Los Arcos, A. Guidelines for Performing Systematic Reviews in Sports Science. Biol. Sport. 2022, 39. in press. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues de Araujo, V.; Lisboa, P.; Boaventura, G.; Caramez, F.; Pires, L.; Oliveira, E.; Moura, E.; Casimiro-Lopes, G. Acute High-Intensity Exercise Test in Soccer Athletes Affects Salivary Biochemical Markers. Free Radic. Res. 2018, 52, 850–855. [Google Scholar] [CrossRef]
- Drust, B.; Reilly, T.; Cable, N.T. Physiological Responses to Laboratory-Based Soccer-Specific Intermittent and Continuous Exercise. J. Sports Sci. 2000, 18, 885–892. [Google Scholar] [CrossRef]
- Page, R.M.; Marrin, K.; Brogden, C.M.; Greig, M. Physical Response to a Simulated Period of Soccer-Specific Fixture Congestion. J. Strength Cond. Res. 2019, 33, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Sari-Sarraf, V.; Reilly, T.; Doran, D. Salivary IgA Response to Intermittent and Continuous Exercise. Int. J. Sports Med. 2006, 27, 849–855. [Google Scholar] [CrossRef]
- Sari-Sarraf, V.; Reilly, T.; Doran, D.A.; Atkinson, G. The Effects of Single and Repeated Bouts of Soccer-Specific Exercise on Salivary IgA. Arch. Oral. Biol. 2007, 52, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Sari-Sarraf, V.; Reilly, T.; Doran, D.; Atkinson, G. Effects of Repeated Bouts of Soccer-Specific Intermittent Exercise on Salivary IgA. Int. J. Sports Med. 2008, 29, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Maya, J.; Marquez, P.; Peñailillo, L.; Contreras-Ferrat, A.; Deldicque, L.; Zbinden-Foncea, H. Salivary Biomarker Responses to Two Final Matches in Women’s Professional Football. J. Sports Sci. Med. 2016, 15, 365. [Google Scholar]
- Moreira, A.; Arsati, F.; Cury, P.R.; Franciscon, C.; de Oliveira, P.R.; de Araújo, V.C. Salivary Immunoglobulin A Response to a Match in Top-Level Brazilian Soccer Players. J. Strength Cond. Res. 2009, 23, 1968–1973. [Google Scholar] [CrossRef]
- Moreira, A.; Bradley, P.; Carling, C.; Arruda, A.F.S.; Spigolon, L.M.P.; Franciscon, C.; Aoki, M.S. Effect of a Congested Match Schedule on Immune-Endocrine Responses, Technical Performance and Session-RPE in Elite Youth Soccer Players. J. Sports Sci. 2016, 34, 2255–2261. [Google Scholar] [CrossRef]
- Morgans, R.; Orme, P.; Anderson, L.; Drust, B.; Morton, J.P. An Intensive Winter Fixture Schedule Induces a Transient Fall in Salivary IgA in English Premier League Soccer Players. Res. Sports Med. 2014, 22, 346–354. [Google Scholar] [CrossRef]
- Peñailillo, L.; Maya, L.; Niño, G.; Torres, H.; Zbinden-Foncea, H. Salivary Hormones and IgA in Relation to Physical Performance in Football. J. Sports Sci. 2015, 33, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
- Morgans, R.; Owen, A.; Doran, D.; Drust, B.; Morton, J.P. Prematch Salivary Secretory Immunoglobulin A in Soccer Players From the 2014 World Cup Qualifying Campaign. Int. J. Sports Physiol. Perform. 2015, 10, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, D.; Akimoto, T.; Suzuki, S.; Kono, I. Daily Changes of Salivary Secretory Immunoglobulin A and Appearance of Upper Respiratory Symptoms during Physical Training. Sports Med. Phys. Fit. 2006, 46, 152–157. [Google Scholar]
- Fredericks, S. Changes in Salivary Immunoglobulin A (IgA) Following Match-Play and Training among English Premiership Footballers. Med. J. Malays. 2012, 67, 5. [Google Scholar]
- Owen, A.L.; Morgans, R.; Kavanagh, R.; Djaoui, L. Salivary IgA and Pre-Training Wellness Status across an International Soccer Qualifying and Finals Campaign (Euro 2016). Int. J. Sports Sci. Coach. 2018, 13, 794–803. [Google Scholar] [CrossRef]
- Francavilla, V.C.; Vitale, F.; Ciaccio, M.; Bongiovanni, T.; Marotta, C.; Caldarella, R.; Todaro, L.; Zarcone, M.; Muratore, R.; Bellia, C.; et al. Use of Saliva in Alternative to Serum Sampling to Monitor Biomarkers Modifications in Professional Soccer Players. Front. Physiol. 2018, 9, 1828. [Google Scholar] [CrossRef] [Green Version]
- Wragg, C.B. Evaluation of the Reliability and Validity of a Soccer-Specific field Test of Repeated Sprint Ability. Eur. J. Appl. Physiol. 2000, 83, 77–83. [Google Scholar] [CrossRef]
- Harper, D.J.; Carling, C.; Kiely, J. High-Intensity Acceleration and Deceleration Demands in Elite Team Sports Competitive Match Play: A Systematic Review and Meta-Analysis of Observational Studies. Sports Med. 2019, 49, 1923–1947. [Google Scholar] [CrossRef] [Green Version]
- Haneishi, K.; Fry, A.C.; Moore, C.A.; Schilling, B.K.; Li, Y.; Fry, M.D. Cortisol and Stress Responses during a Game and Practice in Female Collegiate Soccer Players. J. Strength Cond. Res. 2007, 21, 583–588. [Google Scholar]
- Carmody, S.; Ahmad, I.; Gouttebarge, V.; Malhotra, A.; Glover, D.; Massey, A. Infographics. Football-Specific Strategies to Reduce COVID-19 Transmission. Br. J. Sports Med. 2020, 54, 1362–1364. [Google Scholar] [CrossRef] [PubMed]
- Castagna, C.; Bizzini, M.; Leguizamon, A.P.; Pizzi, A.; Torquati, R.; Póvoas, S. Considerations and Best Practices for Elite Football Officials Return to Play after COVID-19 Confinement. Manag. Sport Leis. 2020, 1–8. [Google Scholar] [CrossRef]
- Mohr, M.; Nassis, G.P.; Brito, J.; Randers, M.B.; Castagna, C.; Parnell, D.; Krustrup, P. Return to Elite Football after the COVID-19 Lockdown. Manag. Sport Leis. 2020, 1–9. [Google Scholar] [CrossRef]
- Huyghe, T.; Bird, S.; Calleja-González, J.; Alcaraz, P.E. Season Suspension and Summer Extension: Unique Opportunity for Professional Team-Sport Athletes and Support Staff during and Following the COVID-19 Crisis. Front. Sports Act. Living 2020, 2, 98. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ref. | Sample | Stressor | Immunology (IgA) | URTS/URTI Relationship | Lesson Learned and Concluding Remarks | ||||
|---|---|---|---|---|---|---|---|---|---|
| Int. Fix. Schedule | Test | Volume | Intensity | Salivary Test | Outcomes | ||||
| Rodrigues de Araujo et al. [23] | 32 male professionals | No | HIIE [39] | 7 × 40 m sprint with 25 s between each of them | Sprint | Post exercise (Immediately) | Unaltered in spite of its exhaustive characteristics | - | HIIE tests could be conducted without short-term immunosuppression risks |
| Sari-Sarraf et al. [26] | 8 males not professionals | No | Soccer-specific intermittent [24] and continuous exercise | Intermittent exercise: 6 periods of 15 min. Continuous exercise: 2 periods of 45 min. | Exercise at the same average work-rate: Continuous: 141 HR/min; RPE: 10.8; Vel: 9.7 km/h. Intermittent: 142 HR/min; RPE: 11.9; Velocity: different intensities. | The week prior to commencement of exercise. -Before, at half-time, immediately post-exercise. -6 h, 24 h, and 48 h post-exercise. | Mean saliva concentration of IgA was unaffected either by both intermittent and continuous exercise. | - | Soccer-specific intermittent exercise did not suppress the sIgA compared to continuous exercise (with the same overall work rate), although there with not significant differences founds. |
| Sari-Sarraf et al. [27] | 10 males non-professionals | Yes | Two trials of soccer-specific intermittent exercise [24]: -Single session. -Double session. | -Single session at 14:30 h. -Double session in 1 day at 10:30 (1st training) and 14:30 (2nd training). | Intermittent exercise | -Before and immediately after exercise. | Single session: sIgA level increased significantly immediately post-exercise. -Double session: it does not appear a suppression of salivary IgA outcomes. | - | Two 90 min exercise sessions performed at a moderate intensity with a 2.25 h rest between them, do not necessarily have adverse effects on sIgA. |
| Sari-Sarraf et al. [28] | 9 males amateur | Yes | 2 trials of intermittent exercise 48 h apart on a motorized treadmill [24] | 6 periods of 15 min. 15 min of rest between 3–4 periods. | Increasing exercise intensities (standing, walking, jogging, cruising and sprinting). | -Before 2 exercise trials. -Immediately after 2 exercise trials. -After 24 and 48 h following the 2 exercise trials. | -SIgA concentration was increased significantly immediately after both exercise trials and returned to pre-exercise levels 24 h later. -Although not statistically significant, there was a progressive decrease in resting SIgA concentration from exercise 1 to pre-exercise 2 (48 h after exercise 1) and to 48 h after exercise 2. | - | 2 bouts of intermittent exercise with 48 h between sessions were not sufficiently stressful to induce compromises in s-IgA responses. The trend for a progressive reduction in resting sIgA observed 48 h after each exercise session has clinical relevance is unclear. |
| Page et al. [25] | 10 male semi-professionals | Yes | Short-term soccer-specific fixture congestion [24]. | Six × 15-min bouts of intermittent activity, with a 15-min rest between 3rd and 4th 3 bouts in 5 days with 48 h between them. | High intensity activity interspersed with periods of low intensity passive and activity recovery. | Two times: -at rest. -Immediately after each trial. | No significant main effects for time or trial, and no significant interactions were identified for the sIgA data. | - | A period of short-term fixture congestion did not show a significant cumulative or residual fatigue response across successive bouts. |
| Ref. | Sample | Stressor | Immunology (IgA) | URTS/URTI Relationship | Conclusions | ||||
|---|---|---|---|---|---|---|---|---|---|
| Int. Fix. Schedule | Test | Volume | Intensity | Salivary Test | Outcomes | ||||
| Moreira et al. [30] | 24 male professionals | No | Friendly match | 70 min | Non-official match. | Before and after the match. | A significant decrease in IgA protein were observed. | - | Participating in a 70-min regulation match does not significantly affect sIgA. |
| Mortatti et al. [9] | 14 male U19 of Brazilian Championship | Yes | Congested match schedule | 7 matches in 20 days | A progressive increment from 1 match to 7 match. | In the morning of each match day. | The decrements in sIgA, specially, in matches 2 and 6 | Significant correlations were seen between the individual reports of URTI and the decrease in IgA levels in match 2 and 6. | The monitoring of sIgA could provide a useful and noninvasive approach for predicting URTI occurrences. In fact, decrements in mucosal immunity (IgA concentrations) may lead to a greater incidence of URTI. |
| Morgans et al. [32] | 21 males English Premier League | Yes | Intensity winter fixture schedule | From match 1 to 5 in 15 days. From match 6 to 7, 1 match/week | - | 2 days after each match prior breakfast | sIgA was significantly decreased after games 3, 4 and 5 when compared with game 1 After match 6–7 values were not different from game 1 | - | A congested winter fixture schedule induces detectable perturbations to mucosal immunity. A decline in sIgA was evident in players that played >50% of the total minutes played. |
| Peñailillo et al. [33] | 9 male professionals. | No | One international match. | Distance covered 9463 ± 458 m | - | Before and 10 min post-match. | IgA concentrations decreased by 74.5% post-match. | - | Decreased after match from pre-match salivary test. It seems that footballers with smaller decreases in testosterone levels covered more distance and decreased their immune function less. |
| Maya et al. [29] | 16 female professionals from the Chilean 1st League. | Yes | Two final matches in 3 days. | 2 final matches. | - | Before and after 2 matches (4 samples). | IgA concentration did not change after any match. | - | Salivary cortisol and testosterone concentrations increased especially after the first match of a final, without affecting IgA levels. It was speculated that increased testosterone concentration in women after football matches may play a protecting role against immune suppression usually observed after intense exercise. |
| Freitas et al. [5] | 26 male young (15 years) | Yes | -One official match. -One simulated match 48 h after the 1st match. | 35 min halves and 10 min rest. | Higher RPE for official match than non-official | 10 min before the pre-match warm-up. Post-match saliva samples were collected within 10–15 min of the end of each match. | - | - | Official match may have led to a decrease in the main mucosal immunity function parameter that could increase the risk of URTI. Plan appropriate training loads and recovery procedures to avoid or minimize the likelihood of URTI occurrences should be considered. |
| Moreira et al. [31] | 16 male young (14 years) | Yes | Congested match schedule | 7 matches in 7 days 1 match = 20 min halves and 10 min rest | Days 1 and 2 = 2 match/day. Days 3, 4 and 5 = rest days. Day 6 = 2 matches. Day 7 = 1 match. | Before breakfast each morning with match day (i.e., 1, 2, 6, and 7), and on day 3 (1st rest day). | A significant change in sIgA concentration was observed across time points. A decrease in sIgA concentration was reported between the 1st and the 7th. The sIgA concentration at the rest day was higher in comparison with all other time points except the 1st time point. | - | Accumulated fatigue induced by a congested match schedule might negatively affect their mucosal immunity. |
| Ref. | Sample | Stressor | Immunology (IgA) | URTS/URTI Relationship | Conclusions | ||||
|---|---|---|---|---|---|---|---|---|---|
| Int. Fix. Schedule | Test | Volume | Intensity | Salivary Test | Outcomes | ||||
| Putlur et al. [13] | 14 NCAA (Div. 3) female collegiate | No | 9-week competitive season | 9 weeks | - | At the beginning of each week | The levels of sIgA were suppressed throughout the course of the season. | 82% of illnesses could be explained by a preceding decrease in sIgA. | Decreased levels of sIgA and increases in the indices of training load (load, strain and monotony) were associated with an increase in the incidence of illness. |
| Nakamura et al. [35] | 12 males collegiate | No | A training period of 2 months | - | - | Daily | - | The saliva flow rate and sIgA secretion rate tended to decrease 3 days before the appearance of URTI symptoms compared to that in the non-infection period. | The findings suggest that monitoring of sIgA secretion rate may be useful for assessment of risk status of athletes for URTI. |
| Vardiman et al. [16] | 12 female collegiate. | No | 13 weeks during season | 2 weeks with 2 training sessions followed by 1 rest day. Four sessions and 2 days competition. Each session: 86 min | - | Eight age-matched controls. Samples were collected bimonthly from the athletes’ pre-and post-sport training sessions and pre- and post-90-min sedentary period for the controls. | There was no significant difference between the athletes’ and controls’ mean difference pre- to post-sport training absolute sIgA levels. | Analysis of URTI total symptom per day indicated that there was no difference between the athletes and controls throughout the 13-week. There was no significant correlation found between URTI per day and absolute sIgA, URTI and Total protein, or URTI and absolute sIgA/Total protein levels. | The lack of relationship between sIgA levels and URTI indicate that sIgA is not an appropriate measure to determine an athlete’s susceptibility. |
| Fredericks [36] | 24 males from EPL. | Yes | Training—training recovery | - | 1st week after summer off-season. Pre-season training exercises. | -Before training. -20 min after training. -18 h after training. | It was a significant difference in sIgA across the pre, post 20-min and post 18 h periods | - | The changes in sIgA reflect the expected pattern of pressures and stresses associated with training and match-play. Overnight rest was enough to reverse a decrease in sIgA observed following a training session, but not following two consecutive matches played within a short period. |
| 9 males from EPL. | Yes | Match—Match recovery | 53 h between matches. -1st half: 5.3 km -Whole match: 10.8 km. | Sample was a bottom team, and it plays against 1st and 2nd top teams. | -20 min after 1st match. -16 h after the 1st match. -20 min after 2nd match. -11 h after the 2nd match. | No significant difference between the 1st match post 20 min and the 1st match post 15h samples. No significant difference between the 20-min and 10 h post 2nd match. | |||
| Moreira et al. [8] | 26 male young (12 years) | No | 21-week competitive season divided into preseason, competitive season, and detraining | Preseason trainings: 12 Competitive period´s sessions: 7 Recovery sessions: 2 | - | Four time points: Before (T1) and after (T2) preseason, after the competitive phase (T3), and after the 2-week detraining phase (T4). | A significant increase in the sIgA rate was detected after the 2-week detraining period (T4), when compared with the value from T1. | URTI total symptom score was attenuated after the 2-week detraining period (T3–T4) when compared with T1–T2 and T2–T3. | Training and competition demand affect the mucosal immune responses. Adequate training periodization, including a short-detraining phase performed after accumulated training and competition periods might minimize undesirable outcomes such as mucosal immunosuppression and reduce URTI symptoms. |
| Morgans et al, [34] | 13 male professionals from the preparation camp for the 2014 FIFA World cup | Yes | Microcycle (days -4, -3, -2, -1) | Four training sessions. | - | 4 days preceding each game | sIgA displayed a progressive decline during the 4 days training period such that MD-1 values were significantly lower than both MD-4 and MD-3. | - | A short-term soccer-training camp in preparation for international competition induces detectable perturbations to mucosal immunity and thereby provides objective evidence for the administration of appropriate interventions to prepare players for the physical stress for the game day by self. |
| Owen et al. [3] | 10 male professionals from European top team | No | Training sessions with different intensities. | Four training sessions. | -Low intensity session: tactical, technical. -High intensity sessions: conditioning sessions | -Before investigation (3 tests for baseline). -Before and after each training session. | Post-training sIgA were not different between high-intensity and low-intensity sessions at the first three periods. However, at the 4th session, SIgA concentration for high-intensity session was significantly lower than the low intensity session. | - | High-intensity sessions may cause a significant decrease in players sIgA values during the post-exercise window when compared against low-intensity training. The intensity and volume of the training sessions may be more appropriate to monitor in order to determine the impact of the IgA value. Coaches and practitioners are encouraged to monitor sIgA in routine, and in particular during high-intensity training periods so as to take precautions to avoid URTI in highly trained athletes. |
| Owen et al. [37] | 37 male professionals. | Yes | Euro 2016 preparation period. Microcycle (days -4, -3, -2, -1) | - | Low, moderate, and high intensity sessions. | Pre-breakfast 90 min before training session. | Higher scores of sIgA were observed in MD-2 and MD-1, comparing to all others. No differences were found between playing positions with sIgA assessment. | - | A short-term preparation for international competition induces detectable perturbations in IgA. |
| Francavilla et al. [38] | 35 male professionals (Italian Serie A) | No | A season. | Players played a higher number of minutes at t1 and t3 while they were substituted more frequently in the t2 and t3. | - | Three times: t1: after the pre-season period and 16 official matches played. t2: after a winter break and three official matches played. t3: 2 days after the final match of the championship and 19 matches played. | sIgA mean concentrations: t1: 122 t2: 131 t3: 147 | - | No significant increase in the period characterized by a limited number of training sessions and of matches played. The weak increase in salivary IgA concentrations documented for the period of the season characterized by a limited number of training sessions, as compared to the periods of high-intensity training. |
| Figueiredo et al. [2] | 18 male professionals from the preparation camp for the Rio 2016 Olympic Games. | Yes | Microcycle | Four training consecutive sessions. | TL increases from day 1 to day 2 but lowered from day 2 to day 3. | 3 consecutive days before breakfast. Thus, the sIgA values reported represent day +1 of the preparation (each test assesses the effects of the previous training day). | -sIgA displayed a likely moderate decrease from day 1 to day 2 but increased on day 3. | - | sIgA can be used as an additional objective tool in monitoring football players. sIgA might be more responsive to training volume rather than intensity. |
| Lopes et al. [10] | U15: 17 players. U17: 22 players. U19: 18 players. | A season. | 1.5 h/session and 70 (U15), 80 (U17) and 90 (U19) minute match per week. | - | Monthly, before the 1st session of the week (after at least, 36 h of rest). | The U19 team tended to show higher mean sIgA values than the younger teams. | There was a trend to younger players (<15 years) were more prone to get an URTS episode. | Monitoring salivary biomarkers provides information on mucosal immunity with impact in URTI symptoms occurrence. Players older than 15 years might have a stronger immune response possibly because of a natural sports selection process, which retains the more resilient athletes. Coaches could manipulate training loads to attenuate the physical stressors imposed on athletes, especially at demanding and stressful periods. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rico-González, M.; Pino-Ortega, J.; Clemente, F.M.; Bustamante-Hernández, N. Relationship between Training Load Management and Immunoglobulin A to Avoid Immunosuppression after Soccer Training and Competition: A Theoretical Framework Based on COVID-19 for Athletes’ Healthcare. Healthcare 2021, 9, 856. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070856
Rico-González M, Pino-Ortega J, Clemente FM, Bustamante-Hernández N. Relationship between Training Load Management and Immunoglobulin A to Avoid Immunosuppression after Soccer Training and Competition: A Theoretical Framework Based on COVID-19 for Athletes’ Healthcare. Healthcare. 2021; 9(7):856. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070856
Chicago/Turabian StyleRico-González, Markel, José Pino-Ortega, Filipe Manuel Clemente, and Naia Bustamante-Hernández. 2021. "Relationship between Training Load Management and Immunoglobulin A to Avoid Immunosuppression after Soccer Training and Competition: A Theoretical Framework Based on COVID-19 for Athletes’ Healthcare" Healthcare 9, no. 7: 856. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9070856