
The Mediation Effect of Health Literacy on Social Support with Exchange and Depression in Community-Dwelling Middle-Aged and Older People in Taiwan


Abstract
:
1. Introduction
1.1. Social Support with Exchange and Depression
1.2. Social Support with Exchange and Health Literacy
1.3. Health Literacy and Depression
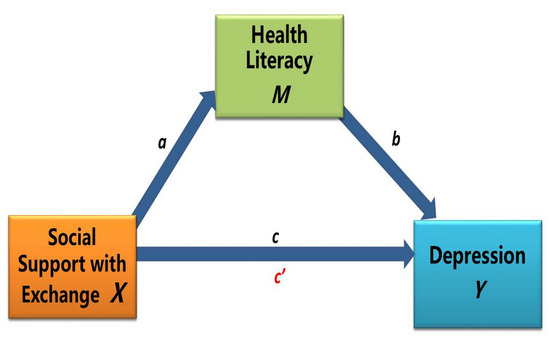
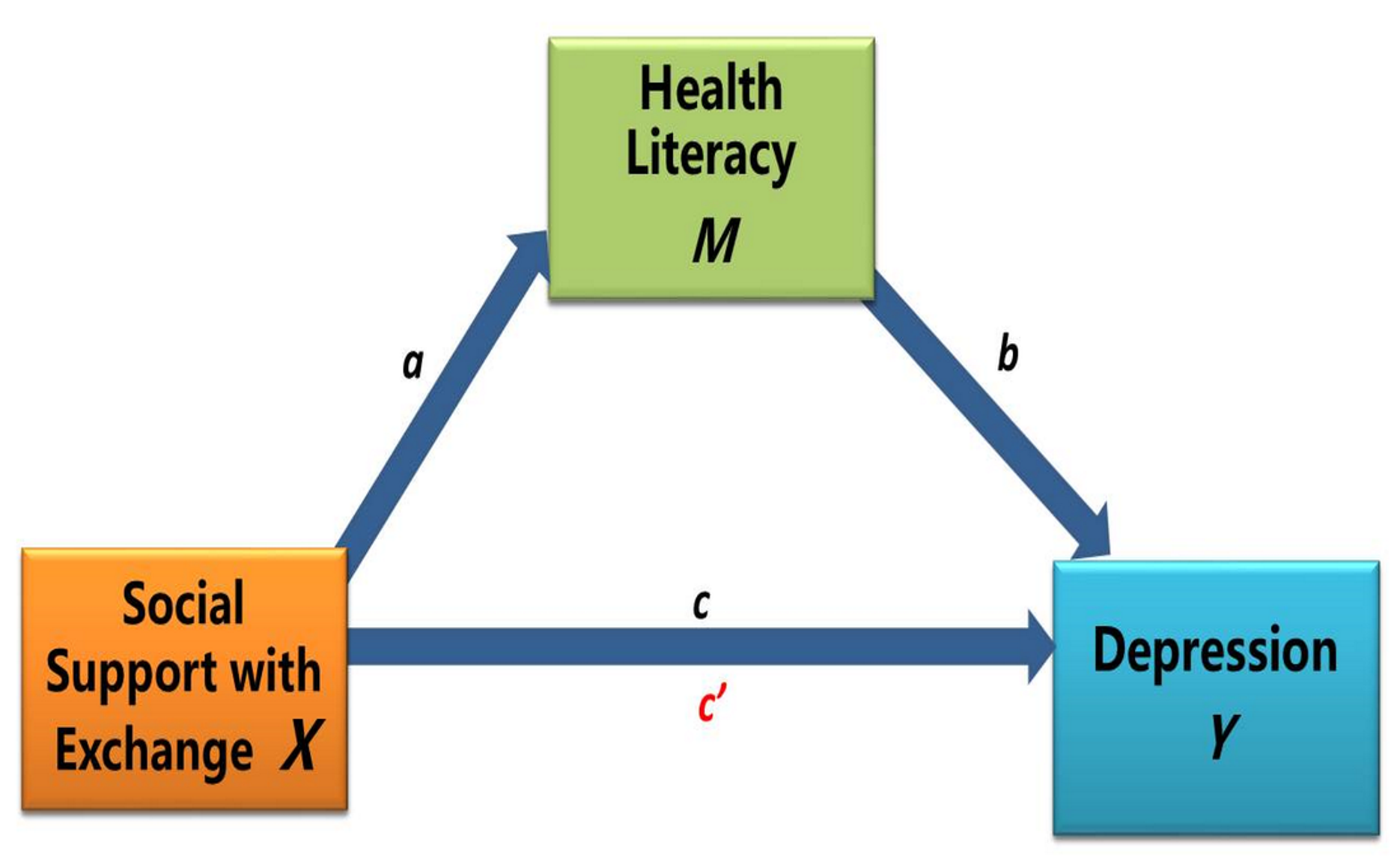
1.4. Health Literacy as a Mediator between Social Support and Depression
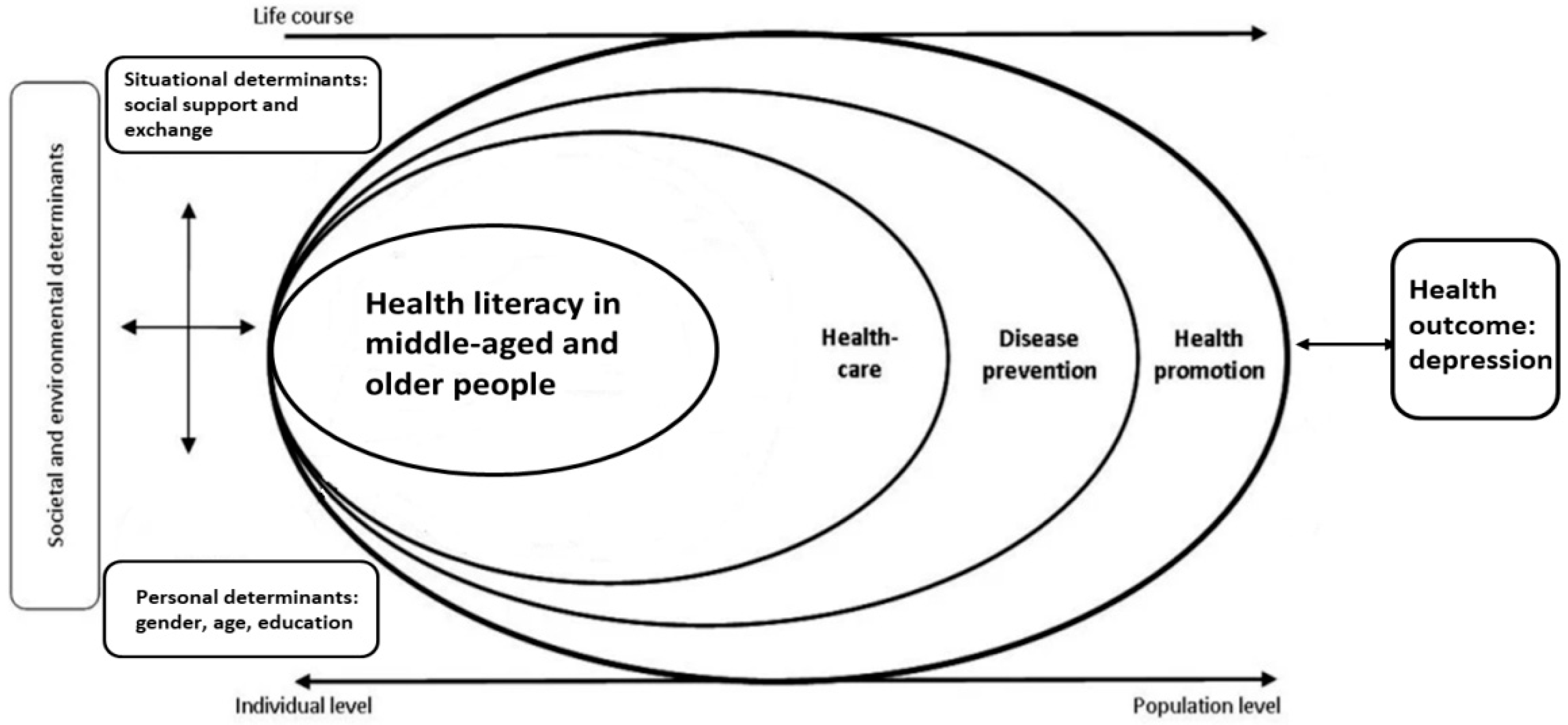
1.5. Theoretical Framework
2. Methods
2.1. Study Design and Data Collection
2.2. Participants
2.3. Measures
2.3.1. Demographic Characteristics
2.3.2. Social Support with Exchange Scale
2.3.3. Health Literacy Scale
2.3.4. Center for Epidemiological Studies Depression Scale (CES-D)
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. The Correlation of Health Literacy and Social Support with Depression
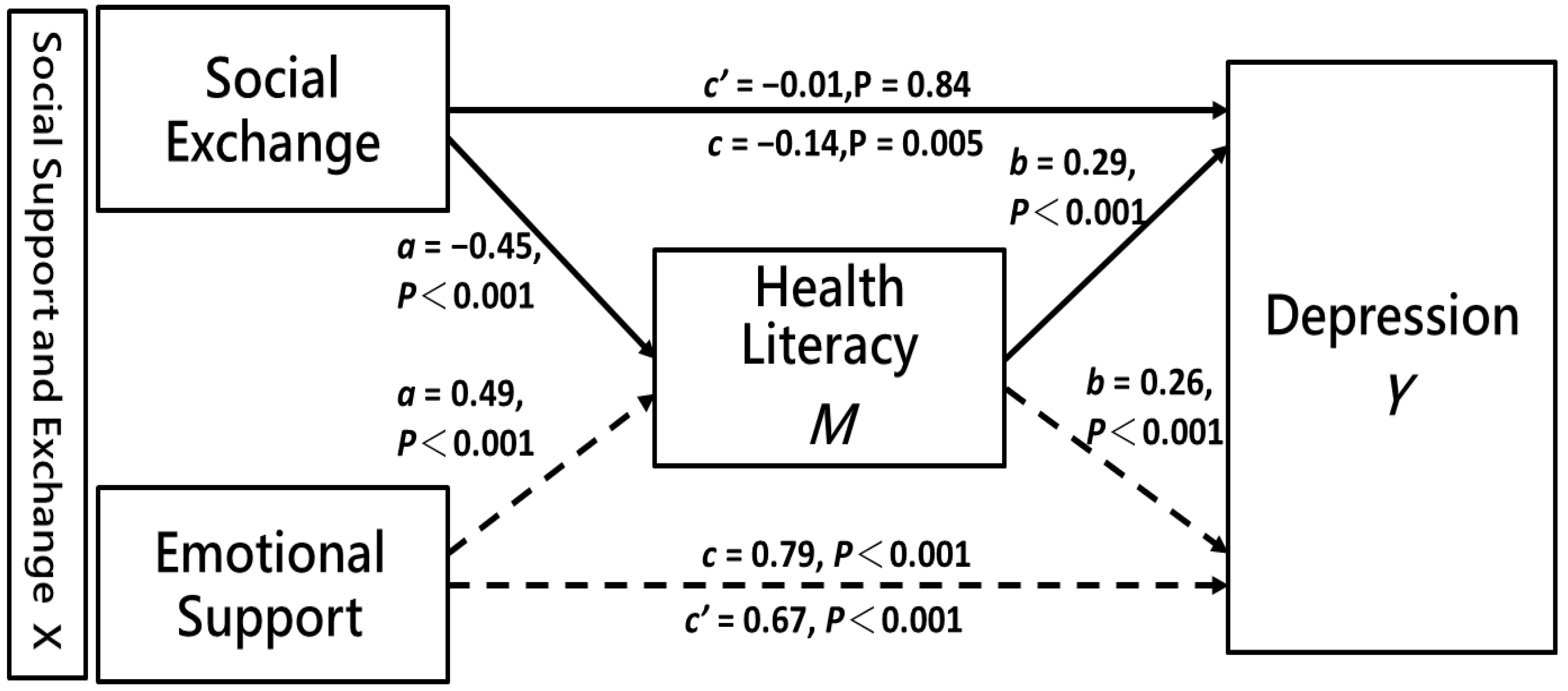
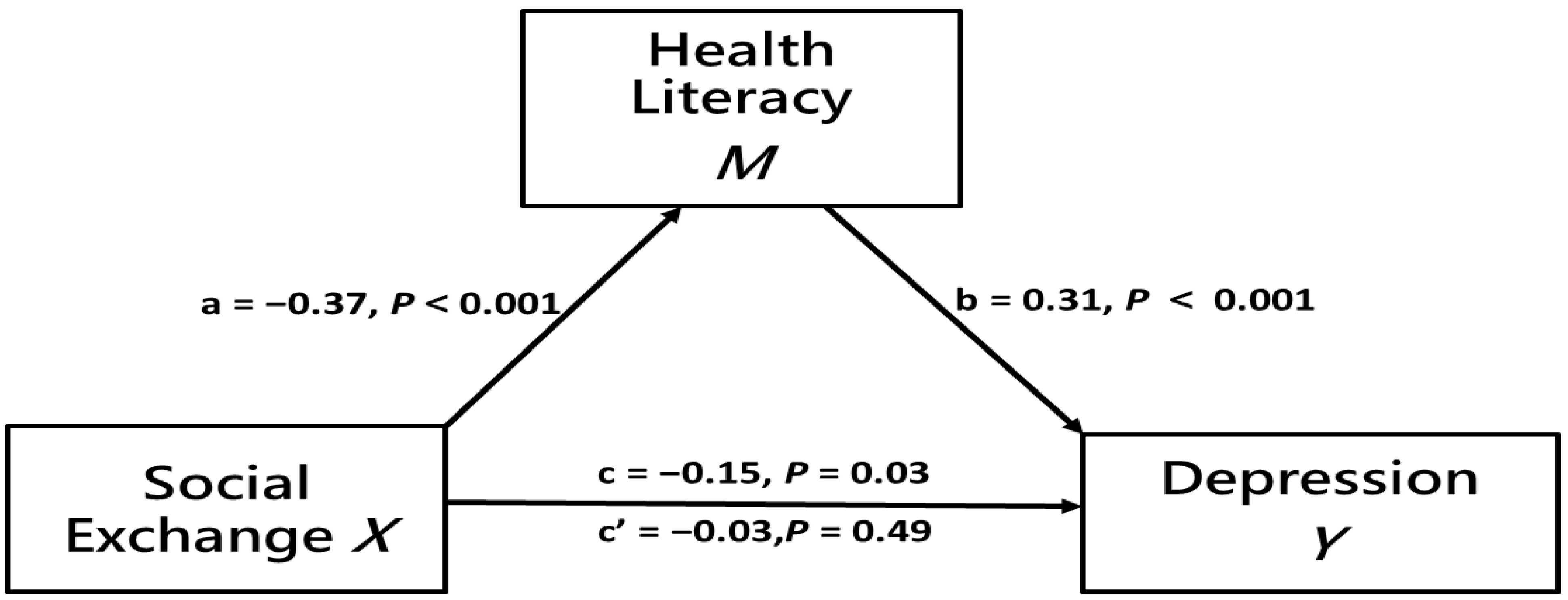
3.3. The Mediation Effect of Health Literacy
4. Discussion
4.1. Health Literacy Status Positively Correlates with Social Support with Exchange, but Is Inversely Associated with Depression
4.2. Components of Social Support with Exchange Differentially Affect Depression
4.3. Social Support with Exchange Reflects Health Literacy Status
4.4. Inadequate Health Literacy Is Implicated in Mental Health Deterioration and Depression
4.5. Health Literacy Significantly Mediates the Relationship between Social Support with Exchange and Depression
4.6. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the global burden of disease study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.S.; Lin, J.P. Depression in middle aged and older adults: A multilevel method study. J. Hum. Dev. Fam. Stud. 2019, 20, 1–23. [Google Scholar]
- World Health Organization. Mental Health of Older Adults. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults (accessed on 3 May 2021).
- Barua, A.; Ghosh, M.K.; Kar, N.; Basilio, M.A. Prevalence of depressive disorders in the elderly. Ann. Saudi Med. 2011, 31, 620–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soysal, P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Solmi, M.; Schofield, P.; Koyanagi, A.; Tseng, P.T.; et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 36, 78–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health and Welfare (Taiwan). 2019 Cause of Death Statistics. Available online: https://www.mohw.gov.tw/lp-4964-2.html (accessed on 3 May 2021).
- Cheng, W.S.; Hwang, T.J.; Lee, M.B.; Liao, S.C. Assessment and management of geriatric depression and suicide. Taiwan Geriatr. Gerontol. 2016, 11, 16–30. [Google Scholar]
- Schwarzbach, M.; Luppa, M.; Forstmeier, S.; König, H.H.; Riedel-Heller, S.G. Social relations and depression in late life—A systematic review. Int. J. Geriatr. Psychiatry 2014, 29, 1–21. [Google Scholar] [CrossRef]
- Gazmararian, J.; Baker, D.; Parker, R.; Blazer, D.G. A multivariate analysis of factors associated with depression: Evaluating the role of health literacy as a potential contributor. Arch. Intern. Med. 2000, 160, 3307–3314. [Google Scholar] [CrossRef]
- Hsu, Y.L.; Su, D.H.; Kuo, S.C. Health literacy and depression in women with type 2 diabetes mellitus. Clinics 2020, 75, e1436. [Google Scholar] [CrossRef]
- Lee, C.-T.; Yeh, C.-J.; Lee, M.-C.; Lin, H.-S.; Chen, V.C.-H.; Hsieh, M.-H.; Yen, C.-H.; Lai, T.-J. Leisure activity, mobility limitation and stress as modifiable risk factors for depressive symptoms in the elderly: Results of a national longitudinal study. Arch. Gerontol. Geriatr. 2012, 54, e221–e229. [Google Scholar] [CrossRef]
- Wang, J.L. The Related Influencing Factors for the Middle-Aged and the Elders Depression-Dynamic Analysis. (Unpublished Master’s Thesis), Department of Healthcare Administration, Asia University, Taichung, Taiwan, 2008. [Google Scholar]
- Rajapakshe, O.B.; Sivayogan, S.; Kulatunga, P.M. Prevalence and correlates of depression among older urban community-dwelling adults in Sri Lanka. Psychogeriatrics 2019, 19, 202–211. [Google Scholar] [CrossRef]
- Sharma, D.; Singh, U. Epidemiological determinants of mental status differences in geriatric population in rural and urban area in anand, gujarat. Int. J. Med. Sci. Public Health 2016, 5, 2536. [Google Scholar] [CrossRef]
- Zou, H.; Chen, Y.; Fang, W.; Zhang, Y.; Fan, X. The mediation effect of health literacy between subjective social status and depressive symptoms in patients with heart failure. J. Psychosom. Res. 2016, 91, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Patra, P.; Alikari, V.; Fradelos, E.C.; Sachlas, A.; Kourakos, M.; Rojas Gil, A.P.; Babatsikou, F.; Zyga, S. Assessment of depression in elderly. Is perceived social support related? A nursing home study: Depression and social support in elderly. Adv. Exp. Med. Biol. 2017, 987, 139–150. [Google Scholar]
- Tengku Mohd, T.A.M.; Yunus, R.M.; Hairi, F.; Hairi, N.N.; Choo, W.Y. Social support and depression among community dwelling older adults in Asia: A systematic review. BMJ Open 2019, 9, e026667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, L.; Argyle, M. Receiving and giving support: Effects on relationships and well-being. Couns. Psychol. Q. 1992, 5, 123–133. [Google Scholar] [CrossRef]
- Hays, J.C.; Landerman, L.R.; George, L.K.; Flint, E.P.; Koenig, H.G.; Land, K.C.; Blazer, D.G. Social correlates of the dimensions of depression in the elderly. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53, P31–P39. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.-C.; Li, C.-R.; Lo, C.; Chiao, C.-Y.; Hsiao, C.-Y.; Wu, H.-S.; Lee, M.-C.; Liao, W.-C. Effect of social support on changes in instrumental activities of daily living in older adults: A national population-based longitudinal study. Int. J. Gerontol. 2019, 13, 17–22. [Google Scholar] [CrossRef]
- Brown, S.L.; Nesse, R.M.; Vinokur, A.D.; Smith, D.M. Providing social support may be more beneficial than receiving it: Results from a prospective study of mortality. Psychol. Sci. 2003, 14, 320–327. [Google Scholar] [CrossRef] [PubMed]
- McGee, H.M.; Molloy, G.; O’Hanlon, A.; Layte, R.; Hickey, A. Older people–recipients but also providers of informal care: An analysis among community samples in the Republic of Ireland and Northern Ireland. Health Soc. Care Community 2008, 16, 548–553. [Google Scholar] [CrossRef]
- Shih, Y.L.; Hsieh, C.J. Concept analysis: Health literacy of the elderly. Taiwan Geriatr. Gerontol. 2021, in press. [Google Scholar]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Arafat, S.Y.; Majumder, M.A.A.; Kabir, R.; Papadopoulos, K.; Uddin, M.S. Health literacy in school. In Research Anthology on Mental Health Stigma, Education, and Treatment; IGI Global: Hershey PA, USA, 2021; pp. 920–942. [Google Scholar]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Viera, A.; Crotty, K.; Holland, A.; Brasure, M.; Lohr, K.N.; Harden, E. Health literacy interventions and outcomes: An updated systematic review. Evid. Rep./Technol. Assess. (Full Rep.) 2011, 199, 941. [Google Scholar]
- DeWalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Meng, H.; Tu, N.; Liu, D. The relationship between health literacy, social support, depression, and frailty among community-dwelling older patients with hypertension and diabetes in China. Front. Public Health 2020, 8, 280. [Google Scholar] [CrossRef]
- Coffman, M.J.; Norton, C.K. Demands of immigration, health literacy, and depression in recent latino immigrants. Home Health Care Manag. Pract. 2010, 22, 116–122. [Google Scholar] [CrossRef]
- Lincoln, A.; Paasche-Orlow, M.K.; Cheng, D.M.; Lloyd-Travaglini, C.; Caruso, C.; Saitz, R.; Samet, J.H. Impact of health literacy on depressive symptoms and mental health-related: Quality of life among adults with addiction. J. Gen. Intern. Med. 2006, 21, 818–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, T.G.; Lee, H.Y.; Kim, N.K.; Han, G.; Lee, J.; Kim, K. Is health literacy associated with depressive symptoms among korean adults? Implications for mental health nursing. Perspect. Psychiatr. Care 2017, 53, 234–242. [Google Scholar] [CrossRef]
- Zhang, B.; Zhang, W.; Sun, X.; Ge, J.; Liu, D. Physical comorbidity and health literacy mediate the relationship between social support and depression among patients with hypertension. Front. Public Health 2020, 8, 304. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Health Promotion Administration (Taiwan). 2015 Taiwan Longitudinal Study on Aging Survey Report; Taiwan Aging Study Series; Health Promotion Administration: Taipei, Taiwan, 2018; pp. 1–258. [Google Scholar]
- Lin, Y.H.; Chen, Y.C.; Tseng, Y.C.; Tsai, S.T.; Tseng, Y.H. Physical activity and successful aging among middle-aged and older adults: A systematic review and meta-analysis of cohort studies. Aging 2020, 12, 7704–7716. [Google Scholar] [CrossRef]
- Xu, L.; Wang, X.; Pan, X.; Wang, X.; Wang, Q.; Wu, B.; Cai, J.; Zhao, Y.; Chen, L.; Li, W.; et al. Education level as a predictor of survival in patients with multiple myeloma. BMC Cancer 2020, 20, 737. [Google Scholar] [CrossRef]
- Health Promotion Administration, Ministry of Health and Welfare. Taiwan Longitudinal Study on Aging (TLSA). Available online: https://www.hpa.gov.tw/EngPages/Detail.aspx?nodeid=1077&pid=6197 (accessed on 12 October 2021).
- Shih, Y.-L.; Hsieh, C.-J.; Li, P.-S.; Liu, C.-Y. Psychometric properties of the health literacy scale used in the Taiwan longitudinal study on middle-aged and older people. Healthcare 2021, 9, 1391. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Kohout, F.J.; Berkman, L.F.; Evans, D.A.; Cornoni-Huntley, J. Two shorter forms of the CES-D depression symptoms index. J. Aging Health 1993, 5, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. The Process Macro for Spss and Sas. Available online: https://afhayes.com/index.html (accessed on 29 June 2021).
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Hayes, A.F.; Preacher, K.J. Statistical mediation analysis with a multicategorical independent variable. Br. J. Math. Stat. Psychol. 2014, 67, 451–470. [Google Scholar] [CrossRef]
- Lin, H.W.; Yang, P.J.; Yang, Y.S.; Chen, C.C.; Chen, S.C.; Yen, C.H.; Lai, T.J.; Lee, M.C. Predictive factors of geriatric depression in Taiwan: A ten-year longitudinal study. Taiwan Geriatr. Gerontol. 2010, 5, 257–265. [Google Scholar]
- Assariparambil, A.R.; Noronha, J.A.; Kamath, A.; Adhikari, P.; Nayak, B.S.; Shankar, R.; George, A. Depression among older adults: A systematic review of South Asian countries. Psychogeriatrics 2021, 21, 201–219. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Yang, F.M. Insomnia symptoms predict both future hypertension and depression. Prev. Med. 2019, 123, 41–47. [Google Scholar] [CrossRef]
- Charoensakulchai, S.; Usawachoke, S.; Kongbangpor, W.; Thanavirun, P.; Mitsiriswat, A.; Pinijnai, O.; Kaensingh, S.; Chaiyakham, N.; Chamnanmont, C.; Ninnakala, N.; et al. Prevalence and associated factors influencing depression in older adults living in rural Thailand: A cross-sectional study. Geriatr. Gerontol. Int. 2019, 19, 1248–1253. [Google Scholar] [CrossRef] [PubMed]
- Conde-Sala, J.L.; Garre-Olmo, J.; Calvó-Perxas, L.; Turró-Garriga, O.; Vilalta-Franch, J. Course of depressive symptoms and associated factors in people aged 65+ in Europe: A two-year follow-up. J. Affect. Disord. 2019, 245, 440–450. [Google Scholar] [CrossRef] [Green Version]
- Grover, S.; Malhotra, N. Depression in elderly: A review of Indian research. J. Geriatr. Ment. Health 2015, 2, 4. [Google Scholar] [CrossRef]
- Portellano-Ortiz, C.; Garre-Olmo, J.; Calvó-Perxas, L.; Conde-Sala, J.L. Factor structure of depressive symptoms using the euro-d scale in the over-50s in europe. Findings from the share project. Aging Ment. Health 2018, 22, 1477–1485. [Google Scholar] [CrossRef]
- Robb, C.E.; de Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H. Associations of social isolation with anxiety and depression during the early COVID-19 pandemic: A survey of older adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef]
- Ylli, A.; Miszkurka, M.; Phillips, S.P.; Guralnik, J.; Deshpande, N.; Zunzunegui, M.V. Clinically relevant depression in old age: An international study with populations from Canada, Latin America and Eastern Europe. Psychiatry Res. 2016, 241, 236–241. [Google Scholar] [PubMed]
- Richardson, R.A.; Keyes, K.M.; Medina, J.T.; Calvo, E. Sociodemographic inequalities in depression among older adults: Cross-sectional evidence from 18 countries. Lancet Psychiatry 2020, 7, 673–681. [Google Scholar] [CrossRef]
- Eronen, J.; Paakkari, L.; Portegijs, E.; Saajanaho, M.; Rantanen, T. Assessment of health literacy among older Finns. Aging Clin. Exp. Res. 2019, 31, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protheroe, J.; Whittle, R.; Bartlam, B.; Estacio, E.V.; Clark, L.; Kurth, J. Health literacy, associated lifestyle and demographic factors in adult population of an English city: A cross-sectional survey. Health Expect. 2017, 20, 112–119. [Google Scholar] [CrossRef]
- Lee, S.Y.D.; Arozullah, A.M.; Cho, Y.I.; Crittenden, K.; Vicencio, D. Health literacy, social support, and health status among older adults. Educ. Gerontol. 2009, 35, 191–201. [Google Scholar] [CrossRef]
- National Health Research Institutes Forum. The Determinates of Health Literacy and Related Health Outcomes among Elders in Taiwan; National Health Research Institutes Ministry of Health and Welfare: Miaoli County, Taiwan, 2019; pp. 1–195. [Google Scholar]
- Vogt, D.; Schaeffer, D.; Messer, M.; Berens, E.-M.; Hurrelmann, K. Health literacy in old age: Results of a German cross-sectional study. Health Promot. Int. 2018, 33, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, H.; Demirci, H. Health literacy among older persons in Turkey. Aging Male 2019, 22, 272–277. [Google Scholar] [CrossRef]
- Lee, C.-F.; Tang, S.-M. The effects of intergenerational supports on the happiness for the people aged over 55 in Taiwan. Taiwan J. Gerontol. Health Res. 2016, 12, 121–138. [Google Scholar]
- Chen, E.; Lam, P.H.; Finegood, E.D.; Turiano, N.A.; Mroczek, D.K.; Miller, G.E. The balance of giving versus receiving social support and all-cause mortality in a US national sample. Proc. Natl. Acad. Sci. USA 2021, 118, e2024770118. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Xi, J.; Hall, B.J.; Fu, M.; Zhang, B.; Guo, J.; Feng, X. Attitudes toward aging, social support and depression among older adults: Difference by urban and rural areas in china. J. Affect. Disord. 2020, 274, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.H.; Juan, C.W. Instrumental and psychological social support of depression tendency among the middle aged and elderly in Taiwan. Hungkuang Academic Review. 2019, 84, 1–20. [Google Scholar]
- Gyasi, R.M.; Phillips, D.R.; Abass, K. Social support networks and psychological wellbeing in community-dwelling older Ghanaian cohorts. Int. Psychogeriatr. 2019, 31, 1047–1057. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.D.; Arozullah, A.M.; Cho, Y.I. Health literacy, social support, and health: A research agenda. Soc. Sci. Med. 2004, 58, 1309–1321. [Google Scholar] [CrossRef]
- Liu, Y.B.; Hou, P.; Xue, H.-P.; Mao, X.-E.; Li, Y.-N. Social support, health literacy, and health care utilization among older adults. Asia Pac. J. Public Health 2019, 31, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Sagong, H.; Yoon, J.Y. Pathways among frailty, health literacy, acculturation, and social support of middle-aged and older Korean immigrants in the USA. Int. J. Environ. Res. Public Health 2021, 18, 1245. [Google Scholar] [CrossRef] [PubMed]
- De Wit, L.; Fenenga, C.; Giammarchi, C.; Di Furia, L.; Hutter, I.; de Winter, A.; Meijering, L. Community-based initiatives improving critical health literacy: A systematic review and meta-synthesis of qualitative evidence. BMC Public Health 2018, 18, 40. [Google Scholar] [CrossRef] [Green Version]
- Do, B.N.; Nguyen, P.A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of health literacy and its associations with health-related behaviors, depression among the older people with and without suspected COVID-19 symptoms: A multi-institutional study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.S.; Parker, R.M.; Nurss, J.R.; Baker, D.W.; Williams, M.V. Shame and health literacy: The unspoken connection. Patient Educ. Couns. 1996, 27, 33–39. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-MentalHealth-2020.1 (accessed on 12 October 2021).
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V. People with suspected COVID-19 symptoms were more likely depressed and had lower health-related quality of life: The potential benefit of health literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duong, V.T.; Lin, I.-F.; Sorensen, K.; Pelikan, J.M.; Van den Broucke, S.; Lin, Y.-C.; Chang, P.W. Health literacy in Taiwan: A population-based study. Asia Pac. J. Public Health 2015, 27, 871–880. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Depression Status | p | ||||
|---|---|---|---|---|---|---|---|
| Non-Depression | Depression | ||||||
| n (mean) | % (S.D) | n (mean) | % (S.D) | n (mean) | % (S.D) | ||
| Age | 7636 | 6155 | 80.60 | 1481 | 19.40 | <0.001 | |
| 50–64 | 3633 | 47.60 | 3097 | 50.30 | 536 | 36.20 | |
| 65–85+ | 4003 | 52.40 | 3058 | 49.70 | 945 | 63.80 | |
| Gender | 7636 | 6155 | 80.60 | 1481 | 19.40 | <0.001 | |
| Male | 3719 | 48.70 | 3146 | 51.10 | 573 | 38.70 | |
| Female | 3917 | 51.30 | 3009 | 48.90 | 908 | 61.30 | |
| Education level | 7636 | 6155 | 80.60 | 1481 | 19.40 | <0.001 | |
| Junior high school or below | 5112 | 66.90 | 3946 | 64.10 | 1166 | 78.70 | |
| Senior high school or or above | 2524 | 33.10 | 2209 | 35.90 | 315 | 21.30 | |
| Social support with exchange | |||||||
| Social exchange | (2.03) | (0.01) | (2.23) | (0.73) | (2.02) | (0.85) | <0.001 |
| Emotional support | (7.33) | (2.55) | (6.96) | (2.24) | (8.82) | (3.13) | <0.001 |
| Health literacy | (15.12) | (5.92) | (14.27) | (0.05) | (18.57) | (6.71) | <0.001 |
| Social Exchange | Emotional Support | Health Literacy | Depression | |
|---|---|---|---|---|
| Social exchange | ||||
| Emotional support | −0.239 ** | |||
| Health literacy | −0.102 ** | 0.212 ** | ||
| depression | −0.145 ** | 0.377 ** | 0.354 ** |
| Independent Variable | Mediator | Dependent Variables | Effect of X on M | Effect of M on Y | Direct Effect | Indirect Effect | Total Effect | |
|---|---|---|---|---|---|---|---|---|
| X | M | Y | a | b | c′ | (a × b) 95% CI | c = c′ + a × b | |
| Model 1 | Social Exchange | Health Literacy | Depression | −0.45 | 0.29 | −0.01 | −0.13 | −0.14 |
| (SE = 0.06) *** | (SE = 0.01) *** | (SE = 0.05) | (−0.17~−0.10) | (SE = 0.05) ** | ||||
| Emotional Support | 0.49 | 0.26 | 0.67 | 0.13 | 0.79 | |||
| (SE = 0.03) *** | (SE = 0.01) *** | (SE = 0.02) *** | (0.11~0.15) | (SE = 0.02) *** | ||||
| Model 2 | Social Exchange | Health Literacy | Depression | −0.37 | 0.31 | −0.03 | −0.11 | −0.15 |
| (SE = 0.05) *** | (SE = 0.01) *** | (SE = 0.05) | (−0.14 −0.09) | (SE = 0.05) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, Y.-L.; Hsieh, C.-J.; Lin, Y.-T.; Wang, Y.-Z.; Liu, C.-Y. The Mediation Effect of Health Literacy on Social Support with Exchange and Depression in Community-Dwelling Middle-Aged and Older People in Taiwan. Healthcare 2021, 9, 1757. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121757
Shih Y-L, Hsieh C-J, Lin Y-T, Wang Y-Z, Liu C-Y. The Mediation Effect of Health Literacy on Social Support with Exchange and Depression in Community-Dwelling Middle-Aged and Older People in Taiwan. Healthcare. 2021; 9(12):1757. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121757
Chicago/Turabian StyleShih, Ya-Ling, Chia-Jung Hsieh, Ya-Ting Lin, Yi-Zhu Wang, and Chieh-Yu Liu. 2021. "The Mediation Effect of Health Literacy on Social Support with Exchange and Depression in Community-Dwelling Middle-Aged and Older People in Taiwan" Healthcare 9, no. 12: 1757. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121757