
Diffusion-Weighted MRI—The Way Forward for MRI in Myeloma?


1
Department of Medicine, Roswell Park Comprehensive Cancer Center, Buffalo, NY 14263, USA
2
Department of Hematology, Cell Therapy and Hemostaseology, University Hospital of Leipzig, 04103 Leipzig, Germany
3
Department of Diagnostic Radiology, Roswell Park Comprehensive Cancer Center, Buffalo, NY 14263, USA
4
Department of Radiology, Musculoskeletal Imaging and Intervention, University of Washington, Seattle, WA 98105, USA
*
Author to whom correspondence should be addressed.
Hemato 2021, 2(4), 672-679; https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040044
Submission received: 8 October 2021
/
Revised: 2 November 2021
/
Accepted: 9 November 2021
/
Published: 12 November 2021
(This article belongs to the Special Issue Current and Upcoming Diagnostics and Prognostics in Multiple Myeloma)
{kind=link}
{kind=link}
Abstract
:Multiple myeloma and other plasma cell disorders infiltrate the bone marrow in different patterns. While some patients show a homogeneous distribution of the clonal plasma cells others present with focal accumulations, commonly called focal lesions. Novel imaging techniques can provide information on these infiltration patterns and, due to their low invasiveness, can be performed repeatedly and therefore be used for monitoring. Conventional magnetic resonance imaging (MRI) has a high sensitivity for bone marrow assessment but cannot safely differentiate between active and inactive lesions. Therefore, positron emission tomography, especially combined with computed tomography (PET/CT), has been more widely used, at least for the monitoring of treatment response. Comparative, but mostly retrospective studies, have shown that functional MRI techniques, namely diffusion-weighted imaging (DWI), which assesses the movement of water molecules, can evaluate tissue cellularity with high sensitivity, which challenges the dominance of PET/CT in treatment response assessment. This review will discuss the benefits and challenges of DWI and compare it to other available imaging techniques used in patients with monoclonal plasma cell disorders.
1. Monoclonal Plasma Cell Disorders
Multiple myeloma (MM) is a malignant manifestation of a group of disorders characterized by the infiltration and proliferation of clonal plasma cells, mainly in the bone marrow [1]. It is persistently preceded by the precancerous stage of monoclonal gammopathy of undetermined significance (MGUS), and by an intermediate stage of smoldering multiple myeloma (SMM) [2]. While, in general, individuals with MGUS have a risk of progression into symptomatic disease of between 7% and 30% in 20 years [3], patients with SMM show a time to progression of between 2 and 10 years [4]. Both MGUS and SMM are defined by a lack of clinical symptoms. Typical manifestations of MM are elevated serum calcium levels, renal insufficiency, anemia and bone disease, summarized as the so called “CRAB” criteria [5]. Osteolytic lesions and hypercalcemia are caused by an over-activation of osteoclasts by the malignant plasma cells. While high calcium levels are rather rare at first diagnosis, about 80% of patients show some form of bone disease at initial presentation [6]. Osteolytic lesions can lead to fractures which have a significant impact on the quality of life of patients. Predicting and preventing bone destruction has a high priority in the care of myeloma patients. Retrospective analyses of osteolytic lesions in imaging have revealed that they appear to be preceded by focal lesions which can be detected by MRI, as well as by PET [7,8].
2. Imaging in Monoclonal Plasma Cell Disorders
The technique initially used to identify myeloma bone disease was conventional skeletal survey. However, comparative studies have shown that this modality misses bone destruction in about 25% of patients compared to CT [9]. Therefore, whole body low dose CT is the current standard imaging modality for screening in patients with suspicion of multiple myeloma [10]. While CT has the highest sensitivity for the detection of changes in the mineralized bone, its sensitivity for detection of bone marrow infiltration is limited, especially in areas with cancellous bone because of the high radio density of bone compared to the bone marrow. Therefore, imaging techniques with higher contrast for soft tissue allow for the detection of bone marrow changes even before bone destruction has occurred. MRI has multiple advantages over PET/CT, including no radiation exposure, no pre-examination nutrition requirements, and no reliance on tumoral cell metabolism.
2.1. MRI in Myeloma
MRI has been used in multiple myeloma for many years due to its sensitivity for detecting compression fractures, spinal cord impairment, bone marrow composition, and bone marrow edema, without the need for ionizing radiation or potentially nephrotoxic, iodine-based, contrast agents [11]. It has the advantage of visualizing bone, bone marrow, and extra-osseous soft-tissue abnormalities. Advances in MRI acquisition techniques have allowed for whole-body screening studies to be acquired in a reasonable time frame and with acceptable resolution, thereby increasing the ability of patients to cooperate [12]. MRI could also evaluate the chronicity of fractures and distinguish pathologic from insufficiency fractures [13]. State-of-the-art MRI sequences, such as diffusion-weighted imaging (DWI), could also assess response to treatment more accurately.
2.2. Early Detection
In the early stages of monoclonal plasma cell disorders, MRI and PET have been shown to be able to detect changes in the bone marrow in the absence of osteolytic lesions or osteoporosis caused by myeloma [7,8,14]. A comparison of PET and MRI, specifically in these patient groups, is currently missing to the best of our knowledge. Follow up examinations of patients with SMM have shown that not only the presence, but also the development and growth, of focal lesions on MRI are associated with an adverse prognosis [15]. Using MRI frequently in smoldering myeloma patients can even prevent the development of end organ damage in some, but not all, patients. A recent prospective study by our group has shown that of 96 evaluable patients with SMM (according to the 2014 IMWG guidelines), 22 progressed into myeloma during the observation period and 15 (68%) of them developed end organ damage [16]. With its high sensitivity and the lack of radiation exposure, MRI is particularly valuable as a screening tool in patients with early stages of monoclonal gammopathies (Figure 1). However, limitations such as availability and costs have led to the recommendation to use MRI as a second, rather than first line screening tool [10].
2.3. Treatment Monitoring
Aside from the early detection of disease and prevention of complications, treatment monitoring is another area where imaging is being deployed in patients with monoclonal plasma cell disorders. Publications from the University of Arkansas reported that residual lesions on PET/CT, after induction treatment, and after high dose chemotherapy with autologous stem cell transplantation, are associated with an adverse prognosis [17,18]. In fact, the presence of more than three residual focal lesions after induction and any residual focal lesions after high dose chemotherapy were significantly adverse prognostic factors. The same group was also able to show that residual lesions on conventional MRI are a negative prognostic factor, which was confirmed by other research groups, and in patients after allogeneic stem cell transplantation [19,20]. However, a comparison of whole body PET/CT and conventional spinal MRI, the latter limited due to availability of whole body MRI, by the Intergroupe Francophone du Myélome, showed that PET/CT more reliably predicted outcomes [21]. This is most likely explained because it can show metabolic activity while conventional MRI shows morphological features only. With regard to residual lesions on MRI, it has been shown that these lesions take a longer time to resolve, possibly because even necrotic tissue can still be present inside osteolytic lesions for several months [18]. But there are other interesting features when it comes to residual lesions on MRI. A retrospective analysis of patients treated in the German-speaking myeloma multicenter group MM5 trial revealed that patients who had cystic transformation of their lesions had a worse prognosis and showed a higher proliferation index in gene expression profiling of their myeloma cells [22]. While the exact histologic correlate of these cystic lesions is unclear at this time, MRI and DWI are the only imaging techniques currently used in myeloma that can provide this information about lesions responding to treatment.
Whole-body DWI, which has become more and more available in larger centers, can improve some of the shortcomings of conventional MRI mentioned above. While direct comparisons of conventional MRI and DWI in myeloma patients are lacking, a whole-body scan will have a more comprehensive field of view than axial MRI alone. Furthermore, the higher sensitivity and specificity of DWI for the assessment of cellularity in the examined tissue is expected to improve the accuracy of assessment of residual focal lesions after therapy (Figure 2).
3. General Application of DWI MRI
DWI is an MRI technique that is sensitive to random water movements at spatial scales at a sub-millimeter range. Normally, water molecules move freely in a large extracellular space relatively unimpeded. The movement of extracellular water depends upon a combination of factors including Brownian motion, hydrostatic pressure gradients, and active transport. The motion of water molecules is more restricted in tissues with a high cellular density associated with numerous intact cell membranes (e.g., tumor tissue). The lipophilic cell membranes act as barriers to the motion of water molecules in both the extracellular and intracellular spaces. By contrast, in areas of low cellularity or where the cellular membrane has been breached, the motion of water molecules is less restricted [23]. DWI is very sensitive to the disturbance in the flow of extracellular water that may occur due to a narrowing of extracellular space by cellular edema (from ischemia or other injury to cells) or due to hypercellularity.
While application of DWI had for many years been restricted to brain imaging (particularly for investigation of stroke), because of its inherent sensitivity to motion [24], the introduction of echoplanar imaging, and the use of fast acquisition techniques capable of imaging during a single breath hold, DWI has found diagnostic applications in imaging of other parts of the body including whole-body MRI analysis in myeloma patients [25].
4. DWI in Myeloma
The development of functional MRI sequences such as DWI have revolutionized the assessment of myeloma lesions from purely anatomic assessment based on size, to quantitative assessment based on tissue cellularity and free water molecule movements. Quantitative imaging with DWI and apparent diffusion coefficient (ADC) maps have been used for diagnosis, staging, and the assessment of treatment response and disease activity in myeloma patients, with promising results.
Analyses correlating findings of DWI and histology from bone marrow biopsies of the pelvis have shown a positive correlation between ADC and bone marrow cellularity and micro-vessel density [26]. However, application of intravoxel incoherent motion imaging (IVIM) revealed that DWI parameters are not only dependent on cellularity but also vascularity, which is an important factor in the pathophysiology of bone marrow infiltration of myeloma as well [27].
DWI provides high contrast between normal and replaced marrow with the opportunity to assess lesions quantitatively based on ADC maps. This is particularly important for treatment response assessment in patients with myeloma. DWI has higher lesion conspicuity compared to conventional MRI with T1-weighted and STIR sequence, and a higher lesion detection rate compared to PET/CT [28]. WB MRI with DWI has been used for the staging of myeloma and has demonstrated superiority compared with radiographic skeletal survey, PET/CT, and conventional MRI, which has a substantial impact on treatment planning [29,30,31].
WB-MRI with DWI provides the opportunity for the quantitative analysis of the entire bone marrow after treatment. DWI is more sensitive for treatment response assessment compared with anatomic MRI sequences, which is mainly size-based assessment [26,32]. Effective treatment results are intra-lesional hemorrhage, necrosis, and edema due to tumor cell death and vascular congestion. This results in changes in the signal fat fraction, which could be used as a surrogate marker for treatment response [33].
In addition, differentiation of benign tumors from pathologic vertebral compression fractures could more reliably be performed when quantitative diffusion measurements are available [13]. Thereby diagnosis is based on the contrast to normal bone marrow with a higher fat content, especially in the aging population who account for most myeloma patients. Hypo- or iso-intensity reflects acute benign collapse, whereas hyperintensity is indicative of the tumorous nature of a fracture. ADC values are significantly lower in metastatic disease than in bone marrow edema [34] and DWI could differentiate benign from malignant vertebral body collapse with a sensitivity and specificity of 95.6% and 90%, respectively [35].
To the best of our knowledge there are no prospective data available for the comparison of DWI and PET/CT. Two retrospective analyses suggest, however, that DWI has a higher sensitivity than PET/CT. In a study in a cohort of 227 patients from the University of Arkansas, 11% of patients were positive in DWI but negative in PET/CT. The authors attributed this, at least in part, to a lower expression of a gene coding for hexokinase-2 which is an important enzyme in glycolysis and therefore has an impact on glucose uptake in cells, which then influences the tracer uptake in FDG-PET/CT [28]. In a smaller study of 24 patients, DWI showed a sensitivity of 77% versus 47% in PET/CT compared to a combination of conventional MRI and CT [36].
5. Technical Considerations
There are some challenges to using MRI and whole body DWI effectively. DWI, as an echoplanar technique is very sensitive to distortion from the magnetic susceptibility artifact which is an artifact resulting from metal, hemorrhage, or any substance in the body, that results in local heterogeneity of the magnetic field. This artifact can make assessment of the marrow near surgical hardware or tissue/air interfaces challenging. Magnetic susceptibility artifacts result in distortions on DWI because it is an echoplanar sequence. These effects are less prominent with lower field strengths but must be balanced by the loss of signal and speed that can be achieved with high field strengths. Our experience suggests 1.5 T is a field strength that provides acceptable imaging speed and signal and fewer susceptibility artifacts than are seen at 3 T. Currently MRI systems cannot cover an entire body with a single scan. For whole-body imaging, multiple stations of image acquisition are needed, thereby requiring software to combine the segments into a full body image. Motion of the patient either on a gross or physiological scale between acquisitions can result in misregistration artifacts at the connection points of the segments, complicating image interpretation. Fortunately, continued improvement in MRI technology and image reconstruction, including the use of artificial intelligence to decrease image noise and artifacts, promises to reduce these challenges over time.
6. Limitations
Limitations of the use of DWI in patients with monoclonal plasma cell disorders are the combined effect of perfusion and cellularity on quantitative assessments which makes more sophisticated analyses necessary that might not be available in clinical routine [27]. Furthermore, the T2-shine-through effect, especially in cystic lesions with a high signal in DWI despite absent vital tumor cells, can be challenging and still make comparison with conventional sequences necessary. Currently, there are no guidelines for standardized quantification available to assess ADC values uniformly since this parameter depends on b-values which are part of the setting of the MRI scanner at image acquisition.
7. Future Directions
New developments in this field include especially the use of hybrid techniques combining PET and MRI with DWI. Since WB-MRI is the most sensitive technique for detecting myeloma lesions and staging the disease, adding functional information from DWI and PET could add value to treatment response evaluation. Therefore, whole-body PET/MRI could be a one-stop-shop examination, including the most sensitive technique for detecting bone marrow involvement, and the most recognized technique for treatment response evaluation.
Furthermore, imaging findings should be integrated into the assessment of minimal residual disease, and, eventually, imaging findings could help to guide therapy and identify patients who do not respond to a certain treatment early on.
8. Summary
MRI has the distinct advantage of avoiding the need for ionizing radiation and nephrotoxic contrast agents, and reliably detecting areas of hypercellularity with high sensitivity, especially when diffusion-weighted techniques are applied. Circumstances where this is of particular value include the early stages of monoclonal plasma cell disorders and the assessment of treatment response.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rajkumar, S.V.; Dimopoulos, M.A.; Palumbo, A.; Blade, J.; Merlini, G.; Mateos, M.-V.; Kumar, S.; Hillengass, J.; Kastritis, E.; Richardson, P.; et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014, 15, e538–e548. [Google Scholar] [CrossRef]
- Landgren, O.; Kyle, R.A.; Pfeiffer, R.M.; Katzmann, J.A.; Caporaso, N.E.; Hayes, R.B.; Dispenzieri, A.; Kumar, S.; Clark, R.J.; Baris, D.; et al. Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: A prospective study. Blood 2009, 113, 5412–5417. [Google Scholar] [CrossRef] [Green Version]
- Kyle, R.A.; Larson, D.R.; Therneau, T.M.; Dispenzieri, A.; Kumar, S.; Cerhan, J.R.; Rajkumar, S.V. Long-Term Follow-up of Monoclonal Gammopathy of Undetermined Significance. N. Engl. J. Med. 2018, 378, 241–249. [Google Scholar] [CrossRef]
- Lakshman, A.; Rajkumar, S.V.; Buadi, F.K.; Binder, M.; Gertz, M.A.; Lacy, M.Q.; Dispenzieri, A.; Dingli, D.; Fonder, A.L.; Hayman, S.R.; et al. Risk stratification of smoldering multiple myeloma incorporating revised IMWG diagnostic criteria. Blood Cancer J. 2018, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: A report of the International Myeloma Working Group. Br. J. Haematol. 2003, 121, 749–757. [Google Scholar] [CrossRef] [Green Version]
- Kyle, R.A.; Gertz, M.A.; Witzig, T.E.; Lust, J.A.; Lacy, M.Q.; Dispenzieri, A.; Fonseca, R.; Rajkumar, S.V.; Offord, J.R.; Larson, D.R.; et al. Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clin. Proc. 2003, 78, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Hillengass, J.; Fechtner, K.; Weber, M.-A.; Bäuerle, T.; Ayyaz, S.; Heiss, C.; Hielscher, T.; Moehler, T.M.; Egerer, G.; Neben, K.; et al. Prognostic significance of focal lesions in whole-body magnetic resonance imaging in patients with asymptomatic multiple myeloma. J. Clin. Oncol. 2010, 28, 1606–1610. [Google Scholar] [CrossRef] [PubMed]
- Zamagni, E.; Nanni, C.; Gay, F.; Pezzi, A.; Patriarca, F.; Bellò, M.; Rambaldi, I.; Tacchetti, P.; Hillengass, J.; Gamberi, B.; et al. 18F-FDG PET/CT focal, but not osteolytic, lesions predict the progression of smoldering myeloma to active disease. Leukemia 2016, 30, 417–422. [Google Scholar] [CrossRef]
- Hillengass, J.; Moulopoulos, L.A.; Delorme, S.; Koutoulidis, V.; Hielscher, T.; Engelhart, J.; Drake, M.; Rajkumar, S.V.; Oestergaard, B.; Abildgaard, N.; et al. Findings of Whole Body Computed Tomography Compared to Conventional Skeletal Survey in Patients with Monoclonal Plasma Cell Disorders––A Study of the International Myeloma Working Group. Blood 2016, 128, 4468. [Google Scholar] [CrossRef]
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.-V.; Lonial, S.; Joao, C.; Anderson, K.C.; García-Sanz, R.; Riva, E.; et al. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019, 20, e302–e312. [Google Scholar] [CrossRef]
- Ludwig, H.; Frühwald, F.; Tscholakoff, D.; Rasoul, S.; Neuhold, A.; Fritz, E. Magnetic resonance imaging of the spine in multiple myeloma. Lancet 1987, 2, 364–366. [Google Scholar] [CrossRef]
- Ghanem, N.; Lohrmann, C.; Engelhardt, M.; Pache, G.; Uhl, M.; Saueressig, U.; Kotter, E.; Langer, M. Whole-body MRI in the detection of bone marrow infiltration in patients with plasma cell neoplasms in comparison to the radiological skeletal survey. Eur. Radiol. 2006, 16, 1005–1014. [Google Scholar] [CrossRef]
- Baur, A.; Stäbler, A.; Brüning, R.; Bartl, R.; Krödel, A.; Reiser, M.; Deimling, M. Diffusion-weighted MR imaging of bone marrow: Differentiation of benign versus pathologic compression fractures. Radiology 1998, 207, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Moulopoulos, L.A.; Terpos, E.; Koutoulidis, V.; Dimopoulos, M.A. The prognostic importance of the presence of more than one focal lesion in spine MRI of patients with asymptomatic (smoldering) multiple myeloma. Leukemia 2014, 28, 2402–2403. [Google Scholar] [CrossRef]
- Merz, M.; Hielscher, T.; Wagner, B.; Sauer, S.; Shah, S.; Raab, M.S.; Jauch, A.; Neben, K.; Hose, D.; Egerer, G.; et al. Predictive value of longitudinal whole-body magnetic resonance imaging in patients with smoldering multiple myeloma. Leukemia 2014, 28, 1902–1908. [Google Scholar] [CrossRef] [PubMed]
- Hillengass, J. Frequent magnetic resonance imaging partially reduces the development of end organ damage in patients with smoldering myeloma. In Proceedings of the 18th International Myeloma Workshop Abstract Book, Vienna, Austria, 8–11 September 2021; p. 278. [Google Scholar]
- Usmani, S.Z.; Mitchell, A.; Waheed, S.; Crowley, J.; Hoering, A.; Petty, N.; Brown, T.; Bartel, T.; Anaissie, E.; van Rhee, F.; et al. Prognostic implications of serial 18-fluoro-deoxyglucose emission tomography in multiple myeloma treated with total therapy 3. Blood 2013, 121, 1819–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, T.B.; Haessler, J.; Brown, T.L.Y.; Shaughnessy, J.D.; Van Rhee, F.; Anaissie, E.; Alpe, T.; Angtuaco, E.; Walker, R.; Epstein, J.; et al. F18-fluorodeoxyglucose positron emission tomography in the context of other imaging techniques and prognostic factors in multiple myeloma. Blood 2009, 114, 2068–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillengass, J.; Ayyaz, S.; Kilk, K.; Weber, M.-A.; Hielscher, T.; Shah, R.; Delorme, S.; Goldschmidt, H.; Neben, K. Changes in magnetic resonance imaging before and after autologous stem cell transplantation correlate with response and survival in multiple myeloma. Haematologica 2012, 97, 1757–1760. [Google Scholar] [CrossRef]
- Mosebach, J.; Shah, S.; Delorme, S.; Hielscher, T.; Goldschmidt, H.; Schlemmer, H.-P.; Schönland, S.; Hegenbart, U.; Hegenbart, U. Prognostic significance of tumor burden assessed by whole-body magnetic resonance imaging in multiple myeloma patients treated with allogeneic stem cell transplantation. Haematologica 2017, 103, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, P.; Attal, M.; Caillot, D.; Macro, M.; Karlin, L.; Garderet, L.; Facon, T.; Benboubker, L.; Escoffre-Barbe, M.; Stoppa, A.M.; et al. Prospective Evaluation of Magnetic Resonance Imaging and [18F] Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients with Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J. Clin. Oncol. 2017, 35, 2911–2918. [Google Scholar]
- Merz, M.; Hielscher, T.; Mai, E.K.; Seckinger, A.; Hose, D.; Jauch, A.; Sauer, S.; Luntz, S.; Bertsch, U.; Raab, M.S.; et al. Cystic transformation of focal lesions after therapy is associated with remission but adverse outcome in myeloma. Blood Cancer J. 2019, 9, 71. [Google Scholar] [CrossRef] [Green Version]
- Koh, D.-M.; Collins, D.J. Diffusion-weighted MRI in the body: Applications and challenges in oncology. Am. J. Roentgenol. 2007, 188, 1622–1635. [Google Scholar] [CrossRef] [Green Version]
- Chalela, J.A.; Kidwell, C.S.; Nentwich, L.M.; Luby, M.; Butman, J.A.; Demchuk, A.M.; Hill, M.D.; Patronas, N.; Latour, L.; Warach, S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: A prospective comparison. Lancet 2007, 369, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Taouli, B.; Beer, A.J.; Chenevert, T.; Collins, D.; Lehman, C.; Matos, C.; Padhani, A.R.; Rosenkrantz, A.B.; Shukla-Dave, A.; Sigmund, E.; et al. Diffusion-weighted imaging outside the brain: Consensus statement from an ISMRM-sponsored workshop. J. Magn. Reason. Imaging. 2016, 44, 521–540. [Google Scholar] [CrossRef]
- Hillengass, J.; Bäuerle, T.; Bartl, R.; Andrulis, M.; McClanahan, F.; Laun, F.B.; Zechmann, C.M.; Shah, R.; Wagner-Gund, B.; Simon, D.; et al. Diffusion-weighted imaging for non-invasive and quantitative monitoring of bone marrow infiltration in patients with monoclonal plasma cell disease: A comparative study with histology. Br. J. Haematol. 2011, 153, 721–728. [Google Scholar] [CrossRef]
- Shah, R.; Stieltjes, B.; Andrulis, M.; Pfeiffer, R.; Sumkauskaite, M.; Delorme, S.; Schlemmer, H.P.; Goldschmidt, H.; Landgren, O.; Hillengass, J. Intravoxel incoherent motion imaging for assessment of bone marrow infiltration of monoclonal plasma cell diseases. Ann. Hematol. 2013, 92, 1553–1557. [Google Scholar] [CrossRef]
- Rasche, L.; Angtuaco, E.; McDonald, J.E.; Buros, A.; Stein, C.; Pawlyn, C.; Thanendrarajan, S.; Schinke, C.; Samant, R.; Yaccoby, S.; et al. Low expression of hexokinase-2 is associated with false-negative FDG-positron emission tomography in multiple myeloma. Blood 2017, 130, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Narquin, S.; Ingrand, P.; Azais, I.; Delwail, V.; Vialle, R.; Boucebci, S.; Tasu, J.P. Comparison of whole-body diffusion MRI and conventional radiological assessment in the staging of myeloma. Diagn. Interv. Imaging. 2013, 94, 629–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squillaci, E.; Bolacchi, F.; Altobelli, S.; Franceschini, L.; Bergamini, A.; Cantonetti, M.; Simonetti, G. Pre-treatment staging of multiple myeloma patients: Comparison of whole-body diffusion weighted imaging with whole-body T1-weighted contrast-enhanced imaging. Acta Radiol. 2015, 56, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giles, S.L.; Desouza, N.M.; Collins, D.J.; Morgan, V.A.; West, S.; Davies, F.E.; Morgan, G.J.; Messiou, C. Assessing myeloma bone disease with whole-body diffusion-weighted imaging: Comparison with x-ray skeletal survey by region and relationship with laboratory estimates of disease burden. Clin. Radiol. 2015, 70, 614–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutoulidis, V.; Fontara, S.; Terpos, E.; Zagouri, F.; Matsaridis, D.; Christoulas, D.; Panourgias, E.; Kastritis, E.; Dimopoulos, M.A.; Moulopoulos, L.A. Quantitative Diffusion-weighted Imaging of the Bone Marrow: An Adjunct Tool for the Diagnosis of a Diffuse MR Imaging Pattern in Patients with Multiple Myeloma. Radiology 2017, 282, 484–493. [Google Scholar] [CrossRef]
- Latifoltojar, A.; Hall-Craggs, M.; Rabin, N.; Popat, R.; Bainbridge, A.; Dikaios, N.; Sokolska, M.; Rismani, A.; D’Sa, S.; Punwani, S. Whole body magnetic resonance imaging in newly diagnosed multiple myeloma: Early changes in lesional signal fat fraction predict disease response. Br. J. Haematol. 2017, 176, 222–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.J.; Lee, S.Y.; Rho, M.H.; Chung, E.C.; Kim, M.S.; Kwon, H.J.; Youn, I.Y. Single-Shot Echo-Planar Diffusion-Weighted MR Imaging at 3T and 1.5T for Differentiation of Benign Vertebral Fracture Edema and Tumor Infiltration. Korean J. Radiol. 2016, 17, 590–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozzi, G.; Garcia Parra, C.; Stradiotti, P.; Tien, T.V.; Luzzati, A.; Zerbi, A. Diffusion-weighted MR imaging in differentiation between osteoporotic and neoplastic vertebral fractures. Eur. Spine J. 2012, 21 (Suppl. 1), 123–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachpekidis, C.; Mosebach, J.; Freitag, M.T.; Wilhelm, T.; Mai, E.K.; Goldschmidt, H.; Haberkorn, U.; Schlemmer, H.-P.; Delorme, S.; Dimitrakopoulou-Strauss, A. Application of (18)F-FDG PET and diffusion weighted imaging (DWI) in multiple myeloma: Comparison of functional imaging modalities. Am. J. Nucl. Med. Mol. Imaging 2015, 5, 479–492. [Google Scholar] [PubMed]
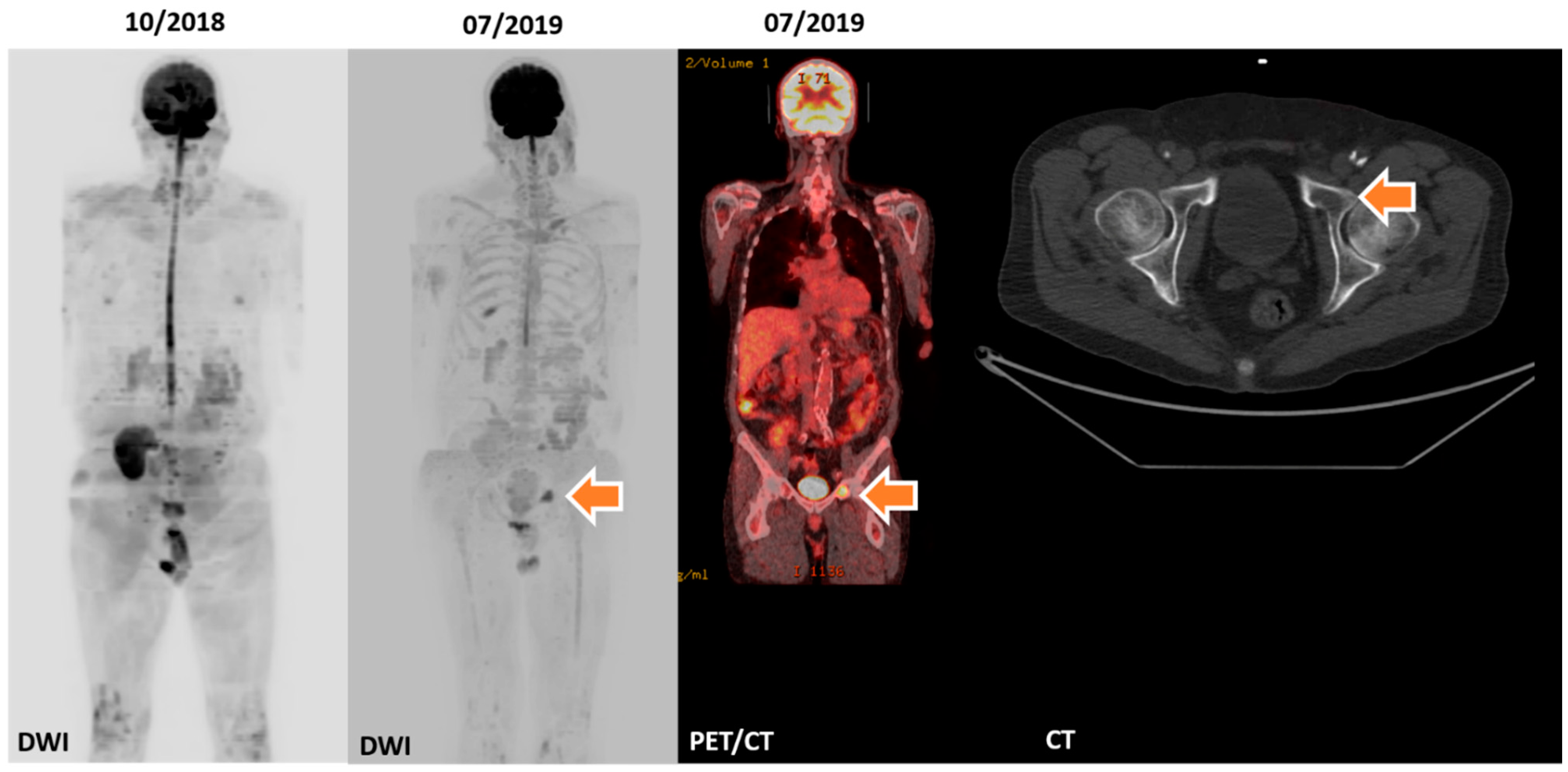
Figure 1.
Shows a patient with regular whole-body MRIs who developed a focal lesion in his pelvis. PET/CT performed at that time confirmed a metabolically active osteolytic lesion which led to the initiation of systemic anti-myeloma treatment.
Figure 1.
Shows a patient with regular whole-body MRIs who developed a focal lesion in his pelvis. PET/CT performed at that time confirmed a metabolically active osteolytic lesion which led to the initiation of systemic anti-myeloma treatment.

Figure 2.
Shows follow up examinations with DWI and PET/CT of a patient treated with standard induction treatment, followed by high dose chemotherapy and autologous stem cell transplantation and NK cell infusion, within the setting of a clinical trial. The patient responded well to this therapy, achieving minimal residual disease negativity with a corresponding normalization of the bone marrow signal in DWI.
Figure 2.
Shows follow up examinations with DWI and PET/CT of a patient treated with standard induction treatment, followed by high dose chemotherapy and autologous stem cell transplantation and NK cell infusion, within the setting of a clinical trial. The patient responded well to this therapy, achieving minimal residual disease negativity with a corresponding normalization of the bone marrow signal in DWI.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hillengass, J.; Merz, M.; Alberico, R.; Chalian, M. Diffusion-Weighted MRI—The Way Forward for MRI in Myeloma? Hemato 2021, 2, 672-679. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040044
AMA Style
Hillengass J, Merz M, Alberico R, Chalian M. Diffusion-Weighted MRI—The Way Forward for MRI in Myeloma? Hemato. 2021; 2(4):672-679. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040044
Chicago/Turabian StyleHillengass, Jens, Maximilian Merz, Ronald Alberico, and Majid Chalian. 2021. "Diffusion-Weighted MRI—The Way Forward for MRI in Myeloma?" Hemato 2, no. 4: 672-679. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2040044