Reducing Spread of Infections with a Photocatalytic Reactor—Potential Applications in Control of Hospital Staphylococcus aureus and Clostridioides difficile Infections and Inactivation of RNA Viruses


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Section
2.1. Assessment of the Effect of the Photocatalytic Reactor on S. aureus and C. difficile
2.2. Onsite Hospital Room Testing
2.3. Propagation of Viruses and Cell Culture
2.4. Viral Inactivation Assay
2.4.1. Inside a Biosafety Cabinet Experiment
2.4.2. Outside a Biosafety Cabinet Experiment
2.5. Data Analysis
3. Results
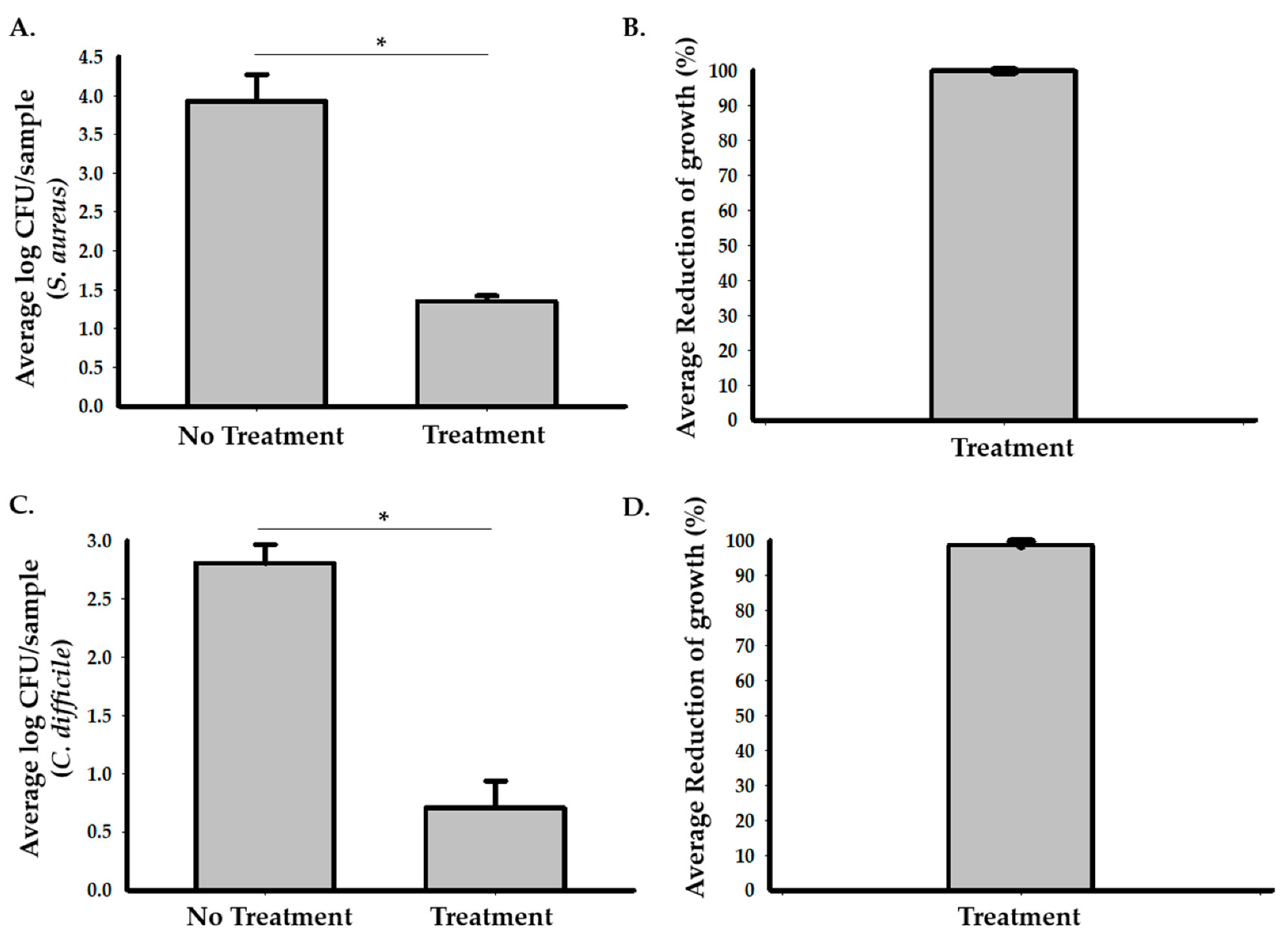
3.1. The Photocatalytic Reactor Reduces Growth of S. aureus and C. difficile Cultures in Hospital Rooms
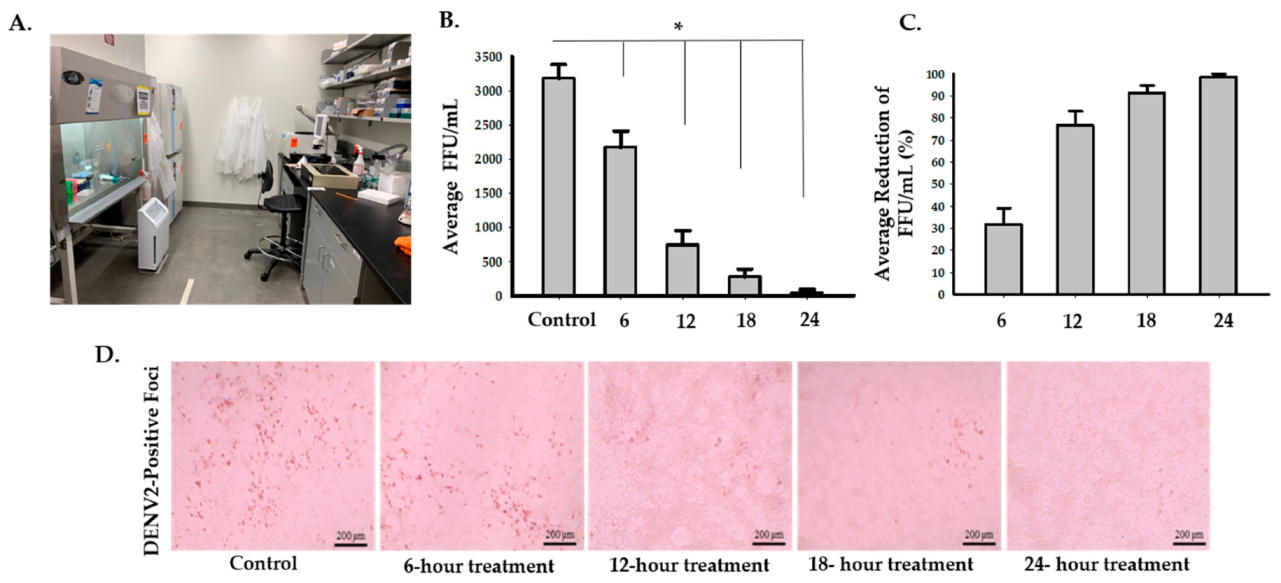
3.2. The Photocatalytic Reactor Reduces the Infectivity of Dengue Virus Type 2
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dancer, S.J. Controlling Hospital-Acquired Infection: Focus on the Role of the Environment and New Technologies for Decontamination. Clin. Microbiol. Rev. 2014, 27, 665–690. [Google Scholar] [CrossRef] [Green Version]
- Peyrony, O.; Marbeuf-Gueye, C.; Truong, V.; Giroud, M.; Rivière, C.; Khenissi, K.; Legay, L.; Simonetta, M.; Elezi, A.; Principe, A.; et al. Accuracy of Emergency Department Clinical Findings for Diagnosis of Coronavirus Disease 2019. Ann. Emerg. Med. 2020, 76, 405–412. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate Point-Prevalence Survey of Health Care—Associated Infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Available online: https://stacks.cdc.gov/view/cdc/11550 (accessed on 25 October 2020).
- Kavanagh, K.T.; Abusalem, S.; Calderon, L.E. The incidence of MRSA infections in the United States: Is a more comprehensive tracking system needed? Antimicrob. Resist. Infect. Control 2017, 6, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krein, S.L.; Mayer, J.; Harrod, M.; Weston, L.E.; Gregory, L.; Petersen, L.; Samore, M.H.; Drews, F.A. Identification and Characterization of Failures in Infectious Agent Transmission Precaution Practices in Hospitals: A Qualitative Study. JAMA Intern. Med. 2018, 178, 1016. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Read, J.M.; Tang, A.; Chen, H.; Riley, S.; Kam, K.M. A systematic review of transmission dynamic studies of methicillin-resistant Staphylococcus aureus in non-hospital residential facilities. BMC Infect. Dis. 2018, 18, 188. [Google Scholar] [CrossRef] [Green Version]
- Fordtran, J.S. Colitis Due to Clostridium difficile Toxins: Underdiagnosed, Highly Virulent, and Nosocomial. Bayl. Univ. Med. Cent. Proc. 2006, 19, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Luo, R.; Barlam, T.F. Ten-Year Review of Clostridium difficile Infection in Acute Care Hospitals in the USA, 2005–2014. J. Hosp. Infect. 2018, 98, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile Infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chitnis, A.S.; Holzbauer, S.M.; Belflower, R.M.; Winston, L.G.; Bamberg, W.M.; Lyons, C.; Farley, M.M.; Dumyati, G.K.; Wilson, L.E.; Beldavs, Z.G.; et al. Epidemiology of Community-Associated Clostridium difficile Infection, 2009 Through 2011. JAMA Intern. Med. 2013, 173, 1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidron, A.I.; Edwards, J.R.; Patel, J.; Horan, T.C.; Sievert, D.M.; Pollock, D.A.; Fridkin, S.K.; National Healthcare Safety Network Team and Participating National Healthcare Safety Network Facilities. Antimicrobial-Resistant Pathogens Associated with Healthcare-Associated Infections: Annual Summary of Data Reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect. Control Hosp. Epidemiol. 2008, 29, 996–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holland, T.L.; Raad, I.; Boucher, H.W.; Anderson, D.J.; Cosgrove, S.E.; Aycock, P.S.; Baddley, J.W.; Chaftari, A.-M.; Chow, S.-C.; Chu, V.H.; et al. Effect of Algorithm-Based Therapy vs Usual Care on Clinical Success and Serious Adverse Events in Patients with Staphylococcal Bacteremia: A Randomized Clinical Trial. JAMA 2018, 320, 1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aitken, C.; Jeffries, D.J. Nosocomial Spread of Viral Disease. Clin. Microbiol. Rev. 2001, 14, 528–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goins, W.P.; Talbot, H.K.; Talbot, T.R. Health Care–Acquired Viral Respiratory Diseases. Infect. Dis. Clin. N. Am. 2011, 25, 227–244. [Google Scholar] [CrossRef] [Green Version]
- Valenti, W.M.; Hall, C.B.; Douglas, R.G.; Menegus, M.A.; Pincus, P.H. Nosocomial Viral Infections: I. Epidemiology and Significance. Infect. Control 1980, 1, 33–37. [Google Scholar] [CrossRef]
- Chow, E.J.; Mermel, L.A. Hospital-Acquired Respiratory Viral Infections: Incidence, Morbidity, and Mortality in Pediatric and Adult Patients. Open Forum Infect. Dis. 2017, 4, ofx006. [Google Scholar] [CrossRef] [Green Version]
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2): An Update. Cureus 2020, 12, e7423. [Google Scholar] [CrossRef] [Green Version]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Walsh, K.A.; Jordan, K.; Clyne, B.; Rohde, D.; Drummond, L.; Byrne, P.; Ahern, S.; Carty, P.G.; O’Brien, K.K.; O’Murchu, E.; et al. SARS-CoV-2 detection, viral load and infectivity over the course of an infection. J. Infect. 2020, 81, 357–371. [Google Scholar] [CrossRef]
- Donskey, C.J. Does improving surface cleaning and disinfection reduce health care-associated infections? Am. J. Infect. Control 2013, 41, S12–S19. [Google Scholar] [CrossRef]
- Boyce, J.M. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob. Resist. Infect. Control 2016, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Acute antimicrobial pesticide-related illnesses among workers in health-care facilities—California, Louisiana, Michigan, and Texas, 2002–2007. MMWR Morb. Mortal. Wkly. Rep. 2010, 59, 551–556. [Google Scholar]
- Decker, B.K.; Palmore, T.N. Hospital Water and Opportunities for Infection Prevention. Curr. Infect. Dis. Rep. 2014, 16, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuijsen, M.J.; Smith, R.; Golfinopoulos, S.; Best, N.; Bennett, J.; Aggazzotti, G.; Righi, E.; Fantuzzi, G.; Bucchini, L.; Cordier, S.; et al. Health impacts of long-term exposure to disinfection by-products in drinking water in Europe: HIWATE. J. Water Health 2009, 7, 185–207. [Google Scholar] [CrossRef] [PubMed]
- Righi, E.; Bechtold, P.; Tortorici, D.; Lauriola, P.; Calzolari, E.; Astolfi, G.; Nieuwenhuijsen, M.J.; Fantuzzi, G.; Aggazzotti, G. Trihalomethanes, chlorite, chlorate in drinking water and risk of congenital anomalies: A population-based case-control study in Northern Italy. Environ. Res. 2012, 116, 66–73. [Google Scholar] [CrossRef]
- Adams, C.E.; Smith, J.; Watson, V.; Robertson, C.; Dancer, S.J. Examining the Association between Surface Bioburden and Frequently Touched Sites in Intensive Care. J. Hosp. Infect. 2017, 95, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Allen, M.; Hall, L.; Halton, K.; Graves, N. Improving Hospital Environmental Hygiene with the Use of a Targeted Multi-Modal Bundle Strategy. Infect. Dis. Health. 2018, 23, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Foster, H.A.; Ditta, I.B.; Varghese, S.; Steele, A. Photocatalytic disinfection using titanium dioxide: Spectrum and mechanism of antimicrobial activity. Appl. Microbiol. Biotechnol. 2011, 90, 1847–1868. [Google Scholar] [CrossRef]
- Nelemans, T.; Kikkert, M. Viral Innate Immune Evasion and the Pathogenesis of Emerging RNA Virus Infections. Viruses 2019, 11, 961. [Google Scholar] [CrossRef] [Green Version]
- EPA MLB SOP MB-28: Procedure for the Production and Storage or Spores of Clostridium difficile for Use in the Efficacy Evaluation of Antimicrobial Agents. 2017. Available online: https://www.epa.gov/sites/production/files/2017-09/documents/mb-28-final.pdf (accessed on 2 December 2020).
- Dunlop, P.S.M.; Sheeran, C.P.; Byrne, J.A.; McMahon, M.A.S.; Boyle, M.A.; McGuigan, K.G. Inactivation of Clinically Relevant Pathogens by Photocatalytic Coatings. J. Photochem. Photobiol. A Chem. 2010, 216, 303–310. [Google Scholar] [CrossRef]
- Serra-Burriel, M.; Keys, M.; Campillo-Artero, C.; Agodi, A.; Barchitta, M.; Gikas, A.; Palos, C.; López-Casasnovas, G. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: Systematic review and meta-analysis. PLoS ONE 2020, 15, e0227139. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Review on Antimicrobial Resistance. 2016. Available online: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf (accessed on 7 January 2021).
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bracken, T.D. Small Air Ion Properties. In Air Ions: Physical and Biological Aspects; Charry, J.M., Kavet, R.I., Eds.; CRC: Boca Raton, FL, USA, 1987; Volume 205, pp. 1–12. [Google Scholar]
- Daniels, S.L. On the ionization of air for removal of noxious effluvia. In Air ionization of indoor environments for control of volatile and particulate contaminants with nonthermal plasmas generated by dielectric-barrier discharge. IEEE Trans. Plasma Sci. 2002, 30, 1471–1481. [Google Scholar] [CrossRef]
- Daniels, S.L. On the qualities of the air as affected by radiant energies (photocatalytic ionization processes for remediation of indoor environments). J. Environ. Eng. Sci. 2007, 6, 329–342. [Google Scholar] [CrossRef]
- Ameta, R.; Solanki, M.S.; Benjamin, S.; Ameta, S.C. Photocatalysis. In Advanced Oxidation Processes for Waste Water Treatment; Elsevier: Amsterdam, The Netherlands, 2018; pp. 135–175. ISBN 978-0-12-810499-6. [Google Scholar]
- Warren, W.W.; Tupman, D.E. Enhanced Photo-Catalytic Cells. U.S. Patent 9457122, 4 October 2016. [Google Scholar]
- Liu, H.-L.; Yang, T.C.-K. Photocatalytic inactivation of Escherichia coli and Lactobacillus helveticus by ZnO and TiO2 activated with ultraviolet light. Process Biochem. 2003, 39, 475–481. [Google Scholar] [CrossRef]
- Dunlop, P.S.M.; Byrne, J.A.; Manga, N.; Eggins, B.R. The photocatalytic removal of bacterial pollutants from drinking water. J. Photochem. Photobiol. A Chem. 2002, 148, 355–363. [Google Scholar] [CrossRef]
- Tatsuma, T.; Takeda, S.; Saitoh, S.; Ohko, Y.; Fujishima, A. Bactericidal effect of an energy storage TiO2–WO3 photocatalyst in dark. Electrochem. Commun. 2003, 5, 793–796. [Google Scholar] [CrossRef]
- Kashyout, A.B.; Soliman, M.; Abd El-Haleem, D. Reprint from Disinfection of bacterial suspensions by photocatalytic oxidation using TiO2 nanoparticles under ultraviolet illumination. Alex. Eng. J. 2006, 45, 367–371. [Google Scholar]
- Li, C.-S.; Tseng, C.-C.; Lai, H.-H.; Chang, C.-W. Ultraviolet Germicidal Irradiation and Titanium Dioxide Photocatalyst for Controlling Legionella pneumophila. Aerosol. Sci. Technol. 2003, 37, 961–966. [Google Scholar] [CrossRef]
- Luo, L.; Miao, L.; Tanemura, S.; Tanemura, M. Photocatalytic sterilization of TiO2 films coated on Al fiber. Mater. Sci. Eng. B 2008, 148, 183–186. [Google Scholar] [CrossRef]
- Pal, A.; Min, X.; Yu, L.E.; Pehkonen, S.O.; Ray, M.B. Photocatalytic Inactivation of Bioaerosols by TiO2 Coated Membrane. Int. J. Chem. React. Eng. 2005, 3. [Google Scholar] [CrossRef]
- Pal, A.; Pehkonen, S.O.; Yu, L.E.; Ray, M.B. Photocatalytic inactivation of Gram-positive and Gram-negative bacteria using fluorescent light. J. Photochem. Photobiol. A Chem. 2007, 186, 335–341. [Google Scholar] [CrossRef]
- Hu, C.; Guo, J.; Qu, J.; Hu, X. Photocatalytic Degradation of Pathogenic Bacteria with AgI/TiO2 under Visible Light Irradiation. Langmuir 2007, 23, 4982–4987. [Google Scholar] [CrossRef] [PubMed]
- Oka, Y.; Kim, W.; Yoshida, T.; Hirashima, T.; Mouri, H.; Urade, H.; Itoh, Y.; Kubo, T. Efficacy of titanium dioxide photocatalyst for inhibition of bacterial colonization on percutaneous implants. J. Biomed. Mater. Res. 2008, 86B, 530–540. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Kim, D.; Cho, D.; Cho, S. Bactericidal effect of TiO2 photocatalyst on selected food-borne pathogenic bacteria. Chemosphere 2003, 52, 277–281. [Google Scholar] [CrossRef]
- Han, W.; Zhang, P.H.; Cao, W.C.; Yang, D.L.; Taira, S.; Okamoto, Y.; Arai, J.I.; Yan, X.Y. The inactivation effect of photocatalytic titanium apatite filter on SARS virus. Prog. Biochem. Biophys. 2004, 31, 982–985. [Google Scholar]
- Lin, Z.; Li, Z.; Wang, X.; Fu, X.; Yang, G.; Lin, H.; Meng, C. Inactivation Efficiency of TiO~ 2 on H1N1 Influenza Virus. Chem. J. Chin. Univ. Chin. Ed. 2006, 27, 721. [Google Scholar]
- Kato, T.; Tohma, H.; Miki, O.; Shibata, T.; Tamura, M. Degradation of norovirus in sewage treatment water by photocatalytic ultraviolet disinfection. Nippon Steel Tech. Rep. 2005, 92, 41–44. [Google Scholar]
- Kozlova, E.A.; Safatov, A.S.; Kiselev, S.A.; Marchenko, V.Y.; Sergeev, A.A.; Skarnovich, M.O.; Emelyanova, E.K.; Smetannikova, M.A.; Buryak, G.A.; Vorontsov, A.V. Inactivation and Mineralization of Aerosol Deposited Model Pathogenic Microorganisms over TiO2 and Pt/TiO2. Environ. Sci. Technol. 2010, 44, 5121–5126. [Google Scholar] [CrossRef]
- Khan, U.; Benabderrazik, N.; Bourdelais, A.J.; Baden, D.G.; Rein, K.; Gardinali, P.R.; Arroyo, L.; O’Shea, K.E. UV and solar TiO2 photocatalysis of brevetoxins (PbTxs). Toxicon 2010, 55, 1008–1016. [Google Scholar] [CrossRef] [Green Version]
- Sunada, K.; Kikuchi, Y.; Hashimoto, K.; Fujishima, A. Bactericidal and Detoxification Effects of TiO2 Thin Film Photocatalysts. Environ. Sci. Technol. 1998, 32, 726–728. [Google Scholar] [CrossRef]
- Feitz, A.J.; Waite, T.D. Kinetic Modeling of TiO2-Catalyzed Photodegradation of Trace Levels of Microcystin-LR. Environ. Sci. Technol. 2003, 37, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Maness, P.C.; Smolinski, S.; Blake, D.M.; Huang, Z.; Wolfrum, E.J.; Jacoby, W.A. Bactericidal activity of photocatalytic TiO(2) reaction: Toward an understanding of its killing mechanism. Appl. Environ. Microbiol. 1999, 65, 4094–4098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunaga, T.; Tomoda, R.; Nakajima, T.; Nakamura, N.; Komine, T. Continuous-sterilization system that uses photosemiconductor powders. Appl. Environ. Microbiol. 1988, 54, 1330–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunaga, T.; Tomoda, R.; Nakajima, T.; Wake, H. Photoelectrochemical sterilization of microbial cells by semiconductor powders. FEMS Microbiol. Lett. 1985, 29, 211–214. [Google Scholar] [CrossRef]
- Huang, Z.; Maness, P.-C.; Blake, D.M.; Wolfrum, E.J.; Smolinski, S.L.; Jacoby, W.A. Bactericidal mode of titanium dioxide photocatalysis. J. Photochem. Photobiol. A Chem. 2000, 130, 163–170. [Google Scholar] [CrossRef]
- Kangwansupamonkon, W.; Lauruengtana, V.; Surassmo, S.; Ruktanonchai, U. Antibacterial effect of apatite-coated titanium dioxide for textiles applications. Nanomed. Nanotechnol. Biol. Med. 2009, 5, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Amezaga-Madrid, P.; Nevarez-Moorillon, G.V.; Orrantia-Borunda, E.; Miki-Yoshida, M. Photoinduced bactericidal activity against Pseudomonas aeruginosa by TiO2 based thin films. FEMS Microbiol. Lett. 2002, 211, 183–188. [Google Scholar] [CrossRef]
- Amezaga-madrid, P.; Silveyramorales, R.; Cordobafierro, L.; Nevarezmoorillon, G.; Mikiyoshida, M.; Orrantiaborunda, E.; Solis, F. TEM evidence of ultrastructural alteration on Pseudomonas aeruginosa by photocatalytic TiO2 thin films. J. Photochem. Photobiol. B Biol. 2003, 70, 45–50. [Google Scholar] [CrossRef]
- Sunada, K.; Watanabe, T.; Hashimoto, K. Studies on photokilling of bacteria on TiO2 thin film. J. Photochem. Photobiol. A Chem. 2003, 156, 227–233. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gharaibeh, A.; Smith, R.H.; Conway, M.J. Reducing Spread of Infections with a Photocatalytic Reactor—Potential Applications in Control of Hospital Staphylococcus aureus and Clostridioides difficile Infections and Inactivation of RNA Viruses. Infect. Dis. Rep. 2021, 13, 58-71. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010008
Gharaibeh A, Smith RH, Conway MJ. Reducing Spread of Infections with a Photocatalytic Reactor—Potential Applications in Control of Hospital Staphylococcus aureus and Clostridioides difficile Infections and Inactivation of RNA Viruses. Infectious Disease Reports. 2021; 13(1):58-71. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010008
Chicago/Turabian StyleGharaibeh, Abeer, Richard H. Smith, and Michael J. Conway. 2021. "Reducing Spread of Infections with a Photocatalytic Reactor—Potential Applications in Control of Hospital Staphylococcus aureus and Clostridioides difficile Infections and Inactivation of RNA Viruses" Infectious Disease Reports 13, no. 1: 58-71. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010008