Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of the Literature



Abstract
:1. Introduction
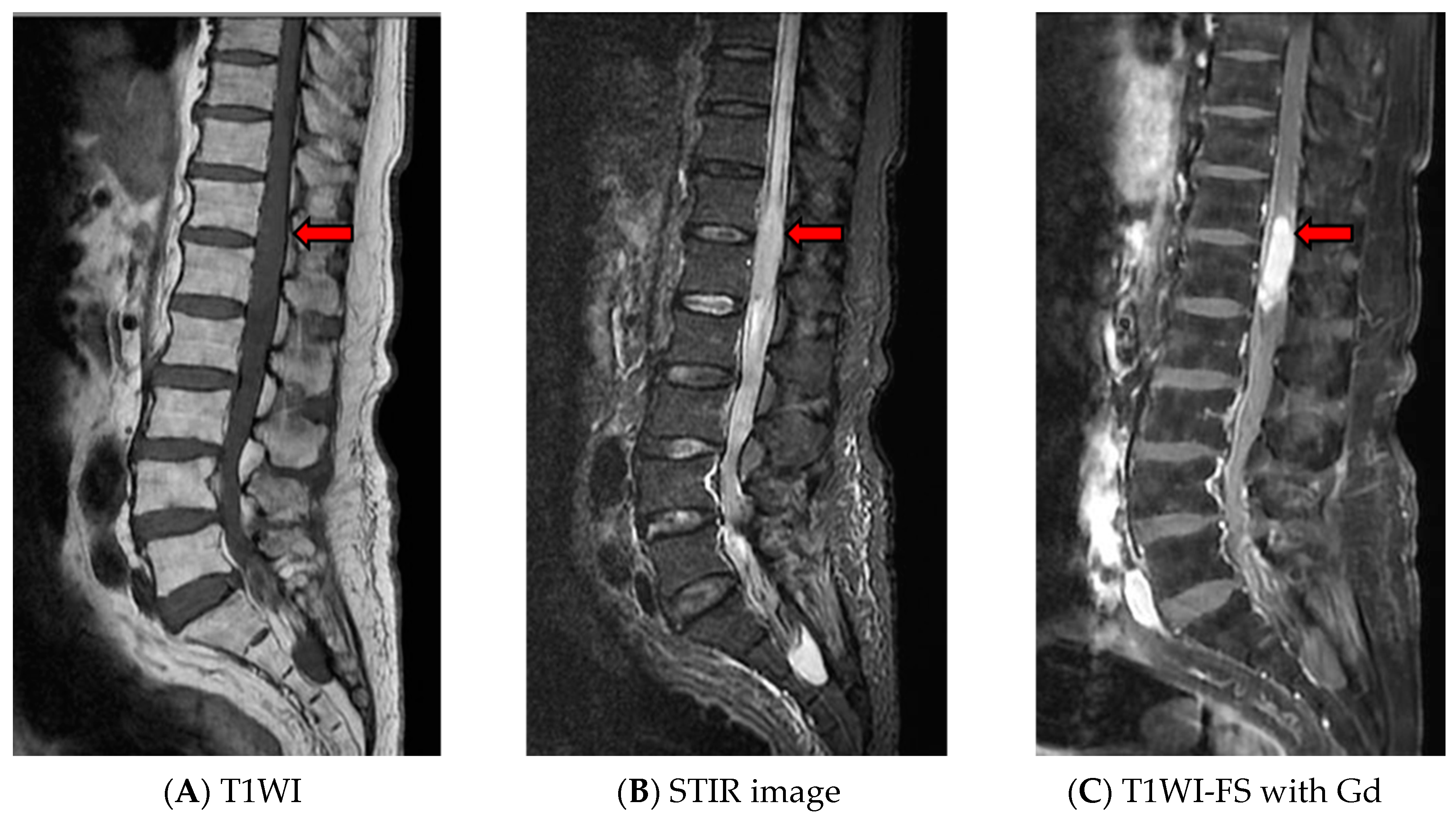
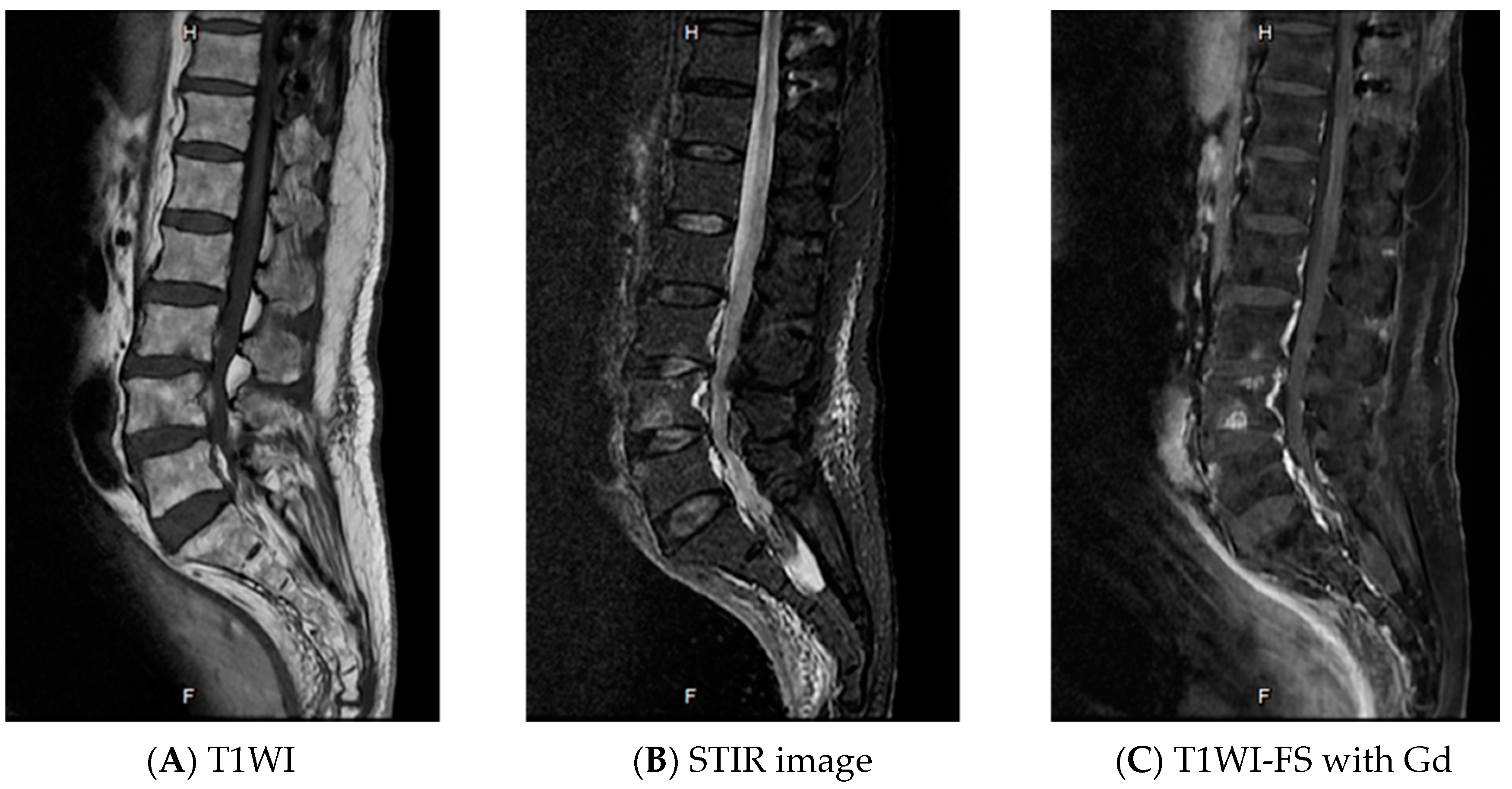
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Chotmongkol, V.; Jitpimolmard, S.; Thavornpitak, Y. Corticosteroid in tuberculous meningitis. J. Med. Assoc. Thai. 1996, 79, 83–90. [Google Scholar] [PubMed]
- MacDonell, A.H.; Baird, R.W.; Bronze, M.S. Intramedullary tuberculomas of the spinal cord: Case report and review. Rev. Infect. Dis. 1990, 12, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.C.; Arora, R.; Deol, P.S.; Mahapatra, A.K.; Sinha, A.K.; Sarkar, C. Intramedullary tuberculoma of the spinal cord: A series of 10 cases. Clin. Neurol. Neurosurg. 2002, 104, 279–284. [Google Scholar] [CrossRef]
- Feres, M.C.; Martino MC, D.; Maldijian, S.; Batista, F.; Gabriel Júnior, A.; Tufik, S. Laboratorial validation of an automated assay for the determination of adenosine deaminase activity in pleural fluid and cerebrospinal fluid. J. Bras Pneumol. 2008, 34, 1033–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa, D.; Connors, J.M.; Shenkier, T.N.; Gascoyne, R.D.; Sehn, L.H.; Savage, K.J. Incidence and risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma: The impact of the addition of rituximab to CHOP chemotherapy. Ann. Oncol. 2010, 21, 1046–1052. [Google Scholar] [CrossRef]
- Bradbury, P.G.; Davis, C.J.F. Conus tuberculoma responding to chemotherapy. Ann. Neurol. 1980, 7, 392–393. [Google Scholar] [CrossRef]
- Choksey, M.S.; Powell, M.; Gibb, W.R.; Casey, A.T.; Geddes, J.F. A conus tuberculoma mimicking an intramedullary tumor: A case report and review of the literature. Br. J. Neurosurg. 1989, 3, 117–121. [Google Scholar] [CrossRef]
- Sie, L.T.; Linssen, W.H. Isolated intramedullary tuberculosis presenting as a conus tumor. Clin. Infect. Dis. 1994, 19, 549–550. [Google Scholar] [CrossRef]
- Dehoux, E.; Awada, A.; Palkar, V. Urinary retention revealing a tuberculoma of the conus medullaris in a patient with intracranial tuberculosis: Case report. Spinal Cord 1996, 34, 630–632. [Google Scholar] [CrossRef]
- Suzer, T.; Coskun, E.; Tahta, K.; Bayramoğglu, H.; Düzcan, E. Intramedullary spinal tuberculoma presenting as a conus tumor: A case report and review of the literature. Eur. Spine J. 1998, 7, 168–171. [Google Scholar] [CrossRef] [Green Version]
- Parmar, H.; Shah, J.; Patkar, D.; Varma, R. Intramedullary tuberculomas. MR findings in seven patients. Acta Radiol. 2000, 41, 572–577. [Google Scholar] [CrossRef]
- Kemaloglu, S.; Gur, A.; Nas, K.; Cevik, R.; Buyukbayram, H.; Saraç, A. Intramedullary tuberculoma of the conus medullaris: Case report and review of the literature. Spinal Cord 2001, 39, 498–501. [Google Scholar] [CrossRef] [Green Version]
- Tureyen, K. Tuberculoma of the conus medullaris: Case report. Neurosurgery 2002, 50, 651–652. [Google Scholar]
- Jaiswal, A.K.; Jaiswal, S.; Gupta, S.K.; Gautam, V.K.S.; Kumar, S. Intramedullary tuberculoma of the conus. J. Clin. Neurosci. 2006, 1, 870–872. [Google Scholar] [CrossRef]
- Skoglund, T.S.; Nilsson, D. Tumor of the conus medullaris treated with antituberculous therapy. Clin. Neurol. Neurosurg. 2007, 109, 192–194. [Google Scholar] [CrossRef]
- Maamar, M.; El Quessar, A.; El Fatemi, N.; El Hassani, M.R.; Chakir, N.; Jiddane, M. Intramedullary tuberculoma: A case report. Radiography 2007, 13, 251–254. [Google Scholar] [CrossRef]
- Lawler, M.; Zulu, S.; Archary, M.; Govender, V. Intramedullary conus medullaris tuberculoma in an HIV-infected child: An unusual immune reconstitution inflammatory syndrome response. S. Afr. J. Epidemiol. Infect. 2013, 2, 69–71. [Google Scholar] [CrossRef]
- Sharoff, L.M.; Unnikrishnan, R.; Jagani, N. Isolated conus medullaris tuberculoma mimicking a tumor: A rare case report. ANZ J. Surg. 2017, 87, E218–E219. [Google Scholar] [CrossRef]
- Jaiswal, M.; Gandhi, A.; Purohit, D.; Mittal, R.S. Concurrent multiple intracranial and intramedullary conus tuberculoma: A rare case report. Asian J. Neurosurg. 2017, 12, 331–333. [Google Scholar] [CrossRef] [Green Version]
- Ebner, F.H.; Roser, F.; Acioly, M.A.; Schoeber, W.; Tatagiba, M. Intramedullary lesions of the conus medullaris: Differential diagnosis and surgical management. Neurosurg. Rev. 2009, 32, 287–300. [Google Scholar] [CrossRef]
- Sullivan, J.L.; Osborne, W.R.; Wedgewood, R.J. Adenosine deaminase activity in lymphocytes. Br. J. Haematol. 1977, 37, 157–158. [Google Scholar] [CrossRef]
- Pormohammad, A.; Riahi, S.M.; Nasiri, M.J.; Fallah, F.; Aghazadeh, M.; Doustdar, F.; Pouriran, R. Diagnostic test accuracy of adenosine deaminase for tuberculous meningitis: A systemic review and meta-analysis. J. Infect. 2017, 74, 545–554. [Google Scholar] [CrossRef]
- Trivedi, R.; Saksena, S.; Gupta, R.K. Magnetic resonance imaging in central nervous system tuberculosis. Indian J. Radiol. Imaging 2009, 19, 256–265. [Google Scholar]
- Perry, M.D.; White, P.L.; Ruddy, M. Potential for use of the Seegene Anyplex MTB/NTM real-time detection assay in a regional reference laboratory. J. Clin. Microbiol. 2014, 52, 1708–1710. [Google Scholar] [CrossRef] [Green Version]
- Parny, I.F.; Johnson, E.S.; Allen, P.B. ‘Idiopathic’ cranial hypertrophic pachymeningitis responsive to antituberculous therapy: Case report. Neurosurgery 1997, 41, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; You, C.; Yang, Y.; He, M.; Cai, B.; Wang, X.; Ju, Y. Intramedullary spinal tuberculoma: Report of three cases. Surg. Neurol. 2006, 65, 185–188. [Google Scholar] [CrossRef]
- Jaiswal, M.; Gandhi, A.; Sharma, A.; Mittal, R.S. Experiences and conceptualization of spinal intramedullary tuberculoma management. Korean J. Spine 2015, 12, 5–11. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author | Age/Sex | Underlying Disease | Clinical Presentation and Duration of Symptoms | Associated TB | Diagnostic Method | Surgical Excision | Duration of Antituberculous Treatment | Clinical Outcome |
|---|---|---|---|---|---|---|---|---|
| Bradbury et al. (1980) [6] | 26/M | No | Rt. Leg weakness, decreased sensation in the L5-S1 distribution duration: N/A | Pulmonary TB | Response to chemotherapy | No | N/A | Complete recovery |
| Choksey et al. (1989) [7] | 31/F | No | Paraparesis, decreased sensation in the sacral dermatome, ascending to the L1-L2 dermatomes, urgency of micturition duration: 4 weeks | No | Histopathology | No | N/A | Marked improvement |
| Sie et al. (1994) [8] | 24/M | No | Paraparesis, hypoesthesia in the sacral dermatomes, urinary urgency, impotence duration: N/A | No | Histopathology | No | N/A | Marked improvement |
| Dehoux et al. (1996) [9] | 58/M | No | Fever, headache, confusion for 1 month, followed by back pain and legs, left hemiparesis, weakness of the right legs for 2 weeks | Tuberculous meningitis and cerebral tuberculoma | Lymphocytic CSF with high protein and low glucose level | No | N/A | Marked improvement |
| Suzer et al. (1998) [10] | 20/M | No | Low back pain, urinary urgency, impotence, distal weakness of both legs, hypoesthesia in the sacral dermatome, ascending to L4 dermatome Duration: 10 days | No | Histopathology | Yes | N/A | Marked improvement |
| Parmar et al. (2000) [11] | 35/M | HIV | Paraparesis Duration: N/A | Pulmonary and left ankle TB | Response to chemotherapy | No | 18 months | improvement |
| Kemaloglu et al. (2001) [12] | 32/M | No | Paraparesis and pain, urinary incontinence Duration: N/A | PulmonaryTB | Histopathology | Yes | 12 months | Marked improvement |
| Tureyen (2002) [13] | 46/M | No | Lt. leg weakness Duration: 7 days | History of PulmonaryTB | Histopathology | Yes | 6 months | Complete recovery |
| Jaiswal et al. (2006) [14] | 12/F | No | Low back pain, paraparesis with numbness, urinary incontinence Duration: 6 weeks | No | Histopathology | Yes | N/A | Marked improvement |
| Skoglund et al. (2007) [15] | 21/M | No | Lumbar pain, sensory disturbance of both legs and perianal, lt. leg weakness, pain during miction, fever Duration: 2 months | PulmonaryTB | Response to chemotherapy | No | 9 months | Marked improvement |
| Maamar et al. (2007) [16] | 22/M | No | Paraparesis with paresthesia, urine retention, fever Duration: 6 months | No | Histopathology | Yes | 12 months | Marked improvement |
| Lawler et al. (2013) [17] | 12/F | HIV | Paraparesis with hyperaesthesia, urinary retention, febrile Duration: 2 days | Cerebellar abscess TB | Response to chemotherapy | No | N/A | Marked improvement |
| Sharoff et al. (2017) [18] | 46/M | No | Low back pain, bladder incontinence, impotence, paraparesis and hypoesthesia below L3 Duration: 1 month | No | Histopathology | Yes | N/A | Complete recovery |
| Jaiswal et al. (2017) [19] | 16/M | No | Back pain, paraparesis, impaired sensation below L1, fever Duration: 2 weeks | Pulmonary TB | Response to chemotherapy | No | N/A | Marked improvement |
| Present case | 78/M | Lymphoma, diabetes mellitus | Paraparesis with dull ache Duration: 6 weeks | No | High level of CSF-ADA | No | 18 months | Minimal improvement |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chotmongkol, V.; Wanitpongpun, C.; Phuttharak, W.; Khamsai, S. Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of the Literature. Infect. Dis. Rep. 2021, 13, 82-88. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010010
Chotmongkol V, Wanitpongpun C, Phuttharak W, Khamsai S. Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of the Literature. Infectious Disease Reports. 2021; 13(1):82-88. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010010
Chicago/Turabian StyleChotmongkol, Verajit, Chinadol Wanitpongpun, Warinthorn Phuttharak, and Sittichai Khamsai. 2021. "Intramedullary Conus Medullaris Tuberculoma: A Case Report and Review of the Literature" Infectious Disease Reports 13, no. 1: 82-88. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010010