
Why Counseling Intervention Fails to Improve Compliance towards Antiretroviral Therapy: Findings from a Mixed-Methods Study among People Living with HIV in Bali Province, Indonesia

 , ,
, ,
Abstract
:1. Introduction
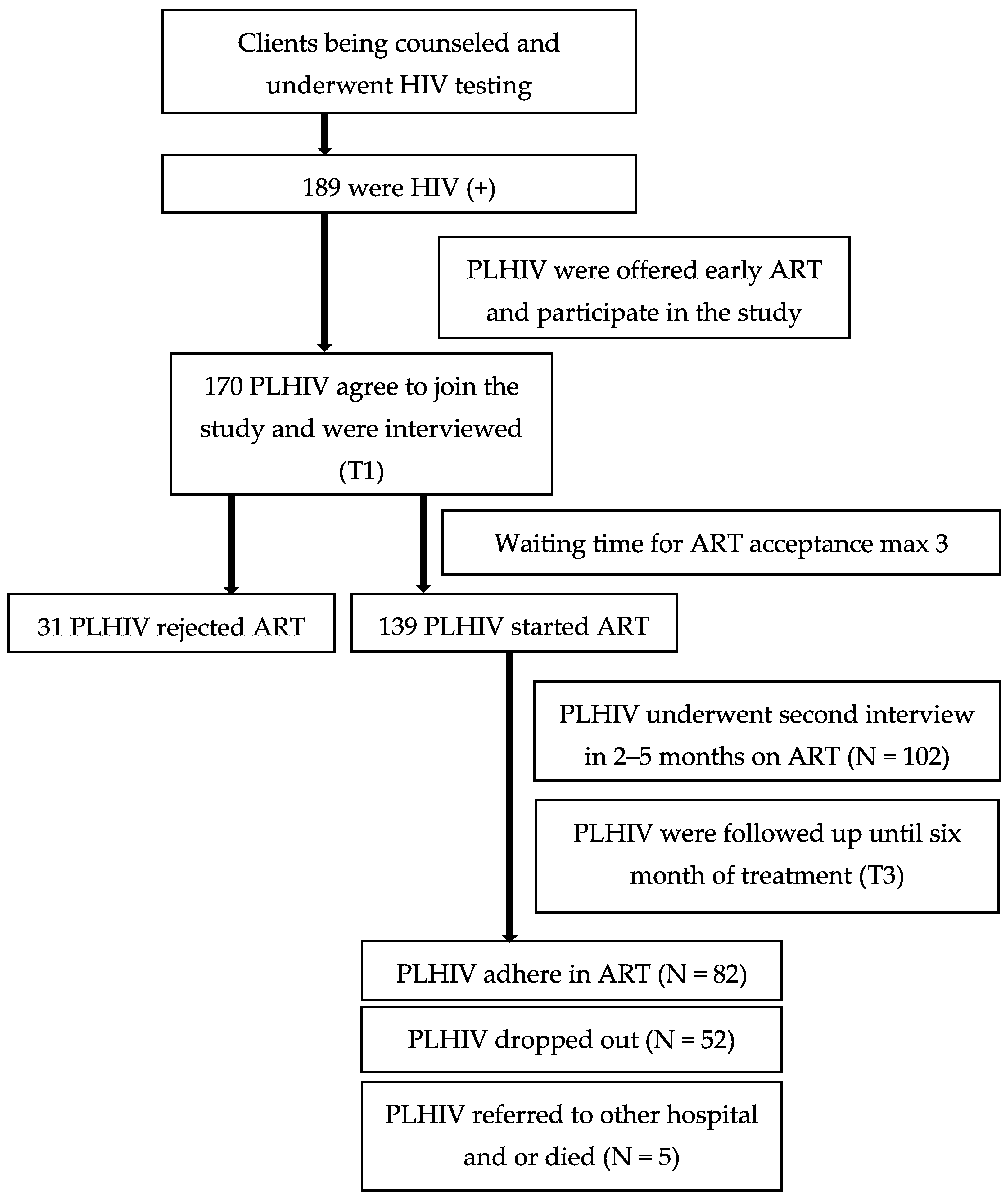
2. Materials and Methods
3. Results
3.1. Socio-Demographics Characteristic of Respondent
3.2. Counseling Activities Reported by People Living with HIV (PLHIV)
3.3. Correlation between Counseling and Acceptance and Adherence to Antiretroviral
3.4. Findings from Qualitative Result
3.4.1. Summary of In-Depth Interviews with Counselors and PLHIV
“All have been explained… feel gap… not like being with your friends, you can tell more… feeling comfortable… I received both information and support from here… ”(Subject-1, MSM)
“I remember to consume the drug…… [OWs] remind me to take my medication regularly through text message…… ”(Subject 2, FSW)
“… They [OWs] advised me to return to the clinic but I cannot go back, … I told [them/OWs] that I suffered from side effects … looks tiny and sick.”(Subject-3, MSM)
“Yes, it contains lots of information, but I could not really get the idea… The counseling was very short… about ten minutes…”(Subject-3, MSM)
“… [OW] told me not to open my status to every one…”(Subject-4, FSW)
“… [OW] not talked about ART processes or its functions as both prevention and treatment… he told me to take my medication for my own health. I did because I want to be healthy…”(Subject-3, MSM)
“… I thought if I am not working in sex work, I could not ask for ART from the clinic”(Subject-4, FSW)
“… I don’t remember anything from the counseling… ”(Subject-2, FSW)
“I never been told about that [stigma and disclosure] … No, the doctor also never discussed that [stigma and disclosure] with me”(Subject-1, MSM)
“No, I cannot tell him…, I looked for more information out there. I have been on herbal medication for one month, while he [OWs counselor] didn’t know… ”(Subject-1, MSM)
“Previously I was sure [to determine whether PLHIV will adhere to ART or not before initiate treatment])… finally, I realized that I commonly make mistake… some people who have long speech and looks smart but finally not adhere to treatment… some people look stupid and accept, but they have strong motivation and adhere to the treatment… ”(Subject-10, OW)
3.4.2. Summary of Exit Interviews to PLHIV and Outreach Counselor Workers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Indonesian Ministry of Health. Laporan perkembangan HIV AIDS & penyakit infeksi menular seksual (PIMS) triwulan II tahun 2020. In Report of HIV AIDS and Sexually Transmitted Infection Trimester II Year 2020); Jakarta, Indonesia. 2020. Available online: https://siha.kemkes.go.id/portal/files_upload/Cover_TW_II_2020_FINAL_OK_050820_1.pdf (accessed on 10 November 2020).
- Indonesian Ministry of Health. Estimates and Projection of HIV AIDS in Indonesia; Dipublikasikan Pada: Sabtu, Indonesia, 2016.
- Indonesian Ministry of Health. Estimates and Projection of HIV/AIDS in Indonesia 2019–2024; Jakarta, Dipublikasikan Pada: Sabtu, Indonesia, 2020.
- Joint United Nations Programme on HIV/AIDS UNAIDS Data 2017; UN Joint Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2017.
- Montaner, J.S.G.; Lima, V.D.; Harrigan, P.R.; Lourenço, L.; Yip, B.; Nosyk, B.; Wood, E.; Kerr, T.; Shannon, K.; Moore, D.; et al. Expansion of HAART coverage is associated with sustained decreases in HIV/AIDS morbidity, mortality and HIV transmission: The “HIV treatment as prevention” sxperience in a Canadian setting. PLoS ONE 2014, 9, e87872. [Google Scholar] [CrossRef]
- WHO; CDC; The Global Fund. HIV Drug Resistance Report 2017; 2017. Available online: https://www.who.int/hiv/pub/drugresistance/hivdr-report-2017/en/ (accessed on 10 November 2020).
- Friedland, G.H. HIV medication adherence. The intersection of biomedical, behavioral, and social science research and clinical practice. J. Acquir. Immune Defic. Syndr. 2006, 43, S3–S9. [Google Scholar] [CrossRef]
- Indonesian Ministry of Health. Pedoman layanan komprehensif HIV-AIDS & IMS di lapas, rutan dan bapas. In Guidelines for HIV-AIDS & STIs Comprehensive Services in Prisons, Detention Centers and Correctional Centers; Dipublikasikan Pada: Sabtu, Indonesia, 2012; ISBN 1955090319. [Google Scholar]
- Indonesian Ministry of Health. Surat edaran menteri kesehatan RI tentang layanan pencegahan penularan HIV dari ibu ke anak (PPIA). In Circular Letter of Minister of Health of the Republic of Indonesia Regarding Services to Prevent Mother-to-Child Transmission of HIV; Dipublikasikan Pada: Sabtu, Indonesia, 2013. [Google Scholar]
- Indonesian Ministry of Health. Pedoman nasional tes dan konseling HIV dan AIDS. In National Guidelines for HIV and AIDS Testing and Counseling; Dipublikasikan Pada: Sabtu, Indonesia, 2014. [Google Scholar]
- Januraga, P.P.; Reekie, J.; Mulyani, T.; Lestari, B.W.; Iskandar, S.; Wisaksana, R.; Kusmayanti, N.A.; Subronto, Y.W.; Widyanthini, D.N.; Wirawan, D.N.; et al. The cascade of HIV care among key populations in Indonesia: A prospective cohort study. Lancet HIV 2018, 5, e560–e568. [Google Scholar] [CrossRef] [Green Version]
- Indonesian Ministry of Health. Kajian Epidemiologi HIV Indonesia 2016 (Indonesian Epidemiological Study of HIV); Kementerian Kesehatan RI: Jakarta, Indonesia, 2016.
- Burtle, D.; Welfare, W.; Elden, S.; Mamvura, C.; Vandelanotte, J.; Petherick, E.; Walley, J.; Wright, J. Introduction and evaluation of a “pre-ART care” service in Swaziland: An operational research study. BMJ Open 2012, 2, e000195. [Google Scholar] [CrossRef] [Green Version]
- Kulkarni, S.; Hoffman, S.; Gadisa, T.; Melaku, Z.; Fantehun, M.; Yigzaw, M.; El-Sadr, W.; Remien, R.; Tymejczyk, O.; Nash, D.; et al. Identifying perceived barriers along the HIV care continuum. J. Int. Assoc. Provid. AIDS Care 2016, 15, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Heyer, A.; Mabuza, L.; Couper, I.; Ogunbanjo, G. Understanding participation in a hospital-based HIV support group in Limpopo Province, South Africa. S. Afr. Fam. Pract. 2010, 52, 234–239. [Google Scholar] [CrossRef]
- Jiamsakul, A.; Kumarasamy, N.; Ditangco, R.; Li, P.C.K.; Phanuphak, P.; Sirisanthana, T.; Sungkanuparph, S.; Kantipong, P.; Lee, C.K.C.; Mustafa, M.; et al. Factors associated with suboptimal adherence to antiretroviral therapy in Asia. J. Int. AIDS Soc. 2014, 17, 1–9. [Google Scholar] [CrossRef]
- Kim, T.W.; Palepu, A.; Cheng, D.M.; Libman, H.; Saitz, R.; Samet, J.H. Factors associated with discontinuation of antiretroviral therapy in HIV-infected patients with alcohol problems. AIDS Care 2007, 19, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.D.; Linnan, L.A.; Emmons, K.M. Fidelity and its relationship to impementation effectiveness, adaptation, and dissemination. In Dissemination and Implementation in Health: Translating Science to Practice; Ross, B.P.E., Graham, C., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 281–304. ISBN 9780199933242. [Google Scholar]
- Mabuto, T.; Charalambous, S.; Hoffmann, C.J. Effective interpersonal health communication for linkage to care after HIV diagnosis in south africa. J. Acquir. Immune Defic. Syndr. 2017, 74, S23–S28. [Google Scholar] [CrossRef] [Green Version]
- Altice, F.L.; Mostashari, F.; Friedland, G.H. Trust and the acceptance of and adherence to antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2001, 28, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of change. J. Clin. Psychol. 2011, 67, 143–154. [Google Scholar] [CrossRef]
- Sylvain, H.; Delmas, P. Readiness in HIV treatment adherence: A matter of confidence. An exploratory study. Open AIDS J. 2011, 5, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Norcross, J.C.; Diclemente, C.C. Applying the stages of change. Psychother. Aust. 2013, 19, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Lenio, J.A. Analysis of the transtheoretical model of behavior change. Appl. Psychol. 2006, 73–86. [Google Scholar]
- Grimes, R.M.; Grimes, D.E. Readiness: The state of the science (or the Lack Thereof). Curr. HIV/AIDS Rep. 2010, 7, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Mthembu, T.G.; Van Wyk, B. Patients’ knowledge and beliefs about antiretroviral treatment and factors associated with adherence in Mpumalanga Province, South Africa. Health SA Gesondheid 2014, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sasse, G.M. Investigating the effects of dogmatism on openness and empathy in counselors-in-training. Diss. Abstr. Int. Sect. A Humanit. Soc. Sci. 2015, 76. Available online: http://0-ovidsp-ovid-com.brum.beds.ac.uk/ovidweb.cgi?T=JS&PAGE=reference&D=psyc12&NEWS=N&AN=2015-99230-254 (accessed on 10 November 2020).
- Malawi Ministry of Health. Malawi Comprehensive HIV Testing and Counselling Training. Participant Handbook; Malawi Ministry of Health: Lilongwe, Malawi, 2013.
- Bureau od International Cooperation on HRD TICA Thailand’s Annual International Training Course (AITC) 2017. Management of Antiretroviral Treatment (ART) and Long-Term Adherence to ART. 2017. Available online: http://tica.thaigov.net/main/en/information/40489-The-Annual-International-Training-Courses-(AITC).html (accessed on 10 November 2020).
- Engender Health Society. Adherence to Treatment for HIV a Training Curriculum for Counselors Facilitator Guide; Engender Health Society: New Delhi, India, 2006; ISBN 9111261471. [Google Scholar]
- Joglekar, N.S.; Momin, A.R. Counseling for HIV/AIDS. In HIV/AIDS in India; Global Vision Publishing House: New Delhi, India, 2016; pp. 190–257. [Google Scholar]
- Peters, M.; Sawyer, C.; Willis, J. Counselor’s crisis self-efficacy scale: A validation study. VISTAS Online 2017. [Google Scholar]
- Ogden, K.R.W.; Sias, S.M. An integrative model of staff development in counseling agencies. VISTAS Online 2016. [Google Scholar]
- Diabaté, S.; Zannou, D.M.; Geraldo, N.; Chamberland, A.; Akakpo, J.; Ahouada, C.; Loembé, M.M.; Anagonou, S.; Labbé, A.C.; Alary, M.; et al. Antiretroviral therapy among HIV-1 infected female sex workers in Benin: A comparative study with patients from the general population. World J. AIDS 2011, 1, 94–99. [Google Scholar] [CrossRef] [Green Version]
- Ndou, T.V.; Risenga, P.R.; Maputle, M.S. Experiences of HIV positive patients on ARV treatment at the thulamela municipality in the Vhembe district of Limpopo Province, South Africa. J. Antivirals Antiretrovir. 2013, 5, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Gmbh, W.V.; Kgaa, C.; Pendyala, V.R.R.; Graham, U.M. Supported by: Supported by. 2010. Available online: https://docs.microsoft.com/en-us/previous-versions/office/lync-server-2013/lync-server-2013-exchange-unified-messaging-um-support (accessed on 10 November 2020).
- Paudel, V.; Baral, K.P. Women living with HIV/AIDS (WLHA), battling stigma, discrimination and denial and the role of support groups as a coping strategy: A review of literature. Reprod. Health 2015, 12. [Google Scholar] [CrossRef] [Green Version]
- Therkelsen, D. Challenges to Adherence among MSM and LGBTI Living with HIV in Kampala, Uganda: Scoping Study; Heard: Durban, South Africa, 2015. [Google Scholar] [CrossRef]
- UNAIDS. Review of Long-Acting Injectable Candidates for HIV Treatment and Prevention. 2018. Available online: https://unitaid.org/assets/Andrew-Hill-WHO-review-of-LA-injectables-HIV-Sept-2018.pdf (accessed on 10 November 2020).
- Barnhart, M. Long-Acting HIV treatment and prevention: Closer to the threshold. Glob. Health Sci. Pract. 2017, 5, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Carillon, S.; Gallardo, L.; Linard, F.; Chakvetadze, C.; Viard, J.P.; Cros, A.; Molina, J.M.; Slama, L. Perspectives of injectable long acting antiretroviral therapies for HIV treatment or prevention: Understanding potential users’ ambivalences. AIDS Care-Psychol. Socio-Med. Asp. AIDS/HIV 2020, 32, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Smith, O.; Minior, T.; Jordan, N.; Woolford, J.; Vitalis, D.; Storm, D. A multidisciplinary approach to improving adherence to antiretroviral therapy. In Proceedings of the XVII International AIDS Conference, Mexico City, Mexico, 3–8 August 2008; p. 1. Available online: http://rbhs.rutgers.edu/fxbweb/downloads/GYposter_Adherence_IAS2008.pdf (accessed on 10 November 2020).
- Huet, C.; Ouedraogo, A.; Konaté, I.; Traore, I.; Rouet, F.; Kaboré, A.; Sanon, A.; Mayaud, P.; Van De Perre, P.; Nagot, N. Long term virological, immunological and mortality outcomes in a cohort of HIV-infected female sex workers treated with highly active antiretroviral therapy in Africa. BMC Public Health 2011, 11, 700. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.A.; Mugavero, M.J.; Amico, K.R.; Cargill, V.A.; Chang, L.W.; Gross, R.; Orrell, C.; Altice, F.L.; Bangsberg, D.R.; Bartlett, J.G.; et al. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: Evidence-based recommendations from an international association of physicians in AIDS care panel. Ann. Intern. Med. 2012, 156, 817–833. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, A.; Srikanth, B.A.; Reddy, K.P.; Reddy, K.N.; Hari, A.; Abhijeet, A.; Pradesh, A. Patient counseling tools for improving adherence to antiretroviral. Int. J. Pharm. Sci. Res. 2014, 3, 4634–4639. [Google Scholar]
- Kennedy, S.; Goggin, K.; Nollen, N. Adherence to HIV medications: Utility of the theory of self-determination. Cognit. Ther. Res. 2004, 28, 611–628. [Google Scholar] [CrossRef]
- Sow, P.G.; Coume, M.; Ka, O.; Gaye, A.; Fall, A.B.; Toure, K.; Traore, I. Investigation of factors affecting medication adherence among people living with HIV/AIDS under non—Governmental organizations in Senegal. Public Health Res. 2012, 2, 143–147. [Google Scholar] [CrossRef]
- Gesesew, H.A.; Ward, P.; Hajito, K.W.; Feyissa, G.T.; Mohammadi, L.; Mwanri, L. Discontinuation from antiretroviral therapy: A continuing challenge among adults in HIV care in Ethiopia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169651. [Google Scholar] [CrossRef] [Green Version]
- Cowan, F.M.; Mtetwa, S.; Davey, C.; Fearon, E.; Dirawo, J.; Wong-Gruenwald, R.; Ndikudze, T.; Chidiya, S.; Benedikt, C.; Busza, J.; et al. Engagement with HIV prevention treatment and care among female sex workers in Zimbabwe: A respondent driven sampling survey. PLoS ONE 2013, 8, e77080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gesesew, H.A.; Ward, P.; Woldemichael, K.; Mwanri, L. Prevalence, trend and risk factors for antiretroviral therapy discontinuation among HIV-infected adults in Ethiopia in 2003–2015. PLoS ONE 2017, 12, e0179533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunstein, S.L.; Umulisa, M.-M.; Veldhuijzen, N.J.; Kestelyn, E.; Ingabire, C.M.; Nyinawabega, J.; van de Wijgert, J.H.H.M.; Nash, D. HIV diagnosis, linkage to HIV care, and HIV risk behaviors among newly diagnosed HIV-positive female sex workers in Kigali, Rwanda. J. Acquir. Immune Defic. Syndr. 2011, 57, e70–e76. [Google Scholar] [CrossRef] [PubMed]
- Poka-Mayap, V.; Pefura-Yone, E.W.; Kengne, A.P.; Kuaban, C. Mortality and its determinants among patients infected with HIV-1 on antiretroviral therapy in a referral centre in Yaounde, Cameroon: A retrospective cohort study. BMJ Open 2013, 3, 1–7. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | PLHIV Agreed to Participate in the Study (n = 170) | PLHIV Accepted ART Three Months after the Counseling (n = 139) | p * | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| PLHIV | ||||||
| Sex | Female | 55 | (32.4) | 43 | (30.9) | 0.78 |
| Male | 115 | (67.7) | 96 | (69.1) | ||
| Age (year) | Median (IQR) | 30.1 | (25.2–36.1) | 29.7 | (25.0–39.9) | 0.93 |
| Education | Illiterate–elementary school | 35 | (20.6) | 25 | (18.0) | 0.56 |
| Junior high school | 25 | (14.7) | 22 | (15.8) | 0.79 | |
| High school and University | 110 | (64.7) | 92 | (66.2) | ||
| Occupation | Unemployed | 23 | (13.5) | 19 | (14.0) | 0.73 |
| Employed | 147 | (86.7) | 120 | (86.0) | ||
| Salary (million, IDR = Indonesia Rupiah) | Median (IQR) | 2.0 | (1.5–3.0) | 2.0 | (1.6–3.1) | |
| Work length (year) | Median (IQR) | 2.0 | (1.0–4.0) | 2.0 | (1.0–4.0) | |
| Marital status | Not married | 97 | (57.1) | 83 | (59.7) | 0.64 |
| Married | 28 | (16.5) | 23 | (16.6) | 0.96 | |
| Widow/divorce | 45 | (26.5) | 33 | (23.8) | ||
| Risk group | Heterosexual (include housewives) | 27 | (15.9) | 25 | (18.0) | 0.63 |
| FSW | 45 | (26.5) | 33 | (23.7) | 0.58 | |
| MSM, bi-sex, transgender | 98 | (57.7) | 81 | (58.3) | ||
| Outreach workers (n = 17) | ||||||
| Sex | Female | 5 | (29.0) | |||
| Male | 12 | (71.0) | ||||
| Education | High School | 10 | (58.9) | |||
| University | 7 | (41.1) | ||||
| Age (year) | Median (IQR) | 36.0 | (33.8–43.0) | |||
| Work length (year) | Median (IQR) | 3 | (2–5.3) | |||
| Counseling Item | T1 (n = 170) | T2 (n = 102) | p * | ||
|---|---|---|---|---|---|
| Yes | Yes | ||||
| n | % | n | % | ||
| Counselor is the OW | 156 | (91.8) | 92 | (90.2) | 0.63 |
| There is someone else during counseling | 19 | (11.2) | 20 | (19.6) | 0.06 |
| Counseling is in private room | 168 | (98.8) | 101 | (99.6) | 0.49 |
| Explained for test result | 169 | (99.4) | 101 | (99.6) | 0.83 |
| Understand the explanation of test result | 167 | (98.2) | 95 | (93.1) | 0.03 |
| Explained risk of HIV transmission | 170 | (100) | 95 | (93.1) | 0.00 |
| Explained on preventing transmission | 170 | (100) | 97 | (95.1) | 0.05 |
| Explained further laboratory examination | 168 | (98.8) | 92 | (90.2) | 0.00 |
| Offered ART | 170 | (100) | 96 | (94.1) | 0.00 |
| Explained benefit of ART | 170 | (100) | 100 | (98.0) | 0.09 |
| Explained of ways to consume ART | 168 | (98.8) | 102 | (100) | 0.22 |
| Explained about overcoming side effect | 165 | (97.1) | 96 | (94.1) | 0.22 |
| Given mobile number of OW | 166 | (97.6) | 100 | (98.0) | 0.83 |
| Given opportunity to ask and express feeling | 169 | (99.4) | 97 | (95.1) | 0.02 |
| Given opportunity to discuss | 167 | (98.2) | 97 | (95.1) | 0.15 |
| Given opportunity to think | 169 | (99.4) | 101 | (99.0) | 0.72 |
| Feel to be supported | 170 | (100) | 102 | (100) | 1.00 |
| Score counseling (1–17) | |||||
| 12–17 | 11–17 | |||
| 16 (0) | 16 (1) | 1.00 | ||
| Length of counseling (minute) | |||||
| 10–80 | 0–60 | |||
| 30 (0) | 10 (15) | 0.00 | ||
| Frequency of counseling | |||||
| 1–4 | 0–15 | |||
| 1 (1) | 3 (2) | 0.00 | ||
| Characteristics of Counseling (T1) | Total (170) | Accept (139) | Reject (31) | p ** | |||
| n | % | n | % | n | % | ||
| Median (IQR) total items | 16 (0) | 16 (0) | 16 (0) | ||||
| >median | 149 | (87.6) | 121 | (81.2) | 28 | (18.9) | 0.77 |
| ≤median | 21 | (12.4) | 18 | (85.7) | 3 | (14.3) | |
| Median (IQR) time | 30 (37.5) | 30 (0) | 30 (10) | ||||
| >median | 23 | (23.5) | 20 | (87.0) | 3 | (13.0) | 0.77 |
| ≤median | 147 | (86.5) | 119 | (81.9) | 28 | (19.1) | |
| Median (IQR) frequency | 1(1) | 1 (1) | 1 (1) | ||||
| >median | 57 | (33.2) | 48 | (84.2) | 9 | (15.8) | 0.68 |
| ≤median | 113 | (66.8) | 91 | (80.5) | 22 | (19.5) | |
| Characteristics of counseling (T1) | Total (134) a | Adhere (82) | Dropout (52) | p** | |||
| n | % | n | % | n | % | ||
| Median (IQR) total items | 16 (0) | 16 (0) | 16 (0) | ||||
| >median | 116 | (86.6) | 71 | (61.2) | 45 | (38.8) | 1.00 |
| ≤median | 18 | (13.4) | 11 | (61.1) | 7 | (38.9) | |
| Median (IQR) time | 30 (0) | 30 (0) | 30 (0) | ||||
| >median | 20 | (14.9) | 15 | (75.0) | 5 | (25.0) | 0.22 |
| ≤median | 114 | (85.1) | 67 | (58.8) | 47 | (41.2) | |
| Median (IQR) frequency | 1 (1) | 1 (1) | 1 (1) | ||||
| >median | 45 | (33.6) | 30 | (66.7) | 15 | (33.3) | 0.45 |
| ≤median | 89 | (66.4) | 52 | (58.4) | 37 | (41.6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sawitri, A.A.S.; Sutarsa, I.N.; Merati, K.T.P.; Bakta, I.M.; Wirawan, D.N. Why Counseling Intervention Fails to Improve Compliance towards Antiretroviral Therapy: Findings from a Mixed-Methods Study among People Living with HIV in Bali Province, Indonesia. Infect. Dis. Rep. 2021, 13, 136-147. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010015
Sawitri AAS, Sutarsa IN, Merati KTP, Bakta IM, Wirawan DN. Why Counseling Intervention Fails to Improve Compliance towards Antiretroviral Therapy: Findings from a Mixed-Methods Study among People Living with HIV in Bali Province, Indonesia. Infectious Disease Reports. 2021; 13(1):136-147. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010015
Chicago/Turabian StyleSawitri, Anak Agung Sagung, I Nyoman Sutarsa, Ketut Tuti Parwati Merati, I Made Bakta, and Dewa Nyoman Wirawan. 2021. "Why Counseling Intervention Fails to Improve Compliance towards Antiretroviral Therapy: Findings from a Mixed-Methods Study among People Living with HIV in Bali Province, Indonesia" Infectious Disease Reports 13, no. 1: 136-147. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010015