
Antibiotic Susceptibilities of Enterococcus Species Isolated from Hospital and Domestic Wastewater Effluents in Alice, Eastern Cape Province of South Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
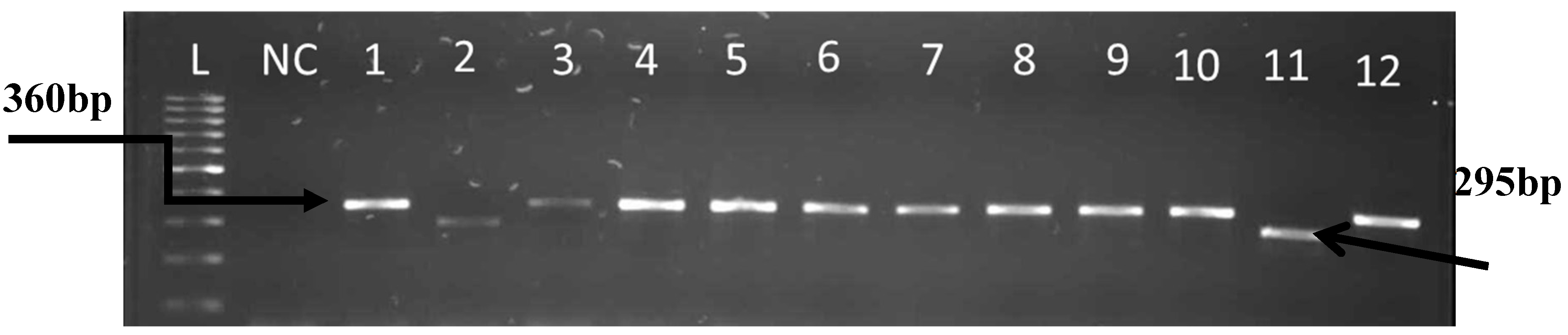
2.1.1. Isolation, Identification, DNA Extraction and Molecular Confirmation and Speciation of Enterococcus spp.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strain | Primer | Sequence (5’–3’) | Product Size(bp) | Ref. |
|---|---|---|---|---|
| E.faecalis ATCC 19433 | FL1 FL2 | ACTTATGTGACTAACTTAACC TAATGGTGAATCTTGGTTTGG | 360 | [11] |
| E.durans ATCC 19432 | DU1 DU2 | CCTACTGATATTAAGACAGCG TAATCCTAAGATAGGTGTTTG | 295 | [11] |
| E.casseliflavus ATCC 25788 | CA1 CA2 | TCCTGAATTAGGTGAAAAAAC GCTAGTTTACCGTCTTTAACG | 288 | [11] |
| E.faecium ATCC19434 | FM1FM2 | GAAAAAACAATAGAAGAATTAT TGCTTTTTTGAATTCTTCTTTA | 215 | [11] |
| E.hirae ATCC 8043 | HI1 HI2 | CTTTCTGATATGGATGCTGTC TAAATTCTTCCTTAAATGTTG | 187 | [11] |
2.1.2. Detection of Virulence Genes
| Gene and Primers | Sequence | Product Size (bp) | Ref. |
|---|---|---|---|
| ace | 320 | [24] | |
| ACE1 | 5’-AAAGTAGAATTAGATCCACAC-3’ | ||
| aceACE1ACE2 | 5’-TCTATCACATTCGGTTGCG-3’ | ||
| gelE | 402 | [24] | |
| gelE1 | 5’-AGTTCATGTCTATTTTCTTCAC-3’ | ||
| gelE2 | 5’-CTTCATTATTTACACGTTTG-3’ | ||
| efaA | 499 | [24] | |
| efaA1 | 5’-CGTGAGAAAGAAATGGAGGA-3’ | ||
| efaA2 | 5’-CTACTAACACGTCACGAATG-3’ | ||
| esp | 913 | [25] | |
| ESP46 | 5’-TTACCAAGATGGTTCTGTAGGCAC-3’ | ||
| ESP47 | 5’-CCAAGTATACTTAGCATCTTTTGG-3’ | ||
| hyl | 276 | [25] | |
| HYL n1 | 5’-ACAGAAGAGCTGCAGGAAATG-3’ | ||
| HYL n2 | 5’-GACTGACGTCCAAGTTTCCAA-3’ | ||
| cylA | 688 | [25] | |
| CYT I | 5’-ACTCGGGGATTGATAGGC-3’ | ||
| CYT II | 5’-GCTGCTAAAGCTGCGCTT-3’ |
2.2. Antimicrobial Susceptibility Testing
PCR Detection of vanA, vanB, vanC1, vanC2/3 and erm(B) Genes
| Gene(s) | Product Size (bp) | Primer Name Oligonucleotide Sequences (5’ to 3’) | Ref. |
|---|---|---|---|
| vanA | 314 | AF-GCGCGGTCCACTTGTAGATA | [29] |
| AR-TGAGCAACCCCCAAACAGTA | |||
| vanB | 220 | BF-AGACATTCCGGTCGAGGAAC | [29] |
| BR-GCTGTCAATTAGTGCGGGAA | |||
| vanC-1 | 402 | C1F-ATCCAAGCTATTGACCCGCT | [29] |
| C1R-TGTGGCAGGATCGTTTTCAT | |||
| vanC-2/3 | 582 | C2F-CTAGCGCAATCGAAGCACTC | [29] |
| erm(B) | 320 | C2R-GTAGGAGCACTGCGGAACAA | [30] |
| BN1-CGAGTGAAAAAGTACTCAACCA | |||
| BN2-CGGTGAATATCCAAGGTACG |
3. Results
3.1. Identification of Enterococcus to Species Level
3.2. Identification of Virulent Genes



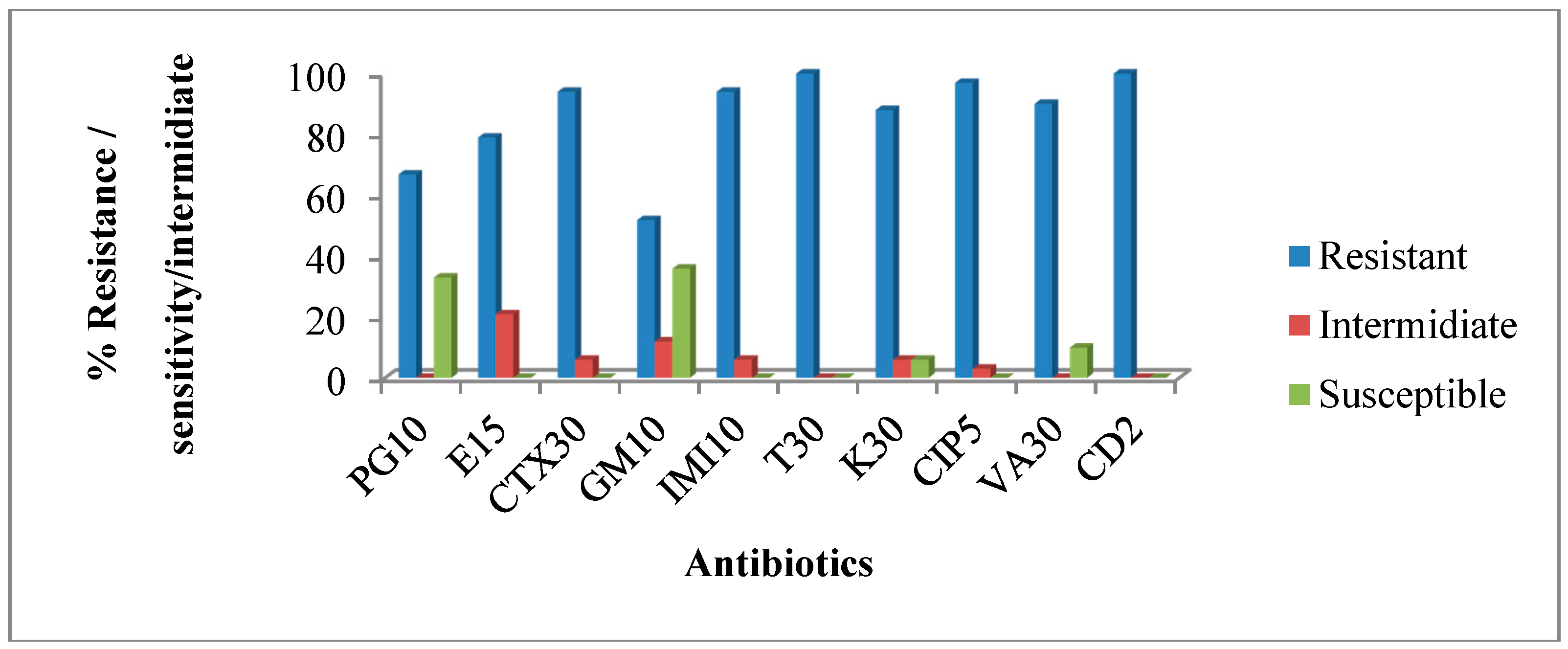
3.3. Antimicrobial Susceptibility Profile of Confirmed Enterococcus Isolates from Hospital Wastewater

| No. of Isolates | Phenotypic Multiple Resistance Patterns |
|---|---|
| 16 | PG/E/CTX/GM/IMI/T/K/CIP/VA/CD |
| 6 | PG/E/CTX /IMI/T/K/CIP/VA/CD |
| 7 | E/CTX /IMI/T/K/CIP/VA/CD |
| 4 | E/CTX/GM/IMI/T/K/CIP/CD |
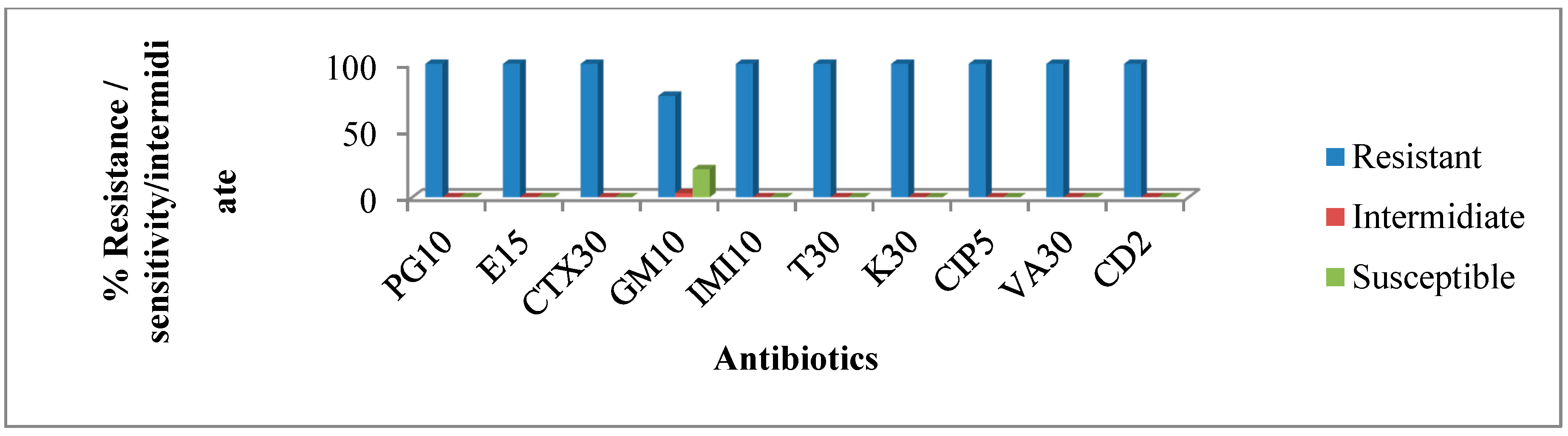
3.4. Antimicrobial Susceptibility Profile of Confirmed Enterococcus Isolates from the Final Effluent of Wastewater Treatment Plant.

| Total No. of Isolates | Resistance Pattern of The Isolates |
|---|---|
| 23 | PG/E/CTX/GM/IMI/T/K/CIP/VA/CD |
| 6 | E/CTX /IMI/T/K/CIP/VA/CD |
3.5. Detection of Antimicrobials Resistance Genes from Confirmed Enterococcus Isolates
| Antibiotic | Class | Resistance Gene | No. of Strain |
|---|---|---|---|
| Erythromycin | Macrolide | erm(B) | 40 (88.8%) |
| Vancomycin | Glycopeptide | vanB, vanC1, van C2/3 | 42 (93.3%) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Periasamy, D.; Sundaram, A. Environmental health A novel approach for pathogen reduction in wastewater treatment. J. Environ. Health Sci. Eng. 2013. [Google Scholar] [CrossRef]
- Alam, M.Z.; Aqil, F.; Ahmad, I.; Ahmad, S. Incidence and transferability of antibiotic resistance in the enteric bacteria isolated from hospital wastewater. Braz. J. Microbiol. 2013, 44, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Novo, A.; Manaia, C.M. Factors influencing antibiotic resistance burden in municipal wastewater treatment plants. Appl. Microbiol. Biotechnol. 2010, 87, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Baquero, F.; Martinez, J.L.; Canton, R. Antibiotics and antibiotic resistance in water environments. Curr. Opin. Biotechnol. 2008, 19, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Kemper, N. Veterinary antibiotics in the aquatic and terrestrial environment. Ecol. Indic. 2008, 8, 1–13. [Google Scholar] [CrossRef]
- Kümmerer, K. The presence of pharmaceuticals in the environment due to human use—Present knowledge and future challenges. J. Environ. Manage. 2009, 90, 2354–2366. [Google Scholar] [CrossRef] [PubMed]
- Byappanahalli, M.N.; Meredith, B.; Asja, K.; Zachery, R.S.; Valerie, J.H. Enterococci in the environment. Microbiol. Mol. Biol. Rev. 2012, 76, 685–706. [Google Scholar] [CrossRef] [PubMed]
- Kaltenthaler, E.C.; Pinfold, J.V. Microbiological methods for assessing hand washing practice in hygiene behaviour studies. J. Trop. Med. Hyg. 1995, 98, 101–106. [Google Scholar]
- Ashbolt, N.J.; Grabow, W.O.K.; Snozzi, M. Indicators of microbial water quality. In Water Quality: Guidelines, Standards and Health; Fewtrell, L., Bartram, J., Eds.; IWA Publishing: London, UK, 2001. [Google Scholar]
- Fernandes, S.C.; Dhanashree, B. Drug resistance & virulence determinants in clinical isolates of enterococcus species. Indian J. Med. Res. 2013, 137, 981–985. [Google Scholar] [PubMed]
- Jackson, C.R.; Fedorka-Cray, P.J.; Barrett, J.B. Use of a genus- and species-specific multiplex PCR for identification of enterococci. J. Clin. Microbiol. 2004, 42, 3558–3565. [Google Scholar] [CrossRef] [PubMed]
- Kafil, H.S.; Mobarez, A.M.; Moghadam, M.F. Multidrug resistant and most virulent Enterococcus faecium (strain 2653), isolated from hospitalized patient wound in Iran. Scholarly J. Med. 2012, 2, 36–39. [Google Scholar]
- Doğru, A.K.; Gençay, Y.E.; Ayaz, N.D. Comparison of Virulence Gene Profiles of Enterococcus faecium and Enterococcus faecalis Chicken Neck Skin and Faeces Isolates。. Kafkas Univ Vet Fak Derg 2010, 16 (Suppl-A), S129–S133. [Google Scholar] [CrossRef]
- Comerlato, C.B.; Resende, M.C.; Caierão, J.; d’Azevedo, P.A. Presence of virulence factors in Enterococcus faecalis and Enterococcus faecium susceptible and resistant to vancomycin. Mem. Inst. Oswaldo. Cruz. 2013, 108, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, A.W.; Pereira, R.I.; Oliveira, D.V.; Martins, P.D.; d’Azevedo, P.A.; van der Sand, S.; Frazzon, J.; Frazzon, A.P.G. Molecular detection of virulence factors among food and clinical Enterococcus faecalis strains in south Brazil. Braz. J. Microbiol. 2014, 332, 327–332. [Google Scholar] [CrossRef]
- Boyd, D.A.; Willey, B.M.; Fawcett, D.; Gillani, N.; Mulvey, M.R. Molecular characterization of Enterococcus faecalis N06-0364 with low-level vancomyc in resistance harboring a novel D-Ala-D-Ser gene cluster, vanL. Antimicrob. Agents Chemother. 2008, 52, 2667–2672. [Google Scholar] [CrossRef] [PubMed]
- Courvalin, P. Vancomycin resistance in gram-positive cocci. Clin. Infect. Dis. 2006, 42, 25–34. [Google Scholar] [CrossRef]
- Lebreton, F.; Depardieu, F.; Bourdon, N. D-Ala-D-SerVanN-type transferable vancomycin resistance in Enterococcus faecium. Antimicrob. Agents Chemother. 2011, 55, 4606–4612. [Google Scholar] [CrossRef] [PubMed]
- Murray, B.E.; Nannini, E.C. Glycopeptides (vancomycin and teicoplanin), streptogramins (quinupristin-dalfopristin), and lipopeptides (daptomycin). In Principles and Practice of Infectious Diseases, 7th ed.; Mandell, G.L., Bennet, J.E., Dolin, R., Eds.; Churchill Livingstone: Philadelphia, PA, USA, 2010. [Google Scholar]
- Murray, B.E. Diversity among multidrug-resistant enterococci. Emerg. Infect Dis. 1998, 4, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, L.M.; Carvalho, M.G.S.C.; Facklam, R.R. Enterococcus. In Manual of Clinical Microbiology, 9th ed.; Murray, P.R., Baron, E.J., Jorgensen, J.H., Landry, M.L., Pfaller, M.A., Eds.; ASM Press: Washington, DC, USA, 2007. [Google Scholar]
- Bai, J.; Paddock, Z.D.; Shi, X.; Li, S.; An, B.; Nagaraja, T.G. Applicability of a multiplex PCR to detect the seven major shiga toxin—Producing escherichia coli based on genes that code for serogroup-specific o-antigens and major virulence factors in cattle feces. Foodborne Pathog. Dis. 2012, 9, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Ke, D.; Picard, F.J.; Martineau, F.; Menard, C.; Roy, P.H.; Ouellette, M.; Bergeron, M.G. Development of a PCR assay for rapid detection of enterococci. J. Clin. Microbiol. 1999, 37, 3497–3503. [Google Scholar] [PubMed]
- Mannu, L.; Paba, A.; Daga, E.; Comunian, R.; Zanetti, S.; Duprè, I.; Sechi, L. Comparison of the incidence of virulence determinants and antibiotic resistance between Enterococcus faecium strains of dairy, animal and clinical origin. Int. J. Food Microbiol. 2007, 88, 291–304. [Google Scholar] [CrossRef]
- Vankerckhoven, V.; Autgaerden, T.V.; Vael, C.; Lammens, C.; Chapelle, S.; Rossi, R.; Jabes, D.; Goossens, H. Development of a multiplex PCR for the detection of asa1, gelE, cylA, esp, and hyl genes in enterococci and survey for virulence determinants among European hospital isolates of Enterococcus faecium. J. Clin. Microbiol. 2004, 42, 4473–4479. [Google Scholar] [CrossRef] [PubMed]
- Af Geijersstam, A.; Culak, R.; Molenaar, L.; Chattaway, M.; Røslie, E.; Peciuliene, V.; Haapasalo, M.; Shah, H.N. Comparative analysis of virulence determinants and mass spectral profiles of Finnish and Lithuanian endodontic Enterococcus faecalis isolates. Oral Microbiol. Immunol. 2007, 22, 87–94. [Google Scholar] [CrossRef]
- Manual on Antimicrobial Susceptibility Testing. http://www.asm.org/ccLibraryFiles/FILENAME/000000002484/Manual%20of%20Antimicrobial%20Susceptibility%20Testing.pdf (assessed on 13 April 2015).
- Performance Standards for Antimicrobial Susceptibility Testing; Twenty-Fourth Informational Supplement 2014. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2014.
- Nam, S.; Kim, M.J.; Park, C.; Park, J.G.; Lee, G.C. Detection and genotyping of vancomycinresistant Enterococcus spp. by multiplex polymerase chain reaction in Korean aquatic environmental samples. Int. J. Hyg. Environ. Health 2012, 216, 421–427. [Google Scholar]
- Okoh, A.I. Impact of discharged wastewater final effluent on the physicochemical qualities of a receiving watershed in a suburban community of the Eastern Cape province. Clean Soil Air Water 2009, 37, 938–944. [Google Scholar] [CrossRef]
- Poh, C.H.; Oh, H.M.L.; Tan, A.L. Epidemiology and clinical outcome of enterococcal bacteraemia in an acute care hospital. J. Infect. 2006, 52, 383–386. [Google Scholar] [CrossRef] [PubMed]
- Kenzaka, T.; Takamura, N.; Kumabe, A.; Takeda, K. A case of subacute infective endocarditis and blood access infection caused by Enterococcus. durans. BMC Infect. Dis. 2013. [Google Scholar] [CrossRef]
- Heim, S.; Lleo, M.M.; Bonato, B.; Guzman, C.A.; Canepari, P. The viable but nonculturable state and starvation are different stress responses of Enterococcus. faecalis, as determined by proteome analysis. J. Bacteriol. 2002, 184, 6739–6745. [Google Scholar] [CrossRef] [PubMed]
- Lleò, M.M.; Tafi, M.C.; Canepari, P. Nonculturable Enterococcus faecalis cells are metabolically active and capable of resuming active growth. Syst. Appl. Microbiol. 1998, 21, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Lleò, M.M.; Bonato, B.; Benedetti, D.; Canepari, P. Survival of Enterococcal species in aquatic environments. Fems. Microbiol. Ecol. 2005, 54, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Dupre, I.; Zanetti, S.; Schito, A.M.; Fadda, G.; Sechi, L.A. Incidence of virulence determinants in clinical Enterococcus faecium and Enterococcus faecalis isolates collected in Sardinia (Italy). J. Med. Microbiol. 2005, 52, 491–498. [Google Scholar] [CrossRef]
- Yousif, N.M.K.; Dawyndt, P.; Abriouel, H.; Wijaya, A.; Schillinger, U.; Vancanneyt, M.; Swings, J.; Dirar, H.A.; Holzapfel, W.H.; Franz, C.M.A.P. Molecular characterization, technological properties and safety aspects of enterococci from Hussuwa, an African fermented sorghum product. J. Appl. Microbiol. 2005, 98, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Abriouel, H.; Ben Omar, N.; Molinos, A.C.; Lo’ pez, R.L.; Grande, M.J.; Martı’nez Viedma, P.; Ortega, E.; Can’amero, M.M.; Ga’lvez, A. Comparative analysis of genetic diversity and incidence of virulence factors and antibiotic resistance among enterococcal populations from raw fruit and vegetable foods, water and soil, and clinical samples. Int. J. Food Microbiol. 2008, 123, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Kayaoglu, G.; Ørstavik, D. Virulence factors of enterococcus faecalis: Relationship to endodontic disease. Crit. Rev. Oral. Biol. Med. 2004, 15, 308–20. [Google Scholar] [CrossRef] [PubMed]
- Sedgley, C.M.; Molander, A.; Flannagan, S.E.; Nagel, A.C.; Appelbe, O.K.; Clewell, D.B.; Dahlén, G. Virulence, phenotype and genotype characteristics of endodontic Enterococcus spp. Oral Microbiol. Immunol. 2005, 20, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Reinthaler, F.F.; Posch, J.; Feierl, G.; Wüst, G.; Haas, D.; Ruckenbauer, G.; Mascher, F.; Marth, E. Antibiotic resistance of E. coli in sewage and sludge. Water Res. 2006, 37, 1685–1690. [Google Scholar] [CrossRef]
- Kümmerer, K. Resistance in the environment. J. Antimicrob. Chemother. 2004, 54, 311–320. [Google Scholar] [CrossRef]
- Martinez, J.L. Environmental pollution by antibiotics and by antibiotic resistance determinants. Environ. Pollut. 2009, 157, 2893–2902. [Google Scholar] [CrossRef] [PubMed]
- Czekalskiet, N.; Berthold, T.; Caucci, S.; Egli, A.; Bürgmann, H. Increased levels of multiresistant bacteria and resistance genes after wastewater treatment and their dissemination into Lake Geneva, Switzerland. Front. Micro. 2012. [Google Scholar] [CrossRef]
- Isogai, N.; Urushibara, N.; Kawaguchiya, M.; Ghosh, S.; Suzaki, K.; Watanabe, N.; Quiñones, D.; Kobayashi, N. Characterization of Enterococcus faecium with macrolide resistance and reduced susceptibility to quinupristin/dalfopristin in a Japanese hospital: Detection of extensive diversity in erm(B)-regulator regions. Microb. Drug Resist. 2013, 19, 298–307. [Google Scholar]
- Moges, F.; Endris, M.; Belyhun, Y.; Worku, W. Isolation and characterization of multiple drug resistance bacterial pathogens from waste water in hospital and non-hospital environments , northwest Ethiopia. BMC Res. Notes 2014, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Borhani, B.; Ahmadi, A; Rahimi, F.; Pourshafie, M.R.; Talebi, M. Determination of vancomycin resistant Enterococcus. Faecium diversity in tehran sewage using plasmid profile, biochemical fingerprinting and antibiotic resistance. Jundishapur. J. Microbiol. 2014. [Google Scholar] [CrossRef]
- Da Silva, M.F.; Tiago, I.; Verissimo, A.; Boaventura, R.A.R.; Nunes, O.C.; Manaia, C.M. Antibiotic resistance of Enterococci and related bacteria in an urban wastewater treatment plant. FEMS Microbiol. Ecol. 2006, 55, 322–329. [Google Scholar] [CrossRef]
- Da Costa, P.M.M.; Vaz-Pires, P.M.; Bernardo, F.M. Antimicrobial resistance in Enterococci spp. isolated from wastewater isolated in inflow, effluent and sludge from municipal sewage water treatment plants. Water Res. 2006, 40, 1735–1740. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Ying, G.G.; Liu, S.; Zhao, J.L.; Yang, B.; Chen, Z.F.; Lai, H.J. Occurrence and fate of eleven classes of antibiotics in two typical wastewater treatment plants in south China. Sci. Total Envirion. 2013, 452–453, 365–376. [Google Scholar] [CrossRef]
- Akiyama, T.; Savin, M.C. Populations of antibiotic-resistant coliform bacteria change rapidly in a wastewater ef fluent dominated stream. Sci. Total Envir. 2010, 408, 6192–6201. [Google Scholar] [CrossRef]
- Gao, L.; Shi, Y.; Li, W.; Niu, H.; Liu, J.; Cai, Y. Occurrence of antibiotics in eight sewage treatment plants in Beijing, China. Chemosphere 2010, 86, 665–671. [Google Scholar] [CrossRef]
- Gibs, J.; Heckathorn, H.A.; Meyer, M.T.; Klapinski, F.R.; Alebus, M.; Lippincott, R.L. Occurrence and partitioning of antibiotic compounds found in the water column and bottom sediments from a stream receiving two wastewater treatment plant ef fluents in Northern New Jersey, 2008. Sci. Total. Envirion. 2013, 458–460, 107–116. [Google Scholar] [CrossRef]
- Silva, J.; Castillo, G.; Callejas, L.; López, H.; Olmos, J. Frequency of transferable multiple antibiotic resistance amongst coliform bacteria isolated from a treated sewage effluent in Antofagasta, Chile. Electron. J. Biotechnol 2006, 9, 533–540. [Google Scholar] [CrossRef]
- Sujatha, S.; Praharaj, I. Glycopeptide resistance in gram-positive cocci: A review. Interdiscip. Perspect. Infect. Dis. 2012. [Google Scholar] [CrossRef]
- Sahin, I.; Kaya, D.; Oksuz, S.; Okay, A.; Sencan, I.; Ozturk, E. The frequency of extened spectrum beta lactamase and antibiotic susceptibility in clinical isolates of gram negative bacilli. Infeksiyon Dergisi 2003, 17, 45–48. [Google Scholar]
- Lupo, A.; Coyne, S.; Berendonk, T.U. Origin and evolution of antibiotic resistance: The common mechanisms of emergence and spread in water bodies. Front. Microbiol. 2012. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iweriebor, B.C.; Gaqavu, S.; Obi, L.C.; Nwodo, U.U.; Okoh, A.I. Antibiotic Susceptibilities of Enterococcus Species Isolated from Hospital and Domestic Wastewater Effluents in Alice, Eastern Cape Province of South Africa. Int. J. Environ. Res. Public Health 2015, 12, 4231-4246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404231
Iweriebor BC, Gaqavu S, Obi LC, Nwodo UU, Okoh AI. Antibiotic Susceptibilities of Enterococcus Species Isolated from Hospital and Domestic Wastewater Effluents in Alice, Eastern Cape Province of South Africa. International Journal of Environmental Research and Public Health. 2015; 12(4):4231-4246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404231
Chicago/Turabian StyleIweriebor, Benson Chuks, Sisipho Gaqavu, Larry Chikwelu Obi, Uchechukwu U. Nwodo, and Anthony I. Okoh. 2015. "Antibiotic Susceptibilities of Enterococcus Species Isolated from Hospital and Domestic Wastewater Effluents in Alice, Eastern Cape Province of South Africa" International Journal of Environmental Research and Public Health 12, no. 4: 4231-4246. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph120404231