
The Urban-Rural Gradient In Asthma: A Population-Based Study in Northern Europe

 and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Questionnaire Information
2.3. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Inner City | Suburb of City | Small Town | Village in Rural Area | Farm without Livestock | Farm with Livestock | Study Population | Eligible Subjects * | |
|---|---|---|---|---|---|---|---|---|
| Subjects, N | 1725 | 3337 | 2720 | 1599 | 250 | 1492 | 11,123 | 12,441 |
| Age in 2011, mean ± SD | 53.5 ± 7.1 | 52.0 ± 7.1 | 52.2 ± 7.0 | 54.14 ± 7.1 | 52.5 ± 6.7 | 55.6 ± 6.6 | 53.1 ± 7.1 | 53.0 ± 7.1 |
| Sex, N (%F) | 872 (51%) | 1765 (53%) | 1441 (53%) | 915 (57%) | 126 (50%) | 850 (57%) | 5969 (54%) | 6612 (53%) |
| Smoking status | ||||||||
| Current smoker, N (%) | 494 (29%) | 824 (24%) | 581 (21%) | 311 (20%) | 64 (26%) | 328 (22%) | 2602 (23%) | 2757 (22%) |
| Ex-smoker, N (%) | 409 (34%) | 822 (25%) | 647 (24%) | 428 (26%) | 60 (24%) | 348 (23%) | 2714 (24%) | 2842 (23%) |
| Never smokers, N (%) | 670 (39%) | 1378 (41%) | 1281 (47%) | 744 (47%) | 108 (43%) | 702 (47%) | 4883 (44%) | 5061 (41%) |
| Age at smoke start, mean ± SD | 16.9 ± 4.4 | 17.2 ± 4.3 | 17.4 ± 4.3 | 17.0 ± 4.1 | 17.3 ± 4.3 | 17.9 ± 4.9 | 17.3 ± 4.4 | 17.3 ± 4.4 |
| Parental smoking: | ||||||||
| No parents smoke, N (%) | 430 (25%) | 976 (29%) | 875 (32%) | 538 (34%) | 74 (30%) | 641 (43%) | 3534 (32%) | 3976 (32%) |
| One parent smoke, N (%) | 630 (37%) | 1284 (39%) | 942 (35%) | 623 (39%) | 95 (38%) | 597 (40%) | 4171 (38%) | 4637 (37%) |
| Both parents smoke, N (%) | 593 (34%) | 972 (29%) | 815 (30%) | 373 (23%) | 73 (29%) | 193 (13%) | 3019 (27%) | 3343 (27%) |
| Don’t know, N (%) | 72 (4%) | 105 (3%) | 88 (3%) | 65 (4%) | 8 (3%) | 61 (4%) | 399 (4%) | 462 (4%) |
| Body silhouette at 8y | ||||||||
| 1–3 (lean), N (%) | 1422 (82%) | 2742 (82%) | 2203 (81%) | 1312 (82%) | 211 (84%) | 1194 (80%) | 9084 (82%) | 9743 (78%) |
| 4–6 (normal), N (%) | 281 (16%) | 552 (17%) | 479 (18%) | 269 (17%) | 37 (15%) | 269 (18%) | 1887 (17%) | 1996 (16%) |
| 7–9 (obese), N (%) | 22 (1%) | 43 (1%) | 38 (1%) | 18 (1%) | 2 (1%) | 29 (2%) | 152 (1%) | 159 (1%) |
| Centre | ||||||||
| Aarhus (DK), N (%) | 351 (20%) | 600 (18%) | 475 (17%) | 271 (17%) | 26 (11%) | 229 (15%) | 1952 (18%) | 2182 (18%) |
| Reykjavik (IS), N (%) | 297 (17%) | 664 (20%) | 454 (17%) | 68 (4%) | 20 (8%) | 131 (9%) | 1634 (15%) | 1862 (15%) |
| Bergen (NO), N (%) | 343 (20%) | 580 (17%) | 488 (18%) | 79 (5%) | 131 (52%) | 231 (15%) | 1852 (17%) | 2050 (16%) |
| Gothenburg (SE), N (%) | 256 (15%) | 660 (20%) | 235 (9%) | 185 (12%) | 15 (6%) | 95 (6%) | 1446 (13%) | 1631 (13%) |
| Umeaa (SE), N (%) | 94 (5%) | 137 (4%) | 464 (17%) | 499 (31%) | 28 (11%) | 432 (29%) | 1654 (15%) | 1840 (15%) |
| Uppsala (SE), N (%) | 256 (15%) | 380 (11%) | 462 (17%) | 375 (23%) | 24 (10%) | 192 (13%) | 1689 (15%) | 1859 (15%) |
| Tartu (EE), N (%) | 128 (7%) | 316 (9%) | 142 (5%) | 122 (8%) | 6 (2%) | 182 (12%) | 896 (8%) | 1017 (8%) |
| Parental asthma | ||||||||
| Mother, N (%) | 144 (8%) | 280 (8%) | 208 (8%) | 120 (8%) | 23 (9%) | 123 (8%) | 898 (8%) | 1021 (8%) |
| Father, N (%) | 80 (5%) | 162 (5%) | 125 (5%) | 87 (5%) | 17 (7%) | 78 (5%) | 549 (5%) | 615 (5%) |
| No parental asthma, N (%) | 1492 (86%) | 2873 (86%) | 2379 (87%) | 1378 (86) | 208 (83%) | 1282 (86%) | 9612 (86%) | 9292 (75%) |
| Both parents asthma, N (%) | 9 (1%) | 22 (1%) | 8 (1%) | 14 (1%) | 2 (1%) | 9 (1%) | 64 (1%) | 70 (1%) |
| Hay fever | ||||||||
| Yes, N (%) | 466 (27%) | 805 (24%) | 706 (26%) | 364 (23%) | 55 (22%) | 301 (20%) | 2697 (24%) | 2998 (24%) |


| Inner City | Suburb of City | Small Town | Village in Rural Area | Farm without Livestock | Farm with Livestock | HR for Urban-Rural Trend “ | p for Urban-Rural Trend | |
|---|---|---|---|---|---|---|---|---|
| Cases with asthma N (%) | 194 (11%) | 334 (10%) | 334 (12%) | 167 (10%) | 27 (11%) | 125 (8%) | ||
| Incidence of asthma per 1000 pyr (95% CI) | 2.25 (1.95–2.59) | 2.06 (1.85–2.29) | 2.55 (2.29–2.84) | 2.07 (1.78–2.41) | 2.22 (1.52–3.24) | 1.59 (1.34–1.90) | ||
| Mean age of asthma onset ± SD | 26.6 ± 15.8 | 24.5 ± 15.6 | 23.6 ± 16.4 | 24.9 ± 17.6 | 22.1 ± 17.3 | 27.3 ± 17.9 | ||
| Cases with wheeze N (%) | 368 (21%) | 628 (19%) | 541 (20%) | 288 (18%) | 47 (19%) | 261 (17%) | ||
| All | ||||||||
| Crude | 1 | 0.91 (0.76–1.09) | 1.13 (0.95–1.35) | 0.92 (0.75–1.13) | 0.98 (0.66–1.47) | 0.71 (0.57–0.89) | 0.95 (0.92–0.99) | 0.01 |
| Adjusted 1 ° | 1 | 0.87 (0.73–1.04) | 1.03 (0.86–1.23) | 0.90 (0.72–1.11) | 0.83 (0.55–1.24) | 0.71 (0.56–0.89) | 0.95 (0.91–0.99) | 0.01 |
| Adjusted 2 * | 1 | 0.88 (0.73–1.05) | 1.04 (0.87–1.24) | 0.90 (0.73–1.12) | 0.83 (0.56–1.25) | 0.72 (0.57–0.91) | 0.95 (0.92–0.99) | 0.02 |
| Inner City | Suburb of City | Small Town | Village in Rural Area | Farm without Livestock | Farm with Livestock | HR for Urban-Rural Trend “ | p for Urban-Rural Trend | |
|---|---|---|---|---|---|---|---|---|
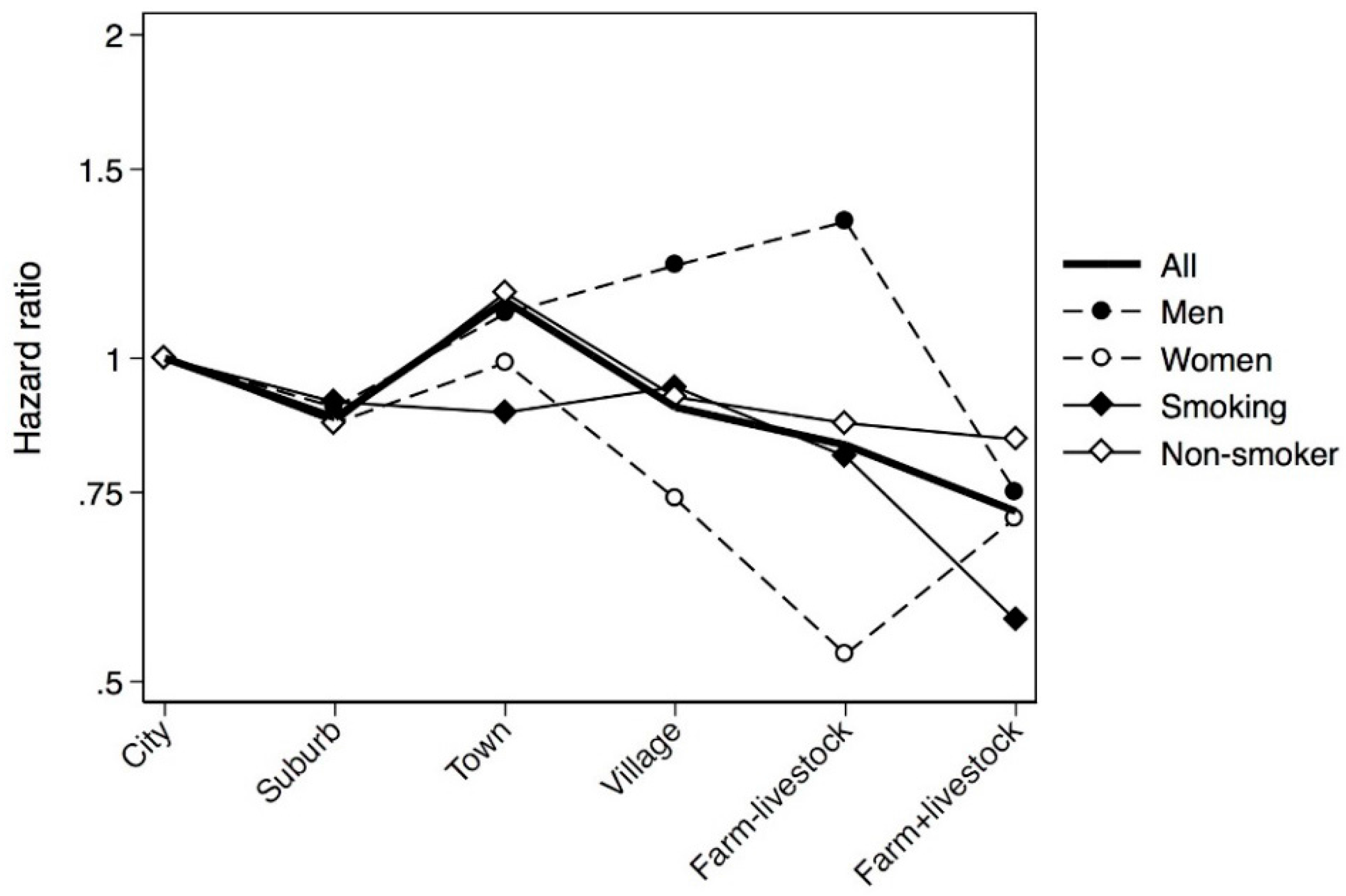
| Men | ||||||||
| Crude | 1 | 0.90 (0.68–1.20) | 1.20 (0.91–1.59) | 1.17 (0.85–1.61) | 1.60 (0.95–2.70) | 0.70 (0.48–1.02) | 0.98 (0.93–1.04) | 0.62 |
| Adjusted 1 ° | 1 | 0.90 (0.67–1.19) | 1.11 (0.83–1.47) | 1.22 (0.88–1.71) | 1.34 (0.79–2.28) | 0.75 (0.51–1.10) | 0.99 (0.93–1.06) | 0.77 |
| Adjusted 2 * | 1 | 0.90 (0.67–1.19) | 1.10 (0.83–1.46) | 1.22 (0.87–1.71) | 1.34 (0.79–2.28) | 0.75 (0.51–1.11) | 0.99 (0.93–1.06) | 0.81 |
| Women | ||||||||
| Crude | 1 | 0.90 (0.72–1.13) | 1.07 (0.85–1.34) | 0.76 (0.58–0.99) | 0.59 (0.31–1.12) | 0.69 (0.52–0.91) | 0.93 (0.88–0.97) | <0.01 |
| Adjusted 1 ° | 1 | 0.86 (0.69–1.08) | 0.97 (0.77–1.22) | 0.73 (0.55–0.97) | 0.52 (0.27–0.99) | 0.68 (0.51–0.91) | 0.93 (0.88–0.97) | <0.01 |
| Adjusted 2 * | 1 | 0.87 (0.70–1.10) | 0.99 (0.79–1.25) | 0.74 (0.56–0.98) | 0.53 (0.27–1.00) | 0.71 (0.53–0.94) | 0.93 (0.88–0.98) | <0.01 |
| Smoking | ||||||||
| Crude | 1 | 0.96 (0.72–1.26) | 0.93 (0.70–1.25) | 0.90 (0.65–1.26) | 0.96 (0.50–1.86) | 0.59 (0.40–0.87) | 0.92 (0.86–0.98) | 0.01 |
| Adjusted 1 ° | 1 | 0.90 (0.69–1.19) | 0.88 (0.66–1.19) | 0.94 (0.66–1.33) | 0.80 (0.41–1.56) | 0.58 (0.39–0.86) | 0.92 (0.86–0.98) | 0.02 |
| Adjusted 2 * | 1 | 0.91 (0.69–1.19) | 0.89 (0.66–1.19) | 0.94 (0.66–1.33) | 0.81 (0.42–1.58) | 0.57 (0.38–0.85) | 0.92 (0.86–0.98) | 0.01 |
| Not smoking | ||||||||
| Crude | 1 | 0.89 (0.70–1.12) | 1.26 (1.01–1.57) | 0.95 (0.73–1.23) | 1.01 (0.61–1.68) | 0.80 (0.60–1.06) | 0.98 (0.93–1.02) | 0.28 |
| Adjusted 1 ° | 1 | 0.87 (0.69–1.09) | 1.14 (0.91–1.43) | 0.91 (0.69–1.20) | 0.85 (0.51–1.43) | 0.82 (0.61–1.10) | 0.97 (0.93–1.02) | 0.29 |
| Adjusted 2 * | 1 | 0.87 (0.69–1.10) | 1.15 (0.92–1.45) | 0.92 (0.70–1.21) | 0.87 (0.51–1.45) | 0.84 (0.63–1.12) | 0.98 (0.93–1.03) | 0.39 |
| Inner City | Suburb of City | Small Town | Village in Rural Area | Farm without Livestock | Farm with Livestock | HR for Urban-Rural Trend “ | p for Urban-Rural Trend | |
|---|---|---|---|---|---|---|---|---|
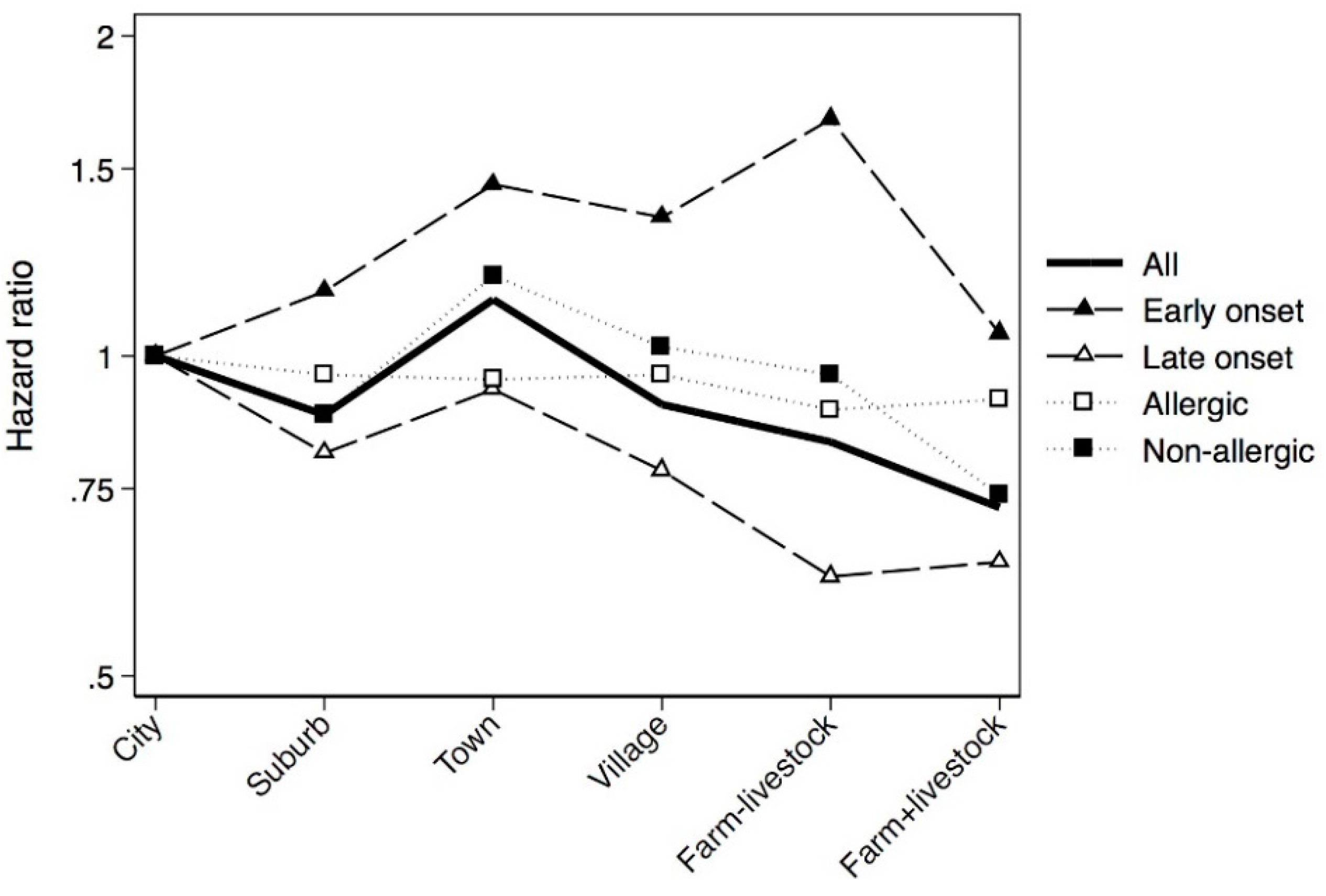
| Early onset (≤10 years of age) | ||||||||
| Crude | 1 | 1.14 (0.78–1.65) | 1.56 (1.08–2.25) | 1.43 (0.95–2.16) | 1.91 (0.98–3.73) | 0.98 (0.62–1.55) | 1.02 (0.95–1.09) | 0.58 |
| Adjusted 1 ° | 1 | 1.15 (0.79–1.68) | 1.44 (1.00–2.09) | 1.34 (0.88–2.04) | 1.65 (0.84–3.23) | 1.03 (0.65–1.64) | 1.02 (0.95–1.10) | 0.61 |
| Adjusted 2 * | 1 | 1.15 (0.79–1.68) | 1.45 (1.00–2.10) | 1.35 (0.89–2.06) | 1.67 (0.85–3.27) | 1.05 (0.65–1.68) | 1.02 (0.95–1.11) | 0.54 |
| Late onset (>10 years of age) | ||||||||
| Crude | 1 | 0.85 (0.70–1.04) | 1.02 (0.83–1.24) | 0.79 (0.62–1.00) | 0.74 (0.44–1.24) | 0.64 (0.50–0.83) | 0.93 (0.89–0.97) | <0.01 |
| Adjusted 1 ° | 1 | 0.80 (0.66–0.98) | 0.92 (0.75–1.13) | 0.78 (0.60–1.00) | 0.61 (0.36–1.02) | 0.63 (0.48–0.82) | 0.92 (0.88–0.97) | <0.01 |
| Adjusted 2 * | 1 | 0.81 (0.66–0.99) | 0.93 (0.76–1.15) | 0.78 (0.61–1.01) | 0.62 (0.37–1.04) | 0.64 (0.49–0.83) | 0.93 (0.88–0.97) | <0.01 |
| Allergic asthma | ||||||||
| Crude | 1 | 0.96 (0.76–1.22) | 1.06 (0.83–1.35) | 1.10 (0.83–1.45) | 1.00 (0.55–1.81) | 0.95 (0.70–1.29) | 1.00 (0.95–1.06) | 0.90 |
| Adjusted 1 ° | 1 | 0.96 (0.75–1.22) | 0.95 (0.74–1.21) | 0.96 (0.72–1.28) | 0.89 (0.49–1.63) | 0.90 (0.66–1.23) | 0.98 (0.93–1.04) | 0.52 |
| Adjusted 2 * | 1 | 0.96 (0.75–1.22) | 0.95 (0.75–1.22) | 0.96 (0.72–1.29) | 0.89 (0.49–1.63) | 0.91 (0.67–1.25) | 0.98 (0.93–1.04) | 0.59 |
| Non-allergic asthma | ||||||||
| Crude | 1 | 0.91 (0.70–1.20) | 1.25 (0.95–1.63) | 0.89 (0.65–1.22) | 1.13 (0.64–1.99) | 0.66 (0.48–0.94) | 0.95 (0.89–1.00) | 0.05 |
| Adjusted 1 ° | 1 | 0.87 (0.66–1.14) | 1.18 (0.90–1.55) | 1.01 (0.72–1.40) | 0.93 (0.52–1.66) | 0.72 (0.51–1.02) | 0.96 (0.91–1.02) | 0.21 |
| Adjusted 2 * | 1 | 0.88 (0.67–1.15) | 1.19 (0.91–1.56) | 1.02 (0.73–1.42) | 0.96 (0.54–1.70) | 0.74 (0.52–1.04) | 0.97 (0.91–1.03) | 0.28 |

4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wlasiuk, G.; Vercelli, D. The farm effect, or: When, what and how a farming environment protects from asthma and allergic disease. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.D.; Poole, J.A.; Romberger, D.J. Influence of farming exposure on the development of asthma and asthma-like symptoms. Int. Immunopharmacol. 2014, 23, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Ege, M.; Mayer, M. Exposure to environmental microorganisms and childhood asthma. N. Engl. J. Med. 2011, 364, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Tischer, C.; Casas, L.; Wouters, I.M.; Doekes, G.; Garcia-Esteban, R.; Gehring, U.; Hyvärinen, A.; Oldenwening, M.; Kerkhof, M.; Sunyer, J.; et al. Early exposure to bio-contaminants and asthma up to 10 years of age: Results of the HITEA study. Eur. Respir. J. 2014, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, A.M.; Hyvärinen, A.; Gehring, U.; Korppi, M.; Doekes, G.; Riedler, J.; Braun-Fahrländer, C.; Bitter, S.; Schmid, S.; Keski-Nisula, L.; et al. Exposure to microbial agents in house dust and wheezing, atopic dermatitis and atopic sensitization in early childhood: A birth cohort study in rural areas. Clin. Exp. Allergy 2012, 42, 1246–1256. [Google Scholar] [CrossRef] [PubMed]
- Smit, L.A.M.; Hooiveld, M.; van der Sman-de Beer, F.; Opstal-van Winden, A.W.J.; Beekhuizen, J.; Wouters, I.M.; Yzermans, C.J.; Heederik, D. Air pollution from livestock farms, and asthma, allergic rhinitis and COPD among neighbouring residents. Occup. Environ. Med. 2014, 71, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Omland, Ø.; Hjort, C.; Pedersen, O.F.; Miller, M.R.; Sigsgaard, T. New-onset asthma and the effect of environment and occupation among farming and nonfarming rural subjects. J. Allergy Clin. Immunol. 2011, 128, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Marks, G.B.; Mitakakis, T.Z.; Lëuppi, J.D.; Car, N.G.; Peat, J.K. Having lived on a farm and protection against allergic diseases in Australia. Clin. Exp. Allergy 2001, 31, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Riedler, J.; Braun-Fahrländer, C.; Eder, W.; Schreuer, M.; Waser, M.; Maisch, S.; Carr, D.; Schierl, R.; Nowak, D.; von Mutius, E.; et al. Exposure to farming in early life and development of asthma and allergy: A cross-sectional survey. Lancet 2001, 358, 1129–1133. [Google Scholar] [CrossRef]
- Adler, A.; Tager, I.; Quintero, D.R. Decreased prevalence of asthma among farm-reared children compared with those who are rural but not farm-reared. J. Allergy Clin. Immunol. 2005, 115, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Bråbäck, L.; Hjern, A.; Rasmussen, F. Trends in asthma, allergic rhinitis and eczema among Swedish conscripts from farming and non-farming environments. A nationwide study over three decades. Clin. Exp. Allergy 2004, 34, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Ege, M.J.; Frei, R.; Bieli, C.; Schram-Bijkerk, D.; Waser, M.; Benz, M.R.; Weiss, G.; Nyberg, F.; van Hage, M.; Pershagen, G.; et al. Not all farming environments protect against the development of asthma and wheeze in children. J. Allergy Clin. Immunol. 2007, 119, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Leynaert, B.; Neukirch, C.; Jarvis, D.; Chinn, S.; Burney, P.; Neukirch, F. Does living on a farm during childhood protect against asthma, allergic rhinitis, and atopy in adulthood? Am. J. Respir. Crit. Care Med. 2001, 164, 1829–1834. [Google Scholar] [CrossRef] [PubMed]
- Wegienka, G.; Zoratti, E.; Johnson, C.C. The role of the early-life environment in the development of allergic disease. Immunol. Allergy Clin. North Am. 2015, 35, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Timm, S.; Svanes, C.; Janson, C.; Sigsgaard, T.; Johannessen, A.; Gislason, T.; Jogi, R.; Omenaas, E.; Forsberg, B.; Torén, K.; et al. Place of upbringing in early childhood as related to inflammatory bowel diseases in adulthood: A population-based cohort study in Northern Europe. Eur. J. Epidemiol. 2014, 29, 429–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elholm, G.; Linneberg, A.; Husemoen, L.L.N.; Omland, Ø.; Grønager, P.M.; Sigsgaard, T.; Schlünssen, V. The Danish urban-rural gradient of allergic sensitization and disease in adults. Clin. Exp. Allergy 2015, 12. [Google Scholar] [CrossRef] [PubMed]
- Burney, P.; Chinn, S.; Jarvis, D.; Luczynska, C.; Lai, E. Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in the European Community Respiratory Health Survey (ECRHS). Eur. Respir. J. 1996, 9, 687–695. [Google Scholar]
- Johannessen, A.; Verlato, G.; Benediktsdottir, B.; Forsberg, B.; Franklin, K.; Gislason, T.; Holm, M.; Janson, C.; Jögi, R.; Lindberg, E.; et al. Longterm follow-up in European respiratory health studies—Patterns and implications. BMC Pulm. Med. 2014, 14, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svanes, C.; Dharmage, S.; Sunyer, J.; Zock, J.P.; Norbäck, D.; Wjst, M.; Heinrich, J.; Jarvis, D.; de Marco, R.; Plana, E.; et al. Long-term reliability in reporting of childhood pets by adults interviewed twice, 9 years apart. Results from the European Community Respiratory Health Survey i and II. Indoor Air 2008, 18, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Douwes, J.; Travier, N.; Huang, K.; Cheng, S.; McKenzie, J.; le Gros, G.; von Mutius, E.; Pearce, N. Lifelong farm exposure may strongly reduce the risk of asthma in adults. Allergy Eur. J. Allergy Clin. Immunol. 2007, 62, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Pekkanen, J.; Pearce, N. Defining asthma in epidemiological studies. Eur. Respir. J. 1999, 14, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Eagan, T.M.L.; Gulsvik, A.; Eide, G.E.; Bakke, P.S. Occupational airborne exposure and the incidence of respiratory symptoms and asthma. Am. J. Respir. Crit. Care Med. 2002, 166, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Torén, K.; Hermansson, B.A. Incidence rate of adult-onset asthma in relation to age, sex, atopy and smoking: A Swedish population-based study of 15813 adults. Int. J. Tuberc. Lung Dis. 1999, 3, 192–197. [Google Scholar] [PubMed]
- Torén, K.; Gislason, T.; Omenaas, E.; Jögi, R.; Forsberg, B.; Nyström, L.; Olin, A.-C.; Svanes, C.; Janson, C. A prospective study of asthma incidence and its predictors: The RHINE study. Eur. Respir. J. 2004, 24, 942–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rook, G.A.W. Hygiene and other early childhood influences on the subsequent function of the immune system. Dig. Dis. 2011, 29, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Lawson, J.A.; Janssen, I.; Bruner, M.W.; Madani, K.; Pickett, W. Urban-rural differences in asthma prevalence among young people in Canada: The roles of health behaviors and obesity. Ann. Allergy Asthma Immunol. 2011, 107, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Genuneit, J. Sex-specific development of asthma differs between farm and nonfarm children: A cohort study. Am. J. Respir. Crit. Care Med. 2014, 190, 588–590. [Google Scholar] [CrossRef] [PubMed]
- Vesterinen, E.; Kaprio, J.; Koskenvuo, M. Prospective study of asthma in relation to smoking habits among 14,729 adults. Thorax 1988, 43, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Eisner, M.D. Smoking and adult asthma—A healthy smoker effect? Am. J. Respir. Crit. Care Med. 2002, 165, 1566–1567. [Google Scholar] [CrossRef] [PubMed]
- Horak, E.; Morass, B.; Ulmer, H.; Genuneit, J.; Braun-Fahrländer, C.; von Mutius, E. Prevalence of wheezing and atopic diseases in Austrian schoolchildren in conjunction with urban, rural or farm residence. Wien. Klin. Wochenschr. 2014, 126, 532–536. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, S.J.; Sozanska, B.; Danielewicz, H.; Debinska, A.; Kosmeda, A.; Boznanski, A.; Illi, S.; Depner, M.; Strunz-Lehner, C.; Waser, M.; et al. Asthma and allergies: Is the farming environment (still) protective in Poland? the GABRIEL Advanced Studies. Allergy Eur. J. Allergy Clin. Immunol. 2013, 68, 771–779. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timm, S.; Frydenberg, M.; Janson, C.; Campbell, B.; Forsberg, B.; Gislason, T.; Holm, M.; Jogi, R.; Omenaas, E.; Sigsgaard, T.; et al. The Urban-Rural Gradient In Asthma: A Population-Based Study in Northern Europe. Int. J. Environ. Res. Public Health 2016, 13, 93. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010093
Timm S, Frydenberg M, Janson C, Campbell B, Forsberg B, Gislason T, Holm M, Jogi R, Omenaas E, Sigsgaard T, et al. The Urban-Rural Gradient In Asthma: A Population-Based Study in Northern Europe. International Journal of Environmental Research and Public Health. 2016; 13(1):93. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010093
Chicago/Turabian StyleTimm, Signe, Morten Frydenberg, Christer Janson, Brittany Campbell, Bertil Forsberg, Thorarinn Gislason, Mathias Holm, Rain Jogi, Ernst Omenaas, Torben Sigsgaard, and et al. 2016. "The Urban-Rural Gradient In Asthma: A Population-Based Study in Northern Europe" International Journal of Environmental Research and Public Health 13, no. 1: 93. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010093