
Geographical Inequalities in Surgical Treatment for Localized Female Breast Cancer, Queensland, Australia 1997–2011: Improvements over Time but Inequalities Remain

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Treatment and Comorbidities
2.1.1. Surgical Procedures
2.1.2. Hospital Type
2.1.3. Comorbidities
2.2. Geographical
2.3. Analyses
3. Results
3.1. Cohort Characteristics
3.2. Associations with Likelihood of Having BCS
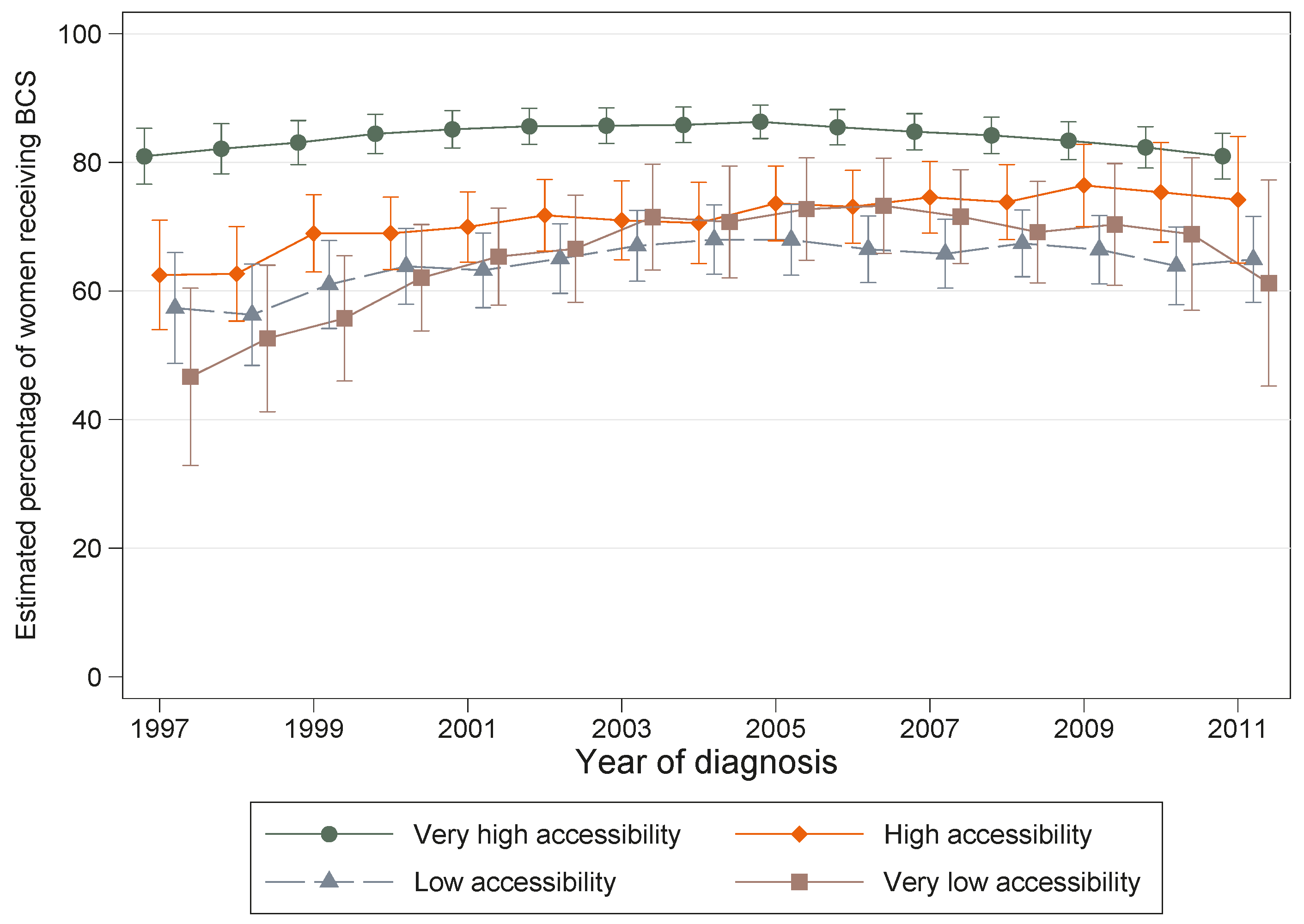
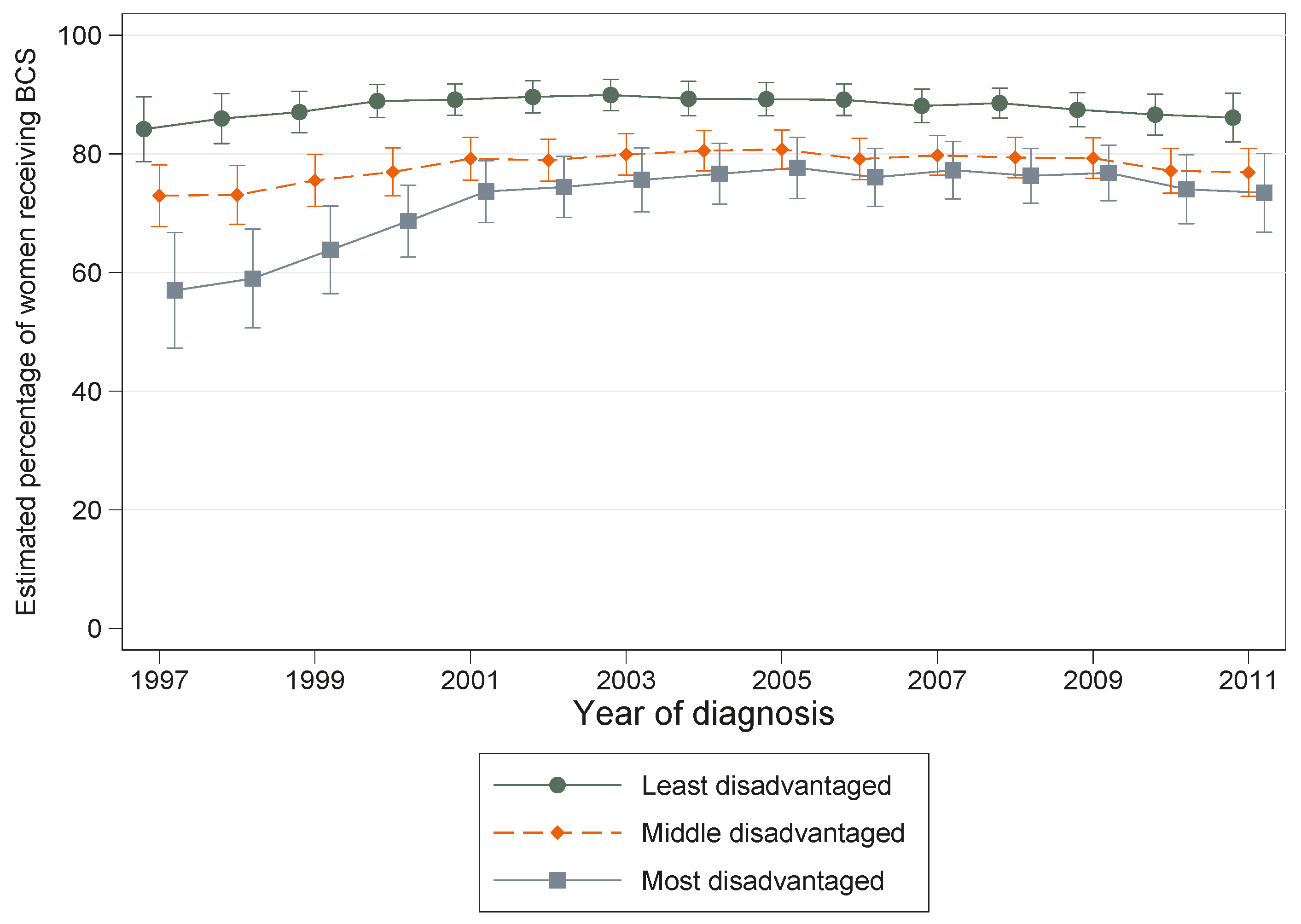
3.3. Interaction Models
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BCS | Breast conserving surgery |
| QHAPDC | Queensland Hospital Admitted Patient Data Collection |
| QCR | Queensland Cancer Registry |
| CCI | Charlson Comorbidity Index |
| SES | Socioeconomic status |
| SLA | Statistical Local Area |
| OR | Odds Ratios |
| CI | Confidence Intervals |
| ICD-9-CM | International Classification of Diseases, 9th Revision, Clinical Modification |
| ICD-10-AM | International Classification of Diseases, 10th Revision, Australian Modification |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F.; Committee, E.G. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. 5), v8–v30. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Clinical Excellence. NICE Clinical Guidelines (CG80)—Early and Locally Advanced Breast Cancer: Diagnosis and Treatment. Available online: http://www.nice.org.uk/guidance/CG80 (accessed on 15 January 2016).
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Early Breast Cancer. Available online: http://www.nhmrc.gov.au/publications/synopses/cp74syn.htm (accessed on 20 January 2016).
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Bellavance, E.C.; Kesmodel, S.B. Decision making in the surgical treatment of breast cancer: Factors influencing women’s choices for mastectomy and breast conserving surgery. Front. Oncol. 2016, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Engel, J.; Kerr, J.; Schlesinger-Raab, A.; Sauer, H.; Holzel, D. Quality of life following breast-conserving therapy or mastectomy: Results of a 5-year prospective study. Breast J. 2004, 10, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.-Y.; Shu, B.-C.; Chang, Y.-J. The effect of breast reconstruction surgery on body image among women after mastectomy: A meta-analysis. Breast Cancer Res. Treat. 2013, 137, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Han, J.; Grothuesmann, D.; Neises, M.; Hille, U.; Hillemanns, P. Quality of life and satisfaction after breast cancer operation. Arch. Gynecol. Obstet. 2010, 282, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.M.; Tamimi, R.M.; Gelber, S.; Ruddy, K.J.; Kereakoglow, S.; Borges, V.F.; Come, S.E.; Schapira, L.; Winer, E.P.; Partridge, A.H. Body image in recently diagnosed young women with early breast cancer. Psychooncology 2013, 22, 1849–1855. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Kim, S.W.; Heo, C.Y.; Kim, D.; Hwang, Y.; Yom, C.K.; Kang, E. Comparison of Quality of Life Based on Surgical Technique in Patients with Breast Cancer. Jpn. J. Clin. Oncol. 2014, 44, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Pyfer, B.; Czerniecki, B.; Rosenkranz, K.; Tchou, J.; Fisher, C. Early postoperative outcomes in lumpectomy versus simple mastectomy. J. Surg. Res. 2015, 198, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Pyfer, B.; Chatterjee, A.; Chen, L.L.; Nigriny, J.; Czerniecki, B.; Tchou, J.; Fisher, C. Early Postoperative Outcomes in Breast Conservation Surgery Versus Simple Mastectomy with Implant Reconstruction: A NSQIP Analysis of 11,645 Patients. Ann. Surg. Oncol. 2016, 23, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Aarts, M.J.; Hamelinck, V.C.; Bastiaannet, E.; Coebergh, J.W.; Liefers, G.J.; Voogd, A.C.; van der Sangen, M.; Louwman, W.J. Small but significant socioeconomic inequalities in axillary staging and treatment of breast cancer in the Netherlands. Br. J. Cancer 2012, 107, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzopardi, J.; Walsh, D.; Chong, C.; Taylor, C. Surgical treatment for women with breast cancer in relation to socioeconomic and insurance status. Breast J. 2014, 20, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Azzopardi, J.; Walsh, D.; Chong, C.; Taylor, C. Impact of geographic location on surgical outcomes of women with breast cancer. ANZ J. Surg. 2014, 84, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.; Gao, H.; Yasui, Y.; Dabbs, K.; Winget, M. Treatment variation in patients diagnosed with early stage breast cancer in Alberta from 2002 to 2010: A population-based study. BMC Health Serv. Res. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.B.; Huang, B.; Dragun, A.E. Patterns of care with regard to surgical choice and application of adjuvant radiation therapy for preinvasive and early stage breast cancer in rural Appalachia. Am. J. Clin. Oncol. 2012, 35, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Lautner, M.; Lin, H.; Shen, Y.; Parker, C.; Kuerer, H.; Shaitelman, S.; Babiera, G.; Bedrosian, I. Disparities in the Use of Breast-Conserving Therapy Among Patients with Early-Stage Breast Cancer. JAMA Surg. 2015, 150, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.A.; Meyricke, R.; O’Neill, T.; Roberts, S. Mastectomy or breast conserving surgery? Factors affecting type of surgical treatment for breast cancer—A classification tree approach. BMC Cancer 2006, 6, 98. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, K.J.; Fritschi, L.; Reid, A.; McEvoy, S.P.; Ingram, D.M.; Jamrozik, K.; Clayforth, C.; Byrne, M.J. Rural-urban differences in the presentation, management and survival of breast cancer in Western Australia. Breast 2006, 15, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Roder, D.; Zorbas, H.; Kollias, J.; Pyke, C.; Walters, D.; Campbell, I.; Taylor, C.; Webster, F. Risk factors for poorer breast cancer outcomes in residents of remote areas of Australia. Asian Pac. J. Cancer Prev. 2013, 14, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Roder, D.; Zorbas, H.; Kollias, J.; Pyke, C.; Walters, D.; Campbell, I.; Taylor, C.; Webster, F. Factors predictive of treatment by Australian breast surgeons of invasive female breast cancer by mastectomy rather than breast conserving surgery. Asian Pac. J. Cancer Prev. 2013, 14, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Baade, P.; Coory, M.; Carriere, P.; Fritschi, L. Patterns of surgical treatment for women diagnosed with early breast cancer in Queensland. Ann. Surg. Oncol. 2008, 15, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Craft, P.S.; Buckingham, J.M.; Dahlstrom, J.E.; Beckmann, K.R.; Zhang, Y.; Stuart-Harris, R.; Jacob, G.; Roder, D.; Tait, N. Variation in the management of early breast cancer in rural and metropolitan centres: Implications for the organisation of rural cancer services. Breast 2010, 19, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Dragun, A.E.; Huang, B.; Tucker, T.C.; Spanos, W.J. Disparities in the application of adjuvant radiotherapy after breast-conserving surgery for early stage breast cancer: Impact on overall survival. Cancer 2011, 117, 2590–2598. [Google Scholar] [CrossRef] [PubMed]
- Ess, S.; Joerger, M.; Frick, H.; Probst-Hensch, N.; Vlastos, G.; Rageth, C.; Lutolf, U.; Savidan, A.; Thurlimann, B. Predictors of state-of-the-art management of early breast cancer in Switzerland. Ann. Oncol. 2011, 22, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Hamelinck, V.C.; Bastiaannet, E.; Pieterse, A.H.; Jannink, I.; van de Velde, C.J.H.; Liefers, G.J.; Stiggelbout, A.M. Patients’ preferences for surgical and adjuvant systemic treatment in early breast cancer: A systematic review. Cancer Treat. Rev. 2014, 40, 1005–1018. [Google Scholar] [CrossRef] [PubMed]
- Meilleur, A.; Subramanian, S.V.; Plascak, J.J.; Fisher, J.L.; Paskett, E.D.; Lamont, E.B. Rural Residence and Cancer Outcomes in the United States: Issues and Challenges. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1657–1667. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Enewold, L.; Zahm, S.H.; Jatoi, I.; Shriver, C.; Anderson, W.F.; Jeffery, D.D.; Andaya, A.; Potter, J.F.; McGlynn, K.A.; et al. Breast conserving surgery versus mastectomy: The influence of comorbidities on choice of surgical operation in the Department of Defense health care system. Am. J. Surg. 2013, 206, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.; Sabesan, S.; Steer, C.; Yates, P.; Booms, A.; Jones, V.; Simpson, A.; Clarke, K.; Eek, R.; Ashley, D.; et al. Oncology service initiatives and research in regional Australia. Aust. J. Rural Health 2015, 23, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Smith, T. A long way from home: Access to cancer care for rural Australians. Radiography 2012, 18, 38–42. [Google Scholar] [CrossRef]
- Fox, P.; Boyce, A. Cancer health inequality persists in regional and remote Australia. Med. J. Aust. 2014, 201, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Sabesan, S.; Kelly, J. Are teleoncology models merely about avoiding long distance travel for patients? Eur. J. Cancer Care (Engl.) 2014, 23, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Queensland Department of Health. Queensland Hospital Admitted Patient Data Collection (QHAPDC) Manual 2014–2015. Available online: https://www.health.qld.gov.au/hsu/collections/qhapdc.asp (accessed on 20 November 2015).
- Queensland Cancer Registry. Cancer in Queensland: Incidence, Mortality, Survival and Prevalence, 1982 to 2012; QCR, Cancer Council Queensland and Queensland Health: Brisbane, Australia, 2014. [Google Scholar]
- IARC; IACR; ENCR. International rules for multiple primary cancers. Asian Pac. J. Cancer Prev. 2005, 6, 104–106. [Google Scholar]
- Baade, P.D.; Turrell, G.; Aitken, J.F. Geographic remoteness, area-level socio-economic disadvantage and advanced breast cancer: A cross-sectional, multilevel study. J. Epidemiol. Community Health 2011, 65, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Obermair, A.; Youlden, D.R.; Baade, P.D.; Janda, M. The impact of risk-reducing hysterectomy and bilateral salpingo-oophorectomy on survival in patients with a history of breast cancer—A population-based data linkage study. Int. J. Cancer 2014, 134, 2211–2222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasgupta, P.; Youlden, D.R.; Baade, P.D. An analysis of competing mortality risks among colorectal cancer survivors in Queensland, 1996–2009. Cancer Causes Control 2013, 24, 897–909. [Google Scholar] [CrossRef] [PubMed]
- National Centre for Classification in Health. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM), 5th ed.; Faculty of Health Sciences, University of Sydney: Sydney, Australia, 2006. [Google Scholar]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Standard Geographic Classification (ASGC), 2006; ABS: Canberra, Australia, 2006.
- Cramb, S.M.; Mengersen, K.L.; Turrell, G.; Baade, P.D. Spatial inequalities in colorectal and breast cancer survival: Premature deaths and associated factors. Health Place 2012, 18, 1412–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Australian Institute of Health and Welfare. Rural, Regional and Remote Health: A Guide to Remoteness Classifications. Cat. No. PHE 53. Available online: http://www.aihw.gov.au/publication-detail/?id=6442467589 (accessed on 28 April 2016).
- Australian Bureau of Statistics. Information Paper: An Introduction to Socio-Economic Indexes for Areas (SEIFA), Australia, 2006. ABS Cat. no. 2039.0; ABS: Canberra, Australia, 2008.
- Bland, J.M.; Altman, D.G. Statistics notes. The odds ratio. BMJ 2000, 320, 1468. [Google Scholar] [CrossRef] [PubMed]
- Gordon, L.; Scuffham, P.; Hayes, S.; Newman, B. Exploring the economic impact of breast cancers during the 18 months following diagnosis. Psychooncology 2007, 16, 1130–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butow, P.N.; Phillips, F.; Schweder, J.; White, K.; Underhill, C.; Goldstein, D.; Clinical Oncological Society of Australia. Psychosocial well-being and supportive care needs of cancer patients living in urban and rural/regional areas: A systematic review. Support. Care Cancer 2012, 20, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Kok, D.L.; Chang, J.H.; Erbas, B.; Fletcher, A.; Kavanagh, A.M.; Henderson, M.A.; Gertig, D.M. Urban-rural differences in the management of screen-detected invasive breast cancer and ductal carcinoma in situ in victoria. ANZ J. Surg. 2006, 76, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Hsieh, S.; Michalski, J.M.; Shinohara, E.T.; Perkins, S.M. Distance to Radiation Facility and Treatment Choice in Early-Stage Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Cook, T.; Foster, S.; Poon, R.; Milross, C.; Sundaresan, P. Examining Determinants of Radiotherapy Access: Do Cost and Radiotherapy Inconvenience Affect Uptake of Breast-conserving Treatment for Early Breast Cancer? Clin. Oncol. (R. Coll. Radiol.) 2015, 27, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Dixon, J.M.; Mak, C. Predictors of Mastectomy in a Certified Breast Center—The Surgeon is an Independent Risk Factor. Breast J. 2008, 14, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Reitsamer, R.; Menzel, C.; Glueck, S.; Hitzl, W.; Peintinger, F. Predictors of Mastectomy in a Certified Breast Center—The Surgeon is an Independent Risk Factor. Breast J. 2008, 14, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Allgood, P.C.; Bachmann, M.O. Effects of specialisation on treatment and outcomes in screen-detected breast cancers in Wales: Cohort study. Br. J. Cancer 2006, 94, 36–42. [Google Scholar] [CrossRef] [PubMed]
- McDermott, A.M.; Wall, D.M.; Waters, P.S.; Cheung, S.; Sibbering, M.; Horgan, K.; Kearins, O.; Lawrence, G.; Patnick, J.; Kerin, M.J.; et al. Surgeon and breast unit volume-outcome relationships in breast cancer surgery and treatment. Ann. Surg. 2013, 258, 808–813; discussion 813–814. [Google Scholar] [CrossRef] [PubMed]
- Mazouni, C.; Naveau, A.; Kane, A.; Dunant, A.; Garbay, J.R.; Leymarie, N.; Sarfati, B.; Delaloge, S.; Rimareix, F. The role of oncoplastic breast surgery in the management of breast cancer treated with primary chemotherapy. Breast 2013, 22, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.S.; Schnitt, S.J.; Giuliano, A.E.; Harris, J.R.; Khan, S.A.; Horton, J.; Klimberg, S.; Chavez-MacGregor, M.; Freedman, G.; Houssami, N.; et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Dragun, A.E.; Huang, B.; Tucker, T.C.; Spanos, W.J. Increasing mastectomy rates among all age groups for early stage breast cancer: A 10-year study of surgical choice. Breast J. 2012, 18, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Chandwani, S.; Haffty, B.G.; Demissie, K. Effect of travel distance and time to radiotherapy on likelihood of receiving mastectomy. Ann. Surg. Oncol. 2015, 22, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- AIHW. Australia’s Health 2014; Cat. no. CAN 68; Australian Institute of Health & Welfare, Canberra: Canberra, Australia, 2014.
- Gentil, J.; Dabakuyo, T.S.; Ouedraogo, S.; Poillot, M.L.; Dejardin, O.; Arveux, P. For patients with breast cancer, geographic and social disparities are independent determinants of access to specialized surgeons. A eleven-year population-based multilevel analysis. BMC Cancer 2012, 12, 351. [Google Scholar] [CrossRef] [PubMed]
- Kong, A.L.; Yen, T.W.; Pezzin, L.E.; Miao, H.; Sparapani, R.A.; Laud, P.W.; Nattinger, A.B. Socioeconomic and racial differences in treatment for breast cancer at a low-volume hospital. Ann. Surg. Oncol. 2011, 18, 3220–3227. [Google Scholar] [CrossRef] [PubMed]
- Roder, D.; Zorbas, H.M.; Kollias, J.; Pyke, C.M.; Walters, D.; Campbell, I.D.; Taylor, C.; Webster, F. Analysing risk factors for poorer breast cancer outcomes in residents of lower socioeconomic areas of Australia. Aust. Health Rev. 2014, 38, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Recio-Saucedo, A.; Gerty, S.; Foster, C.; Eccles, D.; Cutress, R.I. Information requirements of young women with breast cancer treated with mastectomy or breast conserving surgery: A systematic review. Breast 2016, 25, 1–13. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Numbers | Breast Conserving Surgery (BCS) | |
|---|---|---|---|
| N (col %) | N (%) Having BCS | Adjusted Odds Ratio (BCS: Mastectomy with 95% Confidence Interval in Brackets) 2 | |
| Number of women in cohort | 11,631 (100.0) | 9223 (79.3) | |
| Residential disadvantage | p < 0.001 1 | p = 0.013 3 | |
| Least disadvantaged | 2044 (17.6) | 1797 (87.9) | 1.00 |
| Middle socioeconomic status | 8237 (70.8) | 6440 (78.2) | 0.81 (0.69, 0.94) |
| Most disadvantaged | 1350 (11.6) | 986 (73.0) | 0.87 (0.71, 0.98) |
| Accessibility | p < 0.001 | p < 0.001 | |
| Very high (<1 h) | 8523 (73.3) | 7157 (84.0) | 1.00 |
| High (1–2 h) | 932 (8.0) | 653 (70.1) | 0.58 (0.49, 0.69) |
| Low (2–6 h) | 1817 (15.6) | 1179 (64.9) | 0.47 (0.41, 0.54) |
| Very low (≥6 h) | 359 (3.1) | 234 (65.2) | 0.44 (0.34, 0.56) |
| Age at diagnosis (years) | p < 0.001 | p < 0.001 | |
| <40 | 586 (5.0) | 466 (79.5) | 0.80 (0.63, 1.01) |
| 40–49 | 1969 (16.9) | 1613 (81.9) | 0.86 (0.74, 1.01) |
| 50–59 | 3277 (28.2) | 2755 (84.1) | 1.00 |
| 60–69 | 3336 (28.7) | 2656 (79.6) | 0.77 (0.68, 0.88) |
| 70–79 | 1871 (16.1) | 1349 (72.1) | 0.53 (0.45, 0.61) |
| ≥80 | 592 (5.1) | 384 (64.9) | 0.40 (0.32, 0.49) |
| Year of diagnosis 4,5 | p < 0.001 | p = 0.002 | |
| 1997 | 507 (4.4) | 353 (69.6) | 1.00 |
| 1998 | 594 (5.1) | 443 (74.6) | 1.03 (0.99, 1.07) |
| 1999 | 632 (5.4) | 486 (76.9) | 1.17 (1.13, 1.21) |
| 2000 | 678 (5.8) | 549 (81.0) | 1.27 (1.22, 1.32) |
| 2001 | 668 (5.7) | 540 (80.8) | 1.48 (1.43, 1.54) |
| 2002 | 705 (6.1) | 576 (81.7) | 1.49 (1.43, 1.54) |
| 2003 | 704 (6.1) | 565 (80.3) | 1.55 (1.49, 1.61) |
| 2004 | 744 (6.4) | 594 (79.8) | 1.57 (1.51, 1.62) |
| 2005 | 788 (6.8) | 646 (82.0) | 1.63 (1.57, 1.69) |
| 2006 | 838 (7.2) | 687 (82.0) | 1.51 (1.46, 1.56) |
| 2007 | 792 (6.8) | 634 (80.1) | 1.53 (1.48, 1.59) |
| 2008 | 927 (8.0) | 736 (79.4) | 1.49 (1.44, 1.54) |
| 2009 | 1009 (8.7) | 789 (78.2) | 1.48 (1.43, 1.52) |
| 2010 | 1040 (8.9) | 825 (79.3) | 1.32 (1.28, 1.36) |
| 2011 | 1005 (8.6) | 800 (79.6) | 1.30 (1.26, 1.34) |
| Partner 6 | p < 0.001 | p = 0.036 | |
| Partnered | 7427 (63.9) | 6003 (80.8) | 1.00 |
| No partner | 3937 (33.8) | 2990 (75.9) | 0.94 (0.84, 0.96) |
| Unknown | 267 (2.3) | 230 (86.1) | 1.40 (0.95, 2.06) |
| Indigenous | p < 0.001 | p = 0.045 | |
| Non-Indigenous | 10,177 (87.5) | 7993 (78.5) | 1.00 |
| Indigenous | 87 (0.7) | 62 (71.3) | 0.96 (0.71, 1.78) |
| Unknown | 1367 (11.8) | 1168 (85.4) | 1.23 (1.02, 1.47) |
| Histology | p < 0.001 | p < 0.001 | |
| Ductal (8500-3) | 8994 (77.3) | 7168 (79.7) | 1.00 |
| Lobular (8520-3) | 1094 (9.4) | 808 (73.9) | 0.73 (0.62, 0.85) |
| Other | 1543 (13.3) | 1247 (80.8) | 1.11 (0.96, 1.28) |
| Size (mm) | p < 0.001 | p < 0.001 | |
| <10 mm | 3905 (33.6) | 3260 (83.5) | 1.00 |
| 10–20 mm | 7726 (66.4) | 5963 (77.2) | 0.75 (0.67, 0.83) |
| Grade | p < 0.001 | p <0.001 | |
| Low | 3391 (29.2) | 2829 (83.4) | 1.00 |
| Intermediate | 4754 (40.9) | 3727 (78.4) | 0.76 (0.67, 0.86) |
| High | 2370 (20.4) | 1839 (77.6) | 0.67 (0.58, 0.77) |
| Unknown | 1116 (9.5) | 828 (74.2) | 0.63 (0.52, 0.76) |
| Multiple primary cancers 7 | p < 0.001 | p <0.001 | |
| No | 10,941 (94.1) | 8760 (80.1) | 1.00 |
| Yes | 690 (5.9) | 463 (67.1) | 0.53 (0.44, 0.64) |
| Comorbidity 8 | p < 0.001 | p = 0.022 | |
| None | 11,027 (94.8) | 8807 (79.9) | 1.00 |
| Low | 491 (4.2) | 347 (70.7) | 0.76 (0.61, 0.95) |
| Moderate/severe | 113 (1.0) | 69 (61.1) | 0.62 (0.41, 0.94) |
| Hospital type | p < 0.001 | p <0.001 | |
| Public | 5106 (43.9) | 3834 (75.1) | 1.00 |
| Private | 6525 (56.1) | 5389 (82.6) | 1.48 (1.33, 1.64) |
| Hospital volume 9 | p < 0.001 | p <0.001 | |
| 0–74 | 3761 (32.3) | 2763 (73.5) | 1.00 |
| 75–99 | 1636 (14.1) | 1121 (68.5) | 0.78 (0.68, 1.02) |
| ≥100 | 6234 (53.6) | 5339 (85.6) | 1.58 (1.41, 1.78) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baade, P.D.; Dasgupta, P.; Youl, P.H.; Pyke, C.; Aitken, J.F. Geographical Inequalities in Surgical Treatment for Localized Female Breast Cancer, Queensland, Australia 1997–2011: Improvements over Time but Inequalities Remain. Int. J. Environ. Res. Public Health 2016, 13, 729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070729
Baade PD, Dasgupta P, Youl PH, Pyke C, Aitken JF. Geographical Inequalities in Surgical Treatment for Localized Female Breast Cancer, Queensland, Australia 1997–2011: Improvements over Time but Inequalities Remain. International Journal of Environmental Research and Public Health. 2016; 13(7):729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070729
Chicago/Turabian StyleBaade, Peter D., Paramita Dasgupta, Philippa H. Youl, Christopher Pyke, and Joanne F. Aitken. 2016. "Geographical Inequalities in Surgical Treatment for Localized Female Breast Cancer, Queensland, Australia 1997–2011: Improvements over Time but Inequalities Remain" International Journal of Environmental Research and Public Health 13, no. 7: 729. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070729