
High Vaccination Coverage among Children during Influenza A(H1N1)pdm09 as a Potential Factor of Herd Immunity

Abstract
:1. Introduction
2. Materials and Methods
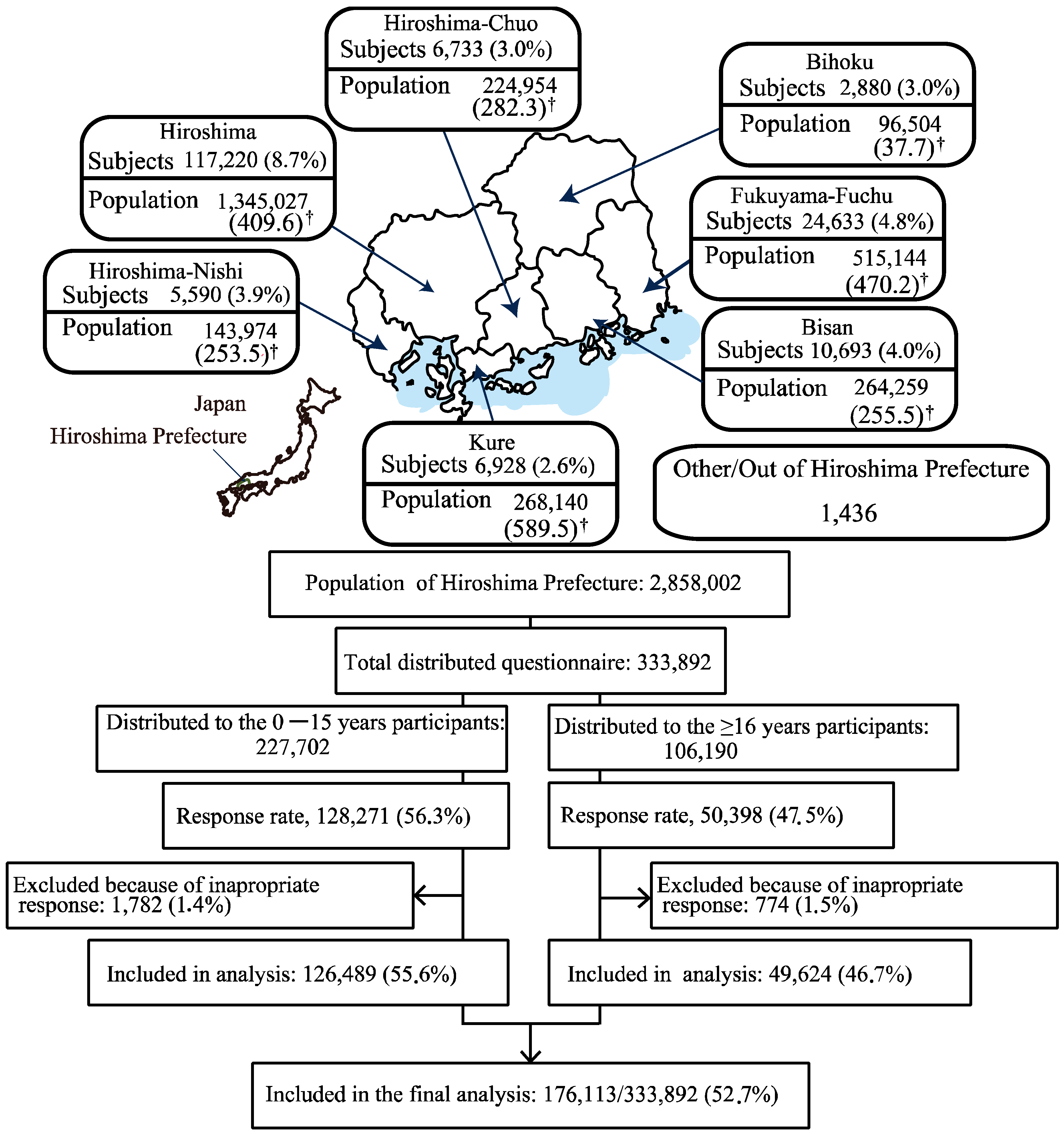
2.1. Study Design and Participants
2.2. Questionnaires
- What was the most helpful information about influenza A(H1N1)pdm09?
- Have you/your child had influenza A(H1N1)pdm09 infection?
- Did a doctor confirm your influenza A(H1N1)pdm09 infection between June 2009 to May 2010? Which month was it?
- How many people are living together in your family?
- Which preventative action did you take against influenza A(H1N1)pdm09?
- Have you/your child been vaccinated against influenza A(H1N1)pdm09?
- What is the reason for being vaccinated?
- What is the reason for not being vaccinated?
2.3. Statistical Analysis
2.3.1. Period Prevalence by Month (June 2009 to May 2010)
2.3.2. Vaccination rates (from November 2009 to May 2010)
2.3.3. Overall Cumulative Incidence (from November 2009 to May 2010)
2.3.4. Cumulative Incidence by Vaccine Status and Odds Ratio (November 2009 to May 2010)
2.3.5. Vaccine Effectiveness (from November 2009 to May 2010)
2.3.6. Correlation between Vaccination Rates and Cumulative Incidence
2.3.7. Logistic Regression Analysis for Preventing Infection
2.3.8. Expansion of Infection
2.4. Ethics Approval and Consent to Participate
3. Results
3.1. Participants’ Characteristics
3.2. Vaccination Rates
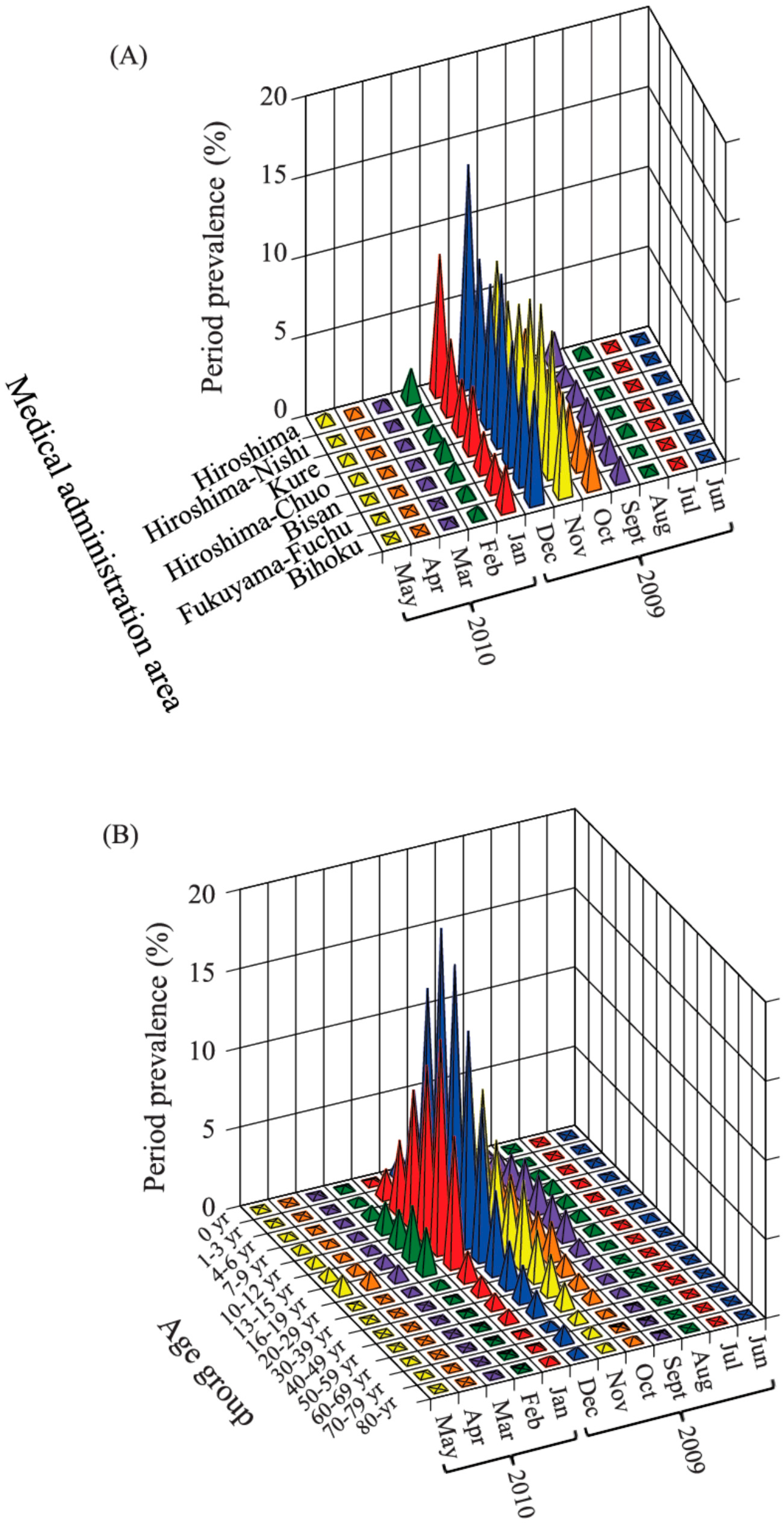
3.3. Period Prevalence
3.4. Overall Cumulative Incidence of Influenza, OR of Cumulative Incidence and VE Based on Vaccination Status
3.5. Correlation between Cumulative Incidence and Vaccination Rate
3.6. Factors Associated with Influenza Infection
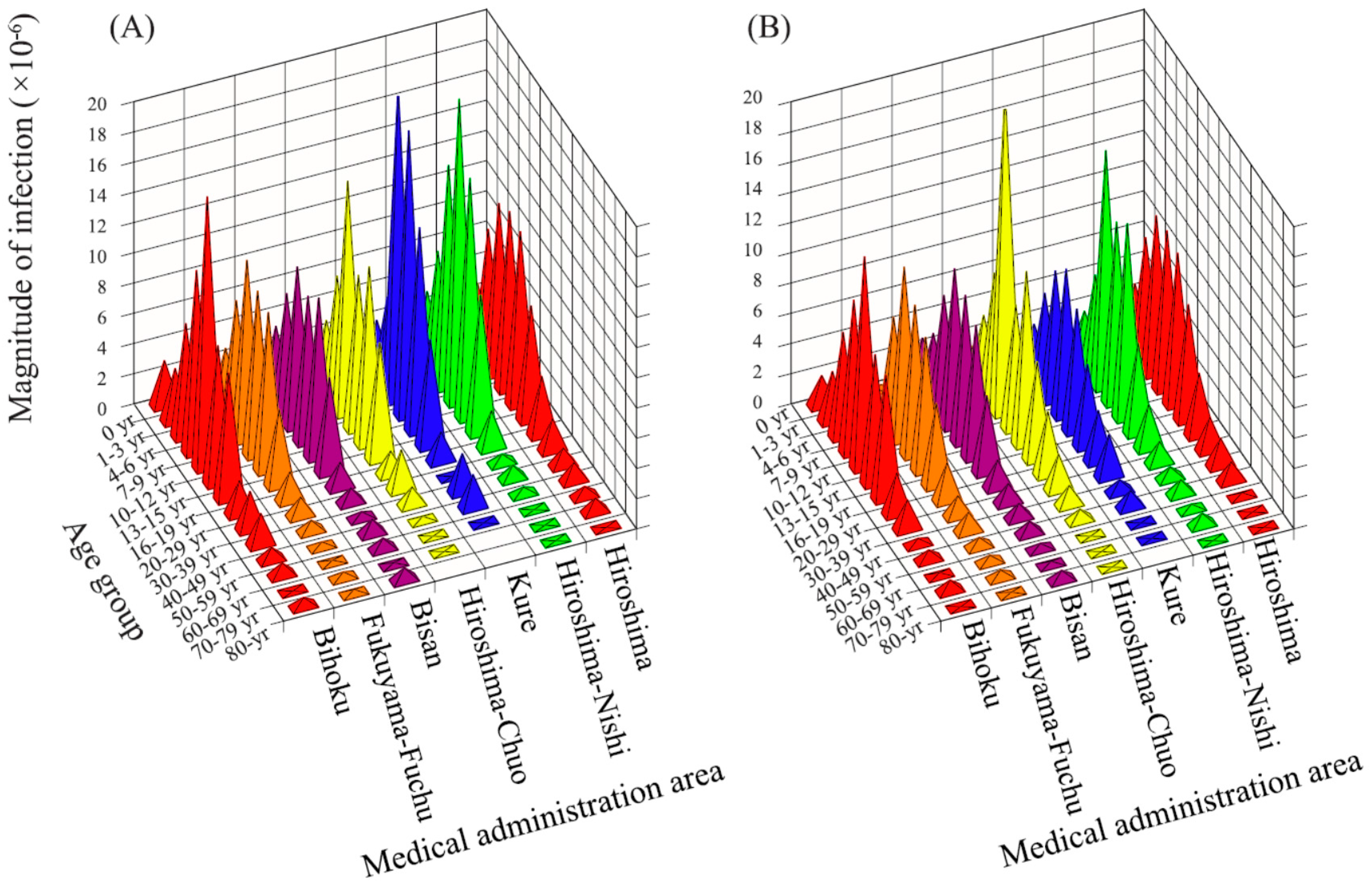
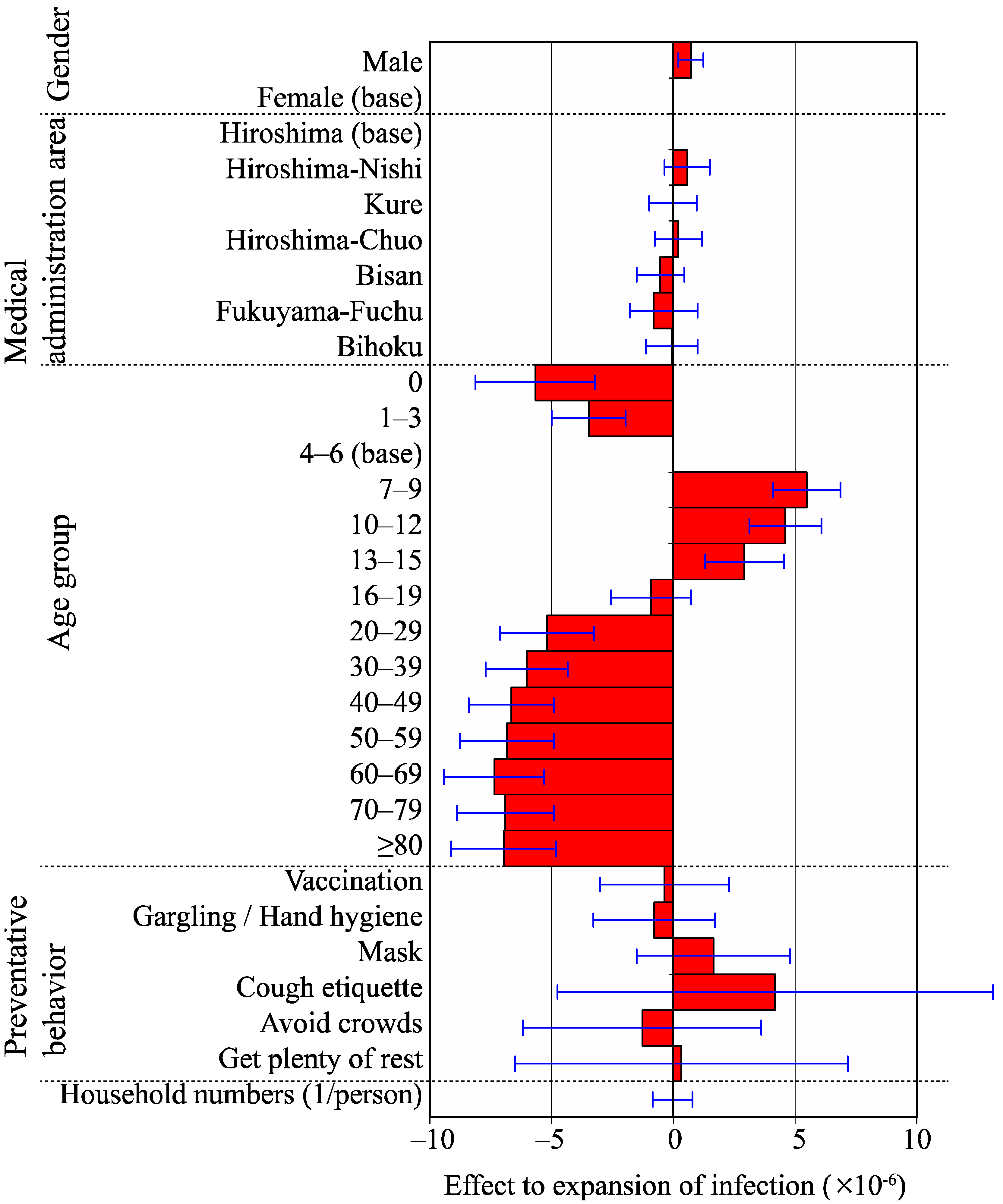
3.7. Expansion of Infection
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Geneva. Influenza. Fact Sheet No.211 Revised March 2014. Available online: http://www.who.int/mediacentre/factsheets/fs211/en/ (accessed on 1 March 2014).
- National Institute of Infectious Diseases, Japan. Infectious Agents Surveillance Report: One Year Since the 2009 Pandemic (H1N1). Available online: http://idsc.Nih.Go.Jp/iasr/31/367/inx367.Html (accessed on 1 March 2014).
- Cabinet Secretariat in Japan. Tokyo National Action Plan for Pandemic Influenza and New Infectious Diseases. 2013. Available online: http://www.Cas.Go.Jp/jp/seisaku/ful/keikaku.Html (accessed on 17 April 2016). [Google Scholar]
- King, J.C., Jr.; Stoddard, J.J.; Gaglani, M.J.; Moore, K.A.; Magder, L.; McClure, E.; Rubin, J.D.; Englund, J.A.; Neuzil, K. Effectiveness of school-based influenza vaccination. N. Engl. J. Med. 2006, 355, 2523–2532. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.; Lee, J.; Fireman, B. Evidence of bias in studies of influenza vaccine effectiveness in elderly patients. J. Infect. Dis. 2010, 201, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Gordis, L. Epidemiology, 4th ed.; Sanders Elsevier: Philadelphia, PA, USA, 2009; pp. 24–25. [Google Scholar]
- Plans-Rubio, P. The vaccination coverage required to establish herd immunity against influenza viruses. Prev. Med. 2012, 55, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Reichert, T.A.; Sugaya, N.; Fedson, D.S.; Glezen, W.P.; Simonsen, L.; Tashiro, M. The Japanese experience with vaccinating schoolchildren against influenza. N. Engl. J. Med. 2001, 344, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, N. Influenza vaccination and excess mortality—A reevaluation of group vaccination of students in Japan. Influenza 2007, 8, 31–34. [Google Scholar]
- Kawai, S.; Nanri, S.; Ban, E.; Inokuchi, M.; Tanaka, T.; Tokumura, M.; Kimura, K.; Sugaya, N. Influenza vaccination of schoolchildren and influenza outbreaks in a school. Clin. Infect. Dis. 2011, 53, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Regional Health Care Council of Hiroshima Prefecture. Report on a Survey of the 2009 Influenza (H1N1) Infection; Regional Health Care Council of Hiroshima Prefecture: Hiroshima, Japan, 2013; pp. 152–155. [Google Scholar]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Aiello, A.E.; Murray, G.F.; Perez, V.; Coulborn, R.M.; Davis, B.M.; Uddin, M.; Shay, D.K.; Waterman, S.H.; Monto, A.S. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: A randomized intervention trial. J. Infect. Dis. 2010, 201, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Chan, K.H.; Fang, V.J.; Cheng, C.K.; Fung, R.O.; Wai, W.; Sin, J.; Seto, W.H.; Yung, R.; Chu, D.W.; et al. Facemasks and hand hygiene to prevent influenza transmission in households: A cluster randomized trial. Ann. Intern. Med. 2009, 151, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Hiroshima Prefecture in Japan. Hiroshima. Population by Estimate (May 2010). Available online: http://www.Pref.Hiroshima.Lg.Jp/soshiki/21/jinkougeppojinkousuiih2203.html (accessed on 17 April 2016).
- Britton, T. Estimation in multitype epidemics. J. R. Stat. Soc. Ser. B-Stat. Methodol. 1998, 60, 663–679. [Google Scholar] [CrossRef]
- Shinjoh, M.; Sugaya, N.; Yamaguchi, Y.; Tomidokoro, Y.; Sekiguchi, S.; Mitamura, K.; Fujino, M.; Shiro, H.; Komiyama, O.; Taguchi, N.; et al. Effectiveness of trivalent inactivated influenza vaccine in children estimated by a Test-negative case-control design study based on influenza rapid diagnostic test results. PLoS ONE 2015, 10, e0136539. [Google Scholar] [CrossRef] [PubMed]
- Jefferson, T.; Di Pietrantonj, C.; Al-Ansary, L.A.; Ferroni, E.; Thorning, S.; Thomas, R.E. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2010, CD004876. [Google Scholar] [CrossRef]
- Jefferson, T.; Di Pietrantonj, C.; Rivetti, A.; Bawazeer, G.A.; Al-Ansary, L.A.; Ferroni, E. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst. Rev. 2010, CD001269. [Google Scholar] [CrossRef]
- Jefferson, T.; Rivetti, A.; Di Pietrantonj, C.; Demicheli, V.; Ferroni, E. Vaccines for preventing influenza in healthy children. Cochrane Database Syst. Rev. 2012, 8, CD004879. [Google Scholar] [PubMed]
- Pannaraj, P.S.; Wang, H.L.; Rivas, H.; Wiryawan, H.; Smit, M.; Green, N.; Aldrovandi, G.M.; El Amin, A.N.; Mascola, L. School-located influenza vaccination decreases laboratory-confirmed influenza and improves school attendance. Clin. Infect. Dis. 2014, 59, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.A.; Chui, K.K.; Naumova, E.N. Influenza vaccination in young children reduces influenza-associated hospitalizations in older adults, 2002–2006. J. Am. Geriatr. Soc. 2011, 59, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, N.; Takeuchi, Y. Mass vaccination of schoolchildren against influenza and its impact on the influenza-associated mortality rate among children in Japan. Clin. Infect. Dis. 2005, 41, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Pitman, R.J.; Nagy, L.D.; Sculpher, M.J. Cost-effectiveness of childhood influenza vaccination in England and Wales: Results from a dynamic transmission model. Vaccine 2013, 31, 927–942. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H.; Castillo-Chavez, C.; Safan, M.; Chowell, G. Transmission potential of the new influenza A(H1N1) virus and its age-specificity in Japan. Euro Surveill. 2009, 14, 19227. [Google Scholar] [PubMed]
- Tsukui, S. Case-Based Surveillance of Pandemic (H1N1) 2009 in Maebashi City, Japan. Jpn. J. Infect. Dis. 2012, 65, 132–137. [Google Scholar] [PubMed]
- Papenburg, J.; Baz, M.; Hamelin, M.E.; Rheaume, C.; Carbonneau, J.; Ouakki, M.; Rouleau, I.; Hardy, I.; Skowronski, D.; Roger, M.; et al. Household transmission of the 2009 pandemic A/H1N1 influenza virus: elevated laboratory-confirmed secondary attack rates and evidence of asymptomatic infections. Clin. Infect. Dis. 2010, 51, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.Y.; Chen, W.H.; Lu, C.Y.; Shao, P.L.; Fan, T.Y.; Cheng, A.L.; Huang, L.M. Household transmission of Pandemic (H1N1) 2009 Virus, Taiwan. Emerg. Infect. Dis. 2011, 17, 1928–1931. [Google Scholar] [CrossRef] [PubMed]
- France, A.M.; Jackson, M.; Schrag, S.; Lynch, M.; Zimmerman, C.; Biggerstaff, M.; Hadler, J. Household transmission of 2009 influenza A (H1N1) virus after a school-based outbreak in New York City, April–May 2009. J. Infect. Dis. 2010, 201, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, L.; Kurkela, S.; Neave, P.E.; Brock, A.; Perkins, S.; Zuckerman, M.; Sudhanva, M.; Bermingham, A.; Ellis, J.; Pebody, R.; et al. Pandemic (H1N1) 2009 virus outbreak in a school in London, April–May 2009: An observational study. Epidemiol. Infect. 2010, 138, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Eames, K.T.; Tilston, N.L.; Brooks-Pollock, E.; Edmunds, W.J. Measured dynamic social contact patterns explain the spread of H1N1v influenza. PLoS Comput. Biol. 2012, 8, e1002425. [Google Scholar] [CrossRef] [PubMed]
- DeStefano, F.; Haber, M.; Currivan, D.; Farris, T.; Burrus, B.; Stone-Wiggins, B.; McCalla, A.; Guled, H.; Shih, H.; Edelson, P.; et al. Factors associated with social contacts in four communities during the 2007–2008 influenza season. Epidemiol. Infect. 2011, 139, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Eshima, N.; Tokumaru, O.; Hara, S.; Bacal, K.; Korematsu, S.; Tabata, M.; Karukaya, S.; Yasui, Y.; Okabe, N.; Matsuishi, T. Sex- and age-related differences in morbidity rates of 2009 pandemic influenza A H1N1 virus of swine origin in Japan. PLoS ONE 2011, 6, e19409. [Google Scholar] [CrossRef] [PubMed]
- Filleul, L.; D’Ortenzio, E.; Kermarec, F.; Le Bot, F.; Renault, P. Pandemic influenza on Reunion Island and school closure. Lancet Infect. Dis. 2010, 10, 294–295. [Google Scholar] [CrossRef]
- Cauchemez, S.; Valleron, A.J.; Boelle, P.Y.; Flahault, A.; Ferguson, N.M. Estimating the impact of school closure on influenza transmission from Sentinel data. Nature 2008, 452, 750–754. [Google Scholar] [CrossRef] [PubMed]
- Talaat, M.; Afifi, S.; Dueger, E.; El-Ashry, N.; Marfin, A.; Kandeel, A.; Mohareb, E.; El-Sayed, N. Effects of hand hygiene campaigns on incidence of laboratory-confirmed influenza and absenteeism in schoolchildren, Cairo, Egypt. Emerg. Infect. Dis. 2011, 17, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, N.; Mitamura, K.; Yamazaki, M.; Tamura, D.; Ichikawa, M.; Kimura, K.; Kawakami, C.; Kiso, M.; Ito, M.; Hatakeyama, S.; et al. Lower clinical effectiveness of oseltamivir against influenza B contrasted with influenza A infection in children. Clin. Infect. Dis. 2007, 44, 197–202. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Male | Female | Total |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Total | 82,738 (47.0) | 93,375 (53.0) | 176,113 (100.0) |
| Medical administration area | |||
| Hiroshima | 56,696 (32.2) | 60,524 (34.4) | 117,220 (66.6) |
| Hiroshima-Nishi | 2962 (1.7) | 2628 (1.5) | 5590 (3.2) |
| Kure | 3079 (1.7) | 3849 (2.2) | 6928 (3.9) |
| Hiroshima-Chuo | 3149 (1.8) | 3584 (2.0) | 6733 (3.8) |
| Bisan | 4721 (2.7) | 5972 (3.4) | 10,693 (6.1) |
| Fukuyama-Fuchu | 10,129 (5.8) | 14,504 (8.2) | 24,633 (14.0) |
| Bihoku | 1193 (0.7) | 1687 (1.0) | 2880 (1.6) |
| Other | 809 (0.5) | 627 (0.4) | 1436 (0.8) |
| Age groups | |||
| 0 year | 437 (0.2) | 387 (0.2) | 824 (0.5) |
| 1–3 years | 9230 (5.2) | 8506 (4.8) | 17,736 (10.1) |
| 4–6 years | 19,012 (10.8) | 18,116 (10.3) | 37,128 (21.1) |
| 7–9 years † | 12,631 (7.2) | 12,605 (7.2) | 25,236 (14.3) |
| 10–12 years †† | 12,814 (7.3) | 13,485 (7.7) | 26,299 (14.9) |
| 13–15 years ††† | 9,174 (5.2) | 10,092 (5.7) | 19,266 (10.9) |
| 16–19 years | 12,741 (7.2) | 11,812 (6.7) | 24,553 (13.9) |
| 20–29 years | 932 (0.5) | 4094 (2.3) | 5026 (2.9) |
| 30–39 years | 1246 (0.7) | 4082 (2.3) | 5328 (3.0) |
| 40–49 years | 1302 (0.7) | 3634 (2.1) | 4936 (2.8) |
| 50–59 years | 1464 (0.8) | 3847 (2.2) | 5311 (3.0) |
| 60–69 years | 937 (0.5) | 1552 (0.9) | 2489 (1.4) |
| 70–79 years | 579 (0.3) | 811 (0.5) | 1390 (0.8) |
| ≥80 years | 239 (0.1) | 352 (0.2) | 591 (0.3) |
| Total | Number of Vaccinated | Vaccination Rate (%) | |
|---|---|---|---|
| Overall | 157,084 | 57,320 | 36.5 |
| By age group (p < 0.0001) | |||
| 0 year | 812 | 85 | 10.5 |
| 1–3 years | 17,220 | 9277 | 53.9 |
| 4–6 years | 34,728 | 17,134 | 49.3 |
| 7–9 years | 22,166 | 7759 | 35.0 |
| 10–12 years | 22,309 | 5345 | 24.0 |
| 13–15 years | 15,381 | 3076 | 20.0 |
| 16–19 years | 20,647 | 6885 | 33.3 |
| 20–29 years | 4706 | 1270 | 27.0 |
| 30–39 years | 5047 | 1621 | 32.1 |
| 40–49 years | 4682 | 1308 | 27.9 |
| 50–59 years | 5082 | 1385 | 27.3 |
| 60–69 years | 2387 | 989 | 41.4 |
| 70–79 years | 1344 | 793 | 59.0 |
| ≥80 years | 573 | 393 | 68.6 |
| By medical administration area (p < 0.0001) | |||
| Hiroshima-Nishi | 5210 | 2015 | 38.7 |
| Hiroshima | 102,518 | 34,074 | 33.2 |
| Kure | 6539 | 2784 | 42.6 |
| Hiroshima-Chuo | 6277 | 2557 | 40.7 |
| Bisan | 10,152 | 4454 | 43.9 |
| Fukuyama-Fuchu | 23,630 | 10,108 | 42.8 |
| Bihoku | 2758 | 1328 | 48.2 |
| By gender (p < 0.0001) | |||
| Men | 72,748 | 27,052 | 37.2 |
| Women | 84,336 | 30,268 | 35.9 |
| Number of Participants n (%) | Cumulative Incidence n/N (%) | Odds Ratio (OR) | Vaccine Effectiveness (VE; %) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Vaccinated Group | Non-Vaccinated Group | OR | 95% Confidence Interval | p Value | VE (%) | 95% Confidence Interval | p Value | ||||
| Overall | 153,308 (100.0) | 10,855/57,320 (18.9) | 32,379/95,988 (33.7) | 2.18 | 2.13 | 2.23 | <0.0001 | 43.9 | 42.8 | 44.9 | <0.0001 |
| By Age Group (p < 0.0001) † | |||||||||||
| 0 year | 755 (0.5) | 10/85 (11.8) | 31/690 (4.5) | 0.35 | 0.17 | 0.71 | 0.0038 | −161.9 | −414.9 | −33.2 | 0.0038 |
| 1–3 years | 16,865 (11.0) | 958/9277 (10.3) | 2188/7588 (28.8) | 3.52 | 3.25 | 3.81 | <0.0001 | 64.2 | 61.6 | 66.6 | <0.0001 |
| 4–6 years | 34,016 (22.2) | 3602/17,134 (21.0) | 8025/16,882 (47.5) | 3.40 | 3.25 | 3.56 | <0.0001 | 55.8 | 54.3 | 57.2 | <0.0001 |
| 7–9 years | 21,728 (14.2) | 2188/7759 (28.2) | 6840/13,969 (49.0) | 2.44 | 2.30 | 2.59 | <0.0001 | 42.4 | 40.1 | 44.6 | <0.0001 |
| 10–12 years | 21,814 (14.2) | 1526/5345 (28.6) | 6931/16,469 (42.1) | 1.82 | 1.70 | 1.94 | <0.0001 | 32.2 | 29.0 | 35.2 | <0.0001 |
| 13–15 years | 14,990 (9.8) | 753/3076 (24.5) | 4049/11,914 (34.0) | 1.59 | 1.45 | 1.74 | <0.0001 | 28.0 | 23.0 | 32.6 | <0.0001 |
| 16–19 years | 19,962 (13.0) | 1544/6885 (22.4) | 2984/13,077 (22.8) | 1.02 | 0.95 | 1.10 | 0.5214 | 1.7 | −3.7 | 6.9 | 0.5214 |
| 20–29 years | 4643 (3.0) | 102/1270 (8.0) | 565/3373 (16.8) | 2.30 | 1.86 | 2.86 | <0.0001 | 52.1 | 41.4 | 60.8 | <0.0001 |
| 30–39 years | 4969 (3.2) | 63/1621 (3.9) | 327/3348 (9.8) | 2.68 | 2.05 | 3.49 | <0.0001 | 60.2 | 48.2 | 69.4 | <0.0001 |
| 40–49 years | 4601 (3.0) | 45/1308 (3.4) | 244/3293 (7.4) | 2.25 | 1.64 | 3.08 | <0.0001 | 53.6 | 36.6 | 66.0 | <0.0001 |
| 50–59 years | 4950 (3.2) | 32/1385 (2.3) | 176/3565 (4.9) | 2.20 | 1.52 | 3.17 | <0.0001 | 53.2 | 32.1 | 67.7 | <0.0001 |
| 60–69 years | 2237 (1.5) | 19/989 (1.9) | 13/1248 (1.0) | 0.54 | 0.27 | 1.06 | 0.0724 | −84.4 | −271.6 | 8.5 | 0.0723 |
| 70–79 years | 1239 (0.8) | 9/793 (1.1) | 5/446 (1.1) | 0.99 | 0.34 | 2.84 | 0.9816 | −1.2 | −200.2 | 65.9 | 0.9816 |
| ≥80 years | 519 (0.3) | 4/393 (1.0) | 1/126 (0.8) | 0.78 | 0.10 | 6.29 | 0.8140 | −28.2 | −1036.9 | 85.5 | 0.8138 |
| By Medical Administration Area (p = 0.0371) † | |||||||||||
| Hiroshima-Nishi | 5118(3.3) | 269/2015 (13.3) | 762/3103 (24.6) | 2.11 | 1.82 | 2.45 | <0.0001 | 45.6 | 38.3 | 52.1 | <0.0001 |
| Hiroshima | 100,116 (65.3) | 7232/34,074 (21.2) | 23,995/66,042 (36.3) | 2.12 | 2.06 | 2.18 | <0.0001 | 41.6 | 40.2 | 42.9 | <0.0001 |
| Kure | 6359(4.1) | 432/2784 (15.5) | 950/3575 (26.6) | 1.97 | 1.74 | 2.23 | <0.0001 | 41.6 | 35.3 | 47.3 | <0.0001 |
| Hiroshima-Chuo | 6158(4.0) | 501/2557 (19.6) | 1141/3601 (31.7) | 1.90 | 1.69 | 2.14 | <0.0001 | 38.2 | 32.2 | 43.6 | <0.0001 |
| Bisan | 9935(6.5) | 716/4454 (16.1) | 1676/5481 (30.6) | 2.30 | 2.09 | 2.53 | <0.0001 | 47.4 | 43.2 | 51.4 | <0.0001 |
| Fukuyama-Fuchu | 22,926(15.0) | 1554/10,108 (15.4) | 3499/12,818 (27.3) | 2.07 | 1.94 | 2.21 | <0.0001 | 43.7 | 40.6 | 46.6 | <0.0001 |
| Bihoku | 2696(1.8) | 151/1328 (11.4) | 356/1368 (26.0) | 2.74 | 2.24 | 3.35 | <0.0001 | 56.3 | 48.0 | 63.3 | <0.0001 |
| By Gender (p = 0.8469) † | |||||||||||
| Men | 70,849(46.2) | 5603/27,052 (20.7) | 15,913/43,797 (36.3) | 2.18 | 2.11 | 2.26 | <0.0001 | 43.0 | 41.5 | 44.5 | <0.0001 |
| Women | 82,459(53.8) | 5252/30,268 (17.4) | 16,466/52,191 (17.4) | 2.20 | 2.12 | 2.27 | <0.0001 | 45.0 | 43.5 | 46.5 | <0.0001 |
| Correlation Coefficient | p Value | |
|---|---|---|
| 0 year | −0.24684 | 0.5936 |
| 1–3 years | −0.24976 | 0.5891 |
| 4–6 years | −0.81175 | 0.0266 |
| 7–9 years | −0.46113 | 0.2977 |
| 10–12 years | −0.82873 | 0.0212 |
| 13–15 years | −0.44746 | 0.3141 |
| 16–19 years | −0.3034 | 0.5083 |
| 20–29 years | −0.06394 | 0.8917 |
| 30–39 years | −0.36538 | 0.4203 |
| 40–49 years | −0.33015 | 0.4696 |
| 50–59 years | −0.44907 | 0.3121 |
| ≥60 years | −0.51402 | 0.2379 |
| Item | 0–15 Years (n = 125,477) | ≥16 Years (n = 49,231) | All Participants (n = 174,708) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | p Value | AOR | 95% CI | p Value | AOR | 95% CI | p Value | |
| Gender | |||||||||
| Male | 1.16 | 1.14–1.19 | <0.001 *** | 1.03 | 0.98–1.08 | 0.3070 | 1.13 | 1.11–1.16 | <0.001 *** |
| Female | 1.00 | 1.00 | 1.00 | ||||||
| Medical administration area | |||||||||
| Hiroshima | 1.00 | 1.00 | 1.00 | ||||||
| Hiroshima-Nishi | 1.00 | 0.92–1.08 | 0.9085 | 0.79 | 0.70–0.88 | <0.001 *** | 0.92 | 0.86–0.98 | 0.0148 * |
| Kure | 0.75 | 0.70–0.81 | <0.001 *** | 0.80 | 0.72–0.88 | <0.001 *** | 0.77 | 0.73–0.82 | <0.001 *** |
| Hiroshima-Chuo | 1.07 | 0.99–1.14 | 0.0730 | 0.90 | 0.82–1.00 | 0.0515 | 1.02 | 0.96–1.08 | 0.5631 |
| Bisan | 1.02 | 0.96–1.08 | 0.5127 | 0.67 | 0.61–0.74 | <0.001 *** | 0.93 | 0.88–0.97 | 0.0021 ** |
| Fukuyama-Fuchu | 0.99 | 0.95–1.02 | 0.4583 | 0.65 | 0.60–0.70 | <0.001 *** | 0.90 | 0.87–0.94 | <0.001 *** |
| Bihoku | 0.88 | 0.78–0.98 | 0.0192 * | 0.76 | 0.61–0.93 | 0.01 * | 0.86 | 0.78–0.95 | 0.0032 ** |
| Other | 0.95 | 0.73–1.24 | 0.7079 | 0.60 | 0.49–0.72 | <0.001 *** | 0.73 | 0.62–0.84 | <0.001 *** |
| Age group | |||||||||
| 0 year | 0.10 | 0.07–0.13 | <0.001 *** | 0.10 | 0.07–0.13 | <0.001 *** | |||
| 1–3 years | 0.46 | 0.44–0.48 | <0.001 *** | 0.46 | 0.44–0.48 | <0.001 *** | |||
| 4–6 years | 1.00 | 1.00 | |||||||
| 7–9 years | 1.35 | 1.30–1.40 | <0.001 *** | 1.34 | 1.30–1.39 | <0.001 *** | |||
| 10–12 years | 1.25 | 1.21–1.29 | <0.001 *** | 1.26 | 1.22–1.30 | <0.001 *** | |||
| 13–15 years | 1.12 | 1.08–1.17 | <0.001 *** | 1.14 | 1.10–1.19 | <0.001 *** | |||
| 16–19 years | 5.04 | 4.55–5.60 | <0.001 *** | 0.80 | 0.77–0.83 | <0.001 *** | |||
| 20–29 years | 2.01 | 1.78–2.27 | <0.001 *** | 0.30 | 0.28–0.33 | <0.001 *** | |||
| 30–39 years | 1.00 | 0.15 | 0.14–0.17 | <0.001 *** | |||||
| 40–49 years | 0.74 | 0.64–0.85 | <0.001 *** | 0.11 | 0.10–0.13 | <0.001 *** | |||
| 50–59 years | 0.52 | 0.44–0.61 | <0.001 *** | 0.08 | 0.07–0.09 | <0.001 *** | |||
| 60–69 years | 0.21 | 0.15–0.29 | <0.001 *** | 0.03 | 0.02–0.04 | <0.001 *** | |||
| 70–79 years | 0.23 | 0.15–0.34 | <0.001 *** | 0.03 | 0.02–0.05 | <0.001 *** | |||
| ≥80 years | 0.14 | 0.05–0.28 | <0.001 *** | 0.02 | 0.01–0.04 | <0.001 *** | |||
| Helpful information | |||||||||
| Television | 0.82 | 0.79–0.85 | <0.001 *** | 0.74 | 0.68–0.81 | <0.001 *** | 0.81 | 0.78–0.83 | <0.001 *** |
| Newspapers | 0.87 | 0.84–0.90 | <0.001 *** | 0.80 | 0.72–0.88 | <0.001 *** | 0.86 | 0.83–0.89 | <0.001 *** |
| Pamphlets | 0.96 | 0.90–1.01 | 0.1399 | 1.04 | 0.88–1.22 | 0.6696 | 0.97 | 0.92–1.02 | 0.2761 |
| Internet | 0.93 | 0.89–0.98 | 0.0034 ** | 0.79 | 0.69–0.89 | 0.0002 *** | 0.90 | 0.87–0.95 | <0.001 *** |
| Preventative behavior | |||||||||
| Vaccination | 0.55 | 0.53–0.56 | <0.001 *** | 1.10 | 1.04–1.16 | 0.0008 *** | 0.62 | 0.61–0.64 | <0.001 *** |
| Gargling/Hand hygiene | 1.19 | 1.16–1.23 | <0.001 *** | 0.91 | 0.87–0.96 | 0.0005 *** | 1.11 | 1.08–1.14 | <0.001 *** |
| Mask | 1.53 | 1.50–1.57 | <0.001 *** | 1.89 | 1.80–1.99 | <0.001 *** | 1.61 | 1.58–1.65 | <0.001 *** |
| Cough etiquette | 1.33 | 1.28–1.39 | <0.001 *** | 1.44 | 1.30–1.60 | <0.001 *** | 1.34 | 1.29–1.40 | <0.001 *** |
| Avoid crowds | 1.16 | 1.18–1.19 | <0.001 *** | 1.37 | 1.26–1.49 | <0.001 *** | 1.19 | 1.16–1.23 | <0.001 *** |
| Get plenty of rest | 1.00 | 0.97–1.04 | 0.9334 | 1.26 | 1.16–1.36 | <0.001 *** | 1.04 | 1.01–1.08 | 0.0081 ** |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuoka, T.; Sato, T.; Akita, T.; Yanagida, J.; Ohge, H.; Kuwabara, M.; Tanaka, J. High Vaccination Coverage among Children during Influenza A(H1N1)pdm09 as a Potential Factor of Herd Immunity. Int. J. Environ. Res. Public Health 2016, 13, 1017. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13101017
Matsuoka T, Sato T, Akita T, Yanagida J, Ohge H, Kuwabara M, Tanaka J. High Vaccination Coverage among Children during Influenza A(H1N1)pdm09 as a Potential Factor of Herd Immunity. International Journal of Environmental Research and Public Health. 2016; 13(10):1017. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13101017
Chicago/Turabian StyleMatsuoka, Toshihiko, Tomoki Sato, Tomoyuki Akita, Jiturou Yanagida, Hiroki Ohge, Masao Kuwabara, and Junko Tanaka. 2016. "High Vaccination Coverage among Children during Influenza A(H1N1)pdm09 as a Potential Factor of Herd Immunity" International Journal of Environmental Research and Public Health 13, no. 10: 1017. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13101017