Microbial Risk Assessment of Tidal−Induced Urban Flooding in Can Tho City (Mekong Delta, Vietnam)


Abstract
:1. Introduction
2. Materials and Methods
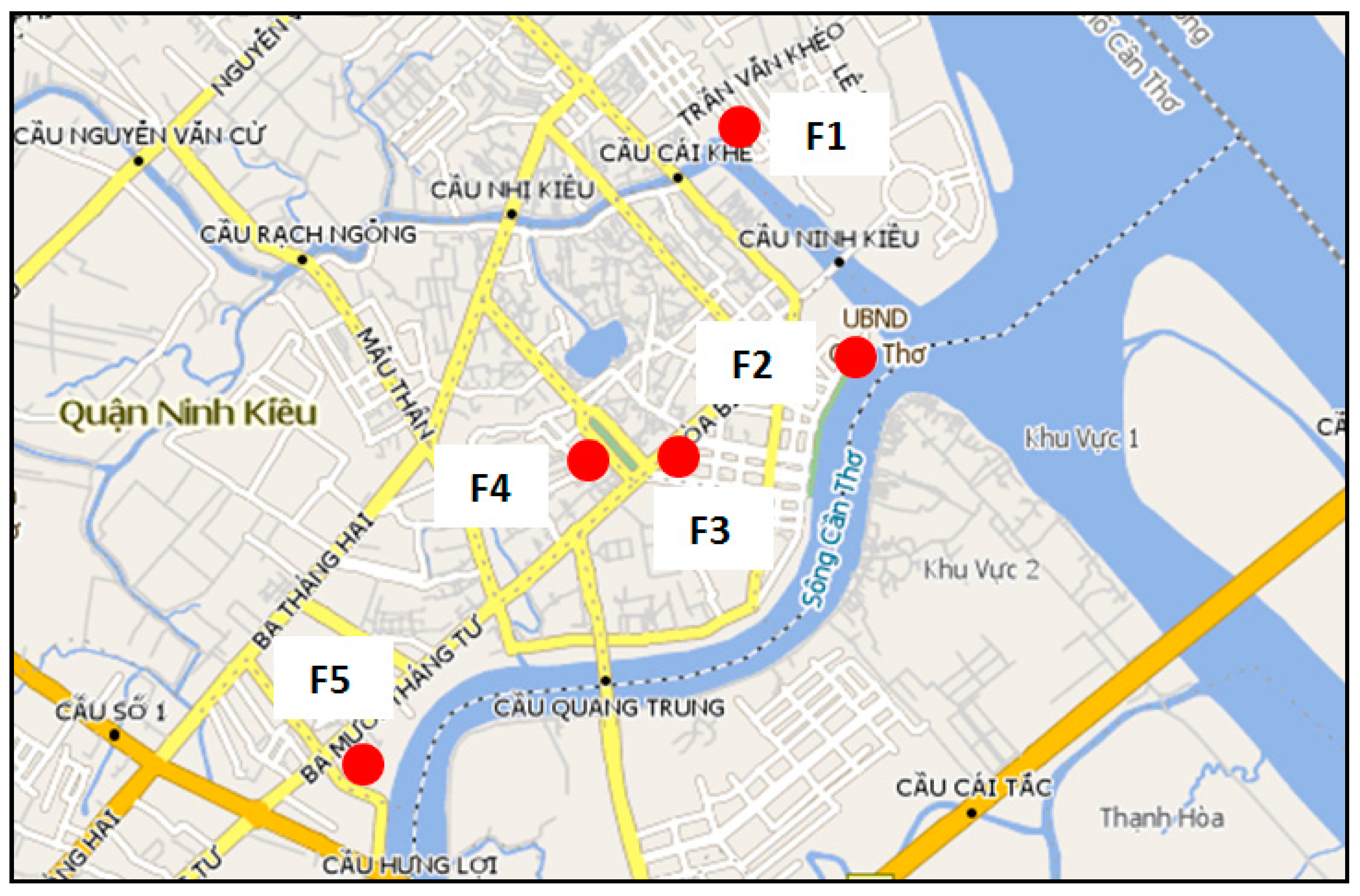
2.1. Study Site
2.2. Flooded Water Sampling and Analysis
2.3. Quantitative Microbial Risk Assessment (QMRA)
2.3.1. Hazard Identification
2.3.2. Exposure Assessment
2.3.3. Dose-Response Relations and Risk Identification
3. Results and Discussion
3.1. Quantitative Microbial Risk Assessment
3.1.1. Hazard Identification
3.1.2. Exposure Assessment
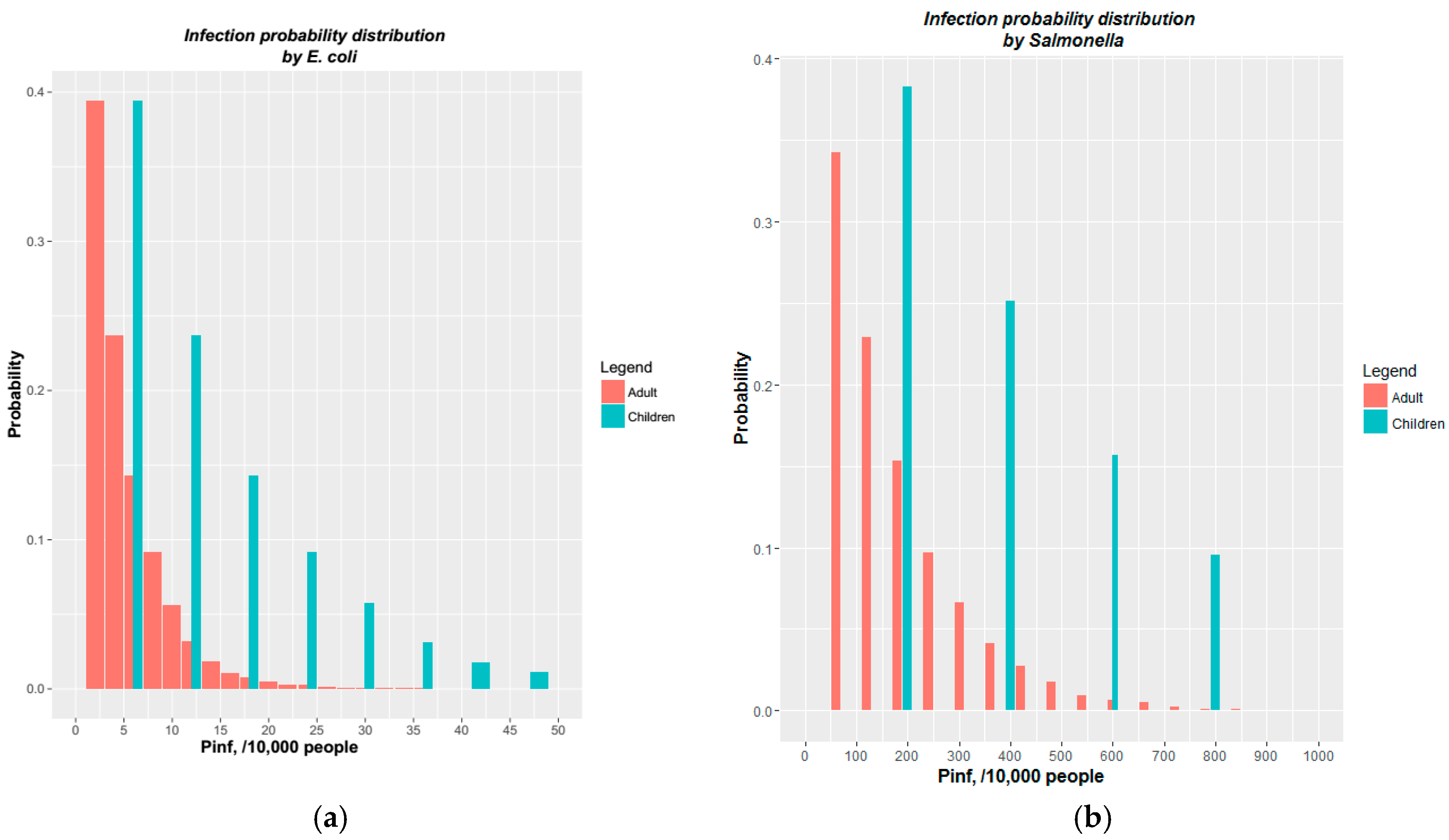
3.1.3. Dose-Response Relations and Risk Identification
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kovats, S.; Akhtar, R. Climate, climate change and human health in Asian cities. Environ. Urban 2008, 20, 165–175. [Google Scholar] [CrossRef]
- Novotny, V. (Ed.) Nonpoint Pollution and Urban Stormwater Management; TECHNOMIC: Lancaster, PA, USA, 1995; Volume 9, p. 434. [Google Scholar]
- Campbell, N.; D’Arcy, B.; Frost, A.; Novotny, V.; Sansom, A. (Eds.) Diffuse Pollution: An Introduction to the Problems and Solutions; IWA Publishing: London, UK, 2005; p. 328. [Google Scholar]
- Gao, L.; Zhang, Y.; Ding, G.; Liu, Q.; Jiang, B. Identifying Flood-Related Infectious Diseases in Anhui Province, China: A Spatial and Temporal Analysis. Am. J. Trop. Med. Hyg. 2016, 94, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Bokhari, H.; Shah, M.A.; Asad, S.; Akhtar, S.; Akram, M.; Wren, B.W. Escherichia coli pathotypes in Pakistan from consecutive floods in 2010 and 2011. Am. J. Trop. Med. Hyg. 2013, 88, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, L.; Kay, D. Flooding and Health—A Review of the Literature; Working Paper; Flood Risk Management Research Consortium, University of Wales: Aberystwyth, UK, 2006. [Google Scholar]
- Fewtrell, L.; Kay, D.; Watkins, J.; Davies, C.; Francis, C. The microbiology of urban UK floodwaters and a quantitative microbial risk assessment of flooding and gastrointestinal illness. J. Flood Risk Manag. 2011, 4, 77–87. [Google Scholar] [CrossRef]
- Kovats, R.S.; Campbell-Lendrum, D.; Matthies, F. Climate change and human health: Estimating avoidable deaths and disease. Risk Anal. 2005, 25, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Labite, H.; Lunani, I.; Van Der Steen, P.; Vairavamoorthy, K.; Drechsel, P.; Lens, P. Quantitative microbial risk analysis to evaluate health effects of interventions in the urban water system of Accra, Ghana. J. Water Health 2010, 8, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Moors, E.; Singh, T.; Siderius, C.; Balakrishnan, S.; Mishra, A. Climate change and waterborne diarrhoea in northern India: Impacts and adaptation strategies. Sci. Total Environ. 2013, 468–469, 139–151. [Google Scholar] [CrossRef] [PubMed]
- Pham, D.P.; Nguyen-Viet, H.; Hattendorf, J.; Zinsstag, J.; Phung, D.C.; Odermatt, P. Risk factors for Entamoeba histolytica infection in an agricultural community in Hanam province, Vietnam. Parasites Vectors 2011, 4, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuhrimann, S.; Pham-Duc, P.; Cisse, G.; Tram, N.T.; Ha, H.T.; Dung, D.T.; Ngoc, P.; Nguyen-Viet, H.; Anh Vuong, T.; Utzinger, J.; et al. Microbial contamination along the main open wastewater and storm water channel of Hanoi, Vietnam, and potential health risks for urban farmers. Sci. Total Environ. 2016, 566–567, 1014–1022. [Google Scholar] [CrossRef] [PubMed]
- Le-Thi, T.; Pham-Duc, P.; Zurbrugg, C.; Luu-Quoc, T.; Nguyen-Mai, H.; Vu-Van, T.; Nguyen-Viet, H. Diarrhea risks by exposure to livestock waste in Vietnam using quantitative microbial risk assessment. Int. J. Public Health 2017, 62, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, A.; Nguyen-Viet, H.; Zinsstag, J. Quantification of diarrhea risk related to wastewater contact in Thailand. Ecohealth 2012, 9, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Thy, P.M.; Raghavan, V.; Pawarr, N.J. Urban Expansion of Can Tho City, Vietnam: A Study based on Multi-Temporal Satellite Images. Geoinformatics 2010, 21, 147–160. [Google Scholar]
- Huong, H.T.L.; Pathirana, A. Urbanization and climate change impacts on future urban flooding in Can Tho city, Vietnam. Hydrol. Earth Syst. Sci. 2013, 17, 379–394. [Google Scholar] [CrossRef]
- Ozaki, H.; Co, T.K.; Le, A.K.; Pham, V.N.; Nguyen, V.B.; Tarao, M.; Nguyen, H.C.; Le, V.D.; Nguyen, H.T.; Sagehashi, M.; et al. Human factors and tidal influences on water quality of an urban river in Can Tho, a major city of the Mekong Delta, Vietnam. Environ. Monit. Assess. 2014, 186, 845–858. [Google Scholar] [CrossRef] [PubMed]
- People Committee in Can Tho City (CTPC). Social-Economic Survey in Can Tho City (Project CTUDR); People Committee in Can Tho City (CTPC): Can Tho City, Vietnam, 2015; p. 138.
- Ahern, M.; Kovats, R.S.; Wilkinson, P.; Few, R.; Matthies, F. Global health impacts of floods: Epidemiologic evidence. Epidemiol. Rev. 2005, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Katukiza, A.Y.; Ronteltap, M.; van der Steen, P.; Foppen, J.W.; Lens, P.N.L. Quantification of microbial risks to human health caused by waterborne viruses and bacteria in an urban slum. J. Appl. Microbiol. 2013, 116, 447–463. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.N.; Rose, J.B.; Gerba, C.P. Quantiative Microbial Risk Assessment; Wiley: New York, NY, USA, 1999; p. 448. [Google Scholar]
- Ten Veldhuis, J.; Clemens, F.; Sterk, G.; Berends, B. Microbial risks associated with exposure to pathogens in contaminated urban flood water. Water Res. 2010, 44, 2910–2918. [Google Scholar] [CrossRef] [PubMed]
- Sales-Ortells, H.; Medema, G. Screening-Level Microbial Risk Assessment of Urban Water Locations: A Tool for Prioritization. Environ. Sci. Technol. 2014, 48, 9780–9789. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.Q.; Radhakrishnan, M.; Huynh, T.T.N.; Baino-Salingay, M.L.; Ho, L.P.; Steen, P.V.D.; Pathirana, A. Water Quality Dynamics of Urban Water Bodies during Flooding in Can Tho City, Vietnam. Water 2017, 9, 260. [Google Scholar] [CrossRef]
- The World Bank (WB). Can Tho, Vietnam_Enhancing Urban Resilience; The World Bank (WB) Group: Washington, DC, USA, 2014; p. 42. [Google Scholar]
- Howard, G.; Ahmed, M.F.; Mahmud, S.G.; Teunis, P.; Davison, A.; Deere, D. Disease burden estimation to support policy decision-making and research prioritization for arsenic mitigation. J. Water Health 2007, 5, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.N.; Rose, J.B.; Gerba, C.P. Quantitative Microbial Risk Assessment, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2014; p. 427. [Google Scholar]
- European Union (EU). Directive 2006/7/EC of the European Parliament and of the Council Concerning the Management of Bathing Water Quality and Repealing Directive 76/160/EEC; Official Journal of the European Union (EU): Strasbourg, France, 2006; p. 15. [Google Scholar]
- Cho, K.H.; Han, D.; Park, Y.; Lee, S.W.; Cha, S.M.; Kang, J.-H.; Kim, J.H. Evaluation of the relationship between two different methods for enumeration fecal indicator bacteria: Colony-forming unit and most probable number. J. Environ. Sci. 2010, 22, 5. [Google Scholar] [CrossRef]
- Huynh, T.T.N. Health Risk from Exposure to Urban Flood Water. Case Study: Ninh Kieu District (Can Tho City, Vietnam); Bach Khoa University: Ho Chi Minh City, Vietnam, 2014. (In Vietnamese) [Google Scholar]
- Phung, D.; Huang, C.; Rutherford, S.; Chu, C.; Wang, X.; Nguyen, M.; Nguyen, N.H.; Manh, C.D.; Nguyen, T.H. Association between climate factors and diarrhoea in a Mekong Delta area. Int. J. Biometeorol. 2015, 59, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- People’s Committee of Can Tho City (CTPC). Social—Economic Report for Can Tho Urban Development and Strengthening Adaptation Project; People’s Committee of Can Tho City (CTPC): Can Tho City, Vietnam, 2015; (In Vietnamese).
- Phung, D.; Chu, C.; Rutherford, S.; Nguyen, H.L.; Luong, M.A.; Do, C.M.; Huang, C. Heavy rainfall and risk of infectious intestinal diseases in the most populous city in Vietnam. Sci. Total Environ. 2017, 580, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.Q.; Huynh, T.T.N.; Van Der Steen, P.; Ho, L.P.; Pathirana, A.; Nguyen, D.H.; Salingay, M.L.B. Water pollution and health risk caused by urban flooding in Can Tho City: Lesson learnt from the field campaigns 2013. In In Proceedings of the 19th IAHR-APD 2014 Congress, Hanoi, Vietnam, 21–24 September 2014; pp. 1–6. [Google Scholar]
- De Man, H.; van den Berg, H.H.J.L.; Leenen, E.J.T.M.; Schijven, J.F.; Schets, F.M.; van der Vliet, J.C.; van Knapen, F.; de Roda Husman, A.M. Quantitative assessment of infection risk from exposure to waterborne pathogens in urban floodwater. Water Res. 2014, 48, 90–99. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Pathogens | μ | N50 |
|---|---|---|
| E. coli | 0.1952 | 3.01× 107 |
| Salmonella | 0.3126 | 2.36 × 104 |
| Campylobacter | 0.1450 | 896 |
| Rotavirus | 0.2531 | 6.17 |
| n | Mean | SD | Median | ||
|---|---|---|---|---|---|
| E. coli (measured) | MPN/100 mL | 20 | 1.84 × 104 | 2.09 × 104 | 1.00 × 104 |
| E. coli (simulated) | MPN/100 mL | 10,000 | 1.83 × 104 | 1.83 × 104 | 1.26 × 104 |
| Difference (%) | 0.37 | 14.31 | 20.52 | ||
| Salmonella (measured) | MPN/100 mL | 20 | 1.33 × 103 | 2.03 × 103 | 7.00 × 102 |
| Salmonella (simulated) | MPN/100 mL | 10,000 | 1.34 × 103 | 1.35 × 103 | 9.23 × 102 |
| Difference (%) | 1.18 | 50.44 | 24.16 | ||
| Mean | SD | Max | 95 Percentile | |||||
|---|---|---|---|---|---|---|---|---|
| Adu. | Chi. | Adu. | Chi. | Adu. | Chi. | Adu. | Chi. | |
| E. coli | 1.8 × 103 | 5.5 × 103 | 1.8 × 103 | 5.5 × 103 | 2.2 × 104 | 6.5 × 104 | 5.5 × 103 | 1.7 × 104 |
| Salmonella | 1.3 × 102 | 4.0 × 102 | 1.3 × 102 | 3.9 × 102 | 1.3 × 103 | 4.0 × 103 | 3.9 × 102 | 1.2 × 103 |
| Rotaviruses | 1.8 × 10−2 | 5.5 × 10−2 | 1.8 × 10−2 | 5.5 × 10−2 | 2.2 × 10−1 | 6.5 × 10−1 | 5.5 × 10−2 | 1.7 × 10−1 |
| Campylobacter | 1.8 × 10−2 | 5.5 × 10−2 | 1.8 × 10−2 | 5.5 × 10−2 | 2.2 × 10−1 | 6.5 × 10−1 | 5.5 × 10−2 | 1.7 × 10−1 |
| Cryptosporidium | 1.8 × 10−3 | 5.5 × 10−3 | 1.8 × 10−3 | 5.5 × 10−3 | 2.2 × 10−2 | 6.5 × 10−2 | 5.5 × 10−3 | 1.7 × 10−2 |
| Mean | SD | Max | 95 Percentile | |||||
|---|---|---|---|---|---|---|---|---|
| Adu. | Chi. | Adu. | Chi. | Adu. | Chi. | Adu. | Chi. | |
| E. coli | 4 | 12 | 4 | 12 | 36 | 105 | 12 | 35 |
| Salmonella | 137 | 374 | 131 | 329 | 1005 | 2196 | 402 | 1040 |
| Rotaviruses | 103 | 284 | 98 | 252 | 793 | 1769 | 299 | 786 |
| Campylobacter | 3 | 10 | 3 | 10 | 31 | 91 | 10 | 31 |
| Cryptosporidium | 0.08 | 0.25 | 0.08 | 0.25 | 0.74 | 2.22 | 0.24 | 0.73 |
| QCVN 01/2009/BYT | QCVN 08/2008/BTNMT | QCVN 10/2008/BTNMT | EU Directive 2006/7/EC | |
|---|---|---|---|---|
| Coliform | 50–150 | 2500–5000 | 1000 | - |
| E. coli | 0–20 | 20–50 | - | 200–500 (*) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, H.Q.; Huynh, T.T.N.; Pathirana, A.; Van der Steen, P. Microbial Risk Assessment of Tidal−Induced Urban Flooding in Can Tho City (Mekong Delta, Vietnam). Int. J. Environ. Res. Public Health 2017, 14, 1485. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121485
Nguyen HQ, Huynh TTN, Pathirana A, Van der Steen P. Microbial Risk Assessment of Tidal−Induced Urban Flooding in Can Tho City (Mekong Delta, Vietnam). International Journal of Environmental Research and Public Health. 2017; 14(12):1485. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121485
Chicago/Turabian StyleNguyen, Hong Quan, Thi Thao Nguyen Huynh, Assela Pathirana, and Peter Van der Steen. 2017. "Microbial Risk Assessment of Tidal−Induced Urban Flooding in Can Tho City (Mekong Delta, Vietnam)" International Journal of Environmental Research and Public Health 14, no. 12: 1485. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121485