A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases


Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria and Study Selection
2.3. Assessment of Risk of Bias for Each Eligible Study
2.4. Data Extraction and Synthesis
3. Results
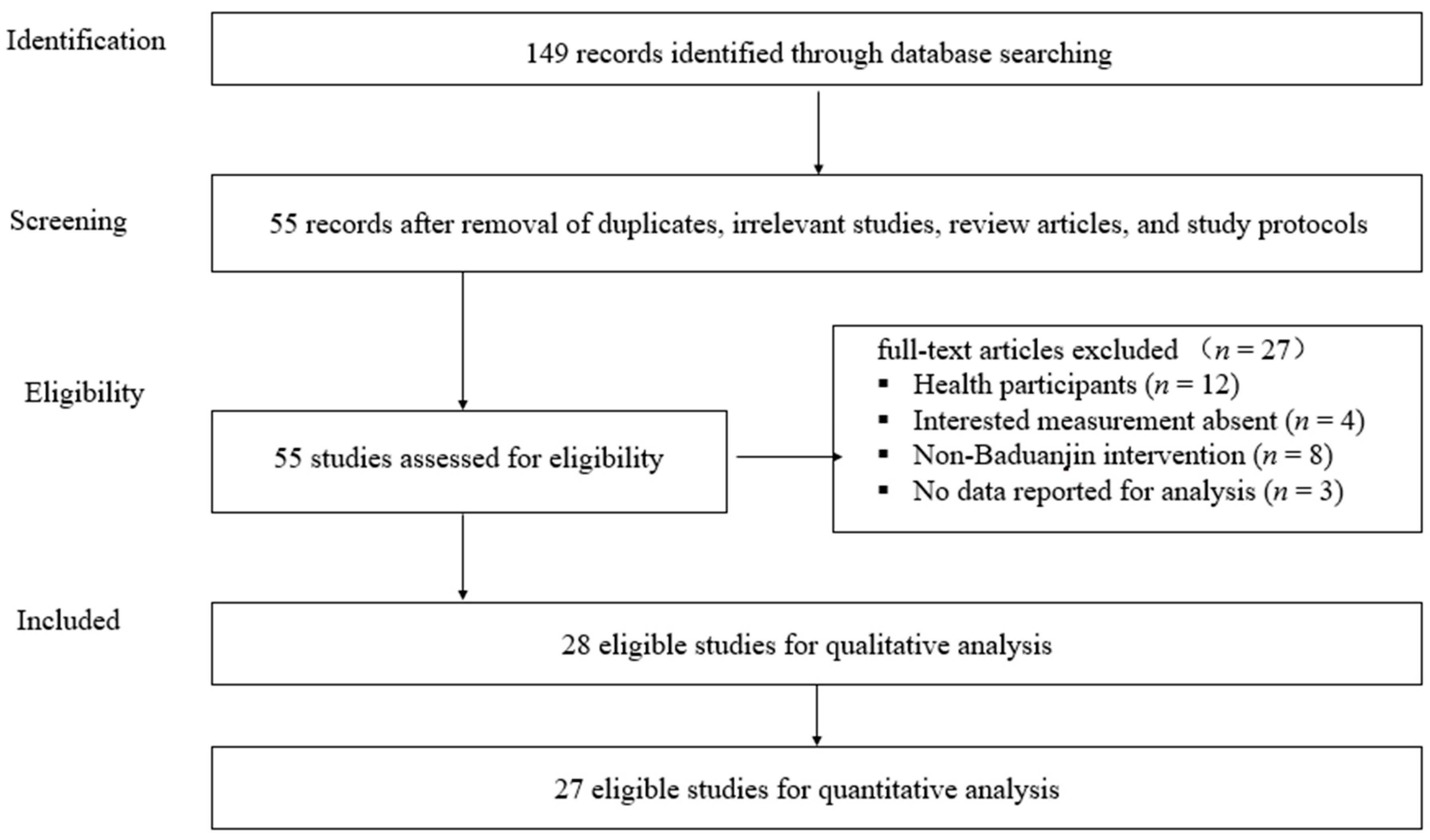
3.1. Literature Search
3.2. Study Characteristics
3.3. Methodological Quality
3.4. Effects of Baduanjin on Musculoskeletal Pain and Overall Sleep Quality
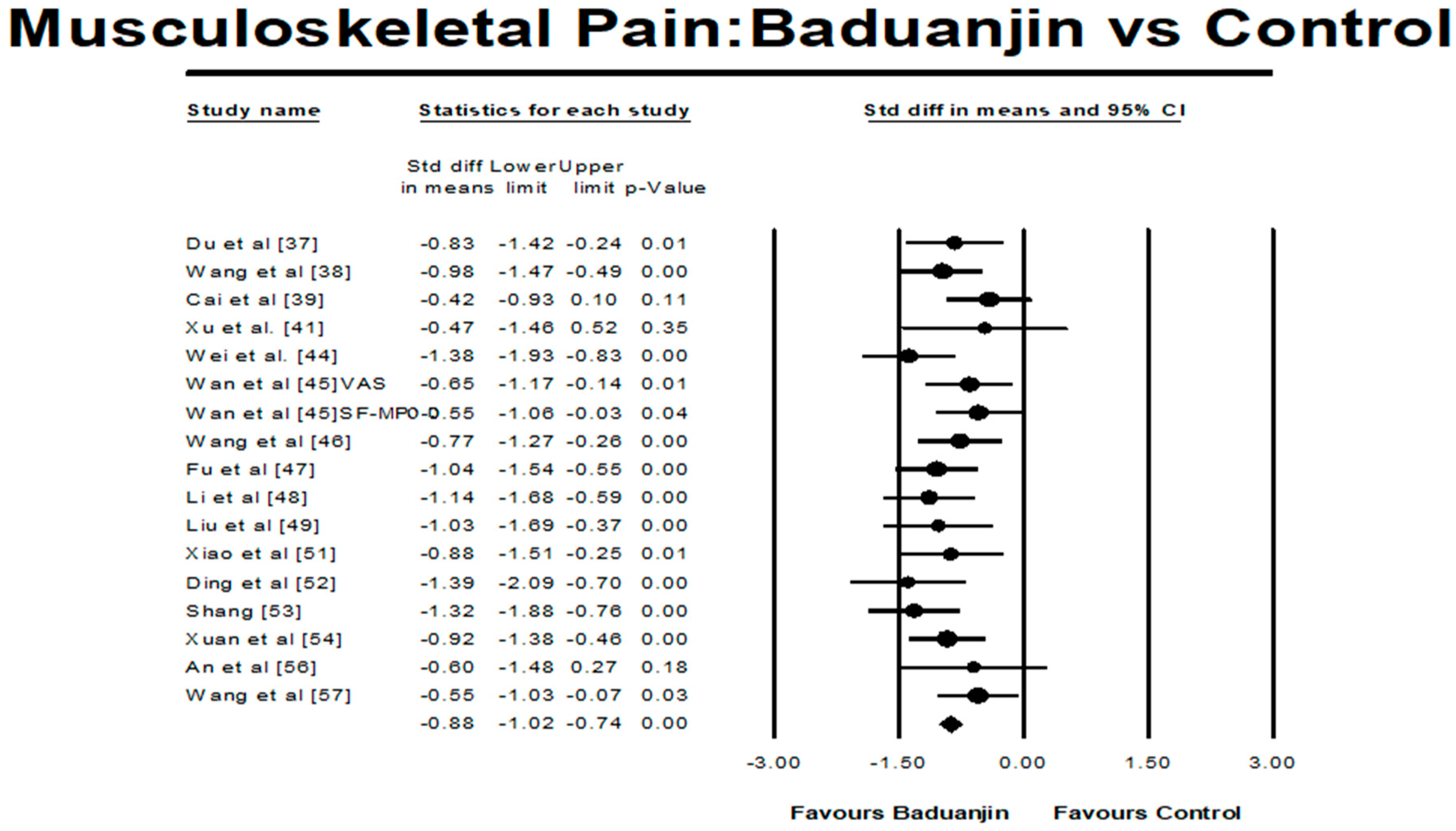
3.4.1. Baduanjin Intervention versus Control Group on Musculoskeletal Pain
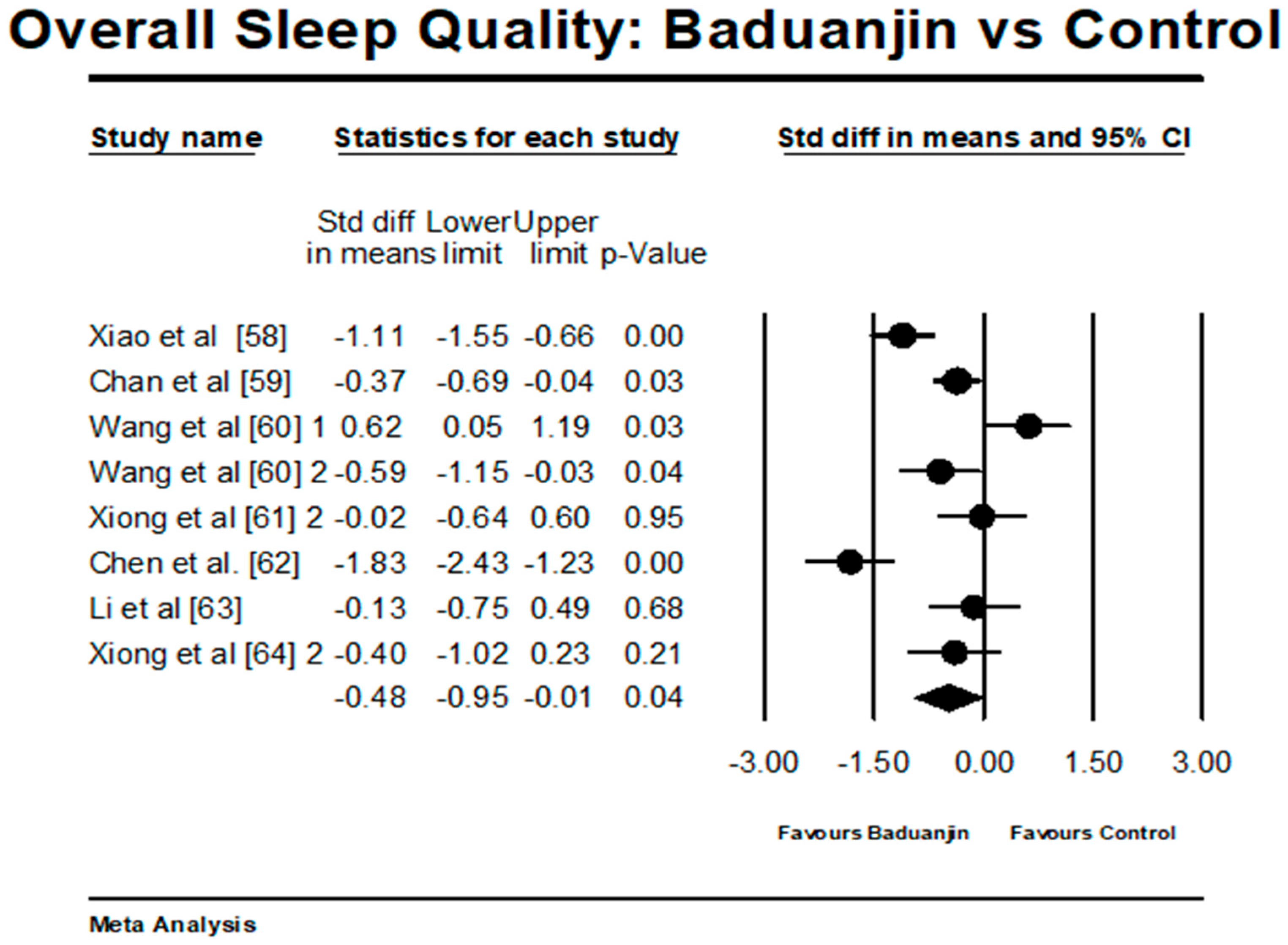
3.4.2. Baduanjin Intervention versus Control Group on Overall Sleep Quality
3.4.3. Moderator Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, J.; Jensen, M.K.; Sjøgren, P.; Ekholm, O.; Rasmussen, N.K. Epidemiology of chronic non-malignant pain in Denmark. Pain 2003, 106, 221–228. [Google Scholar] [CrossRef]
- Rustøen, T.; Wahl, A.K.; Hanestad, B.R.; Lerdal, A.; Paul, S.; Miaskowski, C. Prevalence and characteristics of chronic pain in the general Norwegian population. Eur. J. Pain 2004, 8, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.F.J.; Tsui, S.L.; Chan, W.S. Prevalence of common chronic pain in Hong Kong adults. Clin. J. Pain 2002, 18, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Yeo, S.N.; Tay, K.H. Pain prevalence in Singapore. Ann. Acad. Med. Singap. 2009, 38, 937–942. [Google Scholar] [PubMed]
- Nakamura, M.; Nishiwaki, Y.; Ushida, T.; Toyama, Y. Prevalence and characteristics of chronic musculoskeletal pain in Japan. J. Orthop. Sci. 2011, 16, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Dellaroza, M.S.G.; Pimenta, C.A.M.; Matsuo, T. Prevalência e caracterização da dor crônica em idosos não institucionalizados. Cad. Saude Publica 2007, 23, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Pai, L.-W.; Hung, C.-T.; Li, S.-F.; Chen, L.-L.; Chung, Y.-C.; Liu, H.-L. Musculoskeletal pain in people with and without type 2 diabetes in Taiwan: A population-based, retrospective cohort study. BMC Musculoskelet. Disord. 2015, 16, 364. [Google Scholar] [CrossRef] [PubMed]
- Baysal, O.; Durmus, B.; Ersoy, Y.; Altay, Z.; Senel, K.; Nas, K.; Ugur, M.; Kaya, A.; Gur, A.; Erdal, A.; et al. Relationship between psychological status and disease activity and quality of life in ankylosing spondylitis. Rheumatol. Int. 2011, 31, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Suri, P.; Morgenroth, D.C.; Kwoh, C.K.; Bean, J.F.; Kalichman, L.; Hunter, D.J. Low back pain and other musculoskeletal pain comorbidities in individuals with symptomatic osteoarthritis of the knee: Data from the osteoarthritis initiative. Arthritis Care Res. 2010, 62, 1715–1723. [Google Scholar] [CrossRef] [PubMed]
- Miranda, V.S.; deCarvalho, V.B.; Machado, L.A.; Dias, J.M. Prevalence of chronic musculoskeletal disorders in elderly Brazilians: A systematic review of the literature. BMC Musculoskelet. Disord. 2012, 13, 82. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (Internet). NIH Guide: New Directions in Pain Research: I; National Institutes of Health: Bethesda, MD, USA, 1988.
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Phillips, C.J. The Cost and Burden of Chronic Pain. Rev. Pain 2009, 3, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Tüzün, E.H. Quality of life in chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2007, 21, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Bingefors, K.; Isacson, D. Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain-a gender perspective. Eur. J. Pain 2004, 8, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Moulin, D.E. Systemic drug treatment for chronic musculoskeletal pain. Clin. J. Pain 2001, 17, S86–S93. [Google Scholar] [CrossRef] [PubMed]
- Ndlovu, M.; Bedson, J.; Jones, P.W.; Jordan, K.P. Pain medication management of musculoskeletal conditions at first presentation in primary care: Analysis of routinely collected medical record data. BMC Musculoskelet. Disord. 2014, 15, 418. [Google Scholar] [CrossRef] [PubMed]
- Martel, M.O.; Finan, P.H.; Dolman, A.J.; Subramanian, S.; Edwards, R.R.; Wasan, A.D.; Jamison, R.N. Self-reports of medication side effects and pain-related activity interference in patients with chronic pain: A longitudinal cohort study. Pain 2015, 156, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Feine, J.S.; Lund, J.P. An assessment of the efficacy of physical therapy and physical modalities for the control of chronic musculoskeletal pain. Pain 1997, 71, 5–23. [Google Scholar] [CrossRef]
- Carlson, H.; Carlson, N. An overview of the management of persistent musculoskeletal pain. Ther. Adv. Musculoskelet. Dis. 2011, 3, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.L.; Koes, B.W.; De Vet, H.C.W.; Van der Windt, D.A.W.M.; Assendelft, W.J.J.; Van Mameren, H.; Devillé, W.L.J.M.; Pool, J.J.M.; Scholten, R.J.P.M.; Bouter, L.M. Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain: A randomized, controlled trial. Ann. Intern. Med. 2002, 136, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Korthals-de Bos, I.B.C.; Hoving, J.L.; van Tulder, M.W.; Rutten-van Mölken, M.P.M.; Adèr, H.J.; de Vet, H.C.W.; Koes, B.W.; Vondeling, H.; Bouter, L.M. Cost effectiveness of physiotherapy, manual therapy, and general practitioner care for neck pain: Economic evaluation alongside a randomised controlled trial. BMJ 2003, 326, 911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T.; Du, G.; Liu, Y. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A systematic review and meta-analysis of Baduanjin Qigong for health benefits: Randomized controlled trials. Evid. Based Complement. Altern. Med. 2017, 2017, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and musculoskeletal flexibility in healthy Chinese older women. Sports 2017, 5, 52. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The effect of Taichi practice on attenuating bone mineral density loss: A systematic review and meta-analysis of randomized controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Wang, H. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener Dis. 2017, 2, 46–52. [Google Scholar] [CrossRef]
- Zou, L.; Xiao, Z.; Wang, H. Martial arts for health benefits in children and youth with autism spectrum disorder: A systematic review. Arch. Budo 2017, 13, 79–92. [Google Scholar]
- Lou, L.; Zou, L.; Fang, Q.; Wang, H.; Liu, Y.; Tian, Z.; Han, Y. Effect of Taichi softball on function-related outcomes in older adults: A randomized control trial. Evid. Based Complement. Altern. Med. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Pan, Z.; Yeung, A.; Talwar, S.; Wang, C.; Liu, Y.; Shu, Y.; Chen, X.; Thomas, G.A. A review study on the beneficial effects of Baduanjin. J. Altern. Complement. Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Schmid, C.H.; Iversen, M.D.; Harvey, W.F.; Fielding, R.A.; Driban, J.B.; Price, L.L.; Wong, J.B.; Reid, K.F.; Rones, R.; et al. Comparative effectiveness of Tai Chi versus physical therapy for knee osteoarthritis: A randomized trial. Ann. Intern. Med. 2016, 165, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C. Traditional Chinese Baduanjin Qigong for older adults: A mini-review. Open Access J. Gerontol. Geriatr. Med. 2017, 1, 555561. [Google Scholar]
- Zou, L.; Cui, Y.; Wang, H.; Li, T.; Lu, M.; Wang, C. Effects of traditional Chinese mind-body exercise on disease activity, spinal mobility, and quality of life in patients with ankylosing spondylitis. Trav. Hum. 2017, 80, 1587–1597. [Google Scholar]
- Antonishen, K. Exercise mode heterogeneity among reported studies of the qigong practice Baduanjin. J. Bodyw. Mov. Ther. 2015, 19, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.-C.; Wang, T.-S.; Liu, Y.-P.; Liu, C.-F. Effects of Baduanjin exercise on oxidative stress and antioxidant status and improving quality of life among middle-aged women. Am. J. Chin. Med. 2008, 36, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Du, H.; Liu, J.; Qin, J. Effect of Baduanjin on pain relief in people with discogenic low back pain. Chin. J. Conval. Med. 2017, 26, 482–484. [Google Scholar]
- Wang, C.; Guo, Z.; Chen, Z. Study on the effects of Baduanjin exercise on patients with scapulohumeral pariarthritis. Chin. J. Sports Med. 2010, 29, 285–287. [Google Scholar]
- Cai, J.; Xiao, H.; Shi, X.; Liu, T. Effect of Baduanjin on pain in patients with nerve-root type cervical spondylosis. Guid. J. Tradit. Chin. Med. Pharm. 2015, 21, 98–99. [Google Scholar]
- Li, C.; He, S.; Wu, B.; Wang, L. The effects of Baduanjin exercise on pain and flexibility in people with scapulohumeral periarthritis. Liaoning Sports Sci. Technol. 2010, 32, 43–52. [Google Scholar]
- Xu, H.; Chen, X.; Ji, C.; Zhang, W.; Huang, X.; Lu, Y. Effects of Baduanjin exercise on serum interleukin-1 beta, interleukin-6, and tumor necrosis factor-alpha in patients with lumbar disc herniation. Hunan J. Tradit. Chin. Med. 2015, 31, 16–18. [Google Scholar]
- Chen, Y.; Xiong, X.; Liu, H.; Liu, X.; Chen, Y.; Wang, S.; Xiong, Q.; Wen, Y. Effect of Baduanjin on musculoskeletal pain and quality of life in older adults. China Naturop. 2017, 25, 18–19. [Google Scholar]
- Da Costa, B.R.; Hilfiker, R.; Egger, M. PEDro’s bias: Summary quality scores should not be used in meta-analysis. J. Clin. Epidemiol. 2013, 66, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Wer, R.; Li, Y.; Guo, Y.; Yin, Z. Effects of Baduanjin on physical function and pan in people with ankylosing spondylitis. J. North Med. 2012, 9, 67–68. [Google Scholar]
- Wan, J.; Liang, Z.; Sun, K.; Wu, J.; Ding, X. Combination of Gongfa exercise Baduanjin and manipulation for the treatment of myofascial pain syndrome on shoulder and neck. Shanghai J. Tradit. Chin. Med. 2013, 47, 54–56. [Google Scholar]
- Wang, C.; Guo, Z.; Chen, Z. Effect of Baduanjin on disease-specific symptoms in patients with scapulohumeral periarthritis. Chin. J. Conval. Med. 2009, 18, 1074–1076. [Google Scholar]
- Fu, J.; Tang, R.; Li, X.; Tian, X. The influence of Baduanjin on somatic function and mental health in patients with ankylosing spondylitis. West. J. Tradit. Chin. Med. 2016, 29, 124–126. [Google Scholar]
- Li, L.; Feng, Z. Clinical observation of treating chronic nonspecific low back pain with Baduanjin combining sling exercise therapy. Rheum. Arthritis 2015, 4, 16–19. [Google Scholar]
- Liu, H.; Chen, Y.; Yi, X.; Zhang, Y.; Zhou, Q.; Yu, L. Effect of Baduanjin on physical and mental regulation in patients with type 2 diabetic mellitus with anxiety. Hunan J. Tradit. Chin. Med. 2014, 30, 16–18. [Google Scholar]
- Wang, C.; Liu, L. Effect of 4-week Baduanjin on musculoskeletal pain in patients with scapulohumeral periarthritis. World J. Sports 2009, 5, 24–26. [Google Scholar]
- Xiao, B.; Yuan, S.; Fang, L. Effect of Baduanjin on pain relief in patients with patients with cervical spondylotic radiculopathy. Clin. Res. 2003, 19, 11–12. [Google Scholar]
- Ding, Y.; Wang, J. Effect of Baduanjin on pain in people with chronic low back pain. Chin. J. Gerontol. 2014, 29, 151–152. [Google Scholar]
- Shang, Q. Effect of Baduanjin on pain in patients with lumbar disc herniation. China Foreign Med. Treat. 2014, 29, 151–152. [Google Scholar]
- Xuan, S.; Tao, S.; He, T.; Luo, Y.; Wang, J.; Duan, X.; Zhou, L.; Ding, J.; Song, Y.; Chu, X. Effect of Baduanjin on symptoms in patients with chronic neck pain. J. Sichuan Tradit. Chin. Med. 2016, 34, 188–190. [Google Scholar]
- Peng, X.; Li, Q.; Li, X. The efficacy of sitting Baduanjin exercise on lumbago and back pain of elderly patients with osteoporosis. J. Nurs. Sci. 2015, 20, 4–6. [Google Scholar]
- An, B.; Dai, K.; Zhu, Z.; Wang, Y.; Hao, Y.; Tang, T.; Yan, H. Baduanjin alleviates the symptoms of knee osteoarthritis. J. Altern. Complement. Med. 2008, 14, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Guo, H.; Tang, L.; Meng, J.; Hu, L.Y. Case-control study on regular Ba Duan Jin practice for patients with chronic neck pain. Int. J. Nurs. Sci. 2014, 1, 360–366. [Google Scholar] [CrossRef]
- Xiao, C.M.; Zhuang, Y.C. Effect of health Baduanjin Qigong for mild to moderate Parkinson’s disease. Geriatr. Gerontol. Int. 2016, 16, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.M.; Ho, R.T.H.; Chung, K.F.; Wang, C.W.; Yao, T.J.; Ng, S.M.; Chan, C.L.W. Qigong exercise alleviates fatigue, anxiety, and depressive symptoms, improves sleep quality, and shortens sleep latency in persons with chronic fatigue syndrome-like illness. Evid. Based Complement. Altern. Med. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Wang, W.; Zhang, R.; Lin, Y.; Hong, L.; Zhao, Y.; Ni, Q. Influence of different Qigong practices on sleep quality in patients with type 2 diabetes accompanied by insomnia. J. Beijing Univ. Tradit. Chin. Med. 2009, 32, 636–640. [Google Scholar]
- Xiong, G.; Sun, H. Clinical research of Baduanjin combined with Ziwuliuzhu Nazhi acupuncture method in treatment of insomnia. China Med. Pharm. 2016, 6, 48–50. [Google Scholar]
- Chen, Y.; Liu, R.; He, R. Effect of Baduanjin on sleep quality in older people with hypertension. Hunan J. Tradit. Chin. Med. 2015, 31, 52–54. [Google Scholar]
- Li, L.; Wang, N. Research progress of Baduanjin in the treatment of insomnia patients with type 2 diabetes. Neimenggu Chin. Med. 2014, 27, 86–87. [Google Scholar]
- Xiong, G.; Liu, X. Influence research of Baduanj in combined with acupuncture in insomnia (deficiency type of heart and spleen). China Med. Pharm. 2015, 5, 65–67. [Google Scholar]
- An, B.; Wang, Y.; Jiang, X.; Lu, H.; Fang, Z.; Wang, Y.; Dai, K. Effects of Baduanjin (八段锦) exercise on knee osteoarthritis: A one-year study. Chin. J. Integr. Med. 2013, 19, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Matos, L.C.; Sousa, C.M.; Goncąlves, M.; Gabriel, J.; MacHado, J.; Greten, H.J. Qigong as a traditional vegetative biofeedback therapy: Long-term conditioning of physiological mind-body effects. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Reference] | Location, Language | ISZ (BJ/CG) | Drop-Out % | Study Participants | Intervention Protocol | Test Administration | Adverse Event; Follow-Up | |||||
| Health Status | Mean Age or Age Range | Training Duration and Dosage | Total Hours | Hours Weekly | Total Session | Outcome Measured | Blinded Assessor | |||||
| Du et al. [37], RCT | Qingdao, China (Chinese) | 48 (24/24) | 0% | People with Discogenic low back pain | age range from 38 to 56 | BJ: 5 × 40 min/week for 8 weeks + usual care CG: usual care | 27 | 3.33 | 40 | Pain (VAS) | NR | No/No |
| Wang et al. [38], RCT | Hangzhou, China (Chinese) | 76 (38/38) | 5.3% | People with scapulohumeral periarthritis | Age range from 40 to 66 | BJ: 5 × 60 min/week for 4 weeks + usual care CG: usual care | 20 | 5 | 20 | Pain (VAS) | NR | No/No |
| Cai et al. [39], RCT | Changsha, China (Chinese) | 60 (30/30) | 0% | patients with nerve-root type cervical spondylosis | A mean age of 50.4 | BJ: 7 × 60 min/week for 6 months + usual care CG: usual care | 168 | 7 | 168 | Pain (VAS) | NR | No/No |
| Li et al. [40], RCT | Xi‘an, China (Chinese) | 60 (20/20/20) | 0% | Patients scapulohumeral periarthritis | A mean age of 50.43 | BJ: 5 × 60 min/week for 6 months CG1: Twice per week (manual therapy) CG2: Drug therapy: | 120 | 5 | 120 | Pain (NR) | NR | No/No |
| Xu et al. [41], RCT | Suzhou, China (Chinese) | 16 (8/8) | 0% | Patients with lumbar disc herniation | A mean age of 48.1 | BJ: 7 × 60 min/week for 1 month + drug therapy CG: drug therapy | 28 | 7 | 28 | Pain (VAS) | NR | No/No |
| Chen et al. [42], RCT | Chengdu, China (Chinese) | 60 (30/30) | 0% | People with osteoporosis suffered bodily pain | Age range from 55 to 71 | BJ: 7 × 90 min/week for 8 weeks + usual care CG: usual care | 84 | 10.5 | 56 | Pain (VAS) | NR | No/No |
| Wei et al. [44], RCT | Liuzhou, China, (Chinese) | 62 (31/31) | 0% | People with ankylosing spondylitis | age range from 15 to 60 | BJ: 7 × 40 min/week for 3 months + drug therapy (as same below) CG: drug therapy | 56 | 4.67 | 84 | Pain (VAS) | NR | No/No |
| Wan et al. [45], RCT | Shanghai, China (Chinese) | 60 (30/30) | 0% | People with myofascial pain syndrome on shoulder and neck | A mean age of 41.92 | BJ: 7 × 60 min/week for 35 days + manual therapy (as same below) CG: 20 min manual therapy for 6 sessions | 35 | 7 | 35 | Pain (VAS and SF-MPQ) | NR | No/No |
| Wang et al. [46], RCT | Hangzhou, China, (Chinese) | 67 (34/33) | 3% | People with scapulohumeral periarthritis | Age range from 40 to 66 | BJ: 5 × 60 min/week for 3 months + usual care CG: usual care | 60 | 5 | 60 | Pain (VAS) | NR | NR/No |
| Fu et al. [47], RCT | Langzhou, China (Chinese) | 70 (35/35) | 0% | People with ankylosing spondylitis | Age range from 17 to 42 | BJ: 7 × 60 min/week for 6 months + drug therapy (as same below) CG: drug therapy | 168 | 7 | 168 | Pain (VAS) | NR | No/No |
| Li et al. [48], RCT | Jinan, China (Chinese) | 60 (30/30) | 0% | People with chronic low back pain | Age range from 35 to 60 | BJ: 5 × 60 min/week for 8 weeks CG: Sling exerciser therapy | 40 | 5 | 40 | Pain (VAS) | NR | No/6-month |
| Liu et al. [49], RCT | Changsha, China (Chinese) | 40 (20/20) | 0% | People with Type 2 diabetic mellitus | A mean age of 56 | BJ: 5 × 30 min/week for 6 months + drug therapy (as same below) CG: drug therapy | 60 | 2.5 | 120 | Pain (subscale of SAS) | NR | No/No |
| Wang, Liu et al. [50], RCT | Changsha, China (Chinese) | 60 (30/30) | 0% | People with scapulohumeral periarthritis | A mean age of 53.54 | BJ: 7 × 60 min/week for 30 days + acupuncture (as same below) CG: acupuncture therapy | 30 | 7 | 60 | Pain (NR) | NR | No/No |
| Xiao et al. [51], RCT | Shanghai, China (Chinese) | 44 (26/18) | 0% | patients with cervical spondylotic radiculopathy/chronic neck pain | A mean age of 51 | BJ: 7 × 60 min/week for 30 days + drug therapy CG: drug therapy | 30 | 7 | 30 | Pain (VAS) | NR | No/No |
| Ding et al. [52], RCT | Hefei, China (Chinese) | 40 (22/18) | 0% | people with chronic low back pain | A mean age of 60.98) | BJ: 5 × 40 min/week for 12 weeks CG: usual drug therapy (pain killers | 40 | 3.33 | 60 | Pain (VAS) | NR | No/No |
| Shang [53], RCT | Changchun, China (Chinese) | 60 (30/30) | 0% | People with lumbar disc herniation | Age range from 18 to 60 | BJ: 5 × 60 min/week for 3 months + usual care CG: usual care | 60 | 5 | 60 | Pain (VAS and JOABPEQ) | NR | No/No |
| Xuan et al. [54], RCT | Shanghai, China, (Chinese) | 80 (40/40) | 0% | People with cervical spondylotic radiculopathy suffered from chronic neck pain | A mean age of 31.07 | BJ: daily 40 min for 20 days + manual therapy (as same below) CG: manual therapy | 13 | 4.67 | 20 | Pain (SF-MPQ) | NR | No/No |
| Peng et al. [55], RCT | Guangzhou, China (Chinese) | 100 (50/50) | 9% | Older people with low back pain who suffered from osteoporosis | a mean age of 69.06 | BJ: daily 30 min for 14 days + usual care CG: usual care | 7 | 3.5 | 14 | Pain (VAS) | NR | No/No |
| An et al. [56], RCT | Shanghai, China, (English) | 28 (14/14) | 25% | Female patients with knee osteoarthritis who suffered from bodily pain | a mean age of 65.0 | BJ: 5 × 30 min/week for 8 weeks CG: no intervention | 20 | 2.5 | 40 | Pain (subscale of WOMAC) | NR | NR/No |
| Wang et al. [57] NRCT | Qingdao, China, (English) | 72 (36/36) | 4.2% | Patients with chronic neck pain | Age range 45 to 75 | BJ: 7 × 30 min/week for 6 months + educational lessons CG: educational lessons | 84 | 3.5 | 168 | Pain (VAS) | NR | NR/No |
| Xiao et al. [58], RCT | Beijing, China (English) | 96 (48/48) | 7.3% | Patients with Parkinson’s disease | Age range from 55 to 80 | BJ: 4 × 45 min/week for 6 months + daily walking for 30 min CG: daily walking for 30 min | 72 | 3 | 96 | Sleep quality (PDSS-2) | NR | No/No |
| Chan et al. [59], RCT | Hong Kong, China (English) | 150 (75/75) | 13.3% | People with chronic fatigue syndrome-like illness | A mean age of 39.1 | BJ: 90 mn per session over 9 consecutive weeks, for 16 sessions CG: waitlist | 24 | 2.6 | 16 | Sleep quality (PSQI) | NR | No/3-month |
| Wang et al. [60], RCT | Beijing, China (Chinese) | 90 (30/30/30) | 13.3% | Patients with type 2 Diabetic mellitus accompanied by insomnia | a mean age of 57.8 | BJ: training dosage was NR for 4 months + usual care CG1: LiuZijue (Training dosage was NR) for 4 months + usual care CG2: usual care | NA | NA | NA | Sleep quality (PSQI) | NR | No/No |
| Xiong et al. [61], RCT | Changchun, China, (Chinese) | 60 (20/20/20) | 0% | Middle-aged adults with insomnia | A mean age of 48.7 | BJ1: 5 × 40 min/week for 4 weeks BJ2: Baduanjin (same dosage as above) + acupuncture CG: acupuncture | 13.3 | 3.3 | 20 | Sleep quality (PSQI) | NR | No/No |
| Chen et al. [62], NRCT | Fuzhou, China, (Chinese) | 60 (30/30) | 0% | Older people with hypertension accompanied by insomnia | Age range from 60 to 75 | BJ: 3 × 60 min/week for 3 months + educational lessons CG: educational lessons | 36 | 3 | 36 | Sleep quality (PSQI) | NR | No/No |
| Li et al. [63], RCT | Jiangsu, China, (Chinese) | 40 (20/20) | 0% | Patients with type 2 Diabetic mellitus accompanied by insomnia (mean age of 53.6) | A mean age of 53.6 | BJ: 7 × 30 min/week for 4 weeks + educational lessons CG: educational lessons | 14 | 5.17 | 28 | Sleep quality (PSQI) | NR | No/No |
| Xiong et al. [64], RCT | Changchun, China (Chinese) | 60 (30/30) | 0% | People with insomnia | Age range from 18 to 75 | BJ1: 5 × 40 min/week for 4 weeks BJ2: Baduanjin (same dosage as above) + acupuncture CG: acupuncture | 13.3 | 3.3 | 20 | Sleep quality (PSQI) | NR | No/No |
| Pretest-posttest study without control group | ||||||||||||
| Author Reference | Study location (Language) | Initial sample size | Drop-Out % | Study characteristic | Intervention protocol | Study findings | ||||||
| Health status | Age range or mean age | Training Duration and Dosage | Total Hours | Hours Weekly | Total Session | Outcome Measured | Study results | |||||
| An et al. [65], PPS | Shanghai, China, (English) | 28 | 21.4% | Patients with knee osteoarthritis | A mean age of 65.2 | BJ: 5 × 30 min/week for 1 year | 120 | 2.5 | 336 | Pain (subscale of WOMAC) | BJ significantly reduced the level of pain (132.0 ± 69.6 vs. 56.2 ± 67.6, p = 0.000) | |
| Author (Reference) | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Du et al. [37] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Wang et al. [38] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| Cai et al. [39] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Li et al. [40] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Xu et al. [41] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 5/10 |
| Chen et al. [42] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Wei et al. [44] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Wan et al. [45] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Wang et al. [46] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| Fu et al. [47] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Li et al. [48] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Liu et al. [49] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Wang & Liu [50] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Xiao et al. [51] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Ding et al. [52] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 7/10 |
| Shang [53] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Xuan et al. [54] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Peng et al. [55] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 5/10 |
| An et al. [56] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 5/10 |
| Wang et al. [57] | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 4/10 |
| Xiao et al. [58] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Chan et al. [59] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8/10 |
| Wang et al. [60] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Xiong et al. [61] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Chen et al. [62] | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 5/10 |
| Li et al. [63] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 5/10 |
| Xiong et al. [64] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 6/10 |
| Categorical Moderator | Outcome | Level | No. of Studies/Comparisons | SMD | 95% Confidence Interval | I2, % | Test for between-Group Homogeneity | ||
| Q-Value | df(Q) | p-Value | |||||||
| Intervention Length | Pain | <12 weeks | 4 | −0.85 | −1.24 to −0.46 | 0% | 0.19 | 1 | 0.66 |
| ≥12 weeks | 9 | −0.95 | −1.17 to −0.74 | 39.03% | |||||
| Final sample size | pain | <60 | 6 | −0.92 | −1.22 to −0.61 | 0% | 0.07 | 1 | 0.79 |
| ≥60 | 11 | −0.87 | −1.04 to −0.70 | 30.78% | |||||
| Weekly training hours | Pain | <5 h per week | 7 | −0.95 | −1.18 to −0.71 | 18.7% | 0.49 | 1 | 0.49 |
| ≥5 h per week | 10 | −0.84 | −1.03 to −0.65 | 9.41% | |||||
| Session length | Pain | Less than 45 min | 7 | −0.95 | −1.18 to −0.71 | 18.7% | 0.49 | 1 | 0.49 |
| 45 min or longer | 10 | −0.84 | −1.03 to −0.65 | 9.41% | |||||
| Control type | Pain | Active | 11 | −0.91 | −1.09 to −0.72 | 12.78% | 0.21 | 1 | 0.65 |
| passive | 6 | −0.83 | −1.08 to −0.59 | 18.63% | |||||
| Continuous moderator | Level | No. of Studies/Comparisons | 95% Confidence Interval | Q-Value | df(Q) | p-Value | |||
| Total training hours | Pain | 17 | −0.00111 | −0.0017 to 0.0039 | 0.6 | 1 | 0.44 | ||
| Number of total sessions | Pain | 17 | −0.00108 | −0.00136 to 0.00352 | 0.75 | 1 | 0.39 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Yeung, A.; Quan, X.; Boyden, S.D.; Wang, H. A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020206
Zou L, Yeung A, Quan X, Boyden SD, Wang H. A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. International Journal of Environmental Research and Public Health. 2018; 15(2):206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020206
Chicago/Turabian StyleZou, Liye, Albert Yeung, Xinfeng Quan, Sean David Boyden, and Huiru Wang. 2018. "A Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases" International Journal of Environmental Research and Public Health 15, no. 2: 206. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15020206