Assessment of Whole Body and Local Muscle Fatigue Using Electromyography and a Perceived Exertion Scale for Squat Lifting


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Muscle Selection and Location of Electrodes
2.3. Apparatus
2.4. Pre-Processing of EMG Signal
2.5. Principal Component Analysis
3. Experiment Design
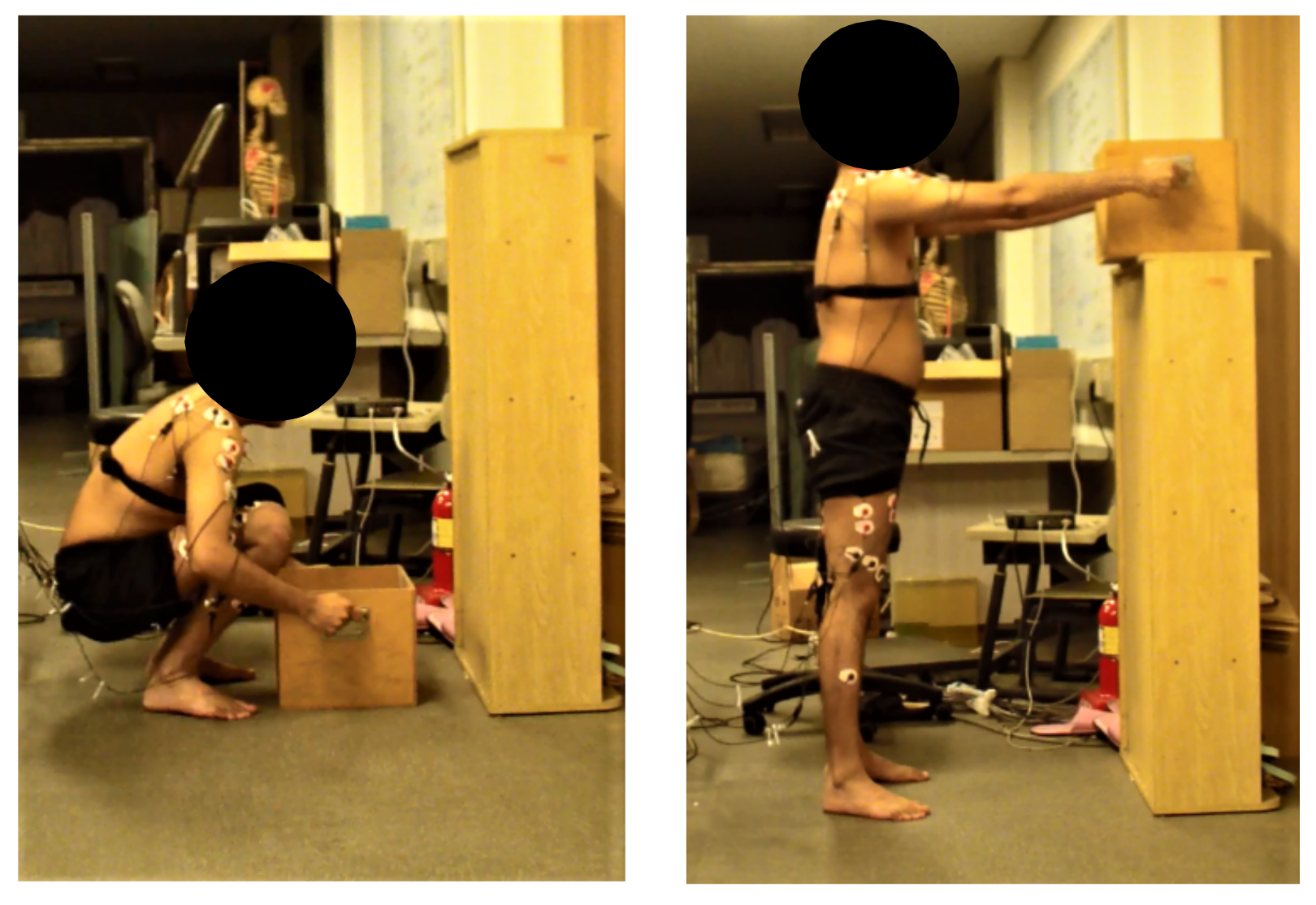
3.1. Procedure
3.2. Data Analysis
3.3. Statistical Analysis
4. Results
5. Discussion
5.1. Perceived Exertions
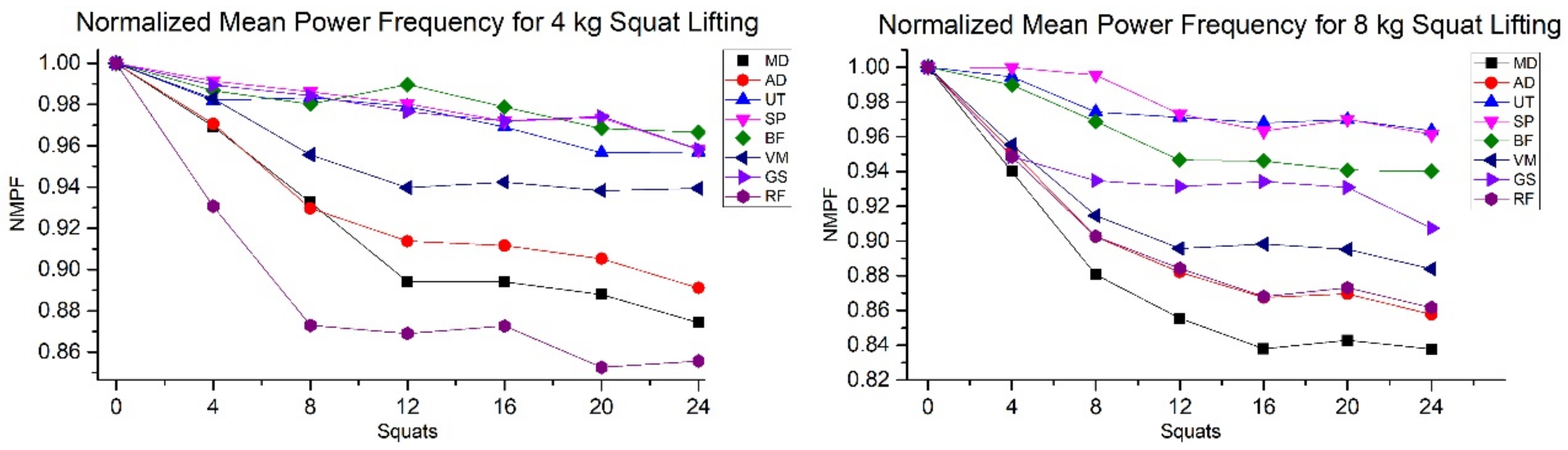
5.2. Mean Power Frequency and Heart Rate
5.3. Principal Component Analysis
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shin, H.J.; Kim, J.Y. Measurement of trunk muscle fatigue during dynamic lifting and lowering as recovery time changes. Int. J. Ind. Ergon. 2007, 37, 545–551. [Google Scholar] [CrossRef]
- Enoka, R.M.; Duchateau, J. Muscle fatigue: What, why and how it influences muscle function. J. Physiol. 2008, 586, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Vahdat, I.; Rostami, M.; Ghomsheh, F.T.; Khorramymehr, S.; Tanbakoosaz, A. The effects of task execution variables on the musculature activation strategy of the lower trunk during squat lifting. Int. J. Ind. Ergon. 2016, 55, 77–85. [Google Scholar] [CrossRef]
- Smale, K.B.; Shourijeh, M.S.; Benoit, D.L. Use of muscle synergies and wavelet transforms to identify fatigue during squatting. J. Electromyogr. Kinesiol. 2016, 28, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Rashedi, E.; Nussbaum, M.A. Cycle time influences the development of muscle fatigue at low to moderate levels of intermittent muscle contraction. J. Electromyogr. Kinesiol. 2016, 28, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Marras, W.S.; Davis, K.G. Variation in spinal load and trunk dynamics during repeated lifting exertions. Clin. Biomech. 1999, 14, 367–375. [Google Scholar] [CrossRef]
- Grant, S.; Aitchison, T.; Henderson, E.; Christie, J.; Zare, S.; Mc Murray, J.; Dargie, H. A Comparison of the Reproducibility and the Sensitivity to Change of Visual Analogue Scales, Borg Scales, and Likert Scales in Normal Subjects during Submaximal Exercise. Chest 1999, 116, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, M.D.; Sundstrup, E.; Persson, R.; Andersen, C.H.; Andersen, L.L. Is Borg’s perceived exertion scale a useful indicator of muscular and cardiovascular load in blue-collar workers with lifting tasks? A cross-sectional workplace study. Eur. J. Appl. Physiol. 2014, 114, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.L.; Clausen, T.; Persson, R.; Holtermann, A. Dose—Response relation between perceived physical exertion during healthcare work and risk of long-term sickness absence. Scand. J. Work Environ. Health 2012, 38, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Ditchen, D.M.; Ellegast, R.P.; Gawliczek, T.; Hartmann, B.; Rieger, M.A. Occupational kneeling and squatting: Development and validation of an assessment method combining measurements and diaries. Int. Arch. Occup. Environ. Health 2015, 88, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Au, J.S.; De Zepetnek, J.O.T.; Macdonald, M.J. Modeling Perceived Exertion during Graded Arm Cycling Exercise in Spinal Cord Injury. Med. Sci. Sports Exerc. 2017, 49, 1190–1196. [Google Scholar] [CrossRef] [PubMed]
- Smirmaul Bde, P. Sense of effort and other unpleasant sensations during exercise: Clarifying concepts and mechanisms. Br. J. Sports Med. 2012, 46, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Ugalde, I.; Figueroa, N.; El Saddik, A. Towards whole body fatigue assessment of human movement: A fatigue-tracking system based on combined semg and accelerometer signals. Sensors 2014, 14, 2052–2070. [Google Scholar] [CrossRef] [PubMed]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Physical Performance and Perceived Exertion; Gleerup: Lund, Sweden, 1962. [Google Scholar]
- Shair, E.; Ahmad, S.A.; Marhaban, M.H.; Mohd Tamrin, S.B.; Abdullah, A.R. EMG Processing Based Measures of Fatigue Assessment during Manual Lifting. BioMed Res. Int. 2017, 2017, 3937254. [Google Scholar] [CrossRef] [PubMed]
- Ghofrani, M.; Olyaei, G.; Talebian, S.; Bagheri, H.; Kazemi, P. Reliability of SEMG measurements for trunk muscles during lifting variable loads in healthy subjects. J. Bodyw. Mov. Ther. 2017, 21, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Özgünen, K.T.; Çelik, U.; Kurdak, S.S. Determination of an optimal threshold value for muscle activity detection in EMG analysis. J. Sports Sci. Med. 2010, 9, 620. [Google Scholar] [PubMed]
- Marras, W.S.; Granata, K.P. The development of an EMG-assisted model to assess spine loading during whole-body free-dynamic lifting. J. Electromyogr. Kinesiol. 1997, 7, 259–268. [Google Scholar] [CrossRef]
- Haddad, O.; Mirka, G.A. Trunk muscle fatigue and its implications in EMG-assisted biomechanical modeling. Int. J. Ind. Ergon. 2013, 43, 425–429. [Google Scholar] [CrossRef]
- Al-Mulla, M.R.; Sepulveda, F.; Colley, M. A review of non-invasive techniques to detect and predict localised muscle fatigue. Sensors 2011, 11, 3545–3594. [Google Scholar] [CrossRef] [PubMed]
- Al-Shair, K.; Kolsum, U.; Singh, D.; Vestbo, J. The Effect of Fatigue and Fatigue Intensity on Exercise Tolerance in Moderate COPD. Lung 2016, 194, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Farina, D. Surface Electromyography: Physiology, Engineering and Applications; John Wiley & Sons: Trenton, NJ, USA, 2016. [Google Scholar]
- Phinyomark, A.; Thongpanja, S.; Hu, H.; Phukpattaranont, P.; Limsakul, C. The usefulness of mean and median frequencies in electromyography analysis. In Computational Intelligence in Electromyography Analysis—A Perspective on Current Applications and Future Challenges; InTech: London, UK, 2012. [Google Scholar]
- Jesus, I.R.; Mello, R.G.; Nadal, J. Muscle Fatigue Assessment during Cycle Ergometer Exercise Using Principal Component Analysis of Electromyogram Power Spectra. J. Appl. Biomech. 2016, 32, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Naik, G.R.; Selvan, S.E.; Gobbo, M.; Acharyya, A.; Nguyen, H.T. Principal component analysis applied to surface electromyography: A comprehensive review. IEEE Access 2016, 4, 4025–4037. [Google Scholar] [CrossRef]
- Jolliffe, I.T. Principal component analysis and factor analysis. In Principal Component Analysis; Springer: New York, NY, USA, 2002; pp. 150–166. [Google Scholar]
- Jolliffe, I.T. Discarding Variables in a Principal Component Analysis. I: Artificial Data. Appl. Stat. 1972, 21, 160–173. [Google Scholar] [CrossRef]
- Dhindsa, I.; Agarwal, R.; Ryait, H. Principal component analysis-based muscle identification for myoelectric-controlled exoskeleton knee. J. Appl. Stat. 2017, 44, 1707–1720. [Google Scholar] [CrossRef]
- Muniz, A.M.; Nadal, J. Application of principal component analysis in vertical ground reaction force to discriminate normal and abnormal gait. Gait Posture 2009, 29, 31–35. [Google Scholar] [CrossRef] [PubMed]
- SENIAM. SENIAM. 2017. Available online: http://www.seniam.org/ (assecced on 4 March 2018).
- Ribeiro, D.C.; de Castro, M.P.; Sole, G.; Vicenzino, B. The initial effects of a sustained glenohumeral postero-lateral glide during elevation on shoulder muscle activity: A repeated measures study on asymptomatic shoulders. Man. Ther. 2016, 22 (Suppl. C), 101–108. [Google Scholar] [CrossRef] [PubMed]
- Plews, D.J.; Scott, B.; Altini, M.; Wood, M.; Kilding, A.E.; Laursen, P.B. Comparison of Heart Rate Variability Recording with Smart Phone Photoplethysmographic, Polar H7 Chest Strap and Electrocardiogram Methods. Int. J. Sports Physiol. Perform. 2017, 12, 1324–1328. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.H.; Hargrove, L.J.; Lock, B.A.; Kuiken, T.A. Determining the optimal window length for pattern recognition-based myoelectric control: Balancing the competing effects of classification error and controller delay. IEEE Trans. Neural Syst. Rehabil. Eng. 2011, 19, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Marras, W.S.; Lavender, S.A.; Leurgans, S.E.; Fathallah, F.A.; Ferguson, S.A.; Allread, W.G.; Rajulu, S.L. Biomechanical risk factors for occupationally related low back disorders. Ergonomics 1995, 38, 377–410. [Google Scholar] [CrossRef] [PubMed]
- Souissi, H.; Chtourou, H.; Chaouachi, A.; Chamari, K.; Souissi, N.; Amri, M. Time-of-day effects on EMG parameters during the Wingate test in boys. J. Sports Sci. Med. 2012, 11, 380. [Google Scholar] [PubMed]
- Serafim, T.H.; Tognato, A.C.; Nakamura, P.M.; Queiroga, M.R.; Pereira, G.; Nakamura, F.Y.; Kokubun, E. Development of the color scale of perceived exertion: Preliminary validation. Percept. Mot. Skills 2014, 119, 884–900. [Google Scholar] [CrossRef] [PubMed]
- Villafañe, J.H.; Gobbo, M.; Peranzoni, M.; Naik, G.; Imperio, G.; Cleland, J.A.; Negrini, S. Validity and everyday clinical applicability of lumbar muscle fatigue assessment methods in patients with chronic non-specific low back pain: A systematic review. Disabil. Rehabil. 2016, 38, 1859–1871. [Google Scholar] [CrossRef] [PubMed]
- Egan, A.D. Session rating of perceived exertion during high intensity and low intensity bouts of resistance exercise. UW-L J. Undergrad Res. 2003, 6, 1–6. [Google Scholar]
- Kulkarni, S.; Swaminathan, R. Analysis of surface EMG signals during dynamic contraction using Lempel-Ziv complexity. In Proceedings of the 2015 41st Annual Northeast Biomedical Engineering Conference (NEBEC), Troy, NY, USA, 17–19 April 2015. [Google Scholar]
- Hummel, A.; Läubli, T.; Pozzo, M.; Schenk, P.; Spillmann, S.; Klipstein, A. Relationship between perceived exertion and mean power frequency of the EMG signal from the upper trapezius muscle during isometric shoulder elevation. Eur. J. Appl. Physiol. 2005, 95, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Charoenpanicha, N.; Boonsinsukhb, R.; Sirisupc, S.; Saengsirisuwana, V. Principal component analysis identifies major muscles recruited during elite vertical jump. ScienceAsia 2013, 39, 257–264. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Regions for RPE | Number of Squats | ||||||
|---|---|---|---|---|---|---|---|
| 4 | 8 | 12 | 16 | 20 | 24 | ||
| Weights | |||||||
| 4 kg vs. 8 kg | 4 kg vs. 8 kg | 4 kg vs. 8 kg | 4 kg vs. 8 kg | 4 kg vs. 8 kg | 4 kg vs. 8 kg | ||
| Lower | F | 11.73 | 47.71 | 54.76 | 22.65 | 33.82 | 3.85 |
| p | 0.001 | * | * | * | * | 0.055 | |
| Upper | F | 21.87 | 56.82 | 40.76 | 36.96 | 47.32 | 87.48 |
| p | * | * | * | * | * | * | |
| Whole body | F | 3.27 | 0.05 | 18.78 | 13.36 | 8.73 | 0.96 |
| p | 0.077 | 0.821 | * | 0.001 | 0.05 | 0.332 | |
| Extremity | Muscle | NMPF Slope | |
|---|---|---|---|
| 4 kg | 8 kg | ||
| Upper | MD * | −0.44 | −0.45 |
| AD | −0.34 | −0.41 | |
| UT | −0.15 | −0.12 | |
| SP | −0.15 | −0.19 | |
| Lower | BF | −0.11 | 0.23 |
| VS | −0.19 | −0.29 | |
| GS | −0.14 | −0.15 | |
| RF * | −0.31 | −0.30 | |
| Whole body | HR | Heart Rate slope | |
| 0.7698 | 0.62 | ||
| Extremity | Muscle Type | Pearson’s r | |
|---|---|---|---|
| 4 kg | 8 kg | ||
| Upper | MD | −0.89 | −0.84 |
| AD | −0.87 | −0.88 | |
| UT | −0.95 | −0.83 | |
| SP | −0.96 * | −0.87 | |
| Lower | BF | −0.84 | 0.87 * |
| VS | −0.95 | 0.79 | |
| GS | −0.90 | −0.83 | |
| RF | −0.78 | −0.82 | |
| Whole body | HR | 0.96 | 0.95 |
| Outcome | Implications | |
|---|---|---|
| 1 | If the perceived whole body fatigue is higher than upper and lower extremity | Whole body fatigue dominates the peripheral fatigue in squat lifting |
| 2 | If upper extremity perceived fatigue is higher than the wholebody and lower extrimty perceived fatigue | Upper body perceived exertion dominates the whole body and lower extremity perceived fatigue in squat lifting |
| 3 | If lower body perceived fatigue is higher than the whole body and upper body perceived exertion | Lower body perceived exertion dominates the whole body the and upper body perceived exertion in squat lifting |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, I.; Kim, J.-Y. Assessment of Whole Body and Local Muscle Fatigue Using Electromyography and a Perceived Exertion Scale for Squat Lifting. Int. J. Environ. Res. Public Health 2018, 15, 784. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040784
Ahmad I, Kim J-Y. Assessment of Whole Body and Local Muscle Fatigue Using Electromyography and a Perceived Exertion Scale for Squat Lifting. International Journal of Environmental Research and Public Health. 2018; 15(4):784. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040784
Chicago/Turabian StyleAhmad, Imran, and Jung-Yong Kim. 2018. "Assessment of Whole Body and Local Muscle Fatigue Using Electromyography and a Perceived Exertion Scale for Squat Lifting" International Journal of Environmental Research and Public Health 15, no. 4: 784. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040784