Heterogeneity in the Relationship between Disinfection By-Products in Drinking Water and Cancer: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
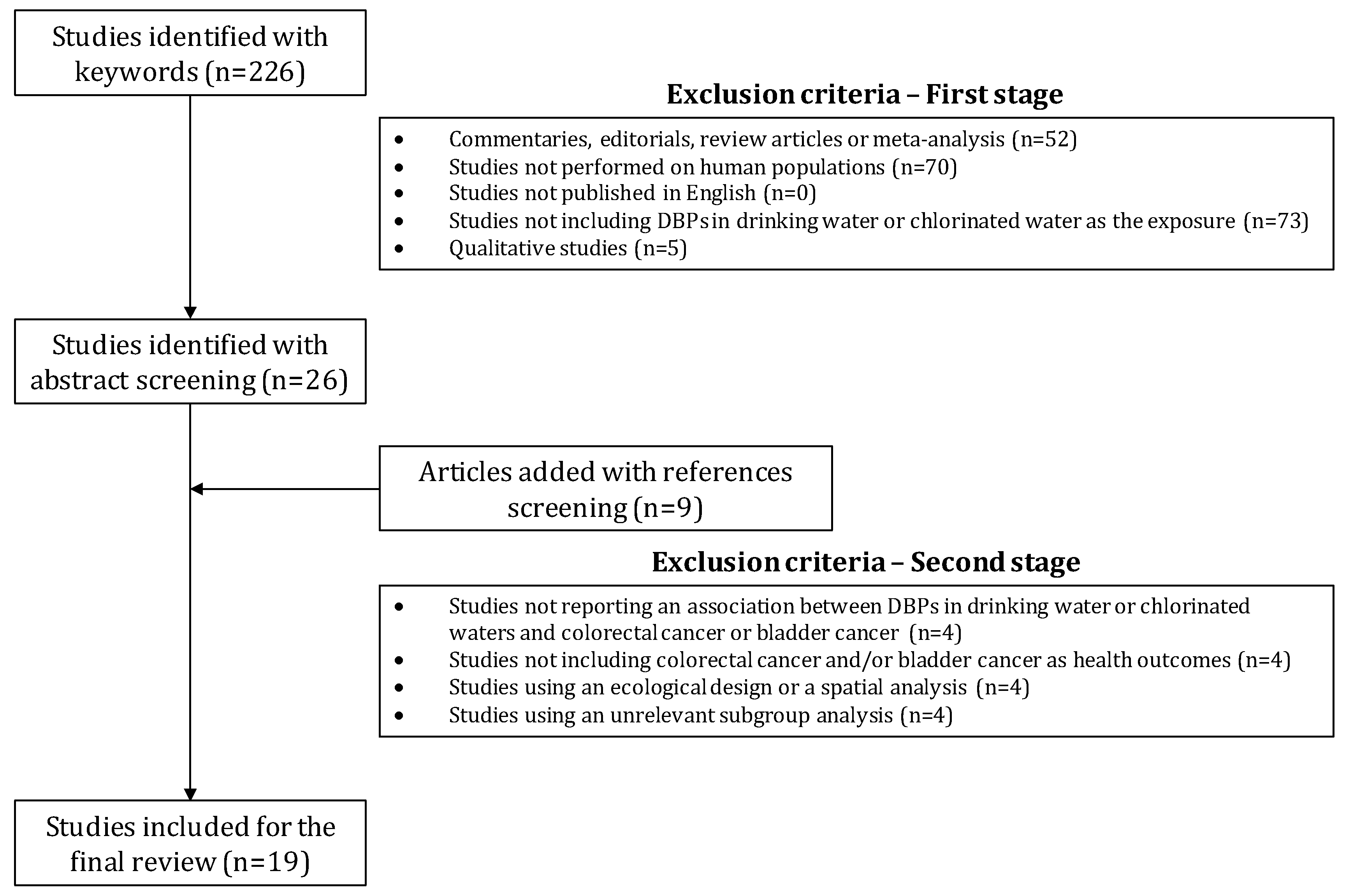
2.1. Search Strategy
2.2. Selection of Studies
- Commentaries, editorials, review articles, or meta-analysis
- Studies not performed on human populations
- Studies not published in English
- Studies not including DBPs in drinking water or chlorinated water as the exposure
- Qualitative studies
- Studies not reporting a quantitative estimate between DBPs in drinking water or chlorinated waters and colorectal cancer or bladder cancer
- Studies not including colorectal cancer and/or bladder cancer as health outcomes
- Studies using an ecological design or only a spatial analysis
2.3. Data Extraction
3. Results
3.1. Description of Studies Selected
3.2. Covariables Collected
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Rook, J.J. Formation of haloforms during chlorination of natural waters. J. Water Treat. Exam 1974, 23, 234–243. [Google Scholar]
- Richardson, S.D.; Plewa, M.J.; Wagner, E.D.; Schoeny, R.; DeMarini, D.M. Occurrence, genotoxicity, and carcinogenicity of regulated and emerging disinfection by-products in drinking water: A review and roadmap for research. Mutat. Res. 2007, 636, 178–242. [Google Scholar] [CrossRef] [PubMed]
- Grellier, J.; Bennett, J.; Patelarou, E.; Smith, R.B.; Toledano, M.B.; Rushton, L.; Briggs, D.J.; Nieuwenhuijsen, M.J. Exposure to Disinfection By-Products, Fetal Growth, and Prematurity: A Systematic Review and Meta-analysis. Epidemiology 2010, 21, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Levallois, P.; Gingras, S.; Marcoux, S.; Legay, C.; Catto, C.; Rodriguez, M.; Tardif, R. Maternal exposure to drinking-water chlorination by-products and small-for-gestational-age neonates. Epidemiology 2012, 23, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Toledano, M.B.; Nieuwenhuijsen, M.J.; Best, N.; Whitaker, H.; Hambly, P.; de Hoogh, C.; Fawell, J.; Jarup, L.; Elliott, P. Relation of trihalomethane concentrations in public water supplies to stillbirth and birth weight in three water regions in England. Environ. Health Perspect. 2005, 113, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.B.; Driscoll, T.; Cowie, C.; Armstrong, B.K. Disinfection by-products in drinking water and colorectal cancer: A meta-analysis. Int. J. Epidemiol. 2010, 39, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.M.; Fernandez, F.; Malats, N.; Grimalt, J.O.; Kogevinas, M. Meta-analysis of studies on individual consumption of chlorinated drinking water and bladder cancer. J. Epidemiol. Community Health 2003, 57, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.M.; Cordier, S.; Font-Ribera, L.; Salas, L.A.; Levallois, P. Overview of disinfection by-products and associated health effects. Curr. Environ. Health Rep. 2015, 2, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Hrudey, S.E.; Fawell, J. 40 years on: What do we know about drinking water disinfection by-products (DBPs) and human health? Water Sci. Technol. Water Supply 2015, 15, 667. [Google Scholar] [CrossRef]
- Parbery, G.; Tivey, D.; McArthur, A. Epidemiological association between chlorinated water and overall risk of cancer: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2012, 10, 1–14. [Google Scholar] [CrossRef]
- Chyou, P.-H.; Nomura, A.M.; Stemmermann, G.N. A prospective study of colon and rectal cancer among Hawaii Japanese men. Ann. Epidemiol. 1996, 6, 276–282. [Google Scholar] [CrossRef]
- Engel, L.S.; Taioli, E.; Pfeiffer, R.; Garcia-Closas, M.; Marcus, P.M.; Lan, Q.; Boffetta, P.; Vineis, P.; Autrup, H.; Bell, D.A. Pooled analysis and meta-analysis of glutathione S-transferase M1 and bladder cancer: A HuGE review. Am. J. Epidemiol. 2002, 156, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Haggar, F.A.; Boushey, R.P. Colorectal cancer epidemiology: Incidence, mortality, survival, and risk factors. Clin. Colon Rectal Surg. 2009, 22, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Heineman, E.F.; Zahm, S.H.; McLaughlin, J.K.; Vaught, J.B. Increased risk of colorectal cancer among smokers: Results of a 26-year follow-up of us veterans and a review. Int. J. Cancer 1994, 59, 728–738. [Google Scholar] [CrossRef] [PubMed]
- Kälble, T. Etiopathology, risk factors, environmental influences and epidemiology of bladder cancer. Der Urol. Ausg. A 2001, 40, 447–450. [Google Scholar] [CrossRef]
- Freudebhiem, J.; Graham, S.; Marshall, J.R.; Haughey, B.P.; Wilkinson, G. A case-control study of diet and rectal cancer in western New York. Am. J. Epidemiol. 1990, 131, 612–624. [Google Scholar] [CrossRef]
- Kiemeney, L.A.; Schoenberg, M. Familial transitional cell carcinoma. J. Urol. 1996, 156, 867–872. [Google Scholar] [CrossRef]
- Ross, R.K.; Jones, P.A.; Yu, M.C. Bladder cancer epidemiology and pathogenesis. Semin. Oncol. 1996, 23, 536–545. [Google Scholar] [PubMed]
- Slattery, M.L.; Sweeney, C.; Murtaugh, M.; Ma, K.N.; Caan, B.J.; Potter, J.D.; Wolff, R. Associations between vitamin D, vitamin D receptor gene and the androgen receptor gene with colon and rectal cancer. Int. J. Cancer 2006, 118, 3140–3146. [Google Scholar] [CrossRef] [PubMed]
- Vena, J.E.; Graham, S.; Freudenheim, J.; Marshall, J.; Zielezny, M.; Swanson, M.; Sufrin, G. Drinking water, fluid intake, and bladder cancer in western New York. Arch. Environ. Health Int. J. 1993, 48, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Woolcott, C.; King, W.; Marrett, L. Coffee and tea consumption and cancers of the bladder, colon and rectum. Eur. J. Cancer Prev. 2002, 11, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Sharp, L.; Donnelly, D.; Hegarty, A.; Carsin, A.-E.; Deady, S.; McCluskey, N.; Gavin, A.; Comber, H. Risk of several cancers is higher in urban areas after adjusting for socioeconomic status. Results from a two-country population-based study of 18 common cancers. J. Urban Health 2014, 91, 510–525. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, C.M.; Cantor, K.P.; Cordier, S.; Jaakkola, J.J.K.; King, W.D.; Lynch, C.F.; Porru, S.; Kogevinas, M. Disinfection byproducts and bladder cancer: A pooled analysis. Epidemiology 2004, 15, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Hanna-Attisha, M.; LaChance, J.; Sadler, R.C.; Champney Schnepp, A. Elevated blood lead levels in children associated with the Flint drinking water crisis: A spatial analysis of risk and public health response. Am. J. Public Health 2016, 106, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Brulle, R.J.; Pellow, D.N. Environmental justice: Human health and environmental inequalities. Annu. Rev. Public Health 2006, 27, 103–124. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.W.; Kantrowitz, E. Socioeconomic status and health: The potential role of environmental risk exposure. Ann. Rev. Public Health 2002, 23, 303–331. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.R.; Richardson, E.A.; Mitchell, R.J.; Shortt, N.K. Environmental justice and health: The implications of the socio-spatial distribution of multiple environmental deprivation for health inequalities in the United Kingdom. Trans. Inst. Br. Geogr. 2010, 35, 522–539. [Google Scholar] [CrossRef]
- O’Neill, M.S.; Jerrett, M.; Kawachi, I.; Levy, J.I.; Cohen, A.J.; Gouveia, N.; Wilkinson, P.; Fletcher, T.; Cifuentes, L.; Schwartz, J. Health, wealth, and air pollution: Advancing theory and methods. Environ. Health Perspect. 2003, 111, 1861–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balazs, C.; Morello-Frosch, R.; Hubbard, A.; Ray, I. Social Disparities in Nitrate Contaminated Drinking Water in California’s San Joaquin Valley. Environ. Health Perspect. 2011, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Balazs, C.L.; Morello-Frosch, R.; Hubbard, A.E.; Ray, I. Environmental justice implications of arsenic contamination in California’s San Joaquin Valley: A cross-sectional, cluster-design examining exposure and compliance in community drinking water systems. Environ. Health 2012, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Balazs, C.L.; Ray, I. The drinking water disparities framework: On the origins and persistence of inequities in exposure. Am. J. Public Health 2014, 104, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Delpla, I.; Benmarhnia, T.; Lebel, A.; Levallois, P.; Rodriguez, M.J. Investigating social inequalities in exposure to drinking water contaminants in rural areas. Environ. Pollut. 2015, 207, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.M.; Wright, J.M.; Meyer, A.; Rivera-Núñez, Z. Spatial variation of disinfection by-product concentrations: Exposure assessment implications. Water Res. 2013, 47, 6130–6140. [Google Scholar] [CrossRef] [PubMed]
- Hales, S.; Black, W.; Skelly, C.; Salmond, C.; Weinstein, P. Social deprivation and the public health risks of community drinking water supplies in New Zealand. J. Epidemiol. Community Health 2003, 57, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Martinez, D.; Aguilera, I.; Ballester, F.; Basterrechea, M.; Esplugues, A.; Guxens, M.; Larrañaga, M.; Lertxundi, A.; Mendez, M.; et al. Socioeconomic status and exposure to multiple environmental pollutants during pregnancy: Evidence for environmental inequity? J. Epidemiol. Community Health 2012, 66, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Briggs, D.; Abellan, J.J.; Fecht, D. Environmental inequity in England: Small area associations between socio-economic status and environmental pollution. Soc. Sci. Med. 2008, 67, 1612–1629. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Community Health 2003, 57, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Barceló, M.A.; Saez, M.; Saurina, C. Spatial variability in mortality inequalities, socioeconomic deprivation, and air pollution in small areas of the Barcelona Metropolitan Region, Spain. Sci. Total Environ. 2009, 407, 5501–5523. [Google Scholar] [CrossRef] [PubMed]
- Hajat, A.; Hsia, C.; O’Neill, M.S. Socioeconomic Disparities and Air Pollution Exposure: A Global Review. Curr. Environ. Health Rep. 2015, 2, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Benmarhnia, T.; Rey, L.; Cartier, Y.; Clary, C.M.; Deguen, S.; Brousselle, A. Addressing equity in interventions to reduce air pollution in urban areas: A systematic review. Int. J. Public Health 2014, 59, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Zanobetti, A.; Dominici, F. Who is more affected by ozone pollution? A systematic review and meta-analysis. Am. J. Epidemiol. 2014, 180, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Boffetta, P. Human cancer from environmental pollutants: The epidemiological evidence. Mutat. Res. 2006, 608, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, N.; Fletcher, T. Time series analysis of air pollution and mortality: Effects by cause, age and socioeconomic status. J. Epidemiol. Community Health 2000, 54, 750–755. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.; Wright, J.; Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2004, 2, 1–13. [Google Scholar] [PubMed]
- Hajat, A.; Diez-Roux, A.V.; Adar, S.D.; Auchincloss, A.H.; Lovasi, G.S.; O’Neill, M.S.; Sheppard, L.; Kaufman, J.D. Air pollution and individual and neighborhood socioeconomic status: Evidence from the Multi-Ethnic Study of Atherosclerosis (MESA). Environ. Health Perspect. 2013, 121, 1325. [Google Scholar] [CrossRef] [PubMed]
- Bertin, M.; Chevrier, C.; Serrano, T.; Monfort, C.; Rouget, F.; Cordier, S.; Viel, J.-F. Association between prenatal exposure to traffic-related air pollution and preterm birth in the PELAGIE mother–child cohort, Brittany, France. Does the urban–rural context matter? Environ. Res. 2015, 142, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madrigano, J.; Jack, D.; Anderson, G.B.; Bell, M.L.; Kinney, P.L. Temperature, ozone, and mortality in urban and non-urban counties in the northeastern United States. Environ. Health 2015, 14, 3. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Krewski, D.; Pope, C.A., III; Chen, Y.; Gapstur, S.M.; Thun, M.J. Long-term ambient fine particulate matter air pollution and lung cancer in a large cohort of never-smokers. Am. J. Respir. Crit. Care Med. 2011, 184, 1374–1381. [Google Scholar] [CrossRef] [PubMed]
- Sobue, T. Association of indoor air pollution and lifestyle with lung cancer in Osaka, Japan. Int. J. Epidemiol. 1990, 19 (Suppl. 1), S62–S66. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, J.R.; Comstock, G.W. Source of drinking water at home and site-specific cancer incidence in Washington County, Maryland. Am. J. Epidemiol. 1981, 114, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Koivusalo, M.; Pukkala, E.; Vartiainen, T.; Jaakkola, J.J.; Hakulinen, T. Drinking water chlorination and cancer–a historical cohort study in Finland. Cancer Cause Control 1997, 8, 192–200. [Google Scholar] [CrossRef]
- McGeehin, M.A.; Reif, J.S.; Becher, J.C.; Mangione, E.J. Case-control study of bladder cancer and water disinfection methods in Colorado. Am. J. Epidemiol. 1993, 138, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.M.; Cantor, K.P.; Lee, N.L.; Chen, L.-S.; Lei, H.-H.; Ruhl, C.E.; Wang, S.S. Bladder cancer and drinking water: A population-based case-control study in Washington County, Maryland (United States). Cancer Cause Control 1997, 8, 738–744. [Google Scholar] [CrossRef]
- Zierler, S.; Feingold, L.; Danley, R.A.; Craun, G. Bladder cancer in Massachusetts related to chlorinated and chloraminated drinking water: A case-control study. Arch. Environ. Health Int. J. 1988, 43, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Koivusalo, M.; Hakulinen, T.; Vartiainen, T.; Pukkala, E.; Jaakkola, J.J.; Tuomist, J. Drinking water mutagenicity and urinary tract cancers: A population-based case-control study in Finland. Am. J. Epidemiol. 1998, 148, 704–712. [Google Scholar] [CrossRef] [PubMed]
- King, W.D.; Marrett, L.D.; Woolcott, C.G. Case-control study of colon and rectal cancers and chlorination by-products in treated water. Cancer Epidemiol. Biomark. Prev. 2000, 9, 813–818. [Google Scholar]
- Chevrier, C.; Junod, B.; Cordier, S. Does ozonation of drinking water reduce the risk of bladder cancer? Epidemiology 2004, 15, 605–614. [Google Scholar] [CrossRef] [PubMed]
- Bove, G.E.; Rogerson, P.A.; Vena, J.E. Case-control study of the effects of trihalomethanes on urinary bladder cancer risk. Arch. Environ. Occup. Health 2007, 62, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Ho, S.-C.; Wang, L.-Y.; Yang, C.-Y. Bladder cancer in Taiwan: Relationship to trihalomethane concentrations present in drinking-water supplies. J. Toxicol. Environ. Health Part A 2007, 70, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Kogevinas, M.; Cantor, K.P.; Villanueva, C.M.; Garcia-Closas, M.; Rothman, N.; Malats, N.; Real, F.X.; Serra, C.; Garcia-Closas, R. Total fluid and water consumption and the joint effect of exposure to disinfection by-products on risk of bladder cancer. Environ. Health Perspect. 2007, 1569–1572. [Google Scholar] [CrossRef] [PubMed]
- Cantor, K.P.; Villanueva, C.M.; Silverman, D.T.; Figueroa, J.D.; Real, F.X.; Garcia-Closas, M.; Malats, N.; Chanock, S.; Yeager, M.; Tardon, A. Polymorphisms in GSTT1, GSTZ1, and CYP2E1, disinfection by-products, and risk of bladder cancer in Spain. Environ. Health Perspect. 2010, 118, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Bove, G.E.; Rogerson, P.A.; Vena, J.E. Case control study of the geographic variability of exposure to disinfectant byproducts and risk for rectal cancer. Int. J. Health Geogr. 2007, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Cantor, K.P.; Lynch, C.F.; Hildesheim, M.; Dosemeci, M.; Lubin, J.; Alavanja, M.; Craun, G. Drinking Water Source and Chlorination Byproducts I. Risk of Bladder Cancer. Epidemiology 1998, 9, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.S.; Carr, J.K. Case-control cancer mortality study and chlorination of drinking water in Louisiana. Environ. Health Perspect. 1982, 46, 169. [Google Scholar] [CrossRef] [PubMed]
- Hildesheim, M.E.; Cantor, K.P.; Lynch, C.F.; Dosemeci, M.; Lubin, J.; Alavanja, M.; Craun, G. Drinking Water Source and Chlorination Byproducts II. Risk of Colon and Rectal Cancers. Epidemiology 1998, 9, 29–35. [Google Scholar] [CrossRef] [PubMed]
- King, W.D.; Marrett, L.D. Case-control study of bladder cancer and chlorination by-products in treated water (Ontario, Canada). Cancer Cause Control 1996, 7, 596–604. [Google Scholar] [CrossRef]
- Villanueva, C.M.; Cantor, K.P.; Grimalt, J.O.; Malats, N.; Silverman, D.; Tardon, A.; Garcia-Closas, R.; Serra, C.; Carrato, A.; Castaño-Vinyals, G.; et al. Bladder cancer and exposure to water disinfection by-products through ingestion, bathing, showering, and swimming in pools. Am. J. Epidemiol. 2007, 165, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.-W.; Tiao, M.-M.; Wu, T.-N.; Yang, C.-Y. Trihalomethanes in drinking water and the risk of death from colon cancer in Taiwan. J. Toxicol. Environ. Health Part A 2009, 72, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E. Gender-related differences in pharmacokinetics and their clinical significance. J. Clin. Pharmacol. Ther. 1999, 24, 339–346. [Google Scholar] [CrossRef]
- Meibohm, B.; Beierle, I.; Derendorf, H. How important are gender differences in pharmacokinetics? Clin. Pharmacokinet. 2002, 41, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.S.; MacLehose, R.F. Which of these things is not like the others? Cancer 2013, 119, 4216–4222. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Bland, J.M. Interaction revisited: The difference between two estimates. Br. Med. J. 2003, 326, 219. [Google Scholar] [CrossRef]
- Villanueva, C.M.; Gracia-Lavedan, E.; Bosetti, C.; Righi, E.; Molina, A.J.; Martín, V.; Boldo, E.; Aragonés, N.; Perez-Gomez, B.; Pollan, M.; et al. Colorectal cancer and long-term exposure to trihalomethanes in drinking water: A multicenter case–control study in Spain and Italy. Environ. Health Perspect. 2017, 125, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Askari, A.; Aziz, O.; Currie, A.; Athanasiou, T.; Faiz, O. Inequalities in Colorectal Cancer Risk and Educational Level in Developed Countries: A Systematic Review and Meta-Analysis of Observational Studies. Br. J. Surg. 2015, 2015, 187. [Google Scholar]
- Choi, K.M. Investigation of cancer mortality inequalities between rural and urban areas in South Korea. Aust. J. Rural Health 2016, 24, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.; Rachet, B.; Coleman, M. Origins of socio-economic inequalities in cancer survival: A review. Ann. Oncol. 2006, 17, 5–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studies | Location | Year of Publication | Sample Size | Study Design | Disinfection by-Products Measurement | Subgroups Included in the Analysis | Effect Size and CI |
|---|---|---|---|---|---|---|---|
| Wilkins and Comstock [51] | Maryland, USA | 1981 | 81 cases and 30,699 controls | Cohort | Exposure to chlorinated drinking water | Sex | All: RR = 2.2 (0.71–9.39); Men: RR = 1.80 (0.80–4.75); Women: RR = 1.60 (0.54–6.32) |
| Zierler et al. [55] | Massachusetts, USA | 1988 | 614 cases and 1074 controls | Case-control | Duration of exposure to chlorinated drinking water | n.d. | All: OR = 2.7 (1.7–4.3) |
| McGeehin et al. [53] | Colorado, USA | 1993 | 327 bladder cancer and 261 other-cancer controls | Case-control | Questionnaire & data for TTHM from site visit of water utilities | Smoking Status | Non–Smokers: OR = 2.9 (1.2–7.4); Smokers: OR = 2.1 (1.1–3.8) |
| King and Marrett [67] | Ontario, Canada | 1996 | 696 cases and 1545 controls | Case-control | Questionnaire about source of water. Water source and chlorination status were provided directly by treatment plant surveys. TTHMs modelling | n.d. | All: OR = 1.66 (1.11–2.51) |
| Freedman et al. [54] | Maryland, USA | 1997 | 294 cases and 2326 controls | Case-control | Exposure to chlorinated drinking water | Sex, smoking habits | All: OR = 1.4 (0.7–2.9); Men: OR = 2.2 (0.8–5.1); Women: OR = 0.6 (0.2–2.2) |
| Koivusalo et al. [52] | Finland | 1997 | 621 431 | Cohort | Questionnaires. Information on water-pipe connections, past drinking water quality, and treatment practices by waterworks was obtained from administrative registers and municipal waterworks. The level of mutagenicity was estimated by modelling | Sex | All: RR = 1.12 (0.93–1.36); Men: RR = 1.03 (0.82–1.28); Women: RR = 1.48 (1.01–2.18) |
| Cantor et al. [64] | Iowa, USA | 1998 | 1123 cases and 1983 controls | Case-control | TTHMs in tap water (measures + estimations) | Sex, smoking habits | All: OR = 1.3 (0.9–2.0); Men: OR = 1.8 (1.2–2.7); Women: OR = 0.6 (0.3–1.4) |
| Koivusalo et al. [56] | Finland | 1998 | 732 cases and 914 controls | Case-control | Questionnaires. Information on water-pipe connections, past drinking water quality, and treatment practices by waterworks was obtained from administrative registers and municipal waterworks. The level of mutagenicity was estimated by modelling | Sex | Men: OR = 1.17 (0.87–1.57); Women: OR = 1.14 (0.71–1.82) |
| Chevrier et al. [58] | France | 2004 | 281 cases and 272 controls | Case-control | TTHMs modelling | Sex | All: OR = 2.99 (1.1–8.5); Men: OR = 3.73 (1.2–11); Women: OR = 1.55 (0.1–32) |
| Bove et al. [59] | New York, USA | 2007 | 182 cases and 385 controls | Case-control | TTHMs in tap water + water consumption | n.d. | THM: OR = 2.34 (1.01–3.66); CLF: OR = 2.55 (1.25–4.66); BRF: OR = 3.05 (1.51–5.69); BDCM: OR = 2.49 (1.19–4.48) |
| Chang et al. [60] | Taiwan | 2007 | 403 cases and 403 controls | Case-control | TTHMs in tap water | n.d. | All: OR = 2.11 (1.43–3.11) |
| Michaud et al. [61] | Spain | 2007 | 397 cases and 664 controls | Case-control | Questionnaire and records searches (including THM measurements) | n.d. | All: OR = 2.06 (0.83–5.08) |
| Villanueva et al. [68] | Spain | 2007 | 1219 cases and 1271 controls | Case-control | Questionnaire and records searches (including THM measurements) | Sex | All: OR = 2.10 (1.09, 4.02); Men: OR = 2.53 (1.23, 5.20); Women: OR = 1.50 (0.26, 8.61) |
| Cantor et al. [62] | Spain | 2010 | 680 cases and 714 controls | Case-control | TTHMs in tap water | Gene polymorphism | All: OR = 1.8 (0.9–3.5) |
| Studies | Location | Year of Publication | Sample Size | Study Design | Exposition Measurement | Site of Cancer | Subgroups Included in the Analysis | Effect Size and CI |
|---|---|---|---|---|---|---|---|---|
| Gottlieb and Carr [65] | Louisiana, USA | 1982 | 546 cases and 534 controls | Case-control | Exposure to chlorinated drinking water | Rectal | n.d. | All: OR = 1.68 (1.17–2.42) |
| Koivusalo et al. [52] | Finland | 1997 | 621 431 | Cohort | Questionnaires. Information on water-pipe connections, past drinking water quality, and treatment practices by waterworks was obtained from administrative registers and municipal waterworks. The level of mutagenicity was estimated by modelling | Colon and rectal | Sex | Colon: All: RR = 0.90 (0.77–1.04); Men: RR = 0.83 (0.66–1.04); Women: RR = 0.95 (0.78–1.85). Rectal: All: RR = 1.04 (0.86–1.26); Men: RR = 0.85 (0.66–1.09); Women: RR = 1.38 (1.03–1.85). |
| Hildesheim et al. [66] | Iowa, USA | 1998 | 560 colon cases, 537 rectal cases, and 1983 controls | Case-control | TTHMs in tap water | Colon and rectal | n.d. | Colon: OR = 1.06 (0.7–1.6); Rectal: OR = 1.66 (1.1–2.6) |
| King et al. [57] | Ontario, Canada | 2000 | 767 colon cases, 661 rectal cases, and 1545 controls | Case-control | Questionnaire about source of water. Water source and chlorination status were provided directly by treatment plant surveys. TTHMs modelling | Colon and rectal | Sex | Colon: OR = 1.87 (1.15–3.05) for Men; OR = 0.92 (0.49–1.71) for Women. Rectal: OR = 0.98 (0.56–1.72) for Men; OR = 0.72 (0.34–1.53) for Women |
| Bove et al. [63] | New York State, USA | 2007 | 128 cases and 253 controls | Case-control | TTHMs in tap water + water consumption | Rectal | n.d. | THM4: OR = 1.01 (0.98–1.03); CLF: OR = 1.00 (0.93–1.09); BRF: OR = 1.20 (1.05–1.35) |
| Kuo et al. [69] | Taiwan | 2009 | 2195 cases and 2195 controls | Case-control | Questionnaire & data on TTHM levels in drinking water in study. Municipalities were collected from the Taiwan Environmental Protection Administration | Colon | n.d. | All: OR = 1.04 (0.89–1.21) |
| Study | Age | Sex | Socio-Economic Factors * | Urbanization Level | Smoking | Other Health Behaviors |
|---|---|---|---|---|---|---|
| Wilkins and Comstock 1981 [51] | X | X | X | X | ||
| Gottlieb and Carr 1982 [65] | X | X | ||||
| Zierler et al. 1988 [55] | X | X | ||||
| McGeehin et al. 1993 [53] | X | |||||
| King and Marrett 1996 [67] | X | X | X | X | ||
| Freedman et al. 1997 [54] | X | X | X | |||
| Koivusalo et al. 1997 [52] | X | X | X | X | X | |
| Cantor et al. 1998 [64] | X | X | X | X | ||
| Hildesheim et al. 1998 [66] | X | X | ||||
| Koivusalo et al. 1998 [56] | X | X | X | X | X | |
| King et al. 2000 [57] | X | X | X | X | ||
| Chevrier et al. 2004 [58] | X | X | X | X | ||
| Bove et al. 2007 [63] | X | X | X | |||
| Bove et al. 2007 [59] | X | X | X | |||
| Chang et al. 2007 [60] | X | X | ||||
| Michaud et al. 2007 [61] | X | X | X | |||
| Villanueva et al. 2007 [68] | X | X | X | X | X | |
| Kuo et al. 2009 [69] | X | X | X | |||
| Cantor et al. 2010 [62] | X | X | X | X |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benmarhnia, T.; Delpla, I.; Schwarz, L.; Rodriguez, M.J.; Levallois, P. Heterogeneity in the Relationship between Disinfection By-Products in Drinking Water and Cancer: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050979
Benmarhnia T, Delpla I, Schwarz L, Rodriguez MJ, Levallois P. Heterogeneity in the Relationship between Disinfection By-Products in Drinking Water and Cancer: A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(5):979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050979
Chicago/Turabian StyleBenmarhnia, Tarik, Ianis Delpla, Lara Schwarz, Manuel J. Rodriguez, and Patrick Levallois. 2018. "Heterogeneity in the Relationship between Disinfection By-Products in Drinking Water and Cancer: A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 5: 979. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050979