Views and Experiences of Persons with Chronic Diseases about Strategies that Aim to Integrate and Re-Integrate Them into Work: A Systematic Review of Qualitative Studies

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy for the Complete PATHWAYS Review
2.2. Selection Criteria for the Complete PATHWAYS Review
- (a)
- had been published between January 2011 and April 2016;
- (b)
- were published in English;
- (c)
- were intervention studies, namely randomized trials, non-randomized controlled trials, non-controlled pre-post intervention studies; were observational studies, namely cohort studies, case-control studies, cross-sectional studies, descriptive longitudinal studies; or were qualitative studies or mixed-methods studies;
- (d)
- had been carried out in the 28 countries of the European Union; in Norway, Lichtenstein, Iceland or Switzerland; or in non-European countries with western lifestyle: Canada, United States of America, or Australia;
- (e)
- reported on effectiveness regarding at least one of the following work outcomes:
- -
- employment status (employed/unemployed);
- -
- return to work;
- -
- absenteeism (sick leave);
- -
- maintain a job;
- -
- obtain a job;
or investigated variables potentially affecting effectiveness (e.g., views and experiences of involved persons with a given strategy); - (f)
- focused on the working population aged 16 to 65 years; and
- (g)
- focused on one of the following health conditions:
- -
- PwCDs in general, i.e., specific conditions are not further specified in the studies or results for different conditions are reported together, and persons with disabilities in general (persons with disabilities were included because people who receive disability benefits usually have chronic diseases and experience significant levels of disability in daily life) [35];
- -
- mental disorders, musculoskeletal disorders, cancer, neurological, metabolic, respiratory and cardiovascular diseases; or
- -
- depression, back and neck pain, migraine, diabetes mellitus, chronic obstructive pulmonary disease and ischemic heart disease.
- (a)
- were published before 2011;
- (b)
- were published in other languages than English;
- (c)
- were case report/case series, psychometric studies, letters, comments, editorials, overviews without empirical primary or secondary data, reviews (systematic and non-systematic reviews, health technology assessments) and meta-analyses, protocols, studies reporting exclusively on design or baseline data;
- (d)
- had been carried out in other countries than those specified above;
- (e)
- considered neither effectiveness outcomes (for example, studies reporting only on costs resulting from the implementation of strategies) nor variables potentially affecting effectiveness;
- (f)
- included participants mostly aged <16 or >65 years;
- (g)
- included participants with mainly chronic diseases other than the ones defined above;
- (h)
- did not focus on a concrete strategy or group of strategies (for example, studies focusing on general factors that facilitate return to work after sick leave); or
- (i)
- had no abstract available.
2.3. Additional Selection Criteria for the Present Review
2.4. Eligibility Assessment
2.5. Data Extraction and Methodological Assessment
2.6. Data Synthesis
2.7. Assessment of Confidence of Findings
- (1)
- Methodological limitations of the primary studies providing data: The extent to which there are concerns about the design or conduct of these studies (for instance, concerns regarding the sampling strategy or the procedures for data collection).
- (2)
- Coherence: Degree to which data from the primary studies support the finding (for instance, if patterns have been identified in studies with similar populations and interventions) or the finding provides a good explanation for those data.
- (3)
- Adequacy of the data contributing to the finding in terms of richness (extent to which data provided by the studies are detailed enough to understand the phenomenon) and quantity of data (for example, if the amount of studies, settings or populations supporting the finding is considered enough).
- (4)
- Relevance of the primary studies to the review question: The extent to which the context of the studies providing data for a given funding addresses the main components of the research question (for instance, population, setting, intervention).
- High: It is highly likely that the review finding is a reasonable representation of the phenomenon of interest.
- Moderate: It is likely that the review finding is a reasonable representation of the phenomenon of interest.
- Low: It is possible that the review finding is a reasonable representation of the phenomenon of interest.
- Very low: It is not clear whether the review finding is a reasonable representation of the phenomenon of interest.
3. Results
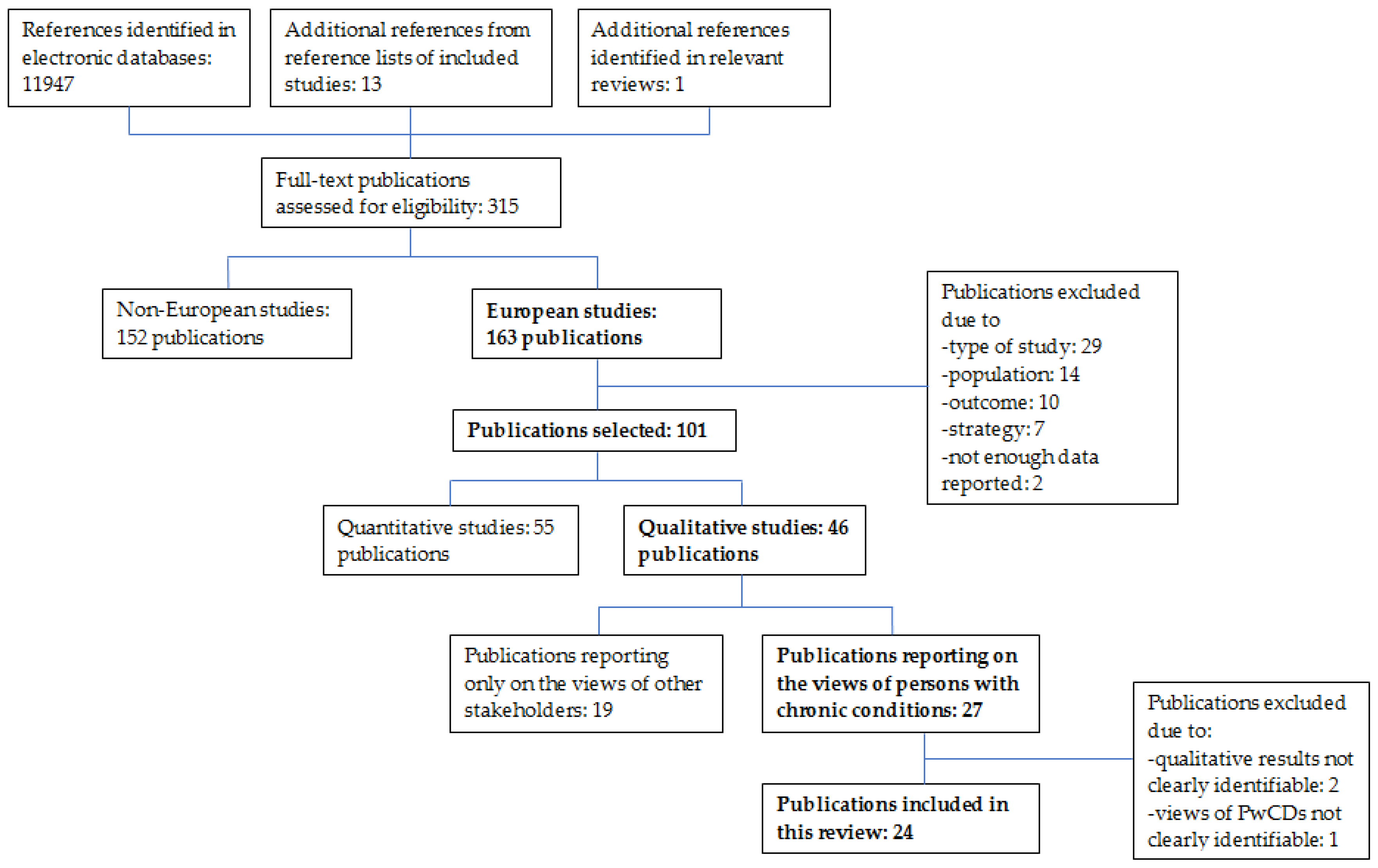
3.1. Results of the Searches
3.2. Main Characteristics of Included Studies
3.3. Themes and Findings Identified in the Included Studies
- (1)
- Individual and holistic approach (3 findings)
- (2)
- Clarity of the integration strategy and process (4 findings)
- (3)
- Timing of the rehabilitation process (2 findings)
- (4)
- Experience of persons with chronic diseases with the professionals (5 findings)
- (5)
- Changes in the understanding of health and work situation (3 findings)
- (6)
- Active involvement of the persons with chronic health conditions in process of professional integration (1 finding)
- (7)
- Competencies developed by the participant (2 findings)
- (8)
- Experience of participating in a group with other persons with chronic health conditions (3 findings)
- (9)
- Experience at the workplace (3 findings)
- (10)
- Motivating aspects of work (5 findings)
3.3.1. Individual and Holistic Approach
- -
- place, time and number of meetings with the professionals;
- -
- rhythm of progress; and
- -
- the kind of activities and how they were implemented.
3.3.2. Clarity of the Integration Strategy and Process
3.3.3. Timing of the Rehabilitation Process
3.3.4. Experience of PwCDs with Professionals
3.3.5. Changes in the Understanding of Health and Work Situation
3.3.6. Active Involvement of the Persons with Chronic Health Conditions in Process of Professional Integration
3.3.7. Competencies Developed by the Participant
3.3.8. Experience of Participating in a Group with Other Persons with Chronic Health Conditions
3.3.9. Experience at the Workplace
3.3.10. Motivating Aspects of Work
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A
Characteristics of Included Studies
| Andersen, 2014 [44] | |
| Context | Denmark; multidisciplinary, coordinated and early return-to-work (RTW) intervention under the management of the municipal sickness benefit offices; program aimed at employed persons on sick leave due to complex health-related problems irrespective of medical diagnoses; participation obligatory if the municipal sickness benefit officer estimates that it would enhance the chances of RTW |
| Participants | 17 workers (13 women); average age 44 years (range 23–61); on sick leave for approximately 8 weeks due to common mental problems; at the last interview 6 were still sick-listed, 3 were no longer sick-listed but unemployed, 8 had returned to work |
| Methods | Semi-structured interviews at 3 time points: (1) before intervention; (2) approximately 3 months after first interview; (3) 6–7 months after first interview; methodology in line with principles of the Interpretative Phenomenological Analysis |
| Areberg, 2013 [45] | |
| Context | Sweden; individual placement and support to help people with severe mental illness to find regular employment; data collected 12 months after the first meeting between participants and employment specialist; ongoing support |
| Participants * | 17 participants (7 female), 20–59 years old, with a diagnosis of schizophrenia, psychosis, affective disorder or other; 2 employed and working at the time of the interview, 2 in a position of repose, 4 in a practice place, 2 in education, 7 looking for a job |
| Methods | Semi-structured interviews 12 months after first contact with employment specialist; stratified sampling; content analysis |
| * Participants from the same RCT as Hasson [52] who published a qualitative study based on interviews performed in the first year of implementation. | |
| Boycott, 2015 [46] | |
| Context | UK; individual placement and support for unemployed persons with severe mental illness recruited from community mental health teams and early intervention in psychosis teams; service offered for at least 6 months |
| Participants | 31 participants (9 female) of the program who received IPS for at least 6 months; mean age 30.8 years; 14 psychosis, 8 schizophrenia, 4 bipolar disorder, 4 depression, 1 other diagnosis; 12 participants had gained employment at interview |
| Methods | Semi-structured interviews; interview after at least six months receiving the intervention; purposive sampling; thematic analysis |
| Buus, 2015 [47] | |
| Context | Denmark; two counselling sessions by an occupational physician encouraging low-back pain (LBP) patients who expressed concerns about their ability to maintain their current job to engage in their own treatment by changing work routines and by exercising; a workplace visit was carried out if required |
| Participants | 25 LBP patients (14 female); mean age 46.8 years |
| Methods | Semi-structured interviews with patients 1–4 years after concluding the counselling intervention; purpose sample; theoretical framework: “interactionism”; analysis: interpretative thematic approach |
| Cameron, 2012 [48] | |
| Context | UK, South of England; vocational guidance model that aims to help workers with mental health problems to retain their employment; project workers listen, clarify, give information, refer on to other services and collaborate to draw up client action plans; referrals to the project are done by general practitioners, other health workers, employers, or by clients themselves |
| Participants | 14 participants (10 female), average age 43.5 years (range 29–54) |
| Methods | Semi-structured individual interviews with project users; critical realist methodology |
| De Blasi, 2014 [49] | |
| Context | France; support groups for vocational rehabilitation integrated in a multidisciplinary hospital department for patients who wish to RTW or who have already returned to work and have difficulties or questions regarding to work; led by an occupational therapist and a psychologist; 4 monthly sessions of 90 min |
| Participants | 20 cancer patients (17 female); mean age at diagnosis: 47 years (range 37–55); cancer site: 16 breast, 2 hematopoietic, 1 digestive, 1 ear-nose-throat; 19 of them employed at diagnosis; 12 of them on sick leave during support group, 8 already working |
| Methods | Open questions in the questionnaire sent to participants one month after the last session; thematic analysis |
| Germundsson, 2011 [50] | |
| Context | Sweden; collaboration projects from a Swedish project group (NTG-New Routes to the Labour Market-Quality Assurance of Collaboration) within the Equal program; unemployed persons with mental health problems are part of the target population; duration: not found |
| Participants | (A) 8 service users (4 female), aged 19–52 years, unemployed and in vocational rehabilitation, sick-listed for 18–60 months due to mental health problems, six of them with little or no experience of paid employment; (B) 20 professionals (results for Group B not reported here) |
| Methods | Semi-structured interviews with service users on two occasions approximately six months apart; purposeful sample; thematic analysis guided by a theoretical framework |
| Glavare, 2012 [51] | |
| Context | Sweden; multi-professional pain-rehabilitation followed by a coached work-training (CWT) program; inclusion criteria for CWT were: unemployment, motivation for return-to work and at least 50% work capacity; the CWT program lasted 3–6 months |
| Participants | 11 participants (8 female); 22–58 years-old; with long-term musculoskeletal pain, who had participated in the CWT program, 8 employed at interview |
| Methods | Semi-structured interviews; interviews performed 4–21 (mean = 11) months after the program; Grounded theory approach |
| Hasson, 2011 [52] | |
| Context | Sweden (Malmö, Southern Sweden); individual placement and support to help people with severe mental illness to find regular employment; ongoing support at work |
| Participants | 15 clients of the service; characteristics not reported |
| Methods | Key informant interviews, non-participant observations and document analysis. Interviews with (A) 15 clients and (B) other actors (e.g., employment specialists, project head, mental health care staff, social insurance officers; results for Group B not considered in this review; content analysis |
| Haugli, 2011 [53] | |
| Context | Norway; multidisciplinary occupational rehabilitation program for patients on long-term sick leave, considered to have a fair chance of return-to work; it included different physical activities and individual and group based counselling aiming to increase function and work related processes; duration: not found |
| Participants | 20 individuals with musculoskeletal and/or psychological complaints; 10 had returned to work (3 men 46–58 years old, 7 women 41–56 years old) and 10 individuals were registered with a disability pension (3 men 41–53 years old, 7 women 41–56 years old) |
| Methods | Semi-structured telephone interviews with individuals who attended the rehabilitation program 3 years ago; purposive sampling; systematic text condensation inspired by Giorgi’s phenomenological analysis |
| Higgins, 2014 [54] | |
| Context | UK, Northern Ireland; the role of the general practitioner when managing illness that may deserve long-term sick leave is investigated; duration: not applicable |
| Participants | (A) 9 employees who had experienced a long-term sickness absence and (B) other stakeholders (e.g., government-level policy makers, trust-level human resources managers, occupational health clinicians; results for Group B not presented here) |
| Methods | Comparative case study within three Health and Social Care Trusts; 61 semi-structured interviews and 3 focus group; purposive sampling for the Trusts, otherwise convenience sampling; theoretically framed by Talcott Parsons’s model of the medical contribution to the sick role; realistic approach |
| Hubertsson, 2011 [55] | |
| Context | Sweden; two actors in the standard management of sickness absence are investigated: the Social Insurance Agency and Health Care; duration: not applicable |
| Participants | 15 participants (11 female); aged 33–63 years; with experience of sickness absence due to musculoskeletal disorders, 5 partly working, 2 partly unemployed, 5 on sick leave, 3 on disability pension |
| Methods | Semi-structured interviews; purposive sampling; latent content analysis |
| Jansson, 2014 [56] | |
| Context | Sweden, two counties; two strategies that aim to improve the work ability of persons with common mental disorders are investigated: (1) a pedagogical model of learning called problem-based method, lasting 12 weeks and (2) cognitive behavioral therapy, number of sessions not standardized |
| Participants | 16 participants (14 female); aged 30 to 63 years; 8 people from each intervention and each county; 13 working, 3 in sick leave |
| Methods | Semi-structured interviews; purposive sampling; content analysis |
| Kalef, 2014 [57] | |
| Context | Norway; job training program at Norway’s largest telecommunications company with financial support from Norway’s Labour and Welfare Organization (NAV), targeted at people with disabilities with a high school diploma and motivated to gain employment; three main components: computer training, personal development, and work-practice; duration: not found |
| Participants | (A) 15 completers of program, 14 current participants, and (B) other stakeholders (e.g., company leaders, program administrators, teachers, community members; results for Group B not presented here) |
| Methods | Personal observations, 29 semi-structured interviews and document review; purposive sampling; thematic analysis |
| Lewis, 2013 [58] | |
| Context | UK; personalized tailored supported employment intervention to help people with disabilities to find employment; funded by the Department for Work and Pensions and managed by its agency, Jobcentre Plus; variable duration, depending on length of absence and follow-along supports |
| Participants | 98 participants (40 female) from a sample of 11 providers; median age group 40–49 years, the primary disability of 48% of participants was a learning disability |
| Methods | Semi-structured interviews; purposive sampling; thematic analysis |
| Martin, 2012 [60] | |
| Context | Denmark; multidisciplinary, coordinated and tailored RTW-intervention for employees with relatively mild mental health problems *; sick-listed for 4–12 weeks; collaboration between a Danish municipality and a private company specialized in RTW; duration of intervention: 12 weeks |
| Participants | (A) 10 persons who completed the intervention; (B) other stakeholders (i.e., municipal social insurance officers and the multidisciplinary team); results for Group B not considered here |
| Methods | Interviews with participants were audio-taped, transcribed verbatim and coded thematically with the software NVivo |
| * Same intervention as in Martin (2015) [59] but implemented in only one municipality. | |
| Martin, 2015 [59] | |
| Context | Denmark; multidisciplinary, coordinated and tailored return-to-work-intervention for employees with common mental health problems; sick-listed for 4–12 weeks; collaboration between three Danish municipalities and a private company specialized in RTW; duration of intervention: 12 weeks |
| Participants | (A) 10 persons who completed the intervention, from three different municipalities; and (B) other stakeholders (i.e., municipal social insurance officers and the multidisciplinary team); results for Group B not considered here |
| Methods | Interviews with participants were audio-taped, transcribed verbatim and coded thematically with the software NVivo. |
| * Same intervention as in Martin (2012) [60] but implemented in 3 further municipalities. | |
| Mikkelsgard, 2014 [61] | |
| Context | Norway; supported employment project mainly targeted at people under the age of 25 years who receive financial assistance from the NAV (Norwegian Labour and Welfare Administration) and have mental health problems; collaboration between NAV and mental health services; voluntary participation based on individual motivation; duration: not found |
| Participants | Seven out of 52 participants of the project (5 women, 2 men); 20–35 years of age |
| Methods | Semi-structured interviews, audio-recorded and transcribed verbatim; content analysis |
| Nieminen, 2012 [62] | |
| Context | Eight European countries; lifelong learning strategy to facilitate social inclusion of unemployed persons with severe mental illness. Participants were offered training related to personal development and planning, employment and recovery, as well as opportunities for unpaid and paid activities *; duration: not found |
| Participants | 23 service users (9 female, 11 male, 3 not known); mean age 42.8 years (range 24–57); with schizophrenia, schizoaffective or bipolar disorder |
| Methods | Interviews (2–5 key informants from each site), chosen at random and interviewed at baseline, and 10 and 20 months; thematic approach |
| * Same intervention as Ramon (2011) [63]; both publications seem to be based on the same interviews; only additional information to Ramon 2011 has been extracted. | |
| Ramon, 2011 [63] | |
| Context | (see Nieminen, 2012) * |
| Participants | Service users with schizophrenia, schizoaffective or bi-polar disorder |
| Methods | Semi-structured interviews (2–5 in each site) at baseline and 21 interviews 10 months later; 138 written self-reports at baseline and 99 ten months later |
| * Same intervention as Nieminen (2012) [62]. | |
| Reagon, 2011 [64] | |
| Context | UK, Wales; condition management programs (CMPs) led by the National Health Service to help individuals to manage health conditions better in relation to a return-to-work; characterized by a biopsychosocial approach and cognitive behavioral therapy techniques; clients are voluntarily referred to the CMP by the Jobcentre; about 13 weeks intervention after the evaluation, depending on individual needs |
| Participants | (A) 15 participants (9 female) who had recently completed the program; 20–50 years-old; with musculoskeletal (n = 7) and mental health problems (n = 8) as primary health condition; (B) 12 staff members; results for Group B not considered in this review |
| Methods | Semi-structured interviews; tape-recorded and transcribed verbatim; purposive sample; thematic analysis |
| Secker, 2012 [65] | |
| Context | UK; Condition Management Programmes aimed at supporting persons on incapacity benefits due to long-term conditions to RTW; joint venture between the UK Department of Health and the Department for Work and Pensions; duration: not found |
| Participants | 39 participants of the program (22 female) with mental health problems (n = 20), musculoskeletal (n = 8), cardiovascular (n = 4), and a combination of conditions (n = 7); most of them (n = 31) in their middle years |
| Methods | Twelve focus groups conducted at the site of the corresponding program; the discussions were tape-recorded and transcribed verbatim; purposive sample; text analysis |
| Tiedtke, 2012 [66] | |
| Context | Belgium; legislation affecting RTW of women with breast cancer; duration: not applicable |
| Participants | (A) 5 women who survived breast cancer and (B) 4 representatives of patient associations and further stakeholders (e.g., treating physicians, employers, social security physicians); results for Group B not considered in this review |
| Methods | Three multidisciplinary focus groups; discussions tape-recorded and transcribed verbatim; purposive sample; thematic analysis |
| Vandekinderen, 2012 [67] | |
| Context | Belgium; labor-market training program for women with mental health problems; five linear modules: registration, observation, guidance, training for employment, and work placement; duration: not found |
| Participants | (A) 11 women with mental health problems and substance dependence and (B) other stakeholders (i.e., the chief manager, support workers, and project partners); results for Group B not considered in this review |
| Methods | Document analysis of all available project documents and 17 interviews with women with mental health problems; the interviews were audio-taped, transcribed and returned to the participants for review; interpretative research approach |
References
- Scaratti, C.; Leonardi, M.; Silvaggi, F.; Ávila, C.; Muñoz-Murillo, A.; Stavroussi, P.; Roka, O.; Burger, H.; Fheodoroff, K.; Tobiasz-Adamczyk, B.; et al. Mapping European welfare models: State of the art of strategies for professional integration and reintegration of persons with chronic diseases including mental health conditions. Int. J. Environ. Res. Public Health 2018, 15, 781. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. The Five Year Forward View for Mental Health. In A Report from the Independent Mental Health Taskforce to the NHS in England; NHS: London, UK, 2016. [Google Scholar]
- European Commission. European Disability Strategy 2010–2020: A Renewed Commitment to a Barrier-Free Europe; European Commission: Brussels, Belgium, 2010. [Google Scholar]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2007. [Google Scholar]
- Pathways Consortium. Report on the Comparison of the Available Strategies for Professionals Integration and Reintegration of Persons with Chronic Diseases and Mental Health Issues. Available online: https://www.path-ways.eu/wp-content/uploads/pathways_report_identify.pdf (accessed on 8 April 2018).
- European Commission. Population Ageing in Europe: Facts, Implications and Policies; Publications Office of the European Union: Luxembourg, 2014; Available online: https://ec.europa.eu/research/social-sciences/pdf/policy_reviews/kina26426enc.pdf (accessed on 13 April 2018).
- Naegele, G.; Walker, A. A guide to Good Practice in Age Management; European Foundation for the Improvement of Living and Working Conditions: Luxembourg, 2006; Available online: http://www.ageingatwork.eu/resources/a-guide-to-good-practice-in-age-management.pdf (accessed on 13 April 2018).
- Rice, D.P.; LaPlante, M.P. Chronic illness, disability, and increasing longevity. In The Economics and Ethics of Long-Term Care and Disability; American Enterprise Institute for Public Policy Research: Washington, DC, USA, 1988. [Google Scholar]
- Rothenberg, R.B.; Koplan, J.P. Chronic disease in the 1990s. Annu. Rev. Public Health 1990, 11, 267–296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Rijken, M.; Struckmann, V.; Dyakova, M.; Melchiorre, M.G.; Rissanen, S.; Ginneken, E.V. ICARE4EU: Improving care for people with multiple chronic conditions in Europe. Eurohealth Int. 2013, 19, 29–31. [Google Scholar]
- Australian Institute of Health and Welfare. Chronic Disease and Participation in Work. Available online: https://www.aihw.gov.au/reports/chronic-disease/chronic-disease-participation-work/contents/table-of-contents (accessed on 9 April 2018).
- Blanc, P.D.; Cisternas, M.; Smith, S.; Yelin, E.H. Asthma, employment status, and disability among adults treated by pulmonary and allergy specialists. Chest 1996, 109, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Kremer, A.; Pal, T.; van Keimpema, A. Employment and disability for work in patients with COPD: A cross-sectional study among Dutch patients. Int. Arch. Occup. Environ. Health 2006, 80, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Lerner, D.; Adler, D.A.; Chang, H.; Lapitsky, L.; Hood, M.Y.; Perissinotto, C.; Reed, J.; McLaughlin, T.J.; Berndt, E.R.; Rogers, W.H. Unemployment, job retention, and productivity loss among employees with depression. Psychiatr. Serv. 2004, 55, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Kraut, A.; Walld, R.; Tate, R.; Mustard, C. Impact of diabetes on employment and income in Manitoba, Canada. Diabetes Care 2001, 24, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.; Brownell, K.D. Bias, discrimination, and obesity. Obesity 2001, 9, 788–805. [Google Scholar] [CrossRef] [PubMed]
- Ameille, J.; Pairon, J.; Bayeux, M.; Brochard, P.; Choudat, D.; Conso, F.; Devienne, A.; Garnier, R.; Iwatsubo, Y. Consequences of occupational asthma on employment and financial status: A follow-up study. Eur. Respir. J. 1997, 10, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Pagan, J.A.; Davila, A. Obesity, occupational attainment, and earnings. Soc. Sci. Q. 1997, 756–770. [Google Scholar]
- Register, C.A.; Williams, D.R. Wage effects of obesity among young workers. Soc. Sci. Q. 1990, 71, 130. [Google Scholar]
- Kessler, R.C.; House, J.S.; Turner, J.B. Unemployment and health in a community sample. J. Health Soc. Behav. 1987, 28, 51–59. [Google Scholar] [CrossRef]
- Glass, J.; Fujimoto, T. Housework, paid work, and depression among husbands and wives. J. Health Soc. Behav. 1994, 35, 179–191. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Does employment affect health? J. Health Soc. Behav. 1995, 36, 230–243. [Google Scholar] [CrossRef]
- Heijbel, B.; Josephson, M.; Jensen, I.; Stark, S.; Vingård, E. Return to work expectation predicts work in chronic musculoskeletal and behavioral health disorders: Prospective study with clinical implications. J. Occup. Rehabil. 2006, 16, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Curtin, R.B.; Oberley, E.T.; Sacksteder, P.; Friedman, A. Differences between employed and nonemployed dialysis patients. Am. J. Kidney Dis. 1996, 27, 533–540. [Google Scholar] [CrossRef]
- Corral, A.; Durán, J.; Isusi, I. Employment Opportunities for People with Chronic Diseases. Available online: https://www.eurofound.europa.eu/sites/default/files/ef1459en.pdf (accessed on 27 March 2018).
- European Chronic Disease Alliance. The Employment of People with Chronic Diseases. Available online: https://ec.europa.eu/health/sites/health/files/interest_groups/docs/ev_20171127_co02_en.pdf (accessed on 27 March 2018).
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:52010DC0636&from=EN (accessed on 28 March 2018).
- Pathways Consortium. Participation to Healthy Workplaces and Inclusive Strategies in the Work Sector. Available online: http://www.path-ways.eu/project/ (accessed on 27 March2018).
- Muñoz-Murillo, A.; Esteban, E.; Ávila, C.C.; Fheodoroff, K.; Haro, J.M.; Leonardi, M.; Olaya, B. Furthering the evidence of the effectiveness of employment strategies for people with mental health disorders in Europe: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 838. [Google Scholar] [CrossRef] [PubMed]
- Sabariego, C.; Coenen, M.; Ito, E.; Fheodoroff, K.; Scaratti, C.; Leonardi, M.; Vlachou, A.; Stavroussi, P.; Brecelj, V.; Kovacic, D.S.; et al. Effectiveness of Integration and Re-Integration into Work Strategies for Persons with Chronic Conditions: A Systematic Review of European Strategies. Int. J. Environ. Res. Public Health 2018, 15, 552. [Google Scholar] [CrossRef] [PubMed]
- Vlachou, A.; Stavroussi, P.; Roka, O.; Vasilou, E.; Papadimitriou, D.; Scaratti, C.; Kadyrbaeva, A.; Fheodoroff, K.; Brecelj, V.; Svestkova, O.; et al. Policy Guidelines for Effective Inclusion and Reintegration of People with Chronic Diseases in the Workplace: National and European Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 493. [Google Scholar] [CrossRef] [PubMed]
- Noyes, J.; Popay, J.; Pearson, A.; Hannes, K.; Booth, A.; Cochrane Qualitative Research Methods Group. Qualitative research and Cochrane reviews. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 (Updated March 2011); Higgins, J., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Ames, H.M.R.; Glenton, C.; Lewin, S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: A synthesis of qualitative evidence. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Oortwijn, W.; Nelissen, E.; Adamini, S.; van den Heuvel, S.; Geuskens, G.; Burdorf, L. Social Determinants State of the Art Reviews—Health of People of Working Age—Full Report; European Commission Directorate General for Health and Consumers: Luxembourg, 2011. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellent. Methods for the Development of NICE Public Health Guidance, 3rd ed.; NICE: Manchester, UK, 2012; Volume 2018. [Google Scholar]
- Critical Appraisal Skills Programme. CASP Qualitative Checklist. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist.pdf (accessed on 8 April 2018).
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook; SAGE: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using Qualitative Evidence in Decision Making for Health and Social Interventions: An Approach to Assess Confidence in Findings from Qualitative Evidence Syntheses (GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Urries, F.B.; Verdugo, M.A. Sheltered Employment Centers: Characteristics and users’ perception. Work 2011, 38, 155–161. [Google Scholar] [PubMed]
- Tamminga, S.J.; de Boer, A.G.; Bos, M.M.; Fons, G.; Kitzen, J.J.; Plaisier, P.W.; Verbeek, J.H.; Frings-Dresen, M.H. A hospital-based work support intervention to enhance the return to work of cancer patients: A process evaluation. J. Occup. Rehabil. 2012, 22, 565–578. [Google Scholar] [CrossRef] [PubMed]
- Fassier, J.B.; Durand, M.J.; Caillard, J.F.; Roquelaure, Y.; Loisel, P. Results of a feasibility study: Barriers and facilitators in implementing the Sherbrooke model in France. Scand. J. Work Environ. Health 2015, 41, 223–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, M.F.; Nielsen, K.; Brinkmann, S. How do workers with common mental disorders experience a multidisciplinary return-to-work intervention? A qualitative study. J. Occup. Rehabil. 2014, 24, 709–724. [Google Scholar] [CrossRef] [PubMed]
- Areberg, C.; Bjorkman, T.; Bejerholm, U. Experiences of the individual placement and support approach in persons with severe mental illness. Scand. J. Caring Sci. 2013, 27, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Boycott, N.; Akhtar, A.; Schneider, J. Work is good for me: Views of mental health service users seeking work during the UK recession, a qualitative analysis. J. Ment. Health 2015, 24, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Buus, N.; Jensen, L.D.; Maribo, T.; Gonge, B.K.; Angel, S. Low back pain patients’ beliefs about effective/ineffective constituents of a counseling intervention: A follow-up interview study. Disabil. Rehabil. 2015, 37, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Cameron, J.; Walker, C.; Hart, A.; Sadlo, G.; Haslam, I.; Retain Support, G. Supporting workers with mental health problems to retain employment: Users’ experiences of a UK job retention project. Work 2012, 42, 461–471. [Google Scholar] [PubMed]
- De Blasi, G.; Bouteyre, E.; Bretteville, J.; Boucher, L.; Rollin, L. Multidisciplinary department of “Return to Work After a Cancer”: A French experience of support groups for vocational rehabilitation. J. Psychosoc. Oncol. 2014, 32, 74–93. [Google Scholar] [CrossRef] [PubMed]
- Germundsson, P.; Hillborg, H.; Danermark, B. Interagency collaboration in vocational rehabilitation for persons with mental health problems: The perspective of the service users and the professionals. Disabil. Soc. 2011, 26, 699–713. [Google Scholar] [CrossRef]
- Glavare, M.; Lofgren, M.; Schult, M.L. Between unemployment and employment: Experience of unemployed long-term pain sufferers. Work 2012, 43, 475–485. [Google Scholar] [PubMed]
- Hasson, H.; Andersson, M.; Bejerholm, U. Barriers in implementation of evidence-based practice: Supported employment in Swedish context. J. Health Organ. Manag. 2011, 25, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Haugli, L.; Maeland, S.; Magnussen, L.H. What facilitates return to work? Patients’ experiences 3 years after occupational rehabilitation. J. Occup. Rehabil. 2011, 21, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, A.; Porter, S.; O’Halloran, P. General practitioners’ management of the long-term sick role. Soc. Sci. Med. 2014, 107, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Hubertsson, J.; Petersson, I.F.; Arvidsson, B.; Thorstensson, C.A. Sickness absence in musculoskeletal disorders—Patients’ experiences of interactions with the social insurance agency and health care. A qualitative study. BMC Public Health 2011, 11, 107. [Google Scholar] [CrossRef] [PubMed]
- Jansson, I.; Perseius, K.I.; Gunnarsson, A.B.; Bjorklund, A. Work and everyday activities: Experiences from two interventions addressing people with common mental disorders. Scand. J. Occup. Ther. 2014, 21, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Kalef, L.; Barrera, M.; Heymann, J. Developing inclusive employment: Lessons from Telenor Open Mind. Work 2014, 48, 423–434. [Google Scholar] [PubMed]
- Lewis, R.; Dobbs, L.; Biddle, P. If this wasn’t here I probably wouldn’t be: Disabled workers’ views of employment support. Disabil. Soc. 2013, 28, 1089–1103. [Google Scholar] [CrossRef]
- Martin, M.H.T.; Moefelt, L.; Nielsen, M.B.D.; Rugulies, R. Barriers and facilitators for implementation of a return-to-work intervention for sickness absence beneficiaries with mental health problems: Results from three Danish municipalities. Scand. J. Public Health 2015, 43, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.H.T.; Nielsen, M.B.D.; Petersen, S.M.A.; Jakobsen, L.M.; Rugulies, R. Implementation of a coordinated and tailored return-to-work intervention for employees with mental health problems. J. Occup. Rehabil. 2012, 22, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsgard, K.A.; Granerud, A.; Hoye, S. People with mental illness returning to work: A qualitative evaluation of a Norwegian project. Scand. J. Occup. Ther. 2014, 21, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Nieminen, I.; Ramon, S.; Dawson, I.; Flores, P.; Leahy, E.; Pedersen, M.L.; Kaunonen, M. Experiences of social inclusion and employment of mental health service users in a European Union project. Int. J. Ment. Health 2012, 41, 3–23. [Google Scholar] [CrossRef]
- Ramon, S.; Griffiths, C.A.; Nieminen, I.; Pedersen, M.; Dawson, I. Towards social inclusion through lifelong learning in mental health: Analysis of change in the lives of the EMILIA project service users. Int. J. Soc. Psychiatry 2011, 57, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Reagon, C. Vocational rehabilitation in Wales: A mixed method evaluation of condition management programmes. Int. J. Rehabil. Res. 2011, 34, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Secker, J.; Pittam, G.; Ford, F. Customers’ perspectives on the impact of the Pathways to Work condition management programme on their health, well-being and vocational activity. Perspect. Public Health 2012, 132, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Tiedtke, C.; Donceel, P.; Knops, L.; Désiron, H.; de Casterlé, B.D.; de Rijk, A. Supporting return-to-work in the face of legislation: Stakeholders’ experiences with return-to-work after breast cancer in Belgium. J. Occup. Rehabil. 2012, 22, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Vandekinderen, C.; Roets, G.; Vandenbroeck, M.; Vanderplasschen, W.; Van Hove, G. One size fits all? The social construction of dis-employ-abled women. Disabil. Soc. 2012, 27, 703–716. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Foitzek, N.; Avila, C.C.; Ivandic, I.; Bitenc, C.; Cabello, M.; Gruber, S.; Leonardi, M.; Munoz-Murillo, A.; Scaratti, C.; Tobiasz-Adamczyk, B.; et al. What Persons with Chronic Health Conditions Need to Maintain or Return to Work-Results of an Online-Survey in Seven European Countries. Int. J. Environ. Res. Public Health 2018, 15, 595. [Google Scholar] [CrossRef] [PubMed]
- Popova, Y.; Kozhevnikova, M. Interdependence of HDI and budget redistribution within the Scandinavian and Continental Social Models. Econ. Manag. 2013, 18, 562–575. [Google Scholar] [CrossRef]
- Eikemo, T.A.; Huisman, M.; Bambra, C.; Kunst, A.E. Health inequalities according to educational level in different welfare regimes: A comparison of 23 European countries. Sociol. Health Illn. 2008, 30, 565–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenger, H. Welfare regimes in central and Eastern Europe: Incorporating post-communist countries in a welfare regime typology. Contemp. Issues Ideas Soc. Sci. 2007, 3, 1–30. [Google Scholar]
- Midttun, A.; Gautesen, K.; Gjølberg, M. The political economy of CSR in Western Europe. Int. J. Bus. Soc. 2006, 6, 369–385. [Google Scholar] [CrossRef]
- Kausto, J.; Miranda, H.; Martimo, K.-P.; Viikari-Juntura, E. Partial sick leave—Review of its use, effects and feasibility in the Nordic countries. Scand. J. Work Environ. Health 2008, 239–249. [Google Scholar] [CrossRef]
- Horwitz, A.; Horwitz, H. Politics and policies. J. Insur. Med. (Seattle) 2014, 44, 49–52. [Google Scholar]
- Eikemo, T.A.; Bambra, C.; Judge, K.; Ringdal, K. Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2281–2295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purnell, J.; Johnson, A. Improving Health and Work: Changing Lives. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/210858/hwwb-improving-health-and-work-changing-lives.pdf (accessed on 9 April 2018).
- Rinaldi, M.; Miller, L.; Perkins, R. Implementing the individual placement and support (IPS) approach for people with mental health conditions in England. Int. Rev. Psychiatry 2010, 22, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Waddell, G.; Burton, A.K. Is Work Good for Your Health and Well-Being; Department for Work and Pensions: London, UK, 2006.
- Bevan, S.; Quadrello, T.; McGee, R. Fit for Work? Musculoskeletal Disorders in the European Workforce. The Work Foundation, 2009. Available online: http://www.bollettinoadapt.it/old/files/document/3704FOUNDATION_19_10.pdf (accessed on 13 April 2018).
- Dorner, T.E.; Alexanderson, K.; Svedberg, P.; Ropponen, A.; Stein, K.V.; Mittendorfer-Rutz, E. Sickness absence due to back pain or depressive episode and the risk of all-cause and diagnosis-specific disability pension: A Swedish cohort study of 4,823,069 individuals. Eur. J. Pain (Lond. Engl.) 2015, 19, 1308–1320. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar]
- Hassard, J.; Cox, T.; Murawski, S.; De Meyer, S.; Muylaert, K. Mental Health Promotion in the Workplace—A Good Practice Report; Flintrop, J., Ed.; European Agency for Safety and Health at Work, EU-OSHA: Bilbao, Spain, 2011; Available online: https://osha.europa.eu/en/tools-and-publications/publications/reports/mental-health-promotion-workplace_TEWE11004ENN (accessed on 13 April 2018).
- Henderson, M.; Glozier, N.; Holland Elliott, K. Long term sickness absence: Is caused by common conditions and needs managing. Br. Med. J. 2005, 330, 802–803. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, A.K.; Overland, S.; Aakvaag, H.F.; Harvey, S.B.; Hotopf, M.; Mykletun, A. Common mental disorders and disability pension award: Seven year follow-up of the HUSK study. J. Psychosom. Res. 2010, 69, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Ruston, A.; Smith, A.; Fernando, B. Diabetes in the workplace—Diabetic’s perceptions and experiences of managing their disease at work: A qualitative study. BMC Public Health 2013, 13, 386. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.A. Diabetes at work: A grounded-theory pilot study. AAOHN J. 2011, 59, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Weijman, I.; Ros, W.J.; Rutten, G.E.; Schaufeli, W.B.; Schabracq, M.J.; Winnubst, J.A. The role of work-related and personal factors in diabetes self-management. Patient Educ. Couns. 2005, 59, 87–96. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Findings | Confidence of Findings * | Explanation for Level Confidence | Contributing Studies | |
|---|---|---|---|---|
| Use of an individual and holistic approach | ||||
| 1. | Persons with chronic health conditions wanted professionals to show a genuine interest to understand and accept them as individuals | Moderate | Moderate concerns about methodological limitations; moderate concerns about relevance | Andersen 2014 [44], Areberg 2013 [45], Glavare 2012 [51], Haugli 2011 [53], Hubertsson 2011 [55], Martin 2012 [60], Mikkelsgard 2014 [61], Reagon 2011 [64] |
| 2. | Persons with chronic conditions found it helpful to be seen from different perspectives (e.g., medical, psychological) and in more areas than the one directly related to work | Moderate | Moderate concerns about methodological limitations; moderate concerns about relevance | Andersen 2014 [44], Glavare 2012 [51], Lewis 2013 [58], Martin 2012 [60], Martin 2015 [59], Mikkelsgard 2014 [61], Secker 2012 [65], Vandekinderen 2012 [67] |
| 3. | Flexibility in the implementation of the strategy and the contact with the professionals was highly appreciated by the participants | Moderate | Moderate concerns about methodological limitations; moderate concerns about relevance | Andersen 2014 [44], Areberg 2013 [45], Cameron 2012 [48], Germundsson 2011 [50], Glavare 2012 [51], Kalef 2014 [57], Lewis 2013 [58], Martin 2012 [60], Mikkelsgard 2014 [61], Reagon 2011 [64], Secker 2012 [65], Vandekinderen 2012 [67] |
| Clarity of the integration strategy and process | ||||
| 4. | Providing a definition and clarification of the problem and setting a clear course of action was found helpful | Low | Minor concerns about methodological limitations; moderate concerns about relevance and adequacy | Andersen 2014 [44], Secker 2012 [65] |
| 5. | The role of activities and professionals is sometimes difficult to understand, leading to confusion and demotivation | Moderate | Moderate concerns about methodological limitations and relevance | Andersen, 2014 [44], Germundsson, 2011 [50], Martin, 2012 [60], Mikkelsgard, 2014 [61] |
| 6. | Some persons found it difficult to move forward because of receiving wrong or insufficient information about requisites, procedures and decisions affecting their professional integration | Moderate | Moderate concerns about methodological limitations, relevance and adequacy | Hubertsson 2011 [55], Mikkelsgard 2014 [61], Tiedtke 2012 [66] |
| 7. | Persons with chronic diseases appreciated that professionals and institutions shared a common understanding of their situation and the intervention plan | Low | Moderate concerns on methodological limitations and adequacy; substantial concerns on relevance | Areberg 2013 [45], Germundsson 2011 [50], Mikkelsgard 2014 [61] |
| Timing of the rehabilitation process | ||||
| 8. | Some people would have liked to start working for their professional integration at an earlier stage | Moderate | Moderate concerns about methodological limitations; minor concerns about relevance | Hubertsson 2011 [55], Jansson 2014 [56], Martin 2012 [60], Martin 2015 [59], Tiedtke 2012 [66] |
| 9. | A continuous rehabilitation process is positively experienced by subjects | Low | Moderate concerns about methodological limitations, relevance and adequacy | Germundsson, 2011 [50], Hubertsson 2011 [55], Mikkelsgard 2014 [61] |
| Experience of persons with chronic diseases with professionals | ||||
| 10. | Perceiving professionals as experts increased the engagement of the participants with the intervention | Moderate | Moderate methodological limitations; minor concerns about relevance | Andersen 2014 [44], Areberg 2013 [45], Cameron 2012 [48], Lewis 2013 [58], Martin 2015 [59], Tiedtke 2012 [66] |
| 11. | The interaction style of the professional was perceived as a key element of the intervention | Moderate | Moderate concerns about methodological limitations; minor concerns about relevance | Andersen 2014 [44], Cameron 2012 [48], Glavare 2012 [51], Hubertsson 2011 [55], Martin 2012 [60], Mikkelsgard 2014 [61], Reagon 2011 [64], Secker 2012 [65], Tiedtke 2012 [66] |
| 12. | Participants appreciated receiving practical support | Moderate | Moderate concerns about methodological limitations; minor concerns about relevance | Areberg 2013 [45], Boycott 2015 [46], Cameron 2012 [48], Glavare 2012 [51], Higgins 2014 [54], Kalef 2014 [57], Lewis 2013 [58], Martin 2015 [59], Mikkelsgard 2014 [61], Secker 2012 [65], Tiedtke 2012 [66] |
| 13. | Stability and availability of the support workers was associated with a sense of security and relief | Moderate | Moderate concerns about methodological limitations and moderate concerns about relevance | Lewis 2013 [58], Mikkelsgard 2014 [61], Secker 2012 [65] |
| 14. | Professionals were a source of emotional support for participants | Moderate | Minor concerns about methodological limitations and moderate concerns about relevance | Areberg 2013 [45], Boycott 2015 [46], Cameron, 2012 [48], Kalef 2014 [57] |
| Changes in the understanding of the health and work situation | ||||
| 15. | Participants liked to increase their understanding of symptoms and mechanisms of the disease, and their health status | High | Minor concerns about methodological limitations, coherence and adequacy | Andersen 2014 [44], Areberg 2013 [45], Buus 2015 [47], De Blasi 2014 [49], Jansson 2014 [56], Reagon 2011 [64], Secker 2012 [65] |
| 16. | Professionals’ focus on workplace conditions helped participants to broaden their understanding of work dynamics and showed them possible ways to be a resource for the company | Moderate | Moderate concerns about methodological limitations and relevance; minor concerns regarding adequacy | Buus 2015 [47], Cameron 2012 [48], Kalef 2014 [57] |
| 17. | Participants appreciated increasing their own understanding | Moderate | Moderate concerns about methodological limitations and relevance | Cameron 2012 [48], Haugli 2011 [53], Kalef 2014 [57], Nieminen 2012 [62] |
| Active involvement of the persons with chronic health conditions in process of professional integration | ||||
| 18. | Participants appreciated working actively and being involved in the development and implementation of the activities to improve their professional integration | Moderate | Minor concerns about methodological limitations; moderate concerns about relevance | Areberg 2013 [45], Buus 2015 [47], Glavare 2012 [51], Jansson 2014 [56], Mikkelsgard 2014 [61], Secker 2012 [65] |
| Competencies developed by the participant | ||||
| 19. | Participants welcomed being taught skills to manage problematic situations in different areas of life | Moderate | Moderate concerns about methodological limitations and relevance | Boycott 2015 [46], Cameron 2012 [48], Glavare 2012 [51], Jansson 2014 [56], Martin 2012 [60], Martin 2015 [59], Mikkelsgard 2014 [61], Ramon 2011 [63], Reagon 2011 [64], Secker 2012 [65] |
| 20. | Participants felt that being immersed in a social atmosphere offered them the opportunity to develop and practice social skills | Low | Moderate concerns about methodological limitations; substantial concerns about relevance | Boycott 2015 [46], Haugli 2011 [53], Kalef 2014 [57] |
| Experience of participating in a group with other persons with chronic health conditions | ||||
| 21. | Several subjects attending an educational or support group found that meeting other persons who face similar problems made them normalize their situation | Moderate | Moderate concerns about methodological limitations; minor concerns about relevance | Andersen 2014 [44], Cameron 2012 [48], De Blassi 2014 [49], Glavare 2012 [51], Haugli 2011 [53], Jansson 2014 [56], Secker 2012 [65] |
| 22. | Meeting persons with similar concerns helped participants to learn more about their situation and motivated them to try a new approach | Moderate | Moderate concerns about methodological limitations and relevance; minor concerns regarding adequacy | De Blassi 2014 [49], Haugli 2011 [53], Jansson 2014 [56], Secker 2012 [65] |
| 23. | Some persons experienced difficulties sharing personal experiences in a group | Low | Serious concerns about methodological limitations; moderate concerns about relevance; minor concerns about adequacy | Haugli 2011 [53], Jansson 2014 [56], Reagon 2011 [64] |
| Experience at the workplace | ||||
| 24. | Support from employers and managers is perceived by employees as a key element to succeed in their professional integration | Moderate | Moderate concerns about methodological limitations and relevance | Areberg 2013 [45], Cameron 2012 [48], Glavare 2012 [51], Haugli 2011 [53], Jansson 2014 [56], Mikkelsgard 2014 [61], Lewis 2013 [58], Tiedtke 2012 [66] |
| 25. | The amount of support provided by colleagues plays an important role in work integration | Moderate | Moderate concerns about methodological limitations and relevance | Cameron 2012 [48], Glavare 2012 [51], Lewis 2013 [58] |
| 26. | Some organizations have a working culture and physical environment that makes the provision of support easier | Moderate | Moderate concerns about methodological limitations and relevance | Cameron 2012 [48], Kalef 2014 [57], Jansson, 2014 [56], Lewis 2013 [58], Nieminen 2012 [62], Vandekinderen 2012 [67] |
| Motivating aspects of work | ||||
| 27. | The expectation to improve their financial situation motivated people with chronic health conditions to find a job | Moderate | Moderate concerns about methodological limitations and relevance | Hasson 2011 [52], Lewis 2013 [58], Mikkelsgard 2014 [61], Vandekinderen 2012 [67] |
| 28. | Subjects found that having a job or doing an internship facilitates social inclusion and interaction | Moderate | Moderate concerns about methodological limitations and relevance | Kalef 2014 [57], Lewis 2013 [58], Mikkelsgard 2014 [61], Nieminen 2012 [62] |
| 29. | Having an occupation allowed persons with chronic diseases to focus on something other than the disease | Low | Moderate concerns about methodological limitations, relevance and adequacy | Areberg 2013 [45], Mikkelsgard 2014 [61], Ramon 2011 [63] |
| 30. | Participants found it very important to do something that they could enjoy | Very low | Serious concerns about methodological limitations, relevance and adequacy; moderate concerns about coherence | Boycott 2015 [46], Ramon 2011 [63] |
| 31. | Having a job was associated with an increase in self-esteem and self-confidence | Low | Moderate concerns about methodological limitations and relevance; minor concerns regarding adequacy | Lewis 2013 [58], Mikkelsgard 2014 [61], Nieminen 2012 [62] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteban, E.; Coenen, M.; Ito, E.; Gruber, S.; Scaratti, C.; Leonardi, M.; Roka, O.; Vasilou, E.; Muñoz-Murillo, A.; Ávila, C.C.; et al. Views and Experiences of Persons with Chronic Diseases about Strategies that Aim to Integrate and Re-Integrate Them into Work: A Systematic Review of Qualitative Studies. Int. J. Environ. Res. Public Health 2018, 15, 1022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051022
Esteban E, Coenen M, Ito E, Gruber S, Scaratti C, Leonardi M, Roka O, Vasilou E, Muñoz-Murillo A, Ávila CC, et al. Views and Experiences of Persons with Chronic Diseases about Strategies that Aim to Integrate and Re-Integrate Them into Work: A Systematic Review of Qualitative Studies. International Journal of Environmental Research and Public Health. 2018; 15(5):1022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051022
Chicago/Turabian StyleEsteban, Eva, Michaela Coenen, Elizabeth Ito, Sonja Gruber, Chiara Scaratti, Matilde Leonardi, Olga Roka, Evdokia Vasilou, Amalia Muñoz-Murillo, Carolina C. Ávila, and et al. 2018. "Views and Experiences of Persons with Chronic Diseases about Strategies that Aim to Integrate and Re-Integrate Them into Work: A Systematic Review of Qualitative Studies" International Journal of Environmental Research and Public Health 15, no. 5: 1022. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051022