Exploring the Determinants of Perceived Risk of Middle East Respiratory Syndrome (MERS) in Korea



Abstract
:1. Introduction
2. Theoretical Background and Hypothesis
2.1. Previous Studies about MERS
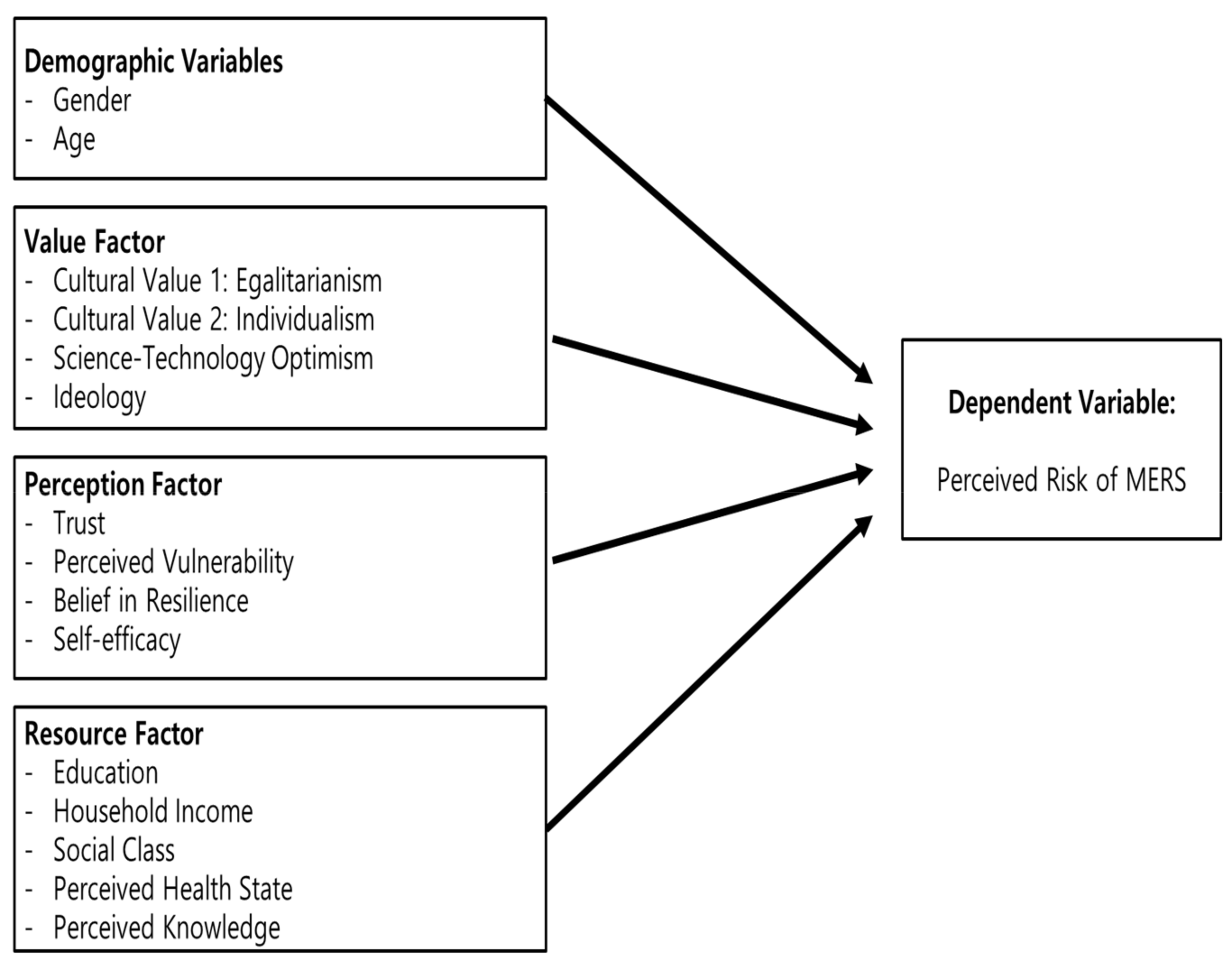
2.2. Determinants of Risk Perception
2.2.1. Value Factor
2.2.2. Perception Factor
2.2.3. Resource Factor
3. Sample and Measure
3.1. Sample
3.2. Measure
4. Analysis
4.1. Basic Description
4.2. Causal Structure
4.3. Discussion
5. Conclusions
5.1. Summary
5.2. Implications
Author Contributions
Conflicts of Interest
References
- Seoul Metropolitan Government. White Paper of MERS; Seoul Metropolitan Government: Seoul, Korea, 2016.
- Slovic, P. Perception of Risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Cho, S. Middle East respiratory syndrome risk perception among students at a university in South Korea, 2015. Am. J. Infect. Control 2017, 45, e53–e60. [Google Scholar] [CrossRef] [PubMed]
- Jacob, B.; Mawson, A.R.; Payton, M.; Guignard, J.C. Disaster Mythology and Fact: Hurricane Katrina and Social Attachment. Public Health Rep. 2008, 123, 555–566. [Google Scholar] [CrossRef] [PubMed]
- Jhoo, D. MERS Fear, Rumors Spreading. Korea Times. 2017. Available online: http://www.koreatimes.co.kr/www/news/nation/2015/06/116_179800.html (accessed on 2 March 2018).
- Al Ghobain, M.; Aldrees, T.; Alenezi, A.; Alqaryan, S.; Aldabeeb, D.; Alotaibi, N.; Aldhabib, A.; Alghalibi, S.; Alharethy, S. Perception and attitude of emergency room resident physicians toward middle east respiratory syndrome outbreak. Emerg. Med. Int. 2017. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Yang, H.J.; Kim, G.; Cheong, H.-K.; Choi, B.Y. Preventive behaviors by the level of perceived infection sensitivity during the Korea outbreak of Middle East Respiratory Syndrome in 2015. Epidemiol. Health 2016, 38. [Google Scholar] [CrossRef]
- Makhlouf, M.M.; Omer, S.R.; Elyamani, R.A.A.; Aabdien, M.H.; Sharaf, M.Q.; El-Sayed, A.M.; Farag, E.A.; Alkubaisi, N.; Al-Hajri, M.M.; Board, A.; et al. Use of health belief model to assess risk perception and practices of camel farm owners in Doha about MERS-COV, 2015. J. Emerg. Med. 2016. [Google Scholar] [CrossRef]
- Song, J.; Song, T.M.; Seo, D.-C.; Jin, D.-L.; Kim, J.S. Social big data analysis of information spread and perceived infection risk during the 2015 middle east respiratory syndrome outbreak in South Korea. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.-H.; Yoo, W.; Noh, G.; Park, K. The impact of social media on risk perceptions during the MERS outbreak in South Korea. Comput. Hum. Behav. 2017, 72, 422–431. [Google Scholar] [CrossRef]
- Kim, C.W.; Song, H.R. Structural relationships among public’s risk characteristics, trust, risk perception and preventive behavioral intention: The case of MERS in Korea. Crisisnomy 2017, 13, 85–95. [Google Scholar] [CrossRef]
- Choi, J.S.; Ha, J.Y.; Lee, J.S.; Lee, Y.T.; Jeong, S.U.; Shin, D.J.; Han, J.H.; Lee, C.; Seo, D.U. Factors affecting MERS-related health behaviors among male high school students. J. Korean Soc. Sch. Health 2015, 28, 150–157. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. The role of value in the social acceptance of science-technology. Int. J. Public Adm. 2015, 20, 305–322. [Google Scholar] [CrossRef]
- Rokeach, M. The Nature of Human Values; Free Press: New York, NY, USA, 1973. [Google Scholar]
- Douglas, M.; Wildavsky, A.B. Risk and Culture: An Essay on the Selection of Technical and Environmental Dangers; University of California Press: Berkeley, CA, USA, 1982. [Google Scholar]
- Wildavsky, A.; Dake, K. Theories of risk perception: Who fears what and why? Daedalus 1990, 119, 41–60. [Google Scholar]
- Brenot, J.; Bonnefous, S.; Marris, C. Testing the cultural theory of risk in France. Risk Anal. 1998, 18, 729–739. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. Cultural Construction of What? Stakeholders’ cultural bias and its effect on acceptance of a new information system. Int. J. Public Adm. 2010, 14, 71–93. [Google Scholar] [CrossRef]
- Xue, W.; Hine, D.; Loi, N.; Thorsteinsson, E.; Phillips, W. Cultural worldviews and environmental risk perceptions: A meta-analysis. J. Environ. Psychol. 2014, 40, 249–258. [Google Scholar] [CrossRef]
- Marris, C.; Langford, I.H.; O’Riordan, T. A Quantitative Test of the Cultural Theory of Risk Perceptions: Comparison with the Psychometric Paradigm. Risk Anal. 1998, 18, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Cobb, M.D.; Macoubrie, J. Public perceptions about nanotechnology: Risks, benefits and trust. J. Nanopart. Res. 2004, 6, 395–405. [Google Scholar] [CrossRef]
- Bredahl, L. Determinants of consumer attitudes and purchase intentions with regard to genetically modified foods–results of a cross-national survey. J. Consum. Policy 2000, 24, 23–61. [Google Scholar] [CrossRef]
- Mohr, P.; Harrison, A.; Wilson, C.; Baghurst, K.I.; Syrette, J. Attitude, values and socio-demographic characteristics that predict acceptance of genetic engineering and application of new technology in Australia. Biotechol. J. 2007, 2, 1169–1178. [Google Scholar] [CrossRef] [PubMed]
- Costa-Font, J.; Mossialos, E.; Rudisill, C. Optimism and the perceptions of new risks. J. Risk Res. 2009, 12, 27–41. [Google Scholar] [CrossRef]
- Fischhoff, B.; Slovic, P.; Lichtenstein, S.; Read, S.; Combs, B. How safe is safe enough? A psychometric study of attitudes towards technological risks and benefits. Policy Sci. 1978, 9, 127–152. [Google Scholar] [CrossRef]
- Siegrist, M.; Gutscher, H.; Earle, T.C. Perception of risk: The influence of general trust, and general confidence. J. Risk Res. 2006, 8, 145–156. [Google Scholar] [CrossRef]
- Hmielowski, J.D.; Feldman, L.; Myers, T.A.; Leiserowitz, A.; Maibach, E. An attack on science? Media use, trust in scientists, and perceptions of global warming. Public Underst. Sci. 2013, 23, 866–883. [Google Scholar] [CrossRef] [PubMed]
- Mayer, A.; O’Connor, S.T.; Ted, C.; Marc, G. environmental risk exposure, risk perception, political ideology and support for climate policy. Sociol. Focus 2017. [Google Scholar] [CrossRef]
- McCright, A.M.; Dunlap, R.E. Cool dudes: The denial of climate change among conservative white males in the United States. Glob. Environ. Chang. 2011, 21, 1163–1172. [Google Scholar] [CrossRef]
- Ock, H. Korea’s MERS Concerns More about Politics Than Health. 5 July 2015. Available online: http://www.koreaherald.com/view.php?ud=20150705000271 (accessed on 2 April 2018).
- Jin, J.; Song, G. Bureaucratic accountability and disaster response: Why Did the Korea Coast Guard fail in its rescue mission during the Sewol ferry accident? RHCPP 2017, 8, 220–243. [Google Scholar] [CrossRef]
- Slovic, P.; Fischhoff, B.; Lichtentstein, S. The Psychometric study of risk perception. In Contemporary Issues in Risk Analysis: The Behavioral and Social Sciences; Menkes, J., Covello, V., Mumpower, J., Eds.; Plenum: New York, NY, USA, 1986. [Google Scholar]
- Tang, C.S.K.; Wong, C. Psychosocial factors influencing the practice of preventive behaviors against the severe acute respiratory syndrome among older Chinese in Hong Kong. J. Aging Health 2005, 17, 490–506. [Google Scholar] [CrossRef] [PubMed]
- Brug, J.; Aro, A.R.; Oenema, A.; de Zwart, O.; Richardus, J.H.; Bishop, G.D. SARS risk perception, knowledge, precautions, and information sources, The Netherlands. Emerg. Infect. Dis. 2004, 10, 1486–1489. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, M.; Cvetkovich, G. Perception of hazards: The role of social trust and knowledge. Risk Anal. 2000, 20, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.Y.; Liao, Q.; Yu, E.S.; Kim, J.H.; Yoon, S.W.; Lam, W.W.T.; Fielding, R. Middle East respiratory syndrome in South Korea during 2015: Risk-related perceptions and quarantine attitudes. Am. J. Infect. Control 2016, 44, 1414–1416. [Google Scholar] [CrossRef] [PubMed]
- Gerrard, M.; Gibbons, F.X.; Bushman, B.J. Relation between perceived vulnerability to HIV and precautionary sexual behavior. Psychol. Bul. 1996, 119, 390–409. [Google Scholar] [CrossRef]
- Holling, C.S. Resilience and stability of ecological systems. Annu. Rev. Ecol. Syst. 1973, 4, 1–23. [Google Scholar] [CrossRef]
- The United Nations Office for Disaster Risk Reduction (UNISDR). Hyogo Framework for Action 2005–2015: Building the resilience of nations and communities to disasters. In Proceedings of the World Conference on Disaster Reduction, Kobe, Japan, 18–22 January 2005. [Google Scholar]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 45–51. [Google Scholar]
- Benford, R.D.; Moore, H.A.; Williams, J.A., Jr. In whose backyard? Concern about siting a nuclear waste facility. Sociol. Inq. 1993, 63, 30–47. [Google Scholar] [CrossRef]
- Huang, L.; Zhou, Y.; Han, Y.; Hammitt, J.K.; Bi, J.; Liub, Y. Effect of the Fukushima nuclear accident on the risk perception of residents near a nuclear power plant in China. Proc. Natl. Acad. Sci. USA 2013, 110, 19742–19747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, E.U.; Blais, A.R.; Betz, N.E. A Domain specific risk attitude scale: Measuring risk perceptions and risk behaviors. J. Behav. Decis. Mak. 2002, 15, 263–290. [Google Scholar] [CrossRef]
- Ko, Y. Self-perceived health versus actual cardiovascular disease risks. Jpn. J. Nurs. Sci. 2016, 13, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Sadique, M.Z.; Edmunds, W.J.; Smith, R.D.; Meerding, W.J.; de Zwart, O.; Brug, J.; Beutels, P. Precautionary behavior in response to perceived threat of pandemic influenza. Emerg. Infect. Dis. 2007, 13. [Google Scholar] [CrossRef] [PubMed]
- Dickson, D. The case for a ‘deficit model’ of science communication. Science and Development Network: London, UK, 2005. [Google Scholar]
- Coulibaly, D.; Traore, Y.; N’gattia, A.K.; Ahoussou, K.E.M.; Kangah, E.A.; Kadjo, H.A.; Cherif, D.; Dagnan, S.N. Knowledge and risk perception of the middle-east respiratory syndrome corona virus [MERS-CoV] among Ivoirian hajj pilgrims in 2013. J. Public Health Epidemiol. 2016, 8, 152–157. [Google Scholar]
- Rolison, J.J.; Hanoch, Y. Knowledge and risk perceptions of the Ebola virus in the United States. Prev. Med. Rep. 2015, 16, 262–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbate, R.; Di Giuseppe, G.; Marinelli, P.; Angelillo, I.F. Knowledge, attitudes, and practices of avian influenza, poultry workers, Italy. Emerg. Infect. Dis. 2006, 12, 1762–1765. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Tang, W. Exploring the sources of institutional trust in China: Culture, mobilization, or performance? Asian Politics Policy 2010, 3, 415–436. [Google Scholar] [CrossRef]
- Rousseau, D.M.; Sitkin, S.B.; Burt, R.S.; Camerer, C. Not so different after all: A cross-discipline view of trust. Acad. Manag. Rev. 1998, 23, 393–404. [Google Scholar] [CrossRef]
- Moy, P.; Pfau, M. With Malice toward All? The Media and Public Confidence in Democratic Institutions; Praeger: Westport, CT, USA, 2000. [Google Scholar]
- Dake, K. Technology on Trial: Orientating Dispositions toward Environmental and Health Hazards. Ph.D. Dissertation, University of California, Berkeley, CA, USA, 1990. [Google Scholar]
- Dake, K. Myths of Nature: Culture and the Social Construction of Risk. J. Soc. Issues 1992, 48, 21–37. [Google Scholar] [CrossRef]
- Jew, C.L.; Green, K.E.; Kroger, J. Development and validation of a measure of resilience. Meas. Eval. Couns. Dev. 1999, 32, 75–89. [Google Scholar]
- WHO. WHO Outbreak Communication Guidelines. Geneva, World Health Organization. Available online: http://www.who.int/csr/resources/publications/WHO_CDS_2005_28en.pdf (accessed on 13 July 2015).
- Lee, I.W. Policy PR and crisis management communication: The case of Seoul metropolitan government on MERS. Social Science Studies. J. Soc. Sci. 2016, 42, 67–104. [Google Scholar]
- Kahan, D.M.; Jenkins-Smith, H.; Braman, D. Cultural cognition of scientific consensus. J. Risk Res. 2011, 14, 147–174. [Google Scholar] [CrossRef] [Green Version]
- Song, G. Understanding public perceptions of benefits and risks of childhood vaccinations in the United States. Risk Anal. 2014, 34, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Song, G.; Silva, C.L.; Jenkins-Smith, H.C. Cultural worldview and preference for childhood vaccination policy. J. Disabil. Policy Stud. 2014, 42, 528–554. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Category | Number (%) | Mean of Perceived Risk of MERS | S.D. of Perceived Risk of MERS | |
|---|---|---|---|---|
| Education | Less than middle school diploma | 16 (1.9%) | 2.938 | 0.605 |
| High school diploma | 174 (21.7%) | 3.056 | 0.634 | |
| Undergraduate | 321 (40.0%) | 2.948 | 0.606 | |
| University graduate | 267 (33.3%) | 2.979 | 0.612 | |
| Graduate school | 25 (3.1%) | 2.920 | 0.866 | |
| Total | 803 (100.0%) | 2.981 | 0.623 | |
| Gender | Male | 387 (47.8%) | 3.019 | 0.612 |
| Female | 423 (52.2%) | 2.953 | 0.633 | |
| Total | 810 (100.0%) | 2.984 | 0.624 | |
| Age (years) | Less than 29 | 425 (52.5%) | 2.955 | 0.586 |
| 30–39 | 113 (14.0%) | 2.940 | 0.653 | |
| 40–49 | 162 (20.0%) | 2.978 | 0.641 | |
| over 50 | 109 (13.5%) | 3.155 | 0.690 | |
| Total | 809 (100.0%) | 2.984 | 0.624 | |
| Household Income(Million won) | ≤299 | 125 (19.7%) | 2.950 | 0.614 |
| 300–499 | 177 (27.9%) | 3.003 | 0.629 | |
| 500–699 | 185 (29.2%) | 2.999 | 0.589 | |
| ≥700 | 147 (23.2%) | 3.021 | 0.661 | |
| Total | 634 (100.0%) | 2.996 | 0.621 | |
| Concept | Measure | Reliability (Cronbach Alpa) |
|---|---|---|
| Perceived risk | -Compared to other diseases, MERS is the most dangerous | 0.593 |
| -MERS is a serious threat to me and my family | ||
| -The MERS is serious risk that threatens the survival of humans | ||
| -I have a high possibility of contracting MERS | ||
| -Compared to others, I am highly likely to contract MERS | ||
| Egalitarianism | -We need an overall reform for the equal distribution of wealth | 0.610 |
| -Making the society equal will solve many problems | ||
| -Equity is the best solution to all problems | ||
| Individualism | -Poverty faced by individuals is caused due to their less efforts | 0.654 |
| -A competitive society is better | ||
| -It is natural that only those who are stronger and competent survive | ||
| S&T (Science and technology) optimism | -Science and technology makes our life healthier and convenient | 0.661 |
| -Due to science and technology, the earth will not face the exhaustion of resources | ||
| -Science and technology will solve all problems | ||
| -Science and technology provides the future generation more opportunities | ||
| Trust | -I do not at all believe the experts’ explanation about MERS (R) | 0.624 |
| -I think that all of rumors related with MERS are true (R) | ||
| -I think that the rumors about MERS that are circulating on the Internet are true (R) | ||
| -I think that the facts that the government argued to be false are actually true (R) | ||
| (Perceived) Vulnerability | -Considering your health condition, to what extent do you think you will acquire the following diseases (each) within the next one or two years? (1) heart disease; (2) Tuberculosis; (3) diabetes (1 = Least likely to acquire, 5 = Most likely to acquire) | 0.873 |
| (Belief in) Resilience | -The problem of MERS will be overcome by human effort | 0.752 |
| -The problem of MERS will be solved by scientific and technological efforts | ||
| Self-Efficacy | -I can certainly overcome MERS if I acquire it | 0.398 |
| -If I acquire MERS, I can be cured more easily than others can | ||
| -MERS is a disease I can avoid if I am careful | ||
| (Perceived) Health State | -My health is good | 0.867 |
| -I keep good health | ||
| Perceived Knowledge | -For the sake of precaution against MERS, I seek much information related to it | 0.755 |
| -I have much more knowledge about MERS than others do |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Perceived Risk of MERS | 1 | ||||||||||||||
| 2. Gender | −0.053 | 1 | |||||||||||||
| 3. Age | 0.082 ** | −0.052 | 1 | ||||||||||||
| 4. Ideology (Progressive) | 0.064 | −0.004 | −0.07 * | 1 | |||||||||||
| 5. Egalitarianism | 0.087 ** | −0.03 | 0.032 | 0.077 * | 1 | ||||||||||
| 6. Individualism | 0.181 *** | −0.098 *** | 0.031 | −0.101 ** | 0.177 *** | 1 | |||||||||
| 7. S&T Optimism | 0.092 *** | −0.134 *** | 0.102 *** | −0.005 | 0.088 ** | 0.097 *** | 1 | ||||||||
| 8. Trust | −0.538 *** | 0.015 | −0.049 | −0.097 ** | −0.137 *** | −0.167 *** | −0.056 | 1 | |||||||
| 9. Perceived Vulnerability | 0.156 *** | −0.033 | 0.023 | −0.021 | 0.05 | 0.073 ** | 0.007 | −0.059 * | 1 | ||||||
| 10. Belief in Resilience | 0.059 * | −0.034 | 0.111 *** | 0.054 | 0.094 *** | 0.091 *** | 0.066 * | −0.032 | −0.156 *** | 1 | |||||
| 11. Self-efficacy | 0.154 *** | −0.021 | 0.090 * | 0.051 | 0.111 *** | 0.183 *** | 0.076 ** | −0.159 *** | −0.119 *** | 0.441 *** | 1 | ||||
| 12. Perceived Knowledge | 0.255 *** | 0.028 | 0.043 | 0.098 ** | −0.027 | 0.032 | 0.04 | −0.270 *** | 0.122 *** | 0.012 | 0.152 *** | 1 | |||
| 13. Education | −0.058 * | −0.048 | −0.454 *** | 0.087 ** | −0.057 | −0.070 ** | −0.064 * | 0.042 | 0.002 | −0.044 | −0.054 | 0.005 | 1 | ||
| 14. H. Income | 0.032 | −0.100 * | 0.022 | 0.099 ** | 0.074 * | 0.046 | 0.033 | −0.027 | −0.048 | 0.035 | 0.006 | −0.037 | 0.118 *** | 1 | |
| 15. Social Class | 0.071 * | 0.041 | 0.035 | 0.184 *** | −0.027 | 0.059 | 0.05 | −0.127 *** | −0.013 | −0.02 | 0.002 | 0.102 *** | 0.097 ** | 0.259 *** | 1 |
| 16. Perceived Health State | 0.019 | −0.066 * | 0.018 | 0.03 | 0.009 | 0.075 ** | 0.052 | −0.141 *** | −0.342 *** | 0.326 *** | 0.358 *** | 0.088 ** | −0.02 | 0.065 | 0.084 ** |
| Factor | Variables | B (Unstandardized Coefficients) | SE (Standard Error) | Beta |
|---|---|---|---|---|
| F1: Socio-demographic Factors | Constant | 4.263 | 0.39 | |
| Gender (1 = female) | −0.051 | 0.047 | −0.041 | |
| Age | 0.001 | 0.002 | 0.008 | |
| Education level | −0.002 | 0.058 | −0.002 | |
| F2: Value Factors | Egalitarianism | −0.04 | 0.033 | −0.046 |
| Individualism | 0.045 | 0.032 | 0.055 | |
| S&T Optimism | 0.043 | 0.036 | 0.044 | |
| Ideology 1 (Conservative) | 0.017 | 0.089 | 0.008 | |
| Ideology 2 (Progressive) | −0.099 | 0.063 | −0.059 | |
| F3: Perception Factors | Trust | −0.526 *** | 0.038 | −0.545 |
| Perceived Vulnerability | 0.064 ** | 0.03 | 0.085 | |
| Belief in Resilience | 0.024 | 0.033 | 0.031 | |
| Self-efficacy | 0.049 | 0.041 | 0.051 | |
| F4: Resource Factors | Household Income | 0.012 | 0.039 | 0.012 |
| Social Class | −0.003 | 0.017 | −0.007 | |
| Perceived Health State | −0.113 *** | 0.031 | −0.158 | |
| Perceived Knowledge | 0.079 *** | 0.029 | 0.109 | |
| F-Value | 17.721 *** | |||
| R2 | 0.378 | |||
| Ad. R2 | 0.356 | |||
| F1’s F-value/R2 | 0.009/3.677 ** | |||
| F2’s F-value/R2 | 0.049/6.540 *** | |||
| F3’s F-value/R2 | 0.313/91.644 *** | |||
| F4’s F-value/R2 | 0.057/6.349 *** | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kim, S. Exploring the Determinants of Perceived Risk of Middle East Respiratory Syndrome (MERS) in Korea. Int. J. Environ. Res. Public Health 2018, 15, 1168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061168
Kim S, Kim S. Exploring the Determinants of Perceived Risk of Middle East Respiratory Syndrome (MERS) in Korea. International Journal of Environmental Research and Public Health. 2018; 15(6):1168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061168
Chicago/Turabian StyleKim, Sunhee, and Seoyong Kim. 2018. "Exploring the Determinants of Perceived Risk of Middle East Respiratory Syndrome (MERS) in Korea" International Journal of Environmental Research and Public Health 15, no. 6: 1168. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061168