Association of Infant Eczema with Childhood and Adult Asthma: Analysis of Data from the 1958 Birth Cohort Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Follow-Up
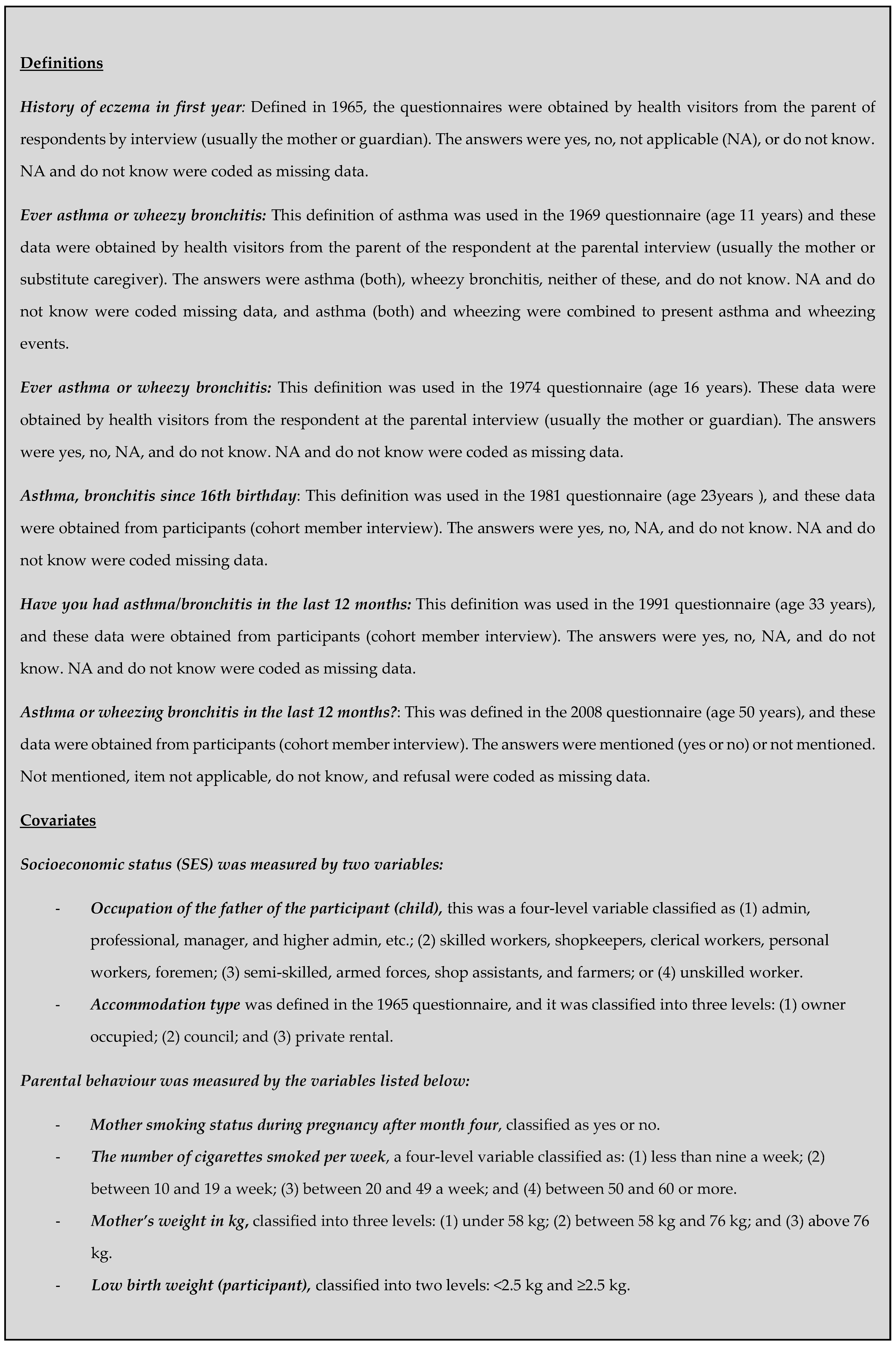
2.3. Self-Reported Outcomes
2.4. Statistical Analysis
3. Results
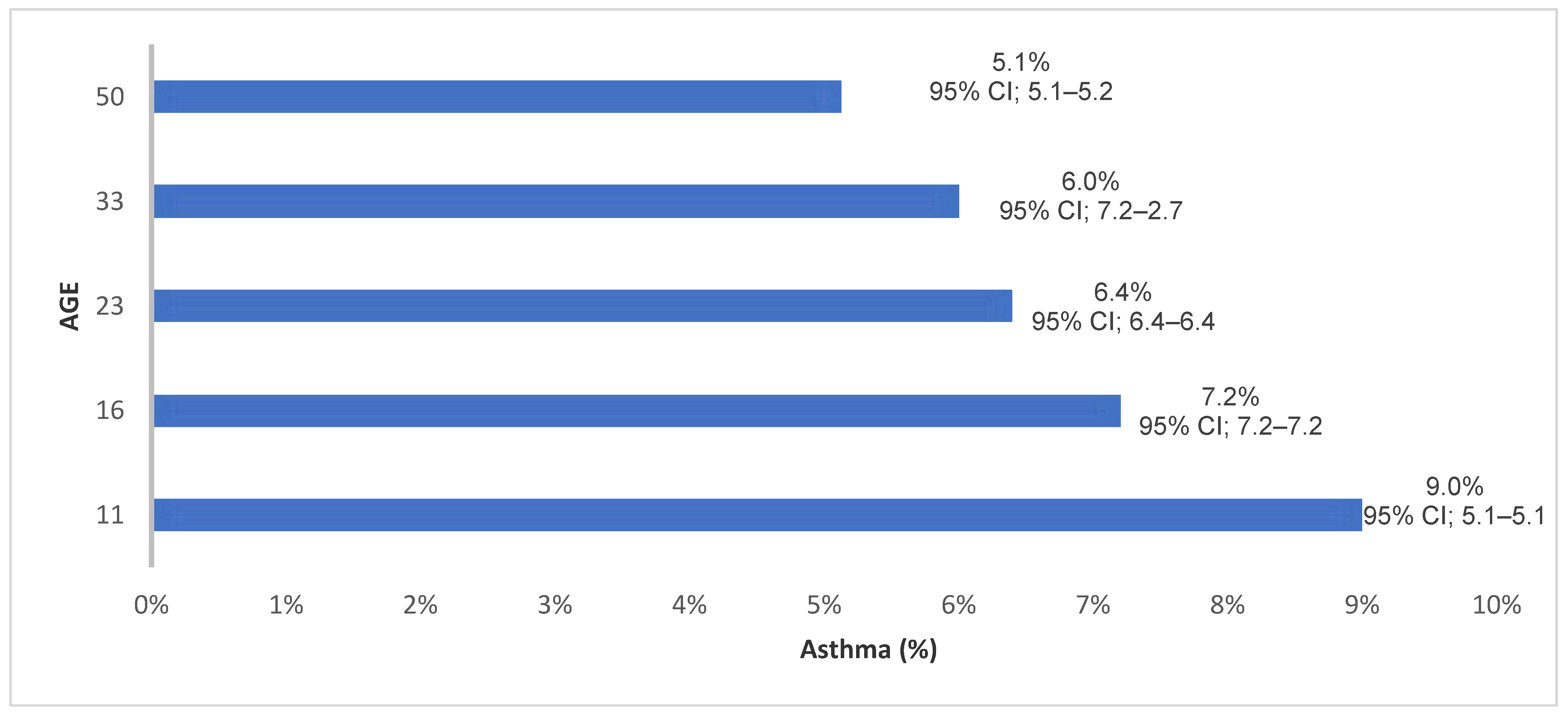
3.1. Prevalence
3.2. Eczema and Risk of Asthma (Logistic Regression Model)
3.2.1. Self-Reported and Spirometry Data
3.2.2. The Interaction between Spirometry and Total IgE (Atopic Asthma Cases)
3.2.3. Eczema and Longitudinal Risk of Asthma (the GEE Model)
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pearce, N.; Aït-Khaled, N.; Beasley, R.; Mallol, J.; Keil, U.; Mitchell, E.; Robertson, C. Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2007, 62, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Dharmage, S.; Lowe, A.; Matheson, M.; Burgess, J.; Allen, K.; Abramson, M. Atopic dermatitis and the atopic march revisited. Allergy 2014, 69, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, R.; Thornton, C.; Tyrrell, J.; Nikolaou, V.; Osborne, N. Variable risk of atopic disease due to indoor fungal exposure in NHANES 2005–2006. Clin. Exp. Allergy 2015, 45, 1566–1578. [Google Scholar] [CrossRef] [PubMed]
- Spergel, J.M.; Paller, A.S. Atopic dermatitis and the atopic march. J. Allergy Clin. Immunol. 2003, 112, S118–S127. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Keiser, E.; Linos, E.; Rotatori, R.M.; Sainani, K.; Lingala, B.; Lane, A.T.; Schneider, L.; Tang, J.Y. Eczema and Sensitization to Common Allergens in the United States: A Multiethnic, Population-Based Study. Pediat. Dermatol. 2014, 31, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Netuveli, G.; Hurwitz, B.; Levy, M.; Fletcher, M.; Barnes, G.; Durham, S.R.; Sheikh, A. Ethnic variations in UK asthma frequency, morbidity, and health-service use: A systematic review and meta-analysis. Lancet 2005, 365, 312–317. [Google Scholar] [CrossRef]
- Anandan, C.; Nurmatov, U.; Van Schayck, O.; Sheikh, A. Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy 2010, 65, 152–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beasley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef]
- Taylor-Robinson, D.C.; Williams, H.; Pearce, A.; Law, C.; Hope, S. Do early-life exposures explain why more advantaged children get eczema? Findings from the U.K. Millennium Cohort Study. Br. J. Dermatol. 2016, 174, 569–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, D.; Sjoberg, O.; Foucard, T. Development of allergies and asthma in infants and young children with atopic dermatitis—A prospective follow-up to 7 years of age. Allergy 2000, 55, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Ekbäck, M.; Tedner, M.; Devenney, I.; Oldaeus, G.; Norrman, G.; Strömberg, L.; Fälth-Magnusson, K. Severe Eczema in Infancy Can Predict Asthma Development. A Prospective Study to the Age of 10 Years. PLoS ONE 2014, 9, e99609. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.; Dharmage, S.C.; Byrnes, G.B.; Matheson, M.C. Childhood eczema and asthma incidence and persistence: A cohort study from childhood to middle age. J. Allergy Clin. Immunol. 2008, 122, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Power, C.; Elliott, J. Cohort profile: 1958 British birth cohort (National Child Development Study). Int. J. Epidemiol. 2006, 35, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Plewis, I.; Nathan, G.; Calderwood, L.; Hawkes, D. National Child Development Study and 1970 British Cohort Study Technical Report: Changes in the NCDS and BCS70 Populations and Samples over Time; Institute of Education, University of London: London, UK, 2004. [Google Scholar]
- Yang, C.; To, T.; Foty, R.; Stieb, D.; Dell, S. Verifying a questionnaire diagnosis of asthma in children using health claims data. BMC Pulm. Med. 2011, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Zuidgeest, M.G.P.; van Dijk, L.; Spreeuwenberg, P.; Smit, H.A.; Brunekreef, B.; Arets, H.G.M.; Bracke, M.; Leufkens, H.G.M. What Drives Prescribing of Asthma Medication to Children? A Multilevel Population-Based Study. Ann. Fam. Med. 2009, 7, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J.L. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Strachan, D.P.; Butland, B.K.; Anderson, H.R. Incidence and prognosis of asthma and wheezing illness from early childhood to age 33 in a national British cohort. BMJ Br. Med. J. 1996, 312, 1195–1199. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, S.; Sterne, J.; Montgomery, S.; Azima, H. Birth weight, body mass index and asthma in young adults. Thorax 1999, 54, 396–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerg, A.; Hedman, L.; Perzanowski, M.; Wennergren, G.; Lundbäck, B.; Rönmark, E. Decreased importance of environmental risk factors for childhood asthma from 1996 to 2006. Clin. Exp. Allergy 2015, 45, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, S.F.; Ulrik, C.S.; Kyvik, K.O.; Larsen, K.; Skadhauge, L.R.; Steffensen, I.; Backer, V. The Incidence of Asthma in Young Adults. Chest 2005, 127, 1928–1934. [Google Scholar] [CrossRef] [PubMed]
- Lötvall, J.; Akdis, C.A.; Bacharier, L.B.; Bjermer, L.; Casale, T.B.; Custovic, A.; Lemanske, R.F., Jr.; Wardlaw, A.J.; Wenzel, S.E.; Greenberger, P.A. Asthma endotypes: A new approach to classification of disease entities within the asthma syndrome. J. Allergy Clin. Immunol. 2011, 127, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.; Matheson, M.C.; Gurrin, L.; Burgess, J.A.; Osborne, N.; Lowe, A.J.; Morrison, S.; Mészáros, D.; Giles, G.G.; Abramson, M.J.; et al. Childhood eczema and rhinitis predict atopic but not nonatopic adult asthma: A prospective cohort study over 4 decades. J. Allergy Clin. Immunol. 2011, 127, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, R.A.; Bearman, N.; Thornton, C.R.; Husk, K.; Osborne, N.J. Indoor fungal diversity and asthma: A meta-analysis and systematic review of risk factors. J. Allergy Clin. Immunol. 2015, 135, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, R.; Thornton, C.; Osborne, N. Modifiable factors governing indoor fungal diversity and risk of asthma. Clin. Exp. Allergy 2014, 44, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Lowe, A.J.; Carlin, J.B.; Bennett, C.M.; Hosking, C.S.; Abramson, M.J.; Hill, D.J.; Dharmage, S.C. Do boys do the atopic march while girls dawdle? J. Allergy Clin. Immunol. 2008, 121, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Hanifin, J.M. Adult eczema prevalence and associations with asthma and other health and demographic factors: A US population–based study. J. Allergy Clin. Immunol. 2013, 132, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, C.; Worm, M.; Leynaert, B. Impact of gender on asthma in childhood and adolescence: A GA2LEN review. Allergy 2008, 63, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Atherton, K.; Fuller, E.; Shepherd, P.; Strachan, D.P.; Power, C. Loss and representativeness in a biomedical survey at age 45 years: 1958 British birth cohort. J. Epidemiol. Community Health 2008, 62, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Centre for Longitudinal Studies. Data Dictionary. Available online: http://www.cls.ioe.ac.uk/datadictionary/page.asp?section=000100010001000300040004&var=n1612#n1612 (accessed on 2 July 2018).
- Westman, M.; Kull, I.; Lind, T.; Melén, E.; Stjärne, P.; Toskala, E.; Wickman, M.; Bergström, A. The link between parental allergy and offspring allergic and nonallergic rhinitis. Allergy 2013, 68, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Sears, M.R. Trends in the prevalence of asthma. CHEST J. 2014, 145, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.; Keil, U.; Anderson, H.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.; Pearce, N.; Sibbald, B.; Stewart, A. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Sears, M.R.; Greene, J.M.; Willan, A.R.; Wiecek, E.M.; Taylor, D.R.; Flannery, E.M.; Cowan, J.O.; Herbison, G.P.; Silva, P.A.; Poulton, R. A longitudinal, population-based, cohort study of childhood asthma followed to adulthood. N. Engl. J. Med. 2003, 349, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Townshend, J.; Hails, S.; McKean, M. Diagnosis of asthma in children. BMJ 2007, 335, 198–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cane, R.; Ranganathan, S.; McKenzie, S. What do parents of wheezy children understand by “wheeze”? Arch. Dis. Child. 2000, 82, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, R.M.; Robalo, B.; Calado, C.; Medeiros, S.; Saianda, A.; Figueira, J.; Rodrigues, R.; Bastardo, C.; Bandeira, T. The multiple meanings of wheezing: A questionnaire survey in Portuguese for parents and health professionals. BMC Pediatr. 2011, 11, 112. [Google Scholar] [CrossRef] [PubMed]
- Michel, G.; Silverman, M.; Strippoli, M.F.; Zwahlen, M.; Brooke, A.M.; Grigg, J.; Kuehni, C.E. Parental understanding of wheeze and its impact on asthma prevalence estimates. Eur. Respir. J. 2006, 28, 1124–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lødrup Carlsen, K.C.; Roll, S.; Carlsen, K.-H.; Mowinckel, P.; Wijga, A.H.; Brunekreef, B.; Torrent, M.; Roberts, G.; Arshad, S.H.; Kull, I.; et al. Does Pet Ownership in Infancy Lead to Asthma or Allergy at School Age? Pooled Analysis of Individual Participant Data from 11 European Birth Cohorts. PLoS ONE 2012, 7, e43214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, O.; Bahmer, T.; Rabe, K.F.; von Mutius, E. Asthma transition from childhood into adulthood. Lancet Respir. Med. 2017, 5, 224–234. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Current Asthma | ||||||
|---|---|---|---|---|---|---|
| Age 11 Years n (%; 95% CI) | Age 16 Years n (%; 95% CI)) | Age 23 Years n (%; 95% CI) | Age 33 Years n (%; 95% CI) | Age 44 Years ** n (%; 95% CI) | Age 50 Years n (%; 95% CI) | |
| Eczema: n (percent) | 199 (1.7; 1.6–1.8) | 147 (1.5; 1.4–1.6) | 130 (1.2; 1.1–1.3) | 211 (2.2; 2.1–2.3) | 85 (1.0; 0.9–1.4) | 91 (1.1; 1.0–1.2) |
| Participant’s father’s occupation | ||||||
| Group I 1 | 232 (15.3; 15.2–15.5) | 185 (15.6; 15.4–15.8) | 551 (51.8; 51.2–51.4) | 381 (14.6; 14.5–14.7) | 164 (13.6; 13.4–13.8) | 111 (13.0; 12.7–13.3) |
| Group II 2 | 768 (50.7; 50.6–50.8) | 620 (52.1; 52.0–52.2) | 213 (20.0; 19.7–20.3) | 1398 (53.5; 53.4–53.6) | 660 (55.0; 54.8–55.0) | 454 (53.3; 53.4–53.6) |
| Group III 3 | 320 (21.1; 21.0–21.2) | 238 (20.0; 19.8–20.2) | 137 (12.9; 13.6–14.2) | 522 (12.0; 11.9–12.1) | 230 (19.1; 18.9–19.3) | 176 (20.7; 20.5–20.9) |
| Group IV4 | 196 (12.9; 12.7–13.1) | 147 (12.4; 12.2–12.6) | 311 (11.9; 11.8–11.1) | 149 (12.4; 12.2–12.6) | 111 (13.0; 12.9–13.1) | |
| Accommodation type at age 7 years | ||||||
| Owner occupied | 656 (53.4; 53.3–53.5) | 514 (53.9; 53.8–54.0) | 459 (53.0; 52.9–53.1) | 1058 (51.1; 51.1–51.2) | 517 (52.7; 52.6–52.8) | 345 (50.3; 50.2–50.4) |
| Council housing and privately rented | 573 (46.6; 46.5–46.7) | 439 (46.1; 46.0–46.2) | 407 (47.0; 46.9–47.1) | 1012 (48.9; 48.8–49.9) | 464 (47.3; 47.2–47.4) | 341 (49.7; 49.6–49.8) |
| Sex | ||||||
| Male | 979 (58.9; 59.8–59.0) | 799 (60.2; 60.1–60.3) | 509 (43.1; 43.0–43.2) | 1408 (48.7; 48.7–48.8) | 672 (49.7; 49.6–49.8) | 397 (41.7; 41.6–41.8) |
| Female | 684 (41.1; 41.0–41.2) | 528 (39.8; 39.7–39.9) | 672 (56.9; 56.8–57.0) | 1482 (51.3; 51.2:51.4) | 680 (50.3; 50.2–50.4) | 555 (58.3; 58.2–58.4) |
| Mother smoked after month four of pregnancy? | ||||||
| Abstain | 1043 (66.3; 66.1–66.4) | 844 (68.0; 67.9–68.1) | 728 (65.6; 65.5–65.7) | 1739 (63.8; 63.7–63.9) | 796 (63.4; 63.3–63.5) | 552 (62.0; 61.9–62.1) |
| Smoke | 530 (33.7; 33.6–33.8) | 397 (32.0; 31.9–32.1) | 381 (34.4; 34.3–34.5) | 989 (36.3); 36.2–36.4) | 460 (36.6; 36.5–36.7) | 338 (38.0; 37.9–38.1) |
| Mother’s weight | ||||||
| Under 57 kg | 1103 (71.0; 70.9–71.1) | 875 (71.3; 71.2–71.4) | 788 (71.8;70.7–71.9) | 1927 (71.4; 71.4–71.5) | 904 (73.1; 73.0–73.1) | 631 (71.7; 71.5–71.9) |
| Between 57 kg and under 76 kg | 354 (22.8; 22.7–22.9) | 283 (23.1; 23.0–23.2) | 245 (22.3;22.1–22.5) | 631 (23.4; 23.1–23.7) | 257 (20.8; 20.6–21.0) | 207 (23.5; 22.5–24.5) |
| From 176 kg to above | 96 (6.2; 5.9–6.5) | 70 (5.7; 5.4–6.0) | 64 (5.8; 5.4–6.2) | 141 (5.2; 5.1–5.2) | 75 (6.1; 5.8–6.4) | 42 (4.8; 4.7–4.8) |
| No. of cigarettes parents smoked per week | ||||||
| None | 799 (67.5; 6.7–6.8) | 710 (65.3; 65.2–65.4) | 534 (60.9; 60.7–60.9) | 1,201 (55.4; 55.3–55.4) | 620 (60.5; ;60.4–60.6) | 439 (61.0; 60.7–61.3) |
| ≤29 a week | 185 (15.6; 15.4;15.8) | 179 (16.5; 16.3–16.7) | 176 (20.0; 19.8–20.2) | 469 (21.6; 21.5–21.7) | 195 (19.0; 18.8–19.2) | 157 (21.8; 21.5–22.1) |
| >29 a week | 199 (16.8; 16.6–17.0) | 199 (18.3; 18.1–18.5) | 169 (19.2; 19.0–19.4) | 497 (22.9; 22.7–23.1) | 210 (20.5; 20.3–20.7) | 124 (17.2; 16.8–17.6) |
| Birth weight (kg) | ||||||
| ≤2.5 | 141 (8.5; 8.3–8.7) | 113 (8.5; 8.3–8.7) | 116 (9.8; 9.5–10.1) | 266 (9.2; 9.1–9.3) | 102 (7.5; 7.2–7.8) | 95 (10.0; 9.0–10.0) |
| > 2.5 | 1522 (91.5; 91.4–91.6) | 1214 (91.5; 91.4–91.6) | 1065 (90.2; 90.1–90.3) | 2624 (90.8; 90.7–90.9) | 1250 (92.5; 92.4–92.5) | 857 (90.0; 89.0–90.0) |
| Eczema | Model 1 (Unadjusted Model) | Model 4 (Adjusted Model) | ||
|---|---|---|---|---|
| All Data | Excluding Smokers | All Data | Excluding Smokers | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age 11 years | 3.76 (3.14–4.49) | ----- | 4.17 (3.30–5.29) | ----- |
| Age 16 years | 3.69 (3.00–4.52) | 3.77 (3.03–4.69) | 4.11 (3.20–5.28) | 4.12 (3.15–5.38) |
| Age 23 years | 3.12 (2.53–3.84) | 3.47 (2.65–4.56) | 3.49 (2.68–4.55) | 4.08 (2.89–5.74) |
| Age 33 years | 2.32 (1.92–2.79) | 2.59 (2.10–3.21) | 2.43 (1.91–3.09) | 2.71 (2.06–3.56) |
| Age 50 years | 2.55 (2.00–3.25) | 2.83 (2.15–3.73) | 3.06 (2.25–4.16) | 3.07 (2.17–4.34) |
| Eczema | Model 1 (Unadjusted Model) | Model 4 (Adjusted Model) | ||
|---|---|---|---|---|
| All Data | Excluding Smokers | All Data | Excluding Smokers | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age 44 years * Spirometry data | 1.36 (1.06–1.75) | 1.69 (1.27–2.25) | 1.29 (0.91–1.79) | 1.61 (1.09–2.32) |
| New Cases Examined at | Number of Cases in Whom Asthma Was Still Present (%) | |||
|---|---|---|---|---|
| Age 16 Years | Age 23 Years | Age 33 Years | Age 50 Years | |
| Age 11 years | 701/1327 (53%) | 367/1181 (31%) | 603/2890 (21%) | 229/952 (24%) |
| Age 16 years | ----- | 364/1181 (31%) | 562/2890 (20%) | 206/952 (22%) |
| Age 23 years | ----- | ----- | 651/2890 (23%) | 307/952 (32%) |
| Age 33 years | ----- | ----- | ----- | 532/952 (56%) |
| Age 50 years | ----- | ----- | ----- | ----- |
| Eczema | Model 1 (Unadjusted Model) | Model 4 (Adjusted Model) | ||
|---|---|---|---|---|
| All Data | Excluding Smokers | All Data | Excluding Smokers | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| All data * | 2.91 (2.64, 3.22) | 3.18 (2.87, 3.48) | 3.19 (2.80, 3.62) | 3.43 (3.01, 3.99) |
| Sex: | ||||
| Male | 4.04 (3.52,4.36) | 4.29 (3.72,4.83) | 3.97 (3.31,4.75) | 4.12 (3.65,4.99) |
| Female | 2.05 (1.77,2.39) | 2.23 (1.99,2.51) | 2.58 (2.13,3.12) | 2.78 (2.38,3.42) |
| Accommodation type | ||||
| Owner occupied | 3.25 (2.84,3.73) | 3.45 (3.04, 3.99) | 3.39 (2.88,3.98) | 3.56 (3.01,4.02) |
| Council rented | 2.56 (2.14, 3.06) | 2.89 (2.41, 3.49) | 2.84 (2.28, 3.53) | 3.28 (2.63, 3.99) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abo-Zaid, G.; Sharpe, R.A.; Fleming, L.E.; Depledge, M.; Osborne, N.J. Association of Infant Eczema with Childhood and Adult Asthma: Analysis of Data from the 1958 Birth Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 1415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071415
Abo-Zaid G, Sharpe RA, Fleming LE, Depledge M, Osborne NJ. Association of Infant Eczema with Childhood and Adult Asthma: Analysis of Data from the 1958 Birth Cohort Study. International Journal of Environmental Research and Public Health. 2018; 15(7):1415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071415
Chicago/Turabian StyleAbo-Zaid, Ghada, Richard A. Sharpe, Lora E. Fleming, Michael Depledge, and Nicholas J. Osborne. 2018. "Association of Infant Eczema with Childhood and Adult Asthma: Analysis of Data from the 1958 Birth Cohort Study" International Journal of Environmental Research and Public Health 15, no. 7: 1415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071415