Poor Dietary Habits in Bullied Adolescents: The Moderating Effects of Diet on Depression

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Measures
2.2.1. Bullying Victimization
2.2.2. Dietary Habits
2.2.3. Depression
2.3. Data Analysis
3. Results
3.1. Relationship between Bullying, Dietary Habits, and Depression
3.2. Differences between High and Low Victimised Adolescents in Dietary Habits
3.3. Prediction Ability of Bullying and Dietary Habits on Depression
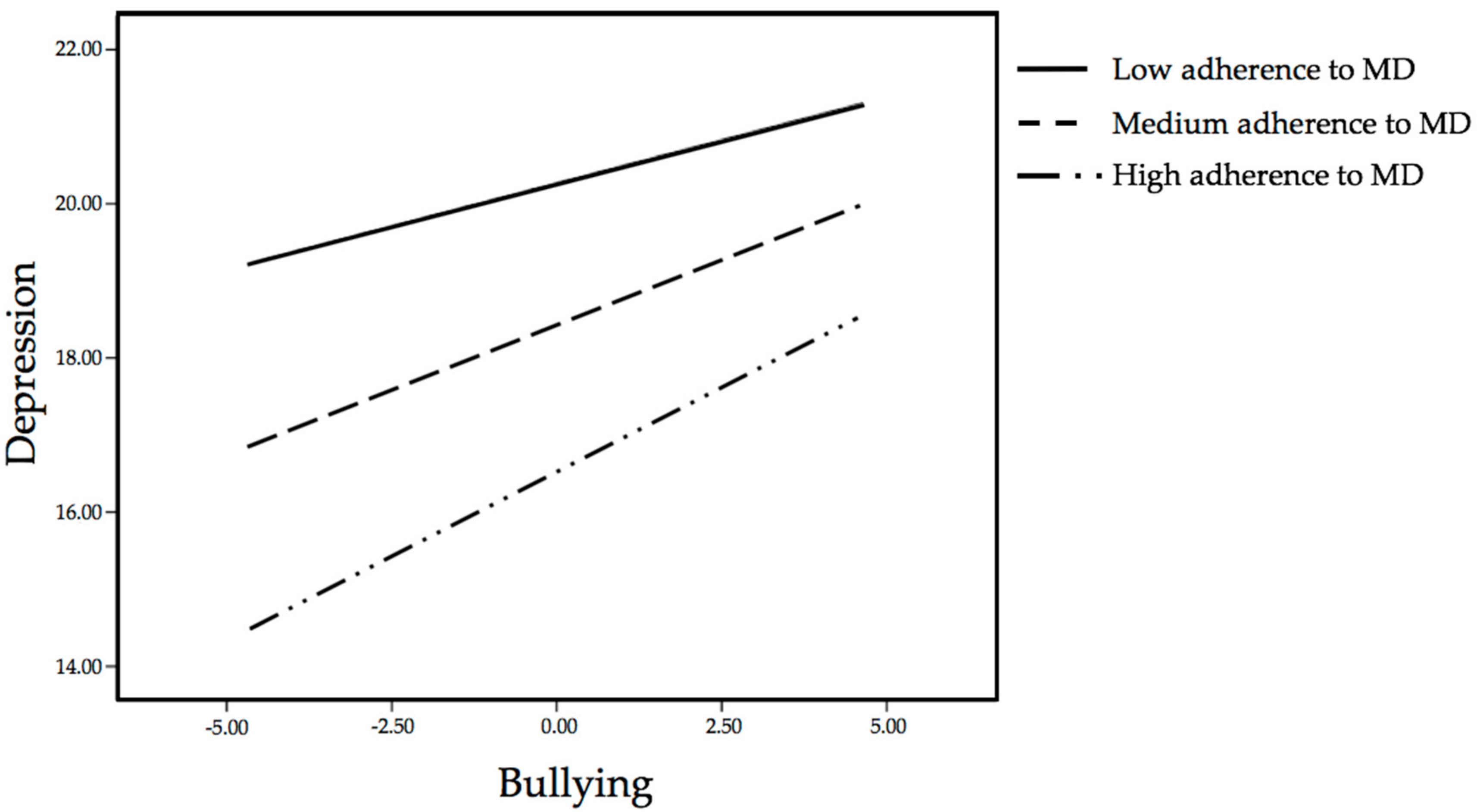
3.4. Moderation Effects of Dietary Habits on the Relationship between Bullying and Depression.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Arseneault, L. Annual Research Review: The persistent and pervasive impact of being bullied in childhood and adolescence: Implications for policy and practice. J. Child Psychol. Psychiatry 2018, 59, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Zych, I.; Farrington, D.P.; Llorent, V.J.; Ttofi, M.M. School Bullying in Different Countries: Prevalence, Risk Factors, and Short-Term Outcomes. In Protecting Children against Bullying and Its Consequences; Springer International Publishing: Basel, Switzerland, 2017; pp. 5–22. [Google Scholar]
- Modecki, K.L.; Minchin, J.; Harbaugh, A.G.; Guerra, N.G.; Runions, K.C. Bullying prevalence across contexts: A meta-analysis measuring cyber and traditional bullying. J. Adolesc. Health 2014, 55, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Ford, R.; King, T.; Priest, N.; Kavanagh, A. Bullying and mental health and suicidal behaviour among 14-to 15-year-olds in a representative sample of Australian children. Aust. N. Z. J. Psychiatry 2017, 51, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Holt, M.K.; Vivolo-Kantor, A.M.; Polanin, J.R.; Holland, K.M.; DeGue, S.; Matjasko, J.L.; Wolfe, M.; Reid, G. Bullying and suicidal ideation and behaviors: A meta-analysis. Pediatrics 2015, 135, E496–E509. [Google Scholar] [CrossRef] [PubMed]
- Zarate-Garza, P.P.; Biggs, B.K.; Croarkin, P.; Morath, B.; Leffler, J.; Cuellar-Barboza, A.; Tye, S.J. How well do we understand the long-term health implications of childhood bullying? Harv. Rev. Psychiatry 2017, 25, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Fantaguzzi, C.; Allen, E.; Miners, A.; Christie, D.; Opondo, C.; Sadique, Z.; Fletcher, A.; Grieve, R.; Bonell, C.; Viner, R.M.; et al. Health-related quality of life associated with bullying and aggression: A cross-sectional study in English secondary schools. Eur. J. Health Econ. 2018, 19, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Frisén, A.; Bjarnelind, S. Health-related quality of life and bullying in adolescence. Acta Paediatr. 2010, 99, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Kaltiala-Heino, R.; Fröjd, S. Correlation between bullying and clinical depression in adolescent patients. Adolesc. Health Med. Ther. 2011, 2, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Wang, L.H.; Zhang, G.D.; Liang, X.B.; Li, J.; Zimmerman, M.A.; Wang, J.L. The promotive effects of peer support and active coping on the relationship between bullying victimization and depression among Chinese boarding students. Psychiatry Res. 2017, 256, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Baiden, P.; Stewart, S.L.; Fallon, B. The mediating effect of depressive symptoms on the relationship between bullying victimization and non-suicidal self-injury among adolescents: Findings from community and inpatient mental health settings in Ontario, Canada. Psychiatry Res. 2017, 255, 238–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodish, T.; Herres, J.; Shearer, A.; Atte, T.; Fein, J. Diamond, G. Bullying, depression, and suicide risk in a pediatric primary care sample. Crisis 2016, 37, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Sampasa-Kanyinga, H.; Roumeliotis, P.; Farrow, C.V.; Shi, Y.F. Breakfast skipping is associated with cyberbullying and school bullying victimization. A school-based cross-sectional study. Appetite 2014, 79, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampasa-Kanyinga, H.; Willmore, J. Relationships between bullying victimization psychological distress and breakfast skipping among boys and girls. Appetite 2015, 89, 41–46. [Google Scholar] [CrossRef] [PubMed]
- García-Toro, M.; Vicens-Pons, E.; Gili, M.; Roca, M.; Serrano-Ripoll, M.J.; Vives, M.; Leiva, A.; Yáñez, A.M.; Bennasar-Veny, M.; Oliván-Blázquez, B. Obesity, metabolic syndrome and Mediterranean diet: Impact on depression outcome. J. Affect. Disord. 2016, 194, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Sergentanis, T.N.; Panagiotakos, D.B.; Sergentanis, I.N.; Kosti, R.; Scarmeas, N. Mediterranean diet, stroke, cognitive impairment, and depression: A meta-analysis. Ann. Neurol. 2013, 74, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Caballo, V.E.; Calderero, M.; Arias, B.; Salazar, I.C.; Irurtia, M.J. Desarrollo y validación de una nueva medida de autoinforme para evaluar el acoso escolar (BULLYING). Behav. Psychol. 2012, 20, 625–647. (In Spanish) [Google Scholar]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; García-Closas, R.; Ribas, L.; Pérez-Rodrigo, C.; Aranceta, J. Food patterns of Spanish schoolchildren and adolescents: The enKid Study. Public Health Nutr. 2001, 4, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Štefan, L.; Prosoli, R.; Juranko, D.; Čule, M.; Milinović, I.; Novak, D.; Sporiš, G. The reliability of the mediterranean diet quality index (KIDMED) questionnaire. Nutrients 2017, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Mendez, M.A.; Ribas-Barba, L.; Covas, M.I.; Serra-Majem, L. Mediterranean diet and waist circumference in a representative national sample of young Spaniards. Int. J. Pediatr. Obes. 2010, 5, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Herrero, J.; Meneses, J. Short Web-based versions of the perceived stress (PSS) and Center for Epidemiological Studies-Depression (CESD) Scales: A comparison to pencil and paper responses among Internet users. Comput. Hum. Behav. 2006, 22, 830–846. [Google Scholar] [CrossRef]
- Carleton, R.N.; Thibodeau, M.A.; Teale, M.J.; Welch, P.G.; Abrams, M.P.; Robinson, T.; Asmundson, G.J. The center for epidemiologic studies depression scale: A review with a theoretical and empirical examination of item content and factor structure. PLoS ONE 2013, 8, e58067. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- De Vriendt, T.; Clays, E.; Huybrechts, I.; De Bourdeaudhuij, I.; Moreno, L.A.; Patterson, E.; Molnár, D.; Mesana, M.I.; Beghin, L.; Widhalm, K.; et al. European adolescents’ level of perceived stress is inversely related to their diet quality: The healthy lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 108, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Hou, F.; Xu, S.; Zhao, Y.; Lu, Q.; Zhang, S.; Zu, P.; Sun, Y.; Su, P.; Tao, F. Effects of emotional symptoms and life stress on eating behaviors among adolescents. Appetite 2013, 68, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, M.; Wardle, J.; Steggles, N.; Simon, A.E.; Croker, H.; Jarvis, M.J. Stress and dietary practices in adolescents. Health Psychol. 2003, 22, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, emotional eating behaviour and dietary patterns in children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michels, N.; Sioen, I.; Ruige, J.; De Henauw, S. Children's psychosocial stress and emotional eating: A role for leptin? Int. J. Eat. Disord. 2017, 50, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Dao, T.K.; Kerbs, J.J.; Rollin, S.A.; Potts, I.; Gutierrez, R.; Choi, K.; Creason, A.H.; Wolf, A.; Prevatt, F. The association between bullying dynamics and psychological distress. J. Adolesc. Health 2006, 39, 277–282. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Stress, adaptation, and disease: Allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Stressed or stressed out: What is the difference? J. Psychiatry Neurosci. 2005, 30, 315–318. [Google Scholar] [PubMed]
- Juster, R.P.; McEwen, B.S.; Lupien, S.J. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci. Biobehav. Rev. 2010, 35, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Kusano, Y.; Crews, D.E.; Iwamoto, A.; Sone, Y.; Aoyagi, K.; Maeda, T.; Leahy, R. Allostatic load differs by sex and diet, but not age in older Japanese from the Goto Islands. Ann. Hum. Biol. 2016, 43, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Bhupathiraju, S.; Tucker, K.L. Higher adherence to a diet score based on American Heart Association recommendations is associated with lower odds of allostatic load and metabolic syndrome in Puerto Rican adults. J. Nutr. 2013, 143, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Molendijk, M.; Molero, P.; Sánchez-Pedreño, F.O.; Van der Does, W.; Martínez-González, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Khalid, S.; Williams, C.M.; Reynolds, S.A. Is there an association between diet and depression in children and adolescents? A systematic review. Br. J. Nutr. 2016, 116, 2097–2108. [Google Scholar] [CrossRef] [PubMed]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship between diet and mental health in children and adolescents: A systematic review. Am. J. Public Health 2014, 104, e31–e42. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Jones, D.P.; Goldberg, J.; Ziegler, T.R.; Bostick, R.M.; Wilson, P.W.; Manatunga, A.K.; Shallenberger, L.; Jones, L.; Vaccarino, V. Association between adherence to the Mediterranean diet and oxidative stress. Am. J. Clin. Nutr. 2008, 88, 1364–1370. [Google Scholar] [PubMed]
- Holt, E.M.; Steffen, L.M.; Moran, A.; Basu, S.; Steinberger, J.; Ross, J.A.; Hong, C.-P.; Sinaiko, A.R. Fruit and vegetable consumption and its relation to markers of inflammation and oxidative stress in adolescents. J. Am. Diet. Assoc. 2009, 109, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.L.D.; Oliveira, W.A.; Mello, F.C.M.; Andrade, L.S.; Bazon, M.R.; Silva, M.A.I. Anti-bullying interventions in schools: A systematic literature review. Cien Saude Colet 2017, 22, 2329–2340. [Google Scholar] [CrossRef] [PubMed]
- Cantone, E.; Piras, A.P.; Vellante, M.; Preti, A.; Daníelsdóttir, S.; D’Aloja, E.; Lesinskiene, S.; Angermeyer, M.C.; Carta, M.G.; Bhugra, D. Interventions on bullying and cyberbullying in schools: A systematic review. Clin. Pract. Epidemiol. Ment. Health 2015, 11, 58–76. [Google Scholar] [PubMed]


{kind=link}
| Bullying | Depression | |
|---|---|---|
| Fruit or fruit juice daily | −0.723 ** | −0.594 ** |
| Second serving of fruit daily | −0.541 ** | −0.547 ** |
| Fresh or cooked vegetables daily | −0.478 ** | −0.477 ** |
| Fresh or cooked vegetables >1/day | −0.504 ** | −0.542 ** |
| Regular fish consumption (at least 2–3/week) | −0.476 ** | −0.434 ** |
| Fast-food (hamburger) restaurant >1 week | 0.082 | 0.104 * |
| Pulses >1/week | −0.279 ** | −0.320 ** |
| Pasta or rice almost daily (≥5/week) | −0.289 ** | −0.287 ** |
| Cereal or cereal product for breakfast | −0.471 ** | −0.452 ** |
| Regular nut consumption (at least 2–3/week) | −0.269 ** | −0.251 ** |
| Use of olive oil at home | −0.377 ** | −0.260 ** |
| No breakfast | 0.123 ** | 0.076 |
| Dairy product for breakfast | −0.628 ** | −0.575 ** |
| Commercially baked goods or pastries for breakfast | 0.014 | −0.052 |
| Two yogurts and/or 40 g cheese daily | −0.347 ** | −0.349 ** |
| Sweets and candy several times a day | 0.072 | 0.095 * |
| High Victimization n = 235 | Low Victimization n = 292 | |||
|---|---|---|---|---|
| Fruit or fruit juice daily | No | 105 | 6 | χ² = 142.297, p = 0.0001 |
| Yes | 130 | 286 | ||
| Second serving of fruit daily | No | 182 | 78 | χ² = 134.086, p = 0.0001 |
| Yes | 53 | 214 | ||
| Fresh or cooked vegetables daily | No | 133 | 40 | χ² = 108.660, p = 0.0001 |
| Yes | 102 | 252 | ||
| Fresh or cooked vegetables >1/day | No | 206 | 100 | χ² = 152.560, p = 0.0001 |
| Yes | 29 | 192 | ||
| Regular fish consumption (at least 2–3/week) | No | 144 | 56 | χ² = 97.998, p = 0.0001 |
| Yes | 91 | 236 | ||
| Fast food (hamburger) restaurant >1 week | No | 152 | 216 | χ² = 5.336, p = 0.021 |
| Yes | 83 | 76 | ||
| Pulses >1/week | No | 118 | 63 | χ² = 47.356, p = 0.0001 |
| Yes | 117 | 229 | ||
| Pasta or rice almost daily (≥5/week) | No | 133 | 83 | χ² = 42.722, p = 0.0001 |
| Yes | 102 | 209 | ||
| Cereal or cereal product for breakfast | No | 147 | 63 | χ² = 91.218, p = 0.0001 |
| Yes | 88 | 229 | ||
| Regular nut consumption (at least 2–3/week) | No | 147 | 105 | χ² = 36.907, p = 0.0001 |
| Yes | 88 | 187 | ||
| Use of olive oil at home | No | 29 | 5 | χ² = 24.369, p = 0.0001 |
| Yes | 206 | 287 | ||
| No breakfast | No | 179 | 208 | χ² = 1.627, p = 0.202 |
| Yes | 56 | 84 | ||
| Dairy product for breakfast | No | 139 | 36 | χ² = 128.691, p = 0.0001 |
| Yes | 96 | 256 | ||
| Commercially baked goods or pastries for breakfast | No | 152 | 216 | χ² = 5.336, p = 0.021 |
| Yes | 83 | 76 | ||
| Two yogurts and/or 40 g cheese daily | No | 185 | 128 | χ² = 65.713, p = 0.0001 |
| Yes | 50 | 164 | ||
| Sweets and candy several times a day | No | 194 | 257 | χ² = 3.146, p = 0.076 |
| Yes | 41 | 35 | ||
| Low adherence to Mediterranean Diet (MD) | 103 | 0 | χ² = 350.725, p = 0.0001 | |
| Medium adherence to MD | 132 | 65 | ||
| High Adherence to MD | 0 | 227 | ||
| Model 1 | β | R2 | ΔR2 |
|---|---|---|---|
| Age | −0.012 | ||
| Sex | −0.061 | ||
| F(2, 526) = 0.972, p = 0.379 | 0.000 | 0.004 | |
| Model 2 | β | R2 | ΔR2 |
| Age | 0.035 | ||
| Sex | 0.001 | ||
| Bullying | 0.834 ** | ||
| F(3, 526) = 394.983, p = 0.0001 | 0.692 | 0.690 ** | |
| Model 3 | β | R2 | ΔR2 |
| Age | 0.004 | ||
| Sex | 0.001 | ||
| Bullying | 0.118 * | ||
| Fruit or fruit juice daily | −0.106 ** | ||
| Second serving of fruit daily | −0.148 ** | ||
| Fresh or cooked vegetables daily | −0.126 ** | ||
| Fresh or cooked vegetables >1/day | −0.173 ** | ||
| Regular fish consumption (at least 2–3/week) | −0.157 ** | ||
| Fast food (hamburger) restaurant >1 week | 0.115 ** | ||
| Pulses >1/week | −0.153 ** | ||
| Pasta or rice almost daily (≥5/week) | −0.142 ** | ||
| Cereal or cereal product for breakfast | −0.145 ** | ||
| Regular nut consumption (at least 2–3/week) | −0.119 ** | ||
| Use of olive oil at home | −0.036 | ||
| No breakfast | 0.132 ** | ||
| Dairy product for breakfast | −0.140 ** | ||
| Commercially baked goods or pastries for breakfast | 0.143 ** | ||
| Two yogurts and/or 40 g cheese daily | −0.150 ** | ||
| Sweets and candy several times a day | 0.095 ** | ||
| F(19, 526) = 113.735, p = 0.0001 | 0.803 | 0.116 ** |
| B | SE | t | p | 95% CI | |
|---|---|---|---|---|---|
| Bullying | 0.332 | 0.067 | 4.930 | 0.00001 | [0.200, 0.464] |
| Dietary habits (Adherence to MD) | −0.689 | 0.084 | −8.151 | 0.00001 | [−0.855, −0.523] |
| Bullying x Dietary habits (Adherence to MD) | 0.040 | 0.008 | 4.546 | 0.00001 | [0.022, 0.057] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albaladejo-Blázquez, N.; Ferrer-Cascales, R.; Ruiz-Robledillo, N.; Sánchez-Sansegundo, M.; Clement-Carbonell, V.; Zaragoza-Martí, A. Poor Dietary Habits in Bullied Adolescents: The Moderating Effects of Diet on Depression. Int. J. Environ. Res. Public Health 2018, 15, 1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081569
Albaladejo-Blázquez N, Ferrer-Cascales R, Ruiz-Robledillo N, Sánchez-Sansegundo M, Clement-Carbonell V, Zaragoza-Martí A. Poor Dietary Habits in Bullied Adolescents: The Moderating Effects of Diet on Depression. International Journal of Environmental Research and Public Health. 2018; 15(8):1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081569
Chicago/Turabian StyleAlbaladejo-Blázquez, Natalia, Rosario Ferrer-Cascales, Nicolás Ruiz-Robledillo, Miriam Sánchez-Sansegundo, Violeta Clement-Carbonell, and Ana Zaragoza-Martí. 2018. "Poor Dietary Habits in Bullied Adolescents: The Moderating Effects of Diet on Depression" International Journal of Environmental Research and Public Health 15, no. 8: 1569. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15081569