A Daily Cup of Tea or Coffee May Keep You Moving: Association between Tea and Coffee Consumption and Physical Activity


Abstract
:1. Introduction
2. Materials and Methods
2.1. Caffeinated Drinks Intake Assessment
2.2. Physical Activity
2.3. Tiredness and Energy Levels
2.4. Health Variables
2.5. Statistical Analysis
3. Results
3.1. Coffee or Tea Intake and Physical Activity
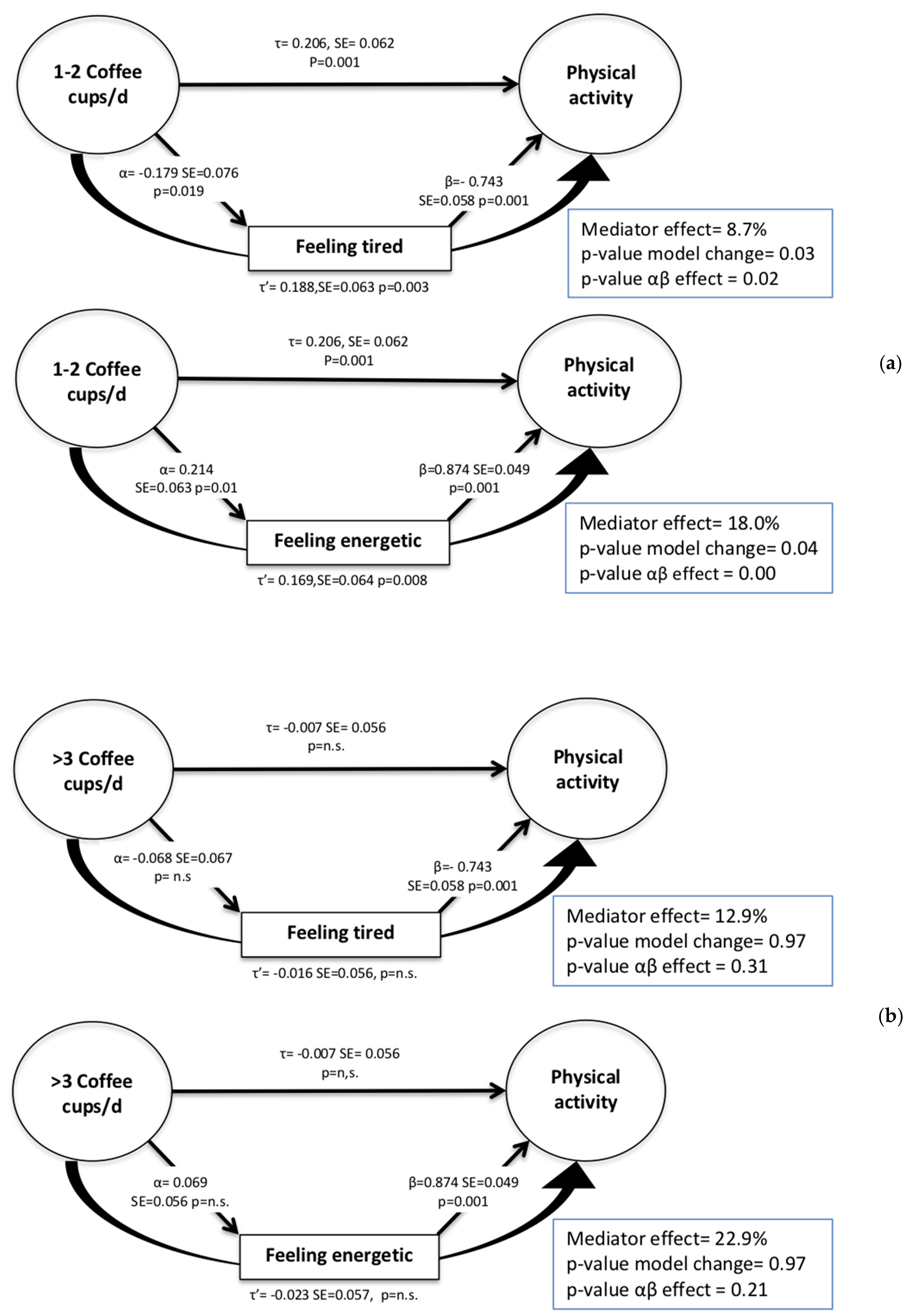
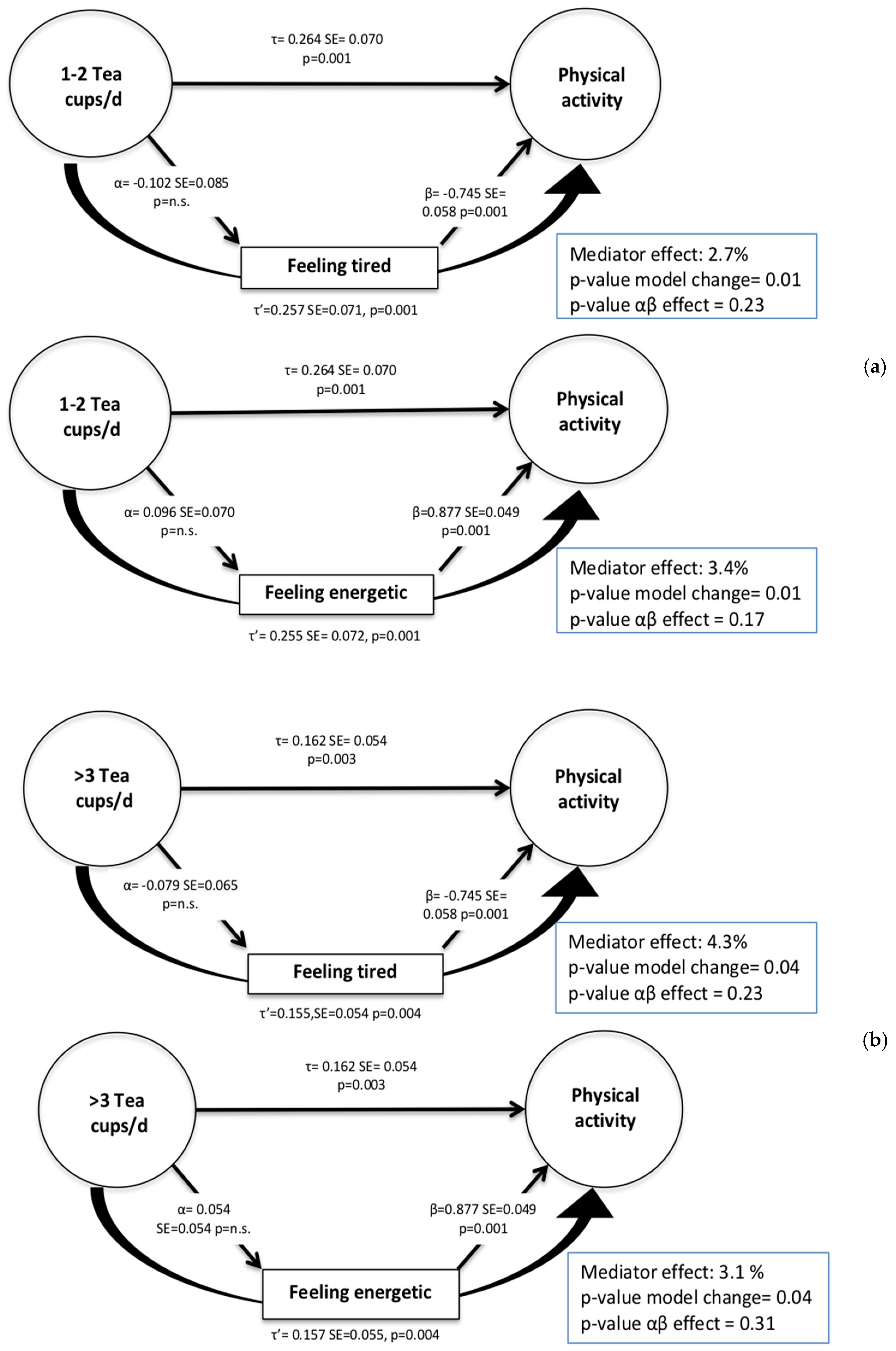
3.2. Mediation Analysis for the Relationship between Coffee and Tea Intake and PA
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- He, X.Z.; Baker, D.W. Body mass index, physical activity, and the risk of decline in overall health and physical functioning in late middle age. Am. J. Public Health 2004, 94, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Gebel, K.; Ding, D.; Chey, T.; Stamatakis, E.; Brown, W.J.; Bauman, A.E. Effect of moderate to vigorous physical activity on all-cause mortality in middle-aged and older Australians. JAMA Intern. Med. 2015, 175, 970–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichert, F.F.; Barros, A.J.; Domingues, M.R.; Hallal, P.C. The role of perceived personal barriers to engagement in leisure-time physical activity. Am. J. Public Health 2007, 97, 515–519. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, J.A.; Benitez, J. Clinically significant pharmacokinetic interactions between dietary caffeine and medications. Clin. Pharmacokinet. 2000, 39, 127–153. [Google Scholar] [CrossRef] [PubMed]
- Heckman, M.A.; Weil, J.; Gonzalez de Mejia, E. Caffeine (1, 3, 7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M.; Feskens, E.J. Coffee consumption and risk of type 2 diabetes mellitus. Lancet 2002, 360, 1477–1478. [Google Scholar] [CrossRef]
- Zhang, Y.; Lee, E.T.; Cowan, L.D.; Fabsitz, R.R.; Howard, B.V. Coffee consumption and the incidence of type 2 diabetes in men and women with normal glucose tolerance: The Strong Heart Study. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, M.S.; Sultan, M.T. Coffee and its consumption: Benefits and risks. Crit. Rev. Food Sci. Nutr. 2011, 51, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A. Are we dependent upon coffee and caffeine? A review on human and animal data. Neurosci. Biobehav. Rev. 1999, 23, 563–576. [Google Scholar] [CrossRef]
- Burke, L.; Desbrow, B.; Spriet, L. Caffeine for Sports Performance; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Schrader, P.; Panek, L.M.; Temple, J.L. Acute and chronic caffeine administration increases physical activity in sedentary adults. Nutr. Res. 2013, 33, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Doherty, M.; Smith, P.M. Effects of caffeine ingestion on rating of perceived exertion during and after exercise: A meta-analysis. Scand. J. Med. Sci. Sports 2005, 15, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Gliottoni, R.C.; Meyers, J.R.; Arngrimsson, S.A.; Broglio, S.P.; Motl, R.W. Effect of caffeine on quadriceps muscle pain during acute cycling exercise in low versus high caffeine consumers. Int. J. Sport Nutr. Exerc. Metab. 2009, 19, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, R.E.; Kates, A. Can the Affective Response to Exercise Predict Future Motives and Physical Activity Behavior? A Systematic Review of Published Evidence. Ann. Behav. Med. 2015, 49, 715–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, W.; Bryson, L.; Byles, J.; Dobson, A.; Manderson, L.; Schofield, M.; Williams, G. Women’s health Australia: Establishment of the Australian longitudinal study on women’s health. J. Women Health 1996, 5, 467–472. [Google Scholar] [CrossRef]
- Hodge, A.; Patterson, A.J.; Brown, W.J.; Ireland, P.; Giles, G. The Anti Cancer Council of Victoria FFQ: Relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust. N. Z. J. Public Health 2000, 24, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.; Milligan, G.; Hunt, A. NUTTAB95 Nutrient Data Table for Use in Australia; Australian Government Publishing Service: Canberra, Australia, 1995.
- Kaaks, R.; Slimani, N.; Riboli, E. Pilot phase studies on the accuracy of dietary intake measurements in the EPIC project: Overall evaluation of results. Int. J. Epidemiol. 1997, 26 (Suppl. 1), S26–S36. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.C.; Knight, C.A.; Hockenberry, J.; Teplansky, R.; Hartman, T.J. Beverage caffeine intakes in the US. Food Chem. Toxicol. 2014, 63, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.; Bauman, A.; Bull, F.; Burton, N. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years); Australian Government Department of Health: Canberra, Australia, 2012.
- Brown, W.J.; Burton, N.W.; Marshall, A.L.; Miller, Y.D. Reliability and validity of a modified self-administered version of the Active Australia physical activity survey in a sample of mid-age women. Aust. N. Z. J. Public Health 2008, 32, 535–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Puetz, T.W. Chronic physical activity and feelings of energy and fatigue. Med. Sci. Sports Exerc. 2005, 37, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.J.; Mishra, G.; Lee, C.; Bauman, A. Leisure time physical activity in Australian women: Relationship with well being and symptoms. Res. Q. Exerc. Sport 2000, 71, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Puetz, T.W. Physical activity and feelings of energy and fatigue: Epidemiological evidence. Sports Med. 2006, 36, 767–780. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef] [PubMed]
- Eskelinen, M.H.; Ngandu, T.; Tuomilehto, J.; Soininen, H.; Kivipelto, M. Midlife coffee and tea drinking and the risk of late-life dementia: A population-based CAIDE study. J. Alzheimers Dis. Rep. 2009, 16, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Desbrow, B.; Hughes, R.; Leveritt, M.; Scheelings, P. An examination of consumer exposure to caffeine from retail coffee outlets. Food Chem. Toxicol. 2007, 45, 1588–1592. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Categories | n (%) |
|---|---|---|
| BMI | Underweight | 94 (1.2) |
| Normal | 2995 (39.5) | |
| Overweight | 2655 (35.0) | |
| Obese | 1836 (24.2) | |
| Education level | No formal qualification | 958 (12.6) |
| School certificate | 2397 (31.6) | |
| Higher school certificate | 1263 (16.7) | |
| Trade/apprenticeship | 258 (3.4) | |
| Certificate/diploma | 1388 (18.3) | |
| University degree or higher | 1316 (16.4) | |
| Smoking | Never | 4799 (63.3) |
| Ex-smoker | 2277 (30.0) | |
| Smoker | 504 (4.7) | |
| A lot of energy in the past four weeks | Never | 380 (5.0) |
| A little | 2465 (32.5) | |
| Most of the time | 4735 (62.5) | |
| Tiredness in the past four weeks | Never | 556 (7.3) |
| A little | 5515 (72.8) | |
| Most of the Time | 1509 (19.9) | |
| Hypertension | Yes | 2533 (33.4) |
| No | 5047 (66.6) | |
| Diabetes | Yes | 583 (7.7) |
| No | 6997 (92.3) | |
| Cardiovascular disease | Yes | 405 (5.3) |
| No | 7175 (94.7) | |
| Coffee intake (cups/day) | <1 cup | 2360 (31.1) |
| 1–2 cups | 2064 (27.2) | |
| >3 cups | 3156 (41.6) | |
| Tea intake (cups/day) | <1 cup | 2306 (30.4) |
| 1–2 cups | 1389 (18.3) | |
| >3 cups | 3885 (51.3) | |
| Meeting PA guidelines | (>500 MET.min/week) | 4642 (61.2) |
| Variables | Category | Coffee (Cups/Day) | Tea (Cups/Day) | ||||
|---|---|---|---|---|---|---|---|
| <1 | 1–2 | ≥3 | <1 | 1–2 | ≥3 | ||
| Level of MVPA Coffee χ2 = 21.39, p < 0.01 Tea χ2 = 21.28, p < 0.01 | None | 15.2 | 12.1 | 14.7 | 16.2 | 11.6 | 13.8 |
| Low | 24.8 | 23.1 | 25.5 | 25.8 | 24.0 | 24.2 | |
| Moderate | 22.4 | 22.0 | 21.8 | 20.9 | 22.8 | 22.5 | |
| High | 37.6 | 42.8 | 38.0 | 37.3 | 41.5 | 39.5 | |
| Meeting MVPA guidelines Coffee χ2 = 15.38, p < 0.01 Tea χ2 = 16.11, p < 0.01 | Yes | 60.0 | 64.8 | 59.8 | 58.1 | 64.4 | 62.0 |
| Tiredness Coffee χ2 = 5.60, p = 0.05 Tea χ2 = 10.85, p = 0.03 | Most of the time | 21.1 | 18.3 | 17.5 | 21.0 | 17.1 | 21.2 |
| Feeling energetic Coffee χ2 = 13.84, p < 0.01 Tea χ2 = 3.29, p = 0.51 | Most of the time | 60.4 | 65.4 | 64.7 | 61.2 | 64.2 | 61.7 |
| Cups/day (Reference: <1 Cup/d) | Coffee | Tea | ||||
|---|---|---|---|---|---|---|
| Crude | Model 1 | Model 2 a | Crude | Model 1 | Model 2 b | |
| 1–2 cups | 1.23 (1.09–1.39) | 1.17 (1.04–1.32) | 1.14 (1.00–1.30) | 1.30 (1.14–1.49) | 1.26 (1.08–1.46) | 1.23 (1.05–1.40) |
| ≥3 cups | 0.99 (0.89–1.10) | 1.03 (0.92–1.16) | 0.98 (0.87–1.10) | 1.18 (1.06–1.30) | 1.13 (1.01–1.26) | 1.09 (0.98–1.22) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torquati, L.; Peeters, G.; Brown, W.J.; Skinner, T.L. A Daily Cup of Tea or Coffee May Keep You Moving: Association between Tea and Coffee Consumption and Physical Activity. Int. J. Environ. Res. Public Health 2018, 15, 1812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091812
Torquati L, Peeters G, Brown WJ, Skinner TL. A Daily Cup of Tea or Coffee May Keep You Moving: Association between Tea and Coffee Consumption and Physical Activity. International Journal of Environmental Research and Public Health. 2018; 15(9):1812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091812
Chicago/Turabian StyleTorquati, Luciana, Geeske Peeters, Wendy J. Brown, and Tina L. Skinner. 2018. "A Daily Cup of Tea or Coffee May Keep You Moving: Association between Tea and Coffee Consumption and Physical Activity" International Journal of Environmental Research and Public Health 15, no. 9: 1812. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15091812