Cancer Health Literacy and Willingness to Participate in Cancer Research and Donate Bio-Specimens

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
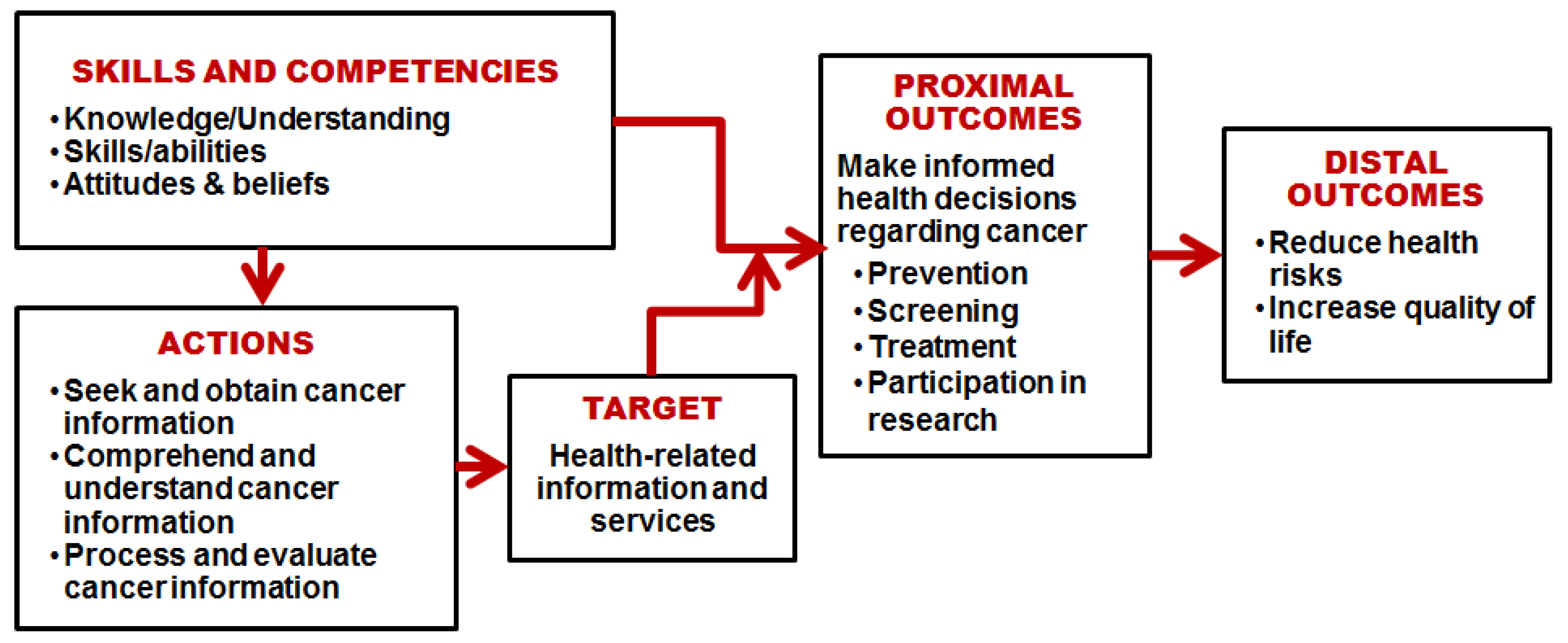
2.1. Conceptual Framework
2.2. Participants and Data Collection Procedures
2.3. Instruments
2.4. Statistical Analysis
3. Results
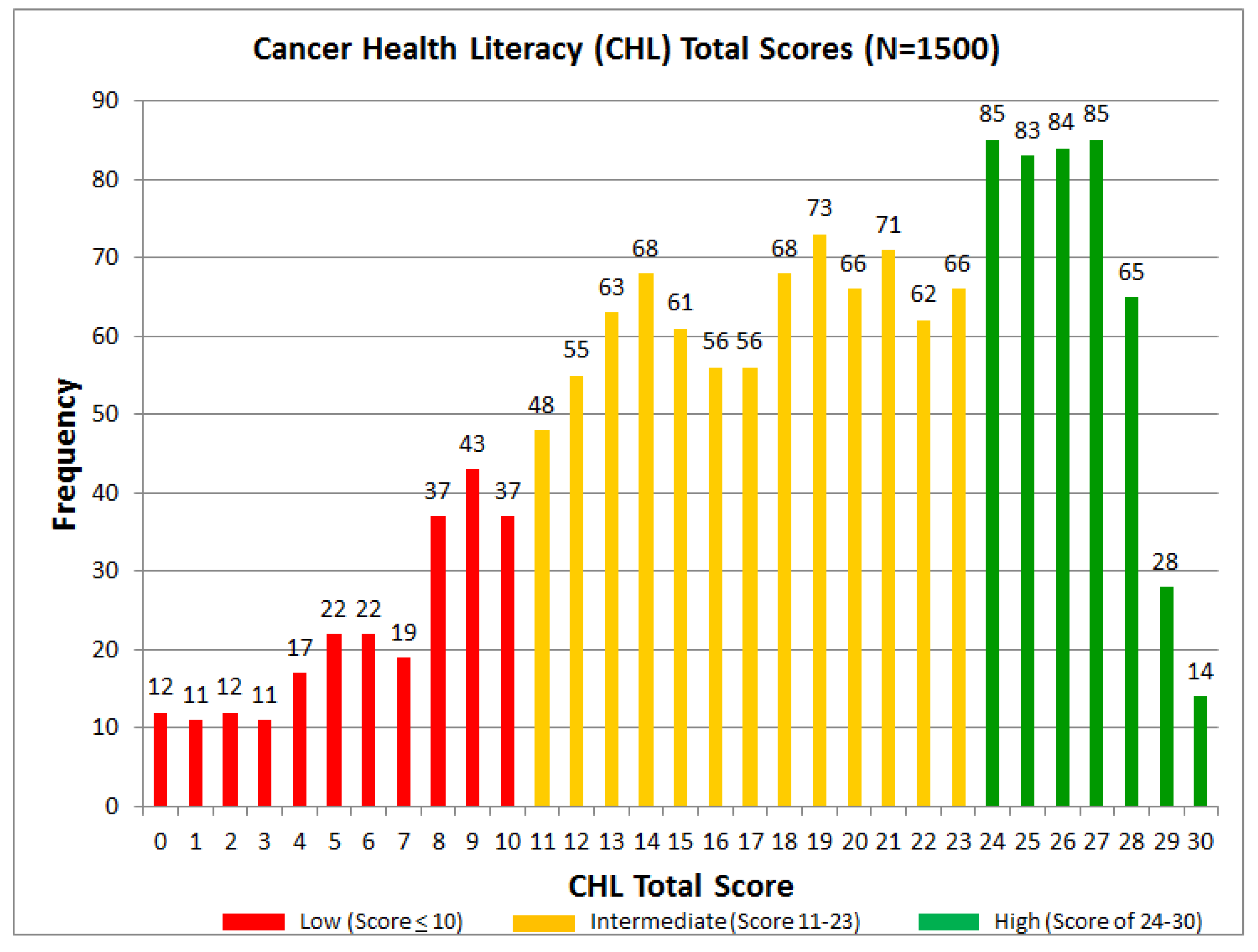
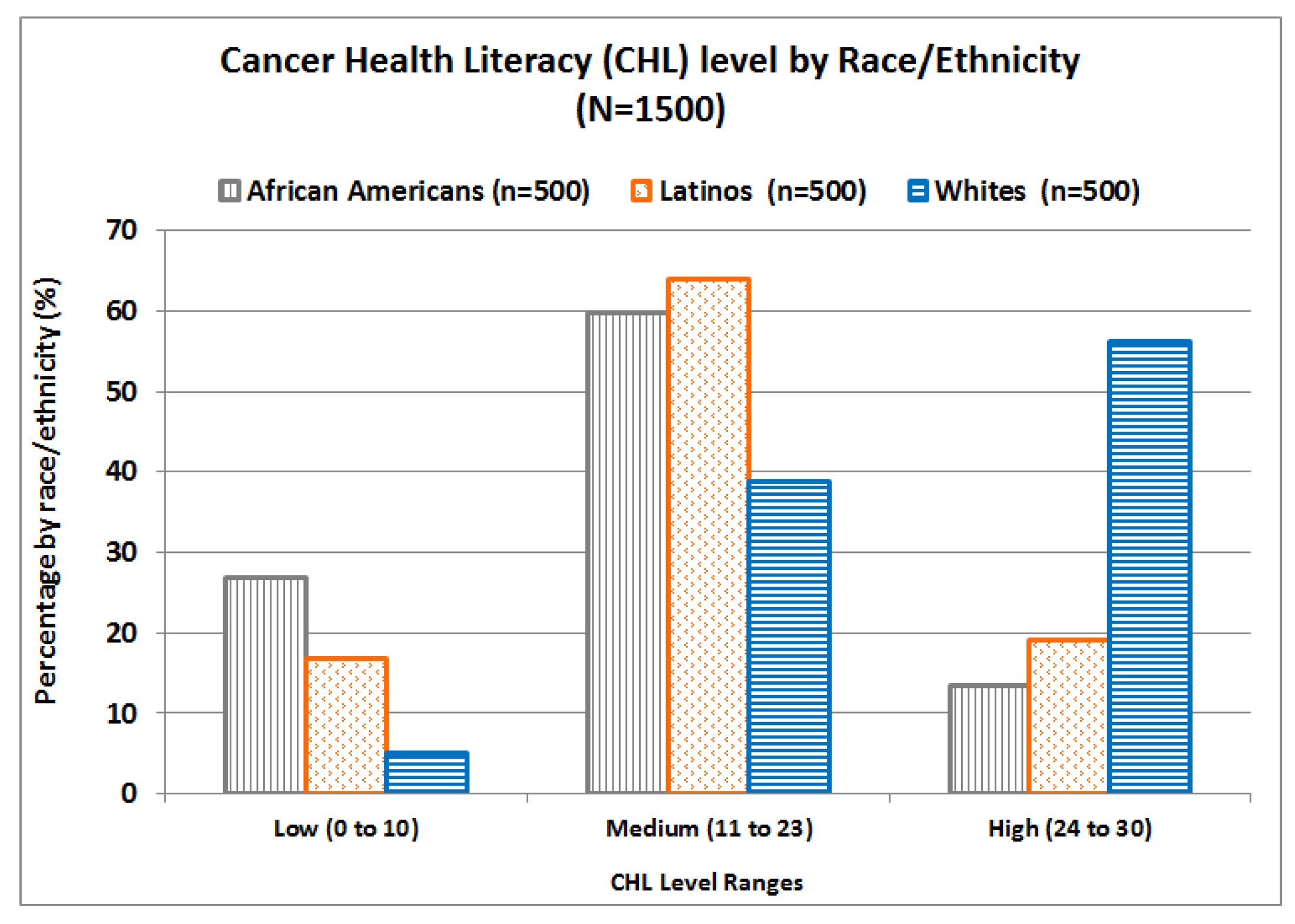
3.1. Cancer Health Literacy (CHL) Scores
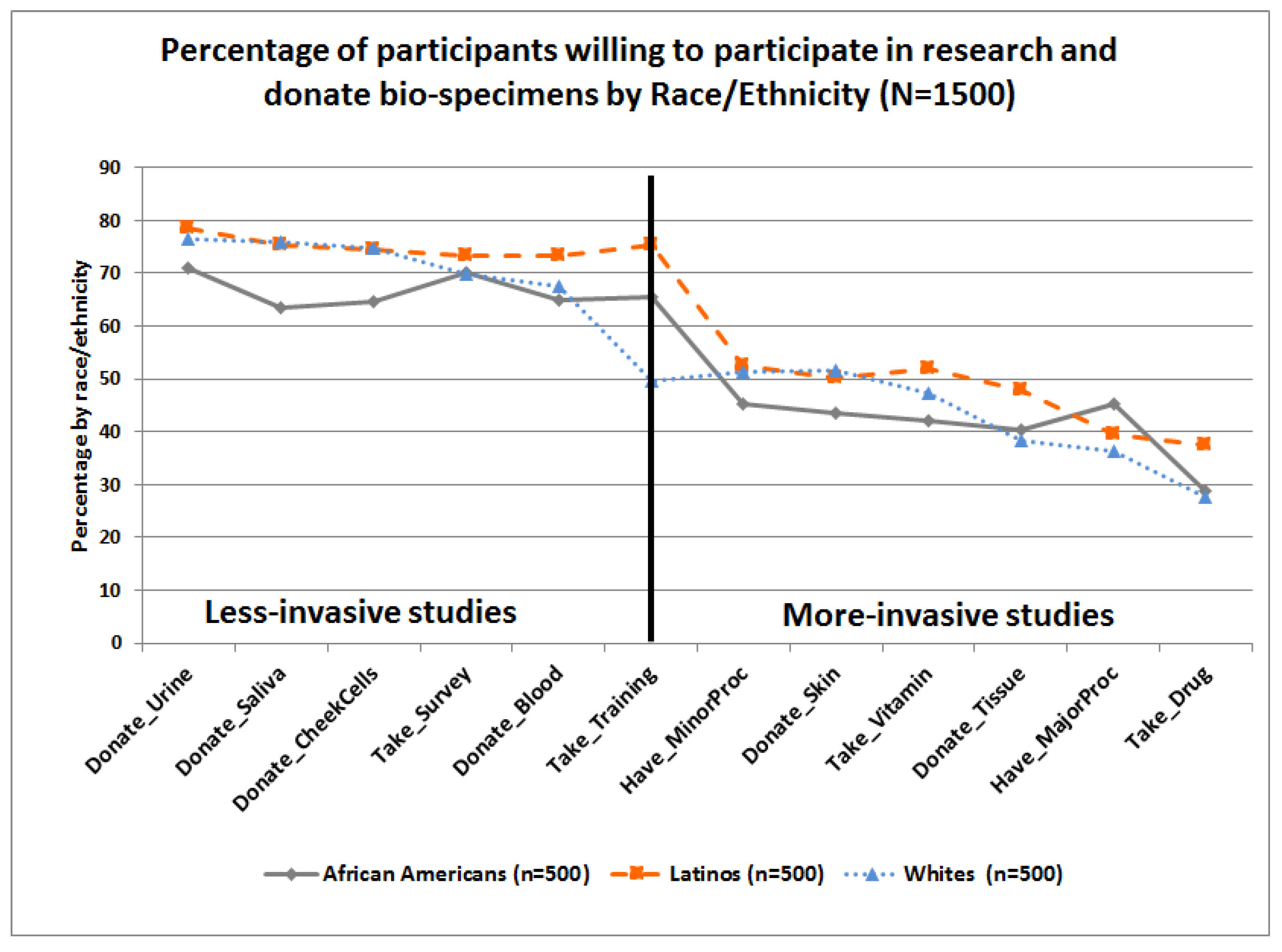
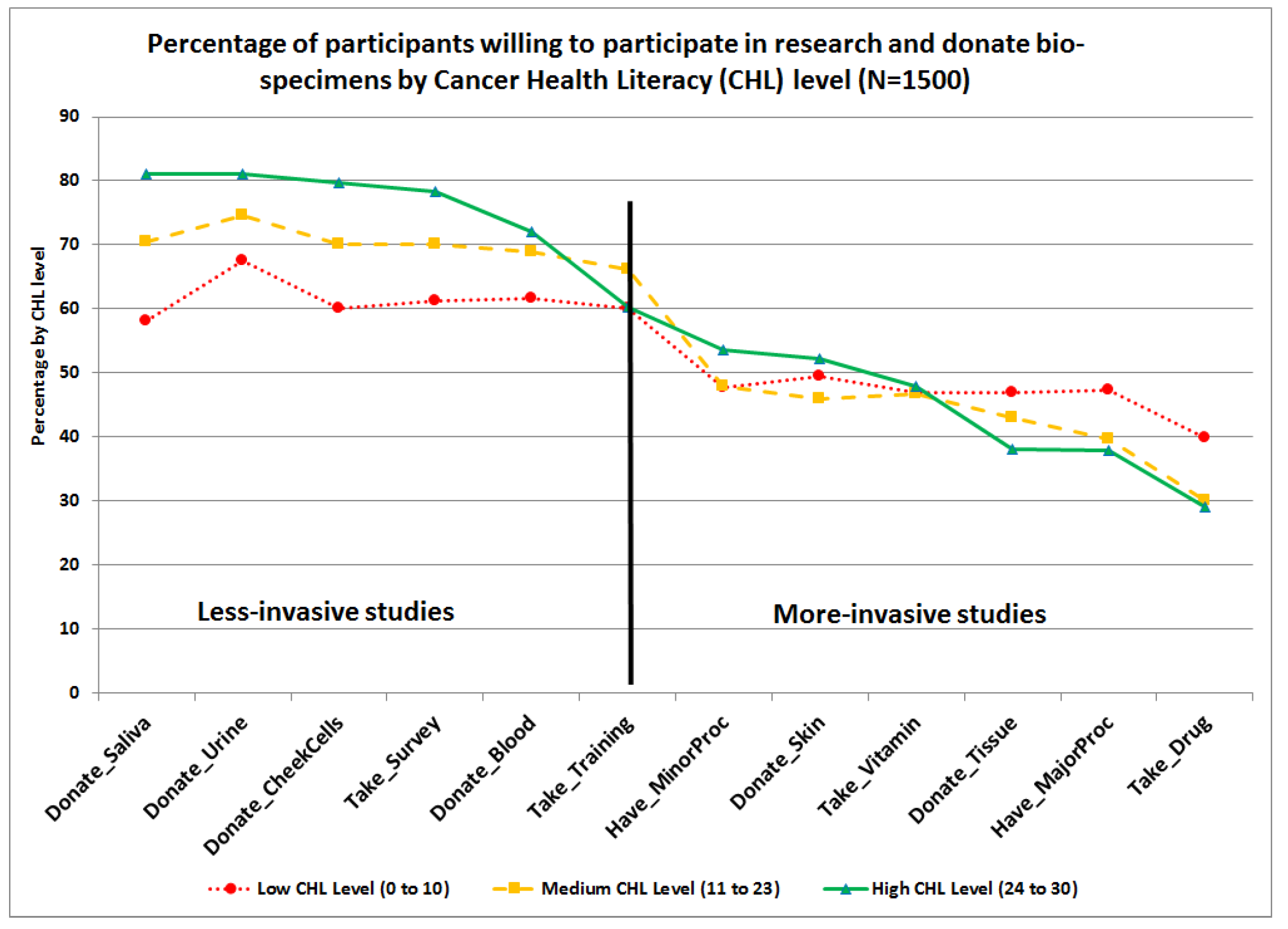
3.2. Willingness to Participate in Research and Donate Bio-Specimens (WPRDB) Scores
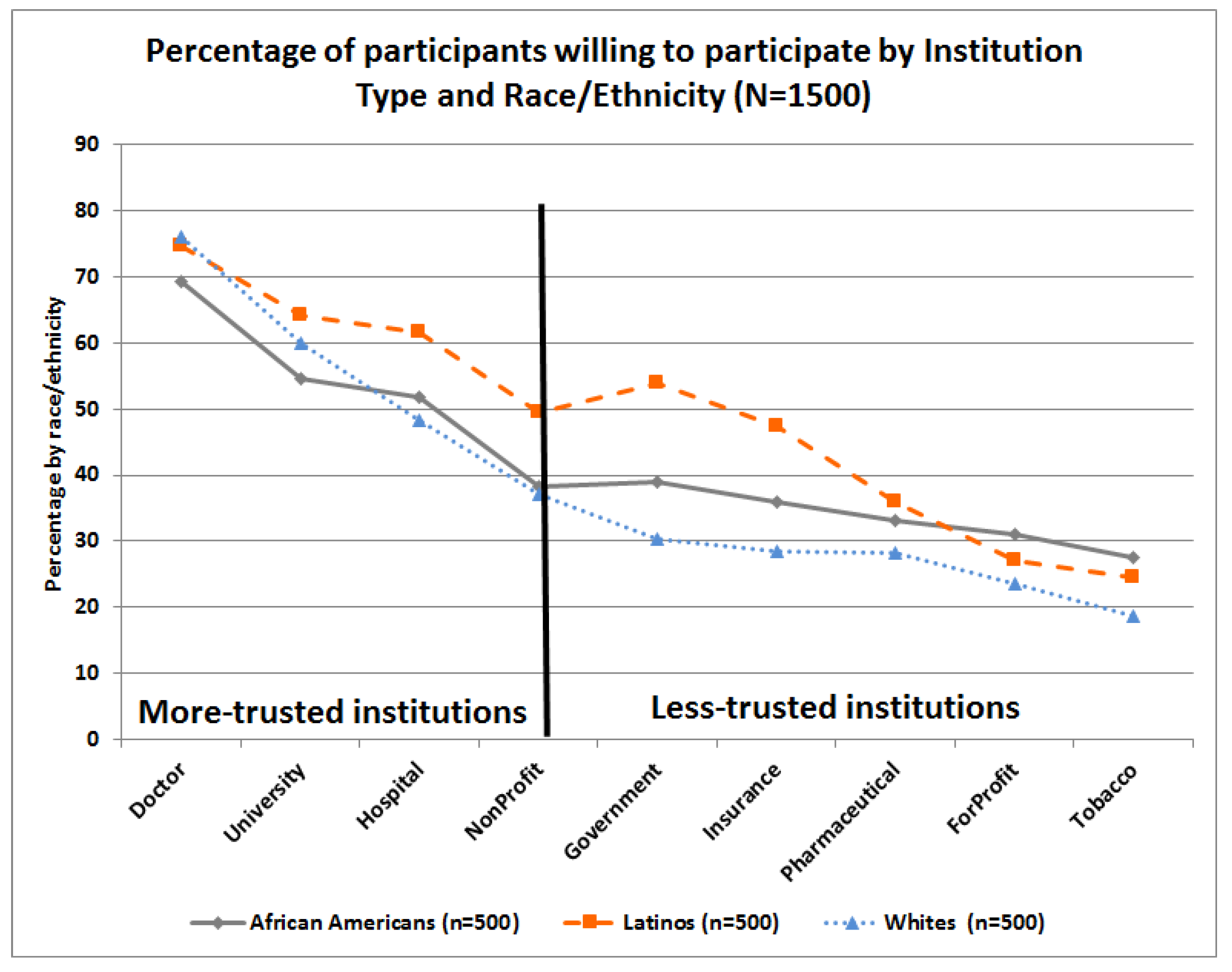
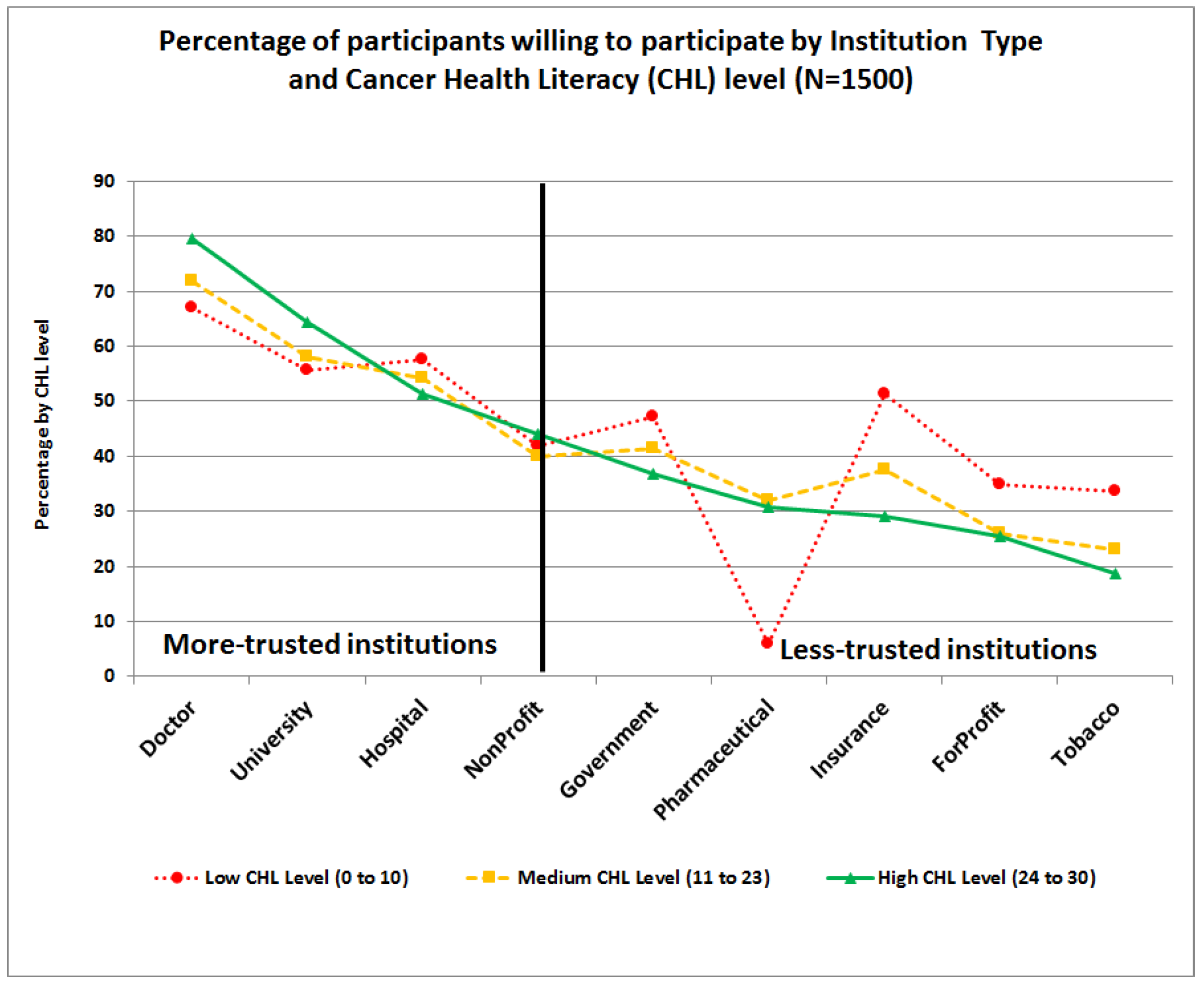
3.3. Willingness to Participate by Institution Type (WILL:Institution)
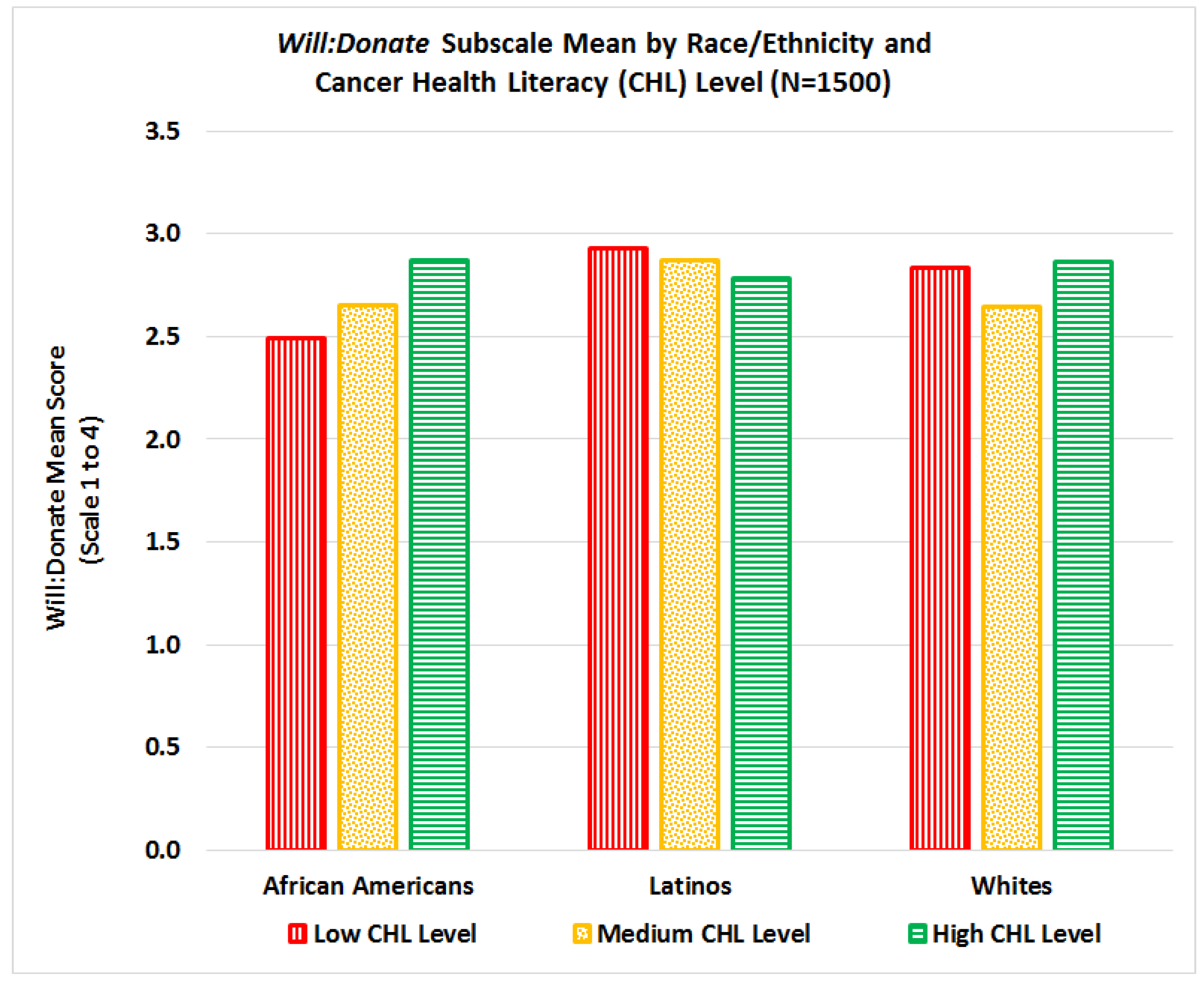
3.4. Interactions Between Cancer Health Literacy, Race/Ethnicity, and Gender on Total WPRDB Scale
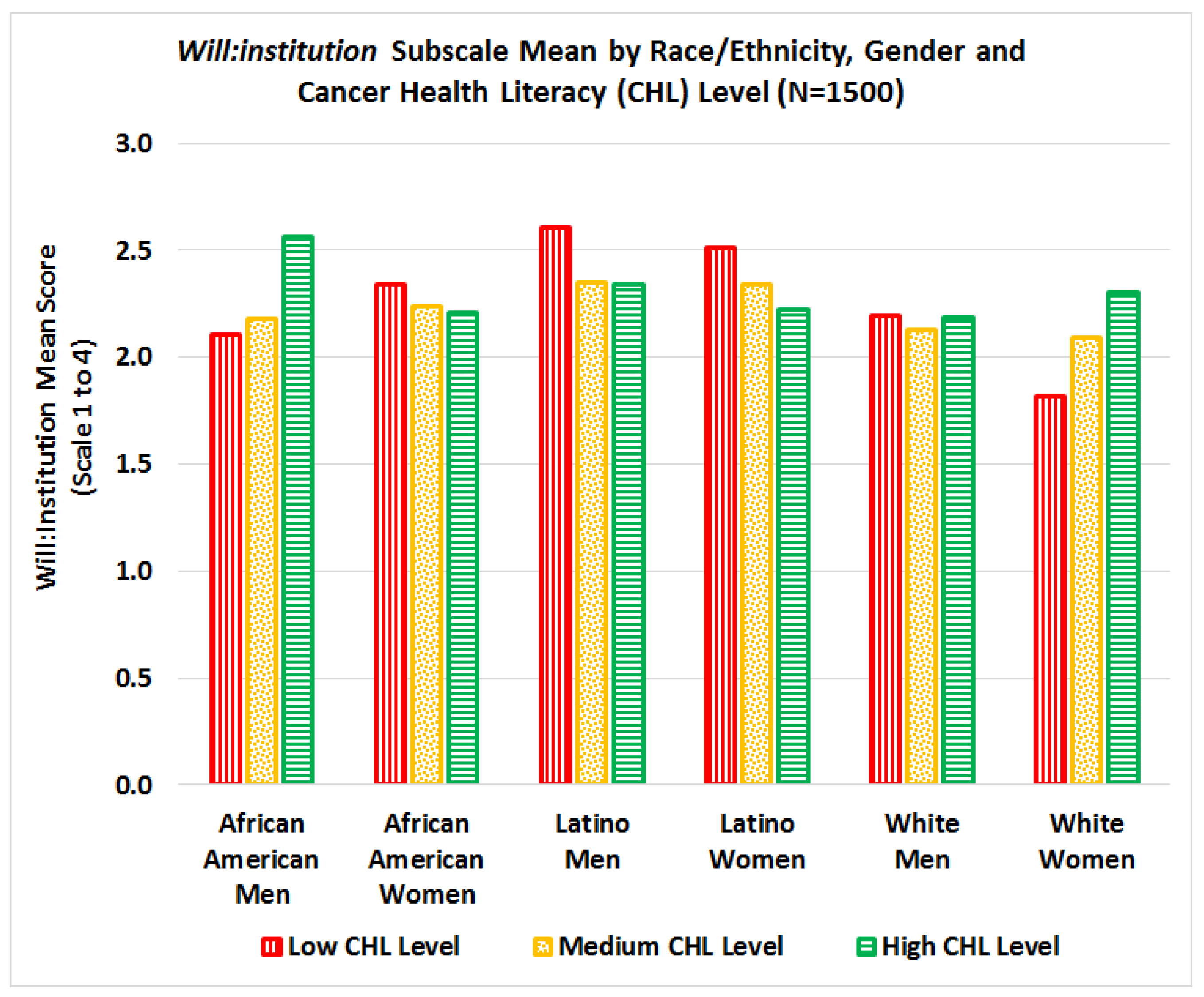
3.5. Interactions in willingness to participate by institution type (WILL:Institution)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Colby, S.L.; Ortman, J.M. Projections of the Size and Composition of the U.S. Population: 2014 to 2060. Current Population Reports, P25-1143; U.S. Census Bureau: Washington, DC, USA, 2014.
- American Cancer Society (ACS). Cancer Facts & Figures for African Americans 2016–2018. American Cancer Society: Atlanta, 2016. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-african-americans/cancer-facts-and-figures-for-african-americans-2016-2018.pdf (accessed on 21 September 2018).
- American Cancer Society (ACS). Cancer Facts & Figures for Hispanics/Latinos 2015–2017. American Cancer Society: Atlanta, 2015. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-hispanics-and-latinos/cancer-facts-and-figures-for-hispanics-and-latinos-2015-2017.pdf. (accessed on 21 September 2018).
- Siegel, R.; Ward, E.; Brawley, O.; Jemal, A. Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J. Clin. 2011, 61, 212–236. [Google Scholar] [CrossRef] [PubMed]
- Evans, K.R.; Lewis, M.J.; Hudson, S.V. The Role of Health Literacy on African American and Hispanic/Hispanic Perspectives on Cancer Clinical Trials. J. Cancer Educ. 2012, 27, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; Lara, P.N.; Dang, J.H.T.; Paterniti, D.A.; Kelly, K. Twenty years post-NIH revitalization act: Enhancing minority participation in clinical trials (EMPaCT): Laying the groundwork for improving minority clinical trial accrual. Cancer 2014, 120, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, K.; Coe, K.; Bailar, J.C.; Swanson, G.M. Inclusion of minorities and women in cancer clinical trials, a decade later: Have we improved? Cancer 2013, 119, 2956–2963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra, A.; Karnad, A.B.; Thompson, I.M. Hispanic accrual on randomized cancer clinical trials: A call to arms. J. Clin. Oncol. 2014, 32, 1871–1873. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (NIH). Enrollment for All Nih Clinical Research at U.S. Sites Racial Categories for Fy 15 and Fy 16 (Figures 1 and 2). Report of the Advisory Committee on Research on Women S Health, Fiscal Years 2015 2016. National Institutes of Health: Bethesda, MD, 2017; Nih Publication No. 17 Od 7995. Available online: https://orwh.od.nih.gov/sites/orwh/files/docs/ORWH_Biennial_Report_WEB_508_FY-15-16.pdf (accessed on 21 September 2018).
- U.S. Food and Drug Administration (FDA). 2015–2016 Global Participation in Clinical Trials Report. FDA’s Center for Drug Evaluation and Research’s (CDER): Silver Spring, MD. Available online: https://www.fda.gov/downloads/Drugs/InformationOnDrugs/UCM570195.pdf (accessed on 22 September 2018).
- Rivers, D.; August, E.M.; Sehovic, I.; Green, B.L.; Quinn, G.P. A systematic review of the factors influencing African Americans’ participation in cancer clinical trials. Contemp. Clin. Trials 2013, 35, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; McIntyre, J.; Gonzalez, L.E.; Muñoz-Antonia, T.; Antolino, P.; Wells, K.J. Improving Awareness of Cancer Clinical Trials among Hispanic Patients and Families: Audience Segmentation Decisions for a Media Intervention. J. Health Commun. 2013, 18, 1131–1147. [Google Scholar] [CrossRef] [PubMed]
- Young, R.F.; Waller, J.B., Jr.; Smitherman, H. A breast cancer education and on-site screening intervention for unscreened African American women. J. Cancer Educ. 2002, 17, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Weekes, C.V. African Americans and health literacy: A systematic review. J. Assoc. Afr. Am. Nurs. Fac. 2012, 23, 76–80. [Google Scholar]
- Muñoz-Antonia, T.; Ung, D.; Montiel-Ishino, F.A.; Nelson, A.; Canales, J.; Quinn, G.P. African Americans’ and Hispanics’ Information Needs About Cancer Care. J. Cancer Educ. 2015, 30, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Zarcadoolas, C.; Pleasant, A.; Greer, D.S. Understanding health literacy: An expanded model. Health Promot. Int. 2005, 20, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Echeverri, M.; Anderson, D.; Nápoles, A.M. Cancer Health Literacy Test-30-Spanish (CHLT-30-DKspa), a new Spanish-language version of the Cancer Health Literacy Test (CHLT-30) for Spanish-speaking Hispanics. J. Health Commun. 2016, 21, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Unger, J.M.; Cook, E.; Tai, E.; Bleyer, A. Role of Clinical Trial Participation in Cancer Research: Barriers, Evidence, and Strategies. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Napoles, A.; Cook, E.; Ginossar, T.; Knight, K.D.; Ford, M.E. Applying a Conceptual Framework to Maximize the Participation of Diverse Populations in Cancer Clinical Trials. Adv. Cancer Res. 2017, 133, 77–94. [Google Scholar] [CrossRef]
- Friesen, L.R.; Williams, K.B. Attitudes and motivations regarding willingness to participate in dental clinical trials. Contemp. Clin. Trials Commun. 2016, 2, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Garza, M.A.; Quinn, S.C.; Li, Y.; Assini-Meytin, L.; Casper, E.T.; Fryer, C.S.; Butler, J.; Brown, N.A.; Kim, K.H.; Thomas, S.B. The influence of race and ethnicity on becoming a human subject: Factors associated with participation in research. Contemp. Clin. Trials Commun. 2017, 7, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.G.; Howerton, M.W.; Lai, G.Y.; Gary, T.L.; Bolen, S.; Gibbons, M.C.; Tilburt, J.; Baffi, C.; Tanpitukpongse, T.P.; Wilson, R.W.; Powe, N.R.; Bass, E.B. Barriers to recruiting underrepresented populations to cancer clinical trials: A systematic review. Cancer 2008, 15, 112, 228–242. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.B.; Corwin, S.J.; Dominick, G.M.; Rose, I.D. African American men’s understanding and perceptions about prostate cancer: Why multiple dimensions of health literacy are important in cancer communication. J. Community Health 2009, 34, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Durant, R.W.; Wenzel, J.A.; Scarinci, I.C.; Paterniti, D.A.; Fouad, M.N.; Hurd, T.C.; Martin, M.Y. Perspectives on barriers and facilitators to minority recruitment for clinical trials among cancer center leaders, investigators, research staff, and referring clinicians: Enhancing minority participation in clinical trials (EMPaCT). Cancer 2014, 120, 1097–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumenci, L.; Matsuyama, R.; Riddle, D.L.; Cartwright, L.A.; Perera, R.A.; Chung, H.; Siminoff, L.A. Measurement of cancer health literacy and identification of patients with limited cancer health literacy. J. Health Commun. 2014, 19 Suppl 2, 205–224. [Google Scholar] [CrossRef]
- Wendler, D.; Kington, R.; Madans, J.; Wye, G.V.; Christ-Schmidt, H.; Pratt, L.A.; Brawley, O.W.; Gross, C.P.; Emanuel, E. Are Racial and Ethnic Minorities Less Willing to Participate in Health Research? PLoS Med. 2006, 3, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Byrne, M.M.; Tannenbaum, S.L.; Glück, S.; Hurley, J.; Antoni, M. Participation in Cancer Clinical Trials: Why Are Patients Not Participating? Med. Decis. Mak. 2014, 34, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Hunt, L.M.; de Voogd, K.B. Are good intentions good enough? Informed consent without trained interpreters. J. Gen. Intern. Med. 2007, 22, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Boualam, N.; Bowers, L. Language as a Barrier in Cancer Clinical Trial Eligibility. Abramson Cancer Center, University of Pennsylvania, 2015. Available online: http://ldi.upenn.edu/sites/default/files/sumr_docs/Language_as_a_Barrier_in_Cancer_Clinical_Trial_Eligibility_Boualam_Bowers_0.pdf (accessed on 22 September 2018).
- Egleston, B.L.; Pedraza, O.; Wong, Y.N.; Dunbrack, R.L.; Griffin, C.L.; Ross, E.A.; Beck, J.R. Characteristics of clinical trials that require participants to be fluent in English. Clin. Trials (UK) 2015, 12, 618–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurt, A.; Semler, L.; Jacoby, J.L.; Johnson, M.B.; Careyva, B.A.; Stello, B.; Friel, T.; Knouse, M.C.; Kincaid, H.; Smulian, J.C. Racial Differences Among Factors Associated with Participation in Clinical Research Trials. J. Racial Ethn. Health Disparities 2017, 4, 827–836. [Google Scholar] [CrossRef] [PubMed]
- National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research. The Commission: Bethesda, MD. Available online: https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/read-the-belmont-report/index.html (accessed on 22 September 2018).
- Office for Human Research Protections. Federal Policy for the Protection of Human Subjects (‘Common Rule’). Federal Register. Available online: https://www.gpo.gov/fdsys/pkg/FR-2017-01-19/pdf/2017-01058.pdf. (accessed on 22 September 2018).
- Kerasidou, A. Trust me, I’m a researcher!: The role of trust in biomedical research. Med. Health Care Philos. 2017, 20, 43–50. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; Townsend, A.; Cox, S.M.; Paterson, N.D.; Lafrenière, D. Trust in health research relationships: Accounts of human subjects. J. Empir. Res. Hum. Res. Ethics 2008, 3, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Resnik, D.B. Scientific Research and the Public Trust. Sci. Eng. Ethics 2011, 17, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Horn, E.J.; Edwards, K.; Terry, S.F. Engaging Research Participants and Building. Genet. Test. Mol. Biomark. 2011, 15, 839–840. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Duran, N.; Norris, K.A. Systematic Review of Barriers and Facilitators to Minority Research Participation among African Americans, Hispanics, Asian Americans, and Pacific Islanders. Am. J. Public Health 2014, 104, e16–e31. [Google Scholar] [CrossRef] [PubMed]
- Ellis, P.M.; Butow, P.N.; Tattersall, M.H.; Dunn, S.M.; Houssami, N. Randomized clinical trials in oncology: Understanding and attitudes predict willingness to participate. J. Clin. Oncol. 2001, 19, 3554–3561. [Google Scholar] [CrossRef] [PubMed]
- Lux, M.P.; Hildebrandt, T.; Knetzger, S.M.; Schrauder, M.G.; Jud, S.M.; Hein, A.; Rauh, C.; Fasching, P.A.; Beckmann, M.W.; Thiel, F.C. Knowledge and attitudes regarding medical research studies among patients with breast cancer and gynecological diseases. BMC Cancer 2015, 15, 587. [Google Scholar] [CrossRef] [PubMed]
- Hughson, J.; Woodward-Kron, R.; Parker, A.; Hajek, J.; Bresin, A.; Knoch, U.; Phan, T.; Story, D. A review of approaches to improve participation of culturally and linguistically diverse populations in clinical trials. Trials 2016, 17, 263. [Google Scholar] [CrossRef] [PubMed]
- Dash, C.; Wallington, S.F.; Muthra, S.; Dodson, E.; Mandelblatt, J.; Adams-Campbell, L.L. Disparities in knowledge and willingness to donate research biospecimens: A mixed-methods study in an underserved urban community. Community Genet. 2014, 4, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Egleston, B.L.; Pedraza, O.; Wong, Y.N.; Griffin, C.L.; Ross, E.A.; Beck, J.R. Temporal trends and characteristics of clinical trials for which only one racial or ethnic group is eligible. Contemp. Clin. Trials Commun. 2018, 9, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Castillo, A.G.; Jandorf, L.; Thélémaque, L.D.; King, S.; Duhamel, K. Reported Benefits of Participation in a Research Study. J. Community Health 2012, 37, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.X.; Tan, Y.; Blakeney, N.C.; Seals, B.F.; Ma, X.S.; Zhai, S.; Liu, A.; Tai, Y.; Michaels, M. The Impact of a Community-Based Clinical Trial Educational Intervention among Underrepresented Chinese Americans. Cancer Epidemiol. Biomark. Prev. 2014, 23, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Mood, D.; Gadgeel, S.; Simon, M.S. An educational video to increase clinical trials enrollment among breast cancer patients. Breast Cancer Res. Treat. 2009, 117, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pino, C.; Boutron, I.; Ravaud, P. Inadequate description of educational interventions in ongoing randomized controlled trials. Trials 2012, 13–63. [Google Scholar] [CrossRef] [PubMed]
- Greiner, K.A.; Friedman, D.B.; Adams, S.A.; Gwede, C.K.; Cupertino, P.; Engelman, K.K.; Meade, C.D.; Hébert, J.R. Effective recruitment strategies and community-based participatory research: Community Networks Program Centers’ recruitment in cancer prevention studies. Cancer Epidemiol. Biomark. Prev. 2014, 23, 416–423. [Google Scholar] [CrossRef] [PubMed]
- De Las Nueces, D.; Hacker, K.; DiGirolamo, A.; Hicks, L.S. A Systematic Review of Community-Based Participatory Research to Enhance Clinical Trials in Racial and Ethnic Minority Groups. Health Serv. Res. 2012, 47, 1363–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanza, M.M.; Goodson, M.; Osman, A.; Porraz Capetillo, M.D.; Hared, A.; Nigon, J.A.; Meiers, S.J.; Weis, J.A.; Wieland, M.L.; Sia, I.G. Lessons Learned From Community-Led Recruitment of Immigrants and Refugee Participants for a Randomized, Community-Based Participatory Research Study. J. Immigr. Minor Health 2016, 18, 1241–1245. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain/Item Description | Number of Items | Mean 2 | Std. Deviation | Variance | Cronbach’s Alpha |
|---|---|---|---|---|---|
| Domain 1: Willingness to participate in research studies (WILL:Research) | 6 | 2.44 | 0.831 | 0.690 | 0.867 |
| 2.92 | 1.019 | 1.038 | ||
| 2.76 | 1.017 | 1.034 | ||
| 2.02 | 1.043 | 1.087 | ||
| 2.34 | 1.090 | 1.187 | ||
| 2.38 | 1.130 | 1.277 | ||
| 2.21 | 1.130 | 1.276 | ||
| Domain 2: Willingness to donate bio-specimens for research (WILL:Donate) | 6 | 2.76 | 0.957 | 0.916 | 0.932 |
| 2.97 | 1.074 | 1.154 | ||
| 2.95 | 1.071 | 1.148 | ||
| 3.05 | 1.037 | 1.075 | ||
| 2.89 | 1.107 | 1.225 | ||
| 2.42 | 1.179 | 1.390 | ||
| 2.28 | 1.173 | 1.376 | ||
| Domain 3: Willingness to participate in a cancer study by type of institution conducting the research (WILL:Institution) | 9 | 2.26 | 0.825 | 0.681 | 0.927 |
| 2.95 | 1.018 | 1.037 | ||
| 2.63 | 1.050 | 1.103 | ||
| 2.52 | 1.062 | 1.129 | ||
| 2.24 | 1.060 | 1.124 | ||
| 2.23 | 1.050 | 1.103 | ||
| 1.91 | 0.989 | 0.978 | ||
| 1.79 | 0.988 | 0.976 | ||
| 2.00 | 1.036 | 1.074 | ||
| 2.11 | 1.083 | 1.173 | ||
| WPRDB Total Scale Score | 21 | 2.46 | 0.746 | 0.557 | .948 |
| Non-Latino African Americans | Latinos (Any Race) | Non-Latino Whites | Total | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Total Participants | 500 | 33.3 | 500 | 33.3 | 500 | 33.33 | 1500 | 100.0 |
| Gender | ||||||||
| Male | 250 | 50.0 | 250 | 50.0 | 250 | 50.0 | 750 | 50.0 |
| Female | 250 | 50.0 | 250 | 50.0 | 250 | 50.0 | 750 | 50.0 |
| Age | ||||||||
| 25–40 | 135 | 27.0 | 211 | 42.2 | 181 | 36.2 | 527 | 35.1 |
| 41–55 | 169 | 33.8 | 150 | 30.0 | 143 | 28.6 | 462 | 30.8 |
| 56+ | 196 | 39.2 | 139 | 27.8 | 176 | 35.2 | 511 | 34.1 |
| Education | ||||||||
| Primary school or less | 11 | 2.2 | 112 | 22.4 | 3 | 0.6 | 126 | 8.4 |
| Some High School | 76 | 15.2 | 74 | 14.8 | 29 | 5.8 | 179 | 11.9 |
| High School Diploma | 187 | 37.4 | 111 | 22.2 | 132 | 26.4 | 430 | 28.7 |
| Some college studies | 152 | 30.4 | 133 | 26.6 | 175 | 35.0 | 460 | 30.7 |
| Bachelor or advanced degree | 74 | 14.8 | 70 | 14.0 | 161 | 32.2 | 305 | 20.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Echeverri, M.; Anderson, D.; Nápoles, A.M.; Haas, J.M.; Johnson, M.E.; Serrano, F.S.A. Cancer Health Literacy and Willingness to Participate in Cancer Research and Donate Bio-Specimens. Int. J. Environ. Res. Public Health 2018, 15, 2091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102091
Echeverri M, Anderson D, Nápoles AM, Haas JM, Johnson ME, Serrano FSA. Cancer Health Literacy and Willingness to Participate in Cancer Research and Donate Bio-Specimens. International Journal of Environmental Research and Public Health. 2018; 15(10):2091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102091
Chicago/Turabian StyleEcheverri, Margarita, David Anderson, Anna María Nápoles, Jacqueline M. Haas, Marc E. Johnson, and Friar Sergio A. Serrano. 2018. "Cancer Health Literacy and Willingness to Participate in Cancer Research and Donate Bio-Specimens" International Journal of Environmental Research and Public Health 15, no. 10: 2091. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102091