Cigarette Smoking Modulation of Saliva Microbial Composition and Cytokine Levels



Abstract
:1. Introduction
2. Methods
2.1. Study Subjects
2.2. Depression Symptomatology
2.3. Sample Collection, DNA Extraction, and Amplification
2.4. Illumina MiSeq Sequence Determination by Nextera XT
2.5. Metagenomics Data Quality Control and Analysis
2.6. Cytokine Assay
2.7. Microbial Biomarkers and Correlation Model
2.8. Statistical Analysis
3. Results
3.1. Demographic Parameters of Study Participants
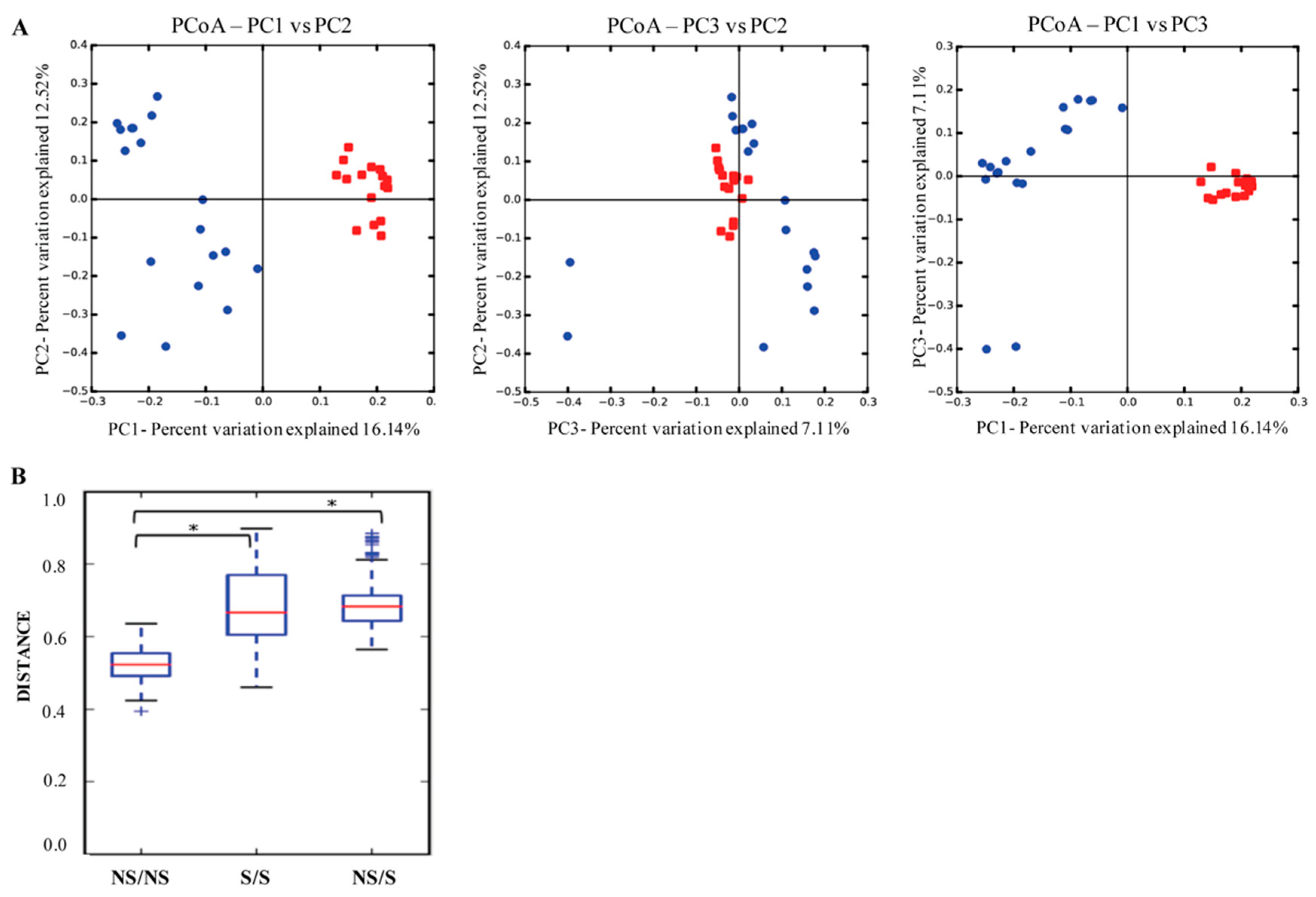
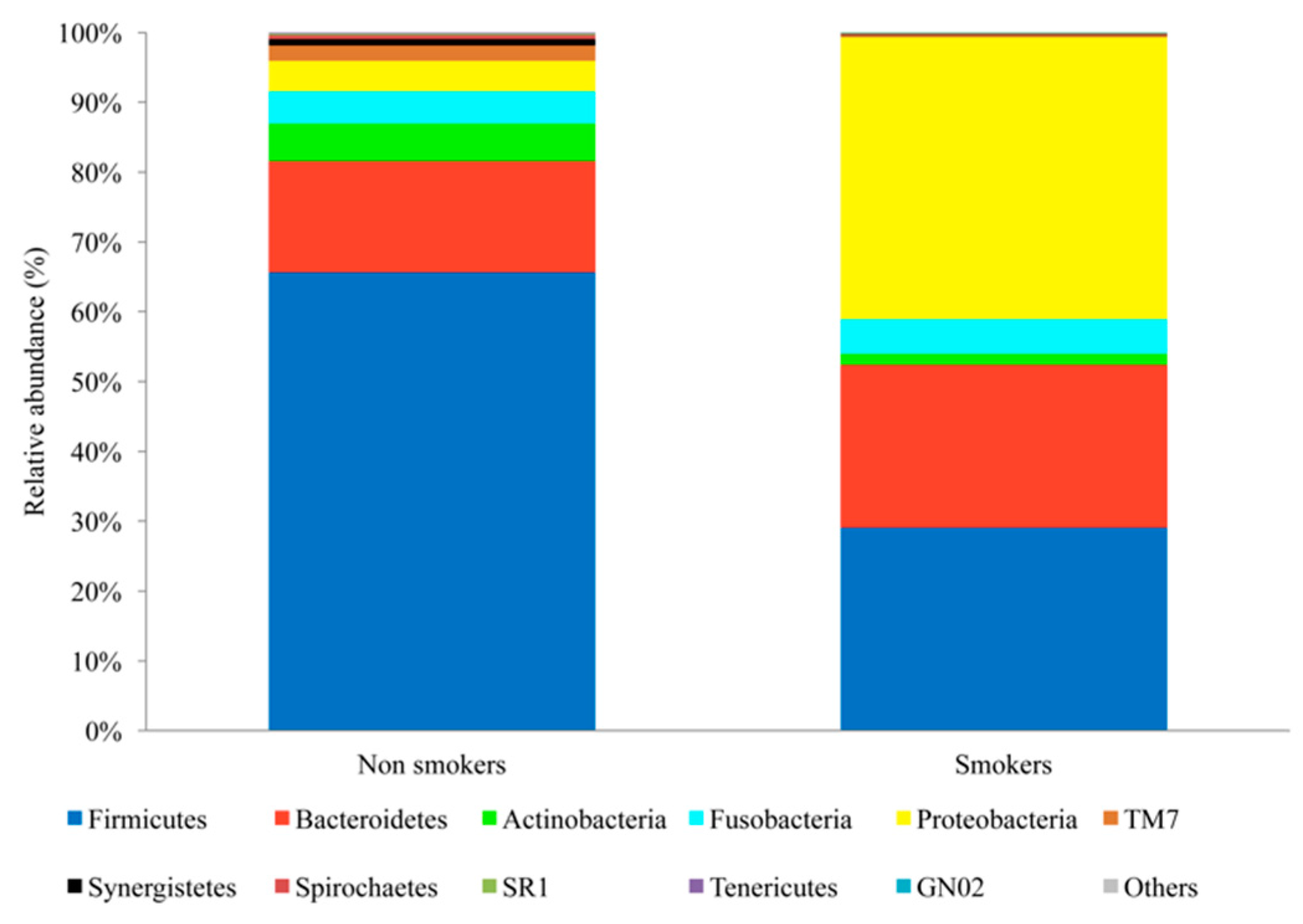
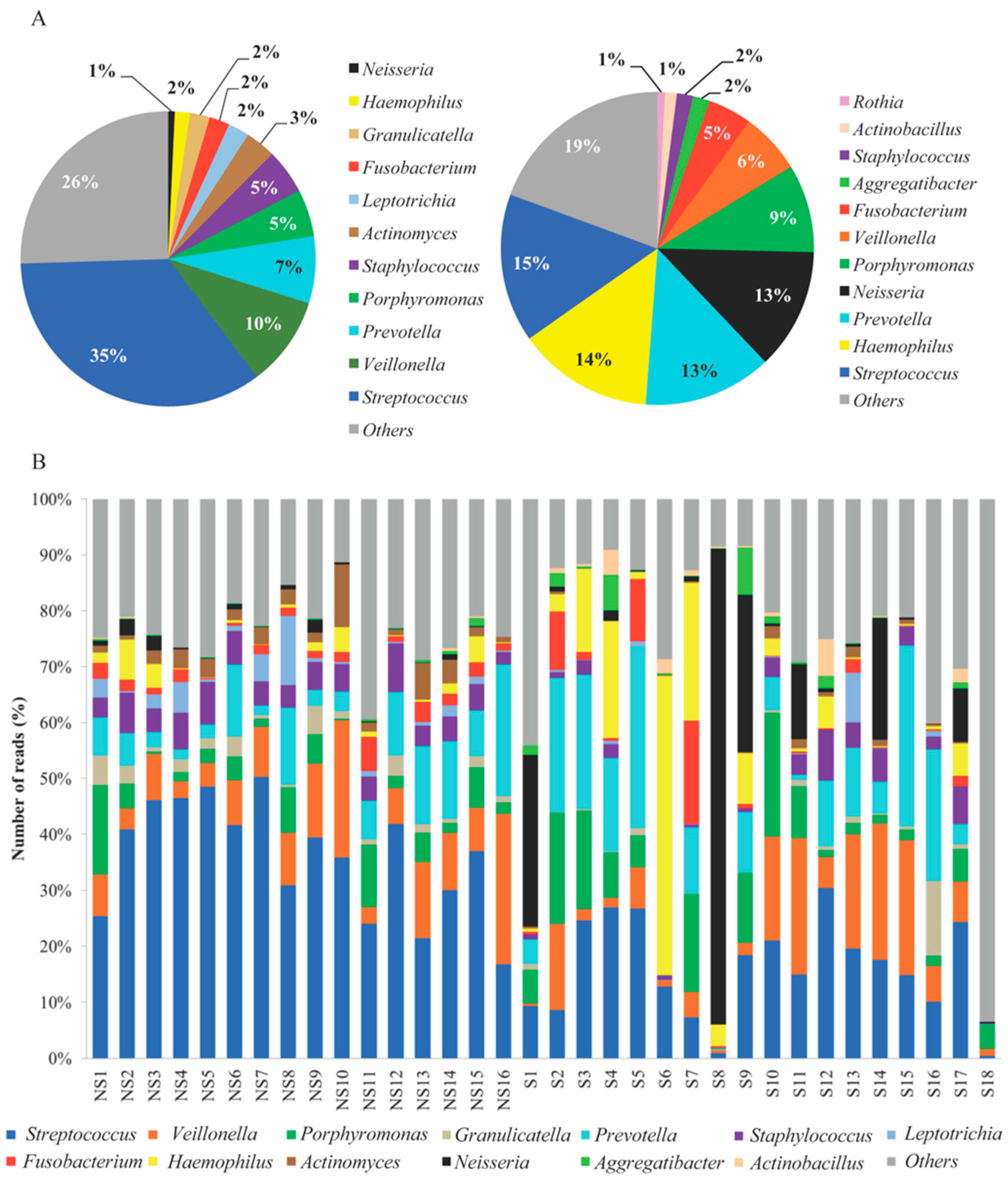
3.2. Microbial Sequencing and Bacterial Diversity
3.3. Cytokines
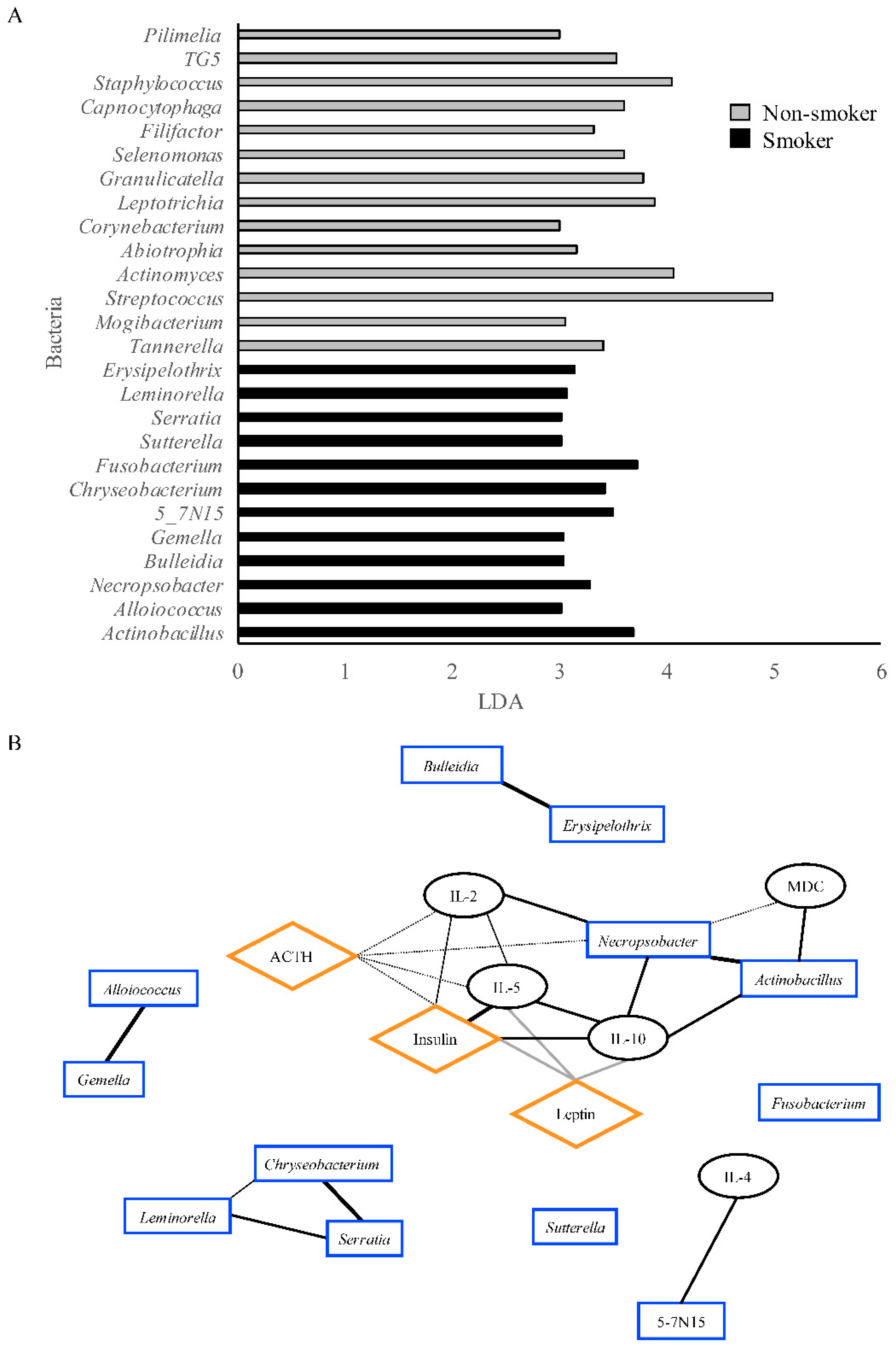
3.4. Correlation Network
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ortiz, A.P.; Diaz-Toro, E.C.; Calo, W.A.; Correa-Fernandez, V.; Cases, A.; Santos-Ortiz, M.C.; Mazas, C.; Mejia, L.; Wetter, D.W. Characteristics of smokers accessing the Puerto Rico quitline. Puerto Rico Health Sci. J. 2008, 27, 213–219. [Google Scholar]
- Centers for Disease Control and Prevention. State Tobacco Activities Tracking and Evaluation (State) System. Available online: https://www.cdc.gov/statesystem/cigaretteuseadult.html (accessed on 9 September 2018).
- Puerto Rico Department of Health. Puerto Rico Chronic Disease Action Plan 2014–2020. Available online: http://www.iccp-portal.org/sites/default/files/plans/Puerto Rico Chronic Disease Action Plan English.pdf (accessed on 7 February 2018).
- Stampfli, M.R.; Anderson, G.P. How cigarette smoke skews immune responses to promote infection, lung disease and cancer. Nat. Rev. Immunol. 2009, 9, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Warren, G.W.; Alberg, A.J.; Kraft, A.S.; Cummings, K.M. The 2014 surgeon general’s report: “The health consequences of smoking—50 years of progress”: A paradigm shift in cancer care. Cancer 2014, 120, 1914–1916. [Google Scholar] [CrossRef] [PubMed]
- Hozawa, A.; Houston, T.; Steffes, M.W.; Widome, R.; Williams, O.D.; Iribarren, C.; Pletcher, M.J.; Daviglus, M.L.; Carr, J.J.; Jacobs, D.R., Jr. The association of cigarette smoking with self-reported disease before middle age: The coronary artery risk development in young adults (cardia) study. Prev. Med. 2006, 42, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Matthews, C.R.; Joshi, V.; de Jager, M.; Aspiras, M. Tobacco smoking affects bacterial acquisition and colonization in oral biofilms. Infect. Immun. 2011, 79, 4730–4738. [Google Scholar] [CrossRef] [PubMed]
- Yu, G.; Phillips, S.; Gail, M.H.; Goedert, J.J.; Humphrys, M.S.; Ravel, J.; Ren, Y.; Caporaso, N.E. The effect of cigarette smoking on the oral and nasal microbiota. Microbiome 2017, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, H.; Yu, Q.; Xue, Q.; Wei, F.; Tao, L. Previous history and cigarette smoking as interfering factors for the effect of vaccine on human papillomavirus infection. J. Infect. Dis. 2014, 209, 1304. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Peters, B.A.; Dominianni, C.; Zhang, Y.; Pei, Z.; Yang, L.; Ma, Y.; Purdue, M.P.; Jacobs, E.J.; Gapstur, S.M.; et al. Cigarette smoking and the oral microbiome in a large study of American adults. ISME J. 2016, 10, 2435–2446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belstrom, D.; Holmstrup, P.; Nielsen, C.H.; Kirkby, N.; Twetman, S.; Heitmann, B.L.; Klepac-Ceraj, V.; Paster, B.J.; Fiehn, N.E. Bacterial profiles of saliva in relation to diet, lifestyle factors, and socioeconomic status. J. Oral. Microbiol. 2014, 6. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Taneja, V.; Vassallo, R. Cigarette smoking and inflammation: Cellular and molecular mechanisms. J. Dent Res. 2012, 91, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Prasad, G.; McCullough, M. Chemokines and cytokines as salivary biomarkers for the early diagnosis of oral cancer. Int. J. Dent. 2013, 2013, 813756. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Castillo, V.; Sanhueza, E.; McNerney, E.; Onate, S.A.; Garcia, A. Microbiota dysbiosis: A new piece in the understanding of the carcinogenesis puzzle. J. Med. Microbiol. 2016, 65, 1347–1362. [Google Scholar] [CrossRef] [PubMed]
- Hayes, R.B.; Bravo-Otero, E.; Kleinman, D.V.; Brown, L.M.; Fraumeni, J.F., Jr.; Harty, L.C.; Winn, D.M. Tobacco and alcohol use and oral cancer in puerto rico. Cancer Causes Control 1999, 10, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Psoter, W.J.; Morse, D.E.; Sanchez-Ayendez, M.; Vega, C.M.; Aguilar, M.L.; Buxo-Martinez, C.J.; Psoter, J.A.; Kerr, A.R.; Lane, C.M.; Scaringi, V.J.; et al. Increasing opportunistic oral cancer screening examinations: Findings from focus groups with general dentists in puerto rico. J. Cancer Educ. 2015, 30, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Martell, B.N.; Garrett, B.E.; Caraballo, R.S. Disparities in adult cigarette smoking—United States, 2002–2005 and 2010–2013. MMWR Morb. Mortal Wkly. Rep. 2016, 65, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.M.; Gridley, G.; Diehl, S.R.; Winn, D.M.; Harty, L.C.; Otero, E.B.; Fraumeni, J.F., Jr.; Hayes, R.B. Family cancer history and susceptibility to oral carcinoma in puerto rico. Cancer 2001, 92, 2102–2108. [Google Scholar] [CrossRef]
- Perera, M.; Al-Hebshi, N.N.; Speicher, D.J.; Perera, I.; Johnson, N.W. Emerging role of bacteria in oral carcinogenesis: A review with special reference to perio-pathogenic bacteria. J. Oral. Microbiol. 2016, 8, 32762. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E. Oral cancer prevention and control—The approach of the world health organization. Oral. Oncol. 2009, 45, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.J.; Crean, S.J.; Fardy, M.J.; Lewis, M.A.; Spratt, D.A.; Wade, W.G.; Wilson, M.J. A molecular analysis of the bacteria present within oral squamous cell carcinoma. J. Med. Microbiol. 2007, 56, 1651–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerrero-Preston, R.; Godoy-Vitorino, F.; Jedlicka, A.; Rodriguez-Hilario, A.; Gonzalez, H.; Bondy, J.; Lawson, F.; Folawiyo, O.; Michailidi, C.; Dziedzic, A.; et al. 16s rrna amplicon sequencing identifies microbiota associated with oral cancer, human papilloma virus infection and surgical treatment. Oncotarget 2016, 7, 51320–51334. [Google Scholar] [CrossRef] [PubMed]
- Kato, I.; Vasquez, A.A.; Moyerbrailean, G.; Land, S.; Sun, J.; Lin, H.S.; Ram, J.L. Oral microbiome and history of smoking and colorectal cancer. J. Epidemiol. Res. 2016, 2, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Zarco, M.F.; Vess, T.J.; Ginsburg, G.S. The oral microbiome in health and disease and the potential impact on personalized dental medicine. Oral. Dis. 2012, 18, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, J.; Segers, S.; Hayes, R.B. Periodontal disease, porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis 2012, 33, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Zackular, J.P.; Rogers, M.A.; Ruffin, M.T.T.; Schloss, P.D. The human gut microbiome as a screening tool for colorectal cancer. Cancer Prev. Res. 2014, 7, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Izard, J. Microbiota, oral microbiome, and pancreatic cancer. Cancer J. 2014, 20, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Izard, J.; Wilhelm-Benartzi, C.S.; You, D.H.; Grote, V.A.; Tjonneland, A.; Dahm, C.C.; Overvad, K.; Jenab, M.; Fedirko, V.; et al. Plasma antibodies to oral bacteria and risk of pancreatic cancer in a large european prospective cohort study. Gut 2013, 62, 1764–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, J.J.; Zhang, L.; Zhou, H.; Chia, D.; Elashoff, D.; Akin, D.; Paster, B.J.; Joshipura, K.; Wong, D.T. Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 2012, 61, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Littman, D.R.; Pamer, E.G. Role of the commensal microbiota in normal and pathogenic host immune responses. Cell Host Microbe 2011, 10, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The phq-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.; Unutzer, J.; Callahan, C.M.; Perkins, A.J.; Kroenke, K. Monitoring depression treatment outcomes with the patient health questionnaire-9. Med. Care 2004, 42, 1194–1201. [Google Scholar] [PubMed]
- Lowe, B.; Schenkel, I.; Carney-Doebbeling, C.; Gobel, C. Responsiveness of the phq-9 to psychopharmacological depression treatment. Psychosomatics 2006, 47, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Williams, J.B.; Kroenke, K.; Hornyak, R.; McMurray, J. Validity and utility of the prime-md patient health questionnaire in assessment of 3000 obstetric-gynecologic patients: The prime-md patient health questionnaire obstetrics-gynecology study. Am. J. Obstet. Gynecol. 2000, 183, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.; Kroenke, K.; Herzog, W.; Grafe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the patient health questionnaire (phq-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glockner, F.O. Evaluation of general 16s ribosomal rna gene pcr primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Pena, A.G.; Goodrich, J.K.; Gordon, J.I.; et al. Qiime allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Navas-Molina, J.A.; Peralta-Sanchez, J.M.; Gonzalez, A.; McMurdie, P.J.; Vazquez-Baeza, Y.; Xu, Z.; Ursell, L.K.; Lauber, C.; Zhou, H.; Song, S.J.; et al. Advancing our understanding of the human microbiome using qiime. Methods Enzymol. 2013, 531, 371–444. [Google Scholar] [PubMed]
- Vazquez-Baeza, Y.; Pirrung, M.; Gonzalez, A.; Knight, R. Emperor: A tool for visualizing high-throughput microbial community data. Gigascience 2013, 2, 16. [Google Scholar] [CrossRef] [PubMed]
- Lozupone, C.A.; Knight, R. The unifrac significance test is sensitive to tree topology. BMC Bioinform. 2015, 16, 211. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.E.; Harris, J.K.; Wagner, B.D.; Granger, D.; Browne, K.; Tatem, B.; Feazel, L.M.; Park, K.; Pace, N.R.; Frank, D.N. Explicet: Graphical user interface software for metadata-driven management, analysis and visualization of microbiome data. Bioinformatics 2013, 29, 3100–3101. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, M.N.; Rodriguez, H.; Burkhardt, B.R.; Alman, A.C. Tumor necrosis factor-alpha, matrix-metalloproteinases 8 and 9 levels in the saliva are associated with increased hemoglobin a1c in type 1 diabetes subjects. PLoS ONE 2015, 10, e0125320. [Google Scholar] [CrossRef] [PubMed]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Cramer, A.; Waldorp, L.; Schmittmann, V.; Borsboom, D. Qgraph: Network visualizations of relationships in psychometric data. J. Stat. Softw. 2012, 48, 1–18. [Google Scholar] [CrossRef]
- Charlson, E.S.; Chen, J.; Custers-Allen, R.; Bittinger, K.; Li, H.; Sinha, R.; Hwang, J.; Bushman, F.D.; Collman, R.G. Disordered microbial communities in the upper respiratory tract of cigarette smokers. PLoS ONE 2010, 5, e15216. [Google Scholar] [CrossRef] [PubMed]
- Grover, N.; Sharma, J.; Sengupta, S.; Singh, S.; Singh, N.; Kaur, H. Long-term effect of tobacco on unstimulated salivary ph. J. Oral. Maxillofac. Pathol. 2016, 20, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Han, C.S.; Martin, M.A.; Dichosa, A.E.K.; Daughton, A.R.; Frietze, S.; Kaplan, H.; Gurven, M.D.; Alcock, J. Salivary microbiomes of indigenous tsimane mothers and infants are distinct despite frequent premastication. PeerJ 2016, 4, e2660. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Quinque, D.; Horz, H.P.; Li, M.; Rzhetskaya, M.; Raff, J.A.; Hayes, M.G.; Stoneking, M. Comparative analysis of the human saliva microbiome from different climate zones: Alaska, Germany, and Africa. BMC Microbiol. 2014, 14, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilian, M.; Chapple, I.L.; Hannig, M.; Marsh, P.D.; Meuric, V.; Pedersen, A.M.; Tonetti, M.S.; Wade, W.G.; Zaura, E. The oral microbiome—An update for oral healthcare professionals. Br. Dent J. 2016, 221, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, D.; Wynder, E.L. Chemical constituents and bioactivity of tobacco smoke. IARC Sci. Publ. 1986, 145–165. [Google Scholar]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A common factor in human diseases. Biomed. Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.M.; Musavian, H.S.; Butt, T.M.; Ingvorsen, C.; Thysen, A.H.; Brix, S. Chronic obstructive pulmonary disease and asthma-associated proteobacteria, but not commensal prevotella spp., promote toll-like receptor 2-independent lung inflammation and pathology. Immunology 2015, 144, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, S.; Rao, R.S.; Amrutha, N.; Sanketh, D. Oral microbial flora in health. World J. Dent. 2013, 4, 262–266. [Google Scholar] [CrossRef]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162, 22–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tribble, G.D.; Lamont, R.J. Bacterial invasion of epithelial cells and spreading in periodontal tissue. Periodontol. 2000 2010, 52, 68–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, A.; Palmer, R.M. A clinical guide to periodontology: Pathology of periodontal disease. Br. Dent. J. 2014, 216, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Stafford, L.; Berk, M.; Jackson, H.J. Tobacco smoking predicts depression and poorer quality of life in heart disease. BMC Cardiovasc. Disord 2013, 13, 35. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Kim, H.C.; Lee, J.Y.; Lee, J.M.; Suh, I. Association between environmental tobacco smoke and depression among Korean women. BMJ Open 2015, 5, e007131. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Mazure, C.M.; McKee, S.A. Smoking and mental illness in the U.S. Population. Tob. Control 2014, 23, e147–e153. [Google Scholar] [CrossRef] [PubMed]
- Malone, K.M.; Waternaux, C.; Haas, G.L.; Cooper, T.B.; Li, S.; Mann, J.J. Cigarette smoking, suicidal behavior, and serotonin function in major psychiatric disorders. Am. J. Psychiatry 2003, 160, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhou, C.; Zhu, D.; Wang, X.; Fang, L.; Zhong, J.; Mao, Q.; Sun, L.; Gong, X.; Xia, J.; et al. Serotonin-1a receptor alterations in depression: A meta-analysis of molecular imaging studies. BMC Psychiatry 2016, 16, 319. [Google Scholar] [CrossRef] [PubMed]
- Mello, N.K. Hormones, nicotine, and cocaine: Clinical studies. Horm. Behav. 2010, 58, 57–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diehl, D.J.; Gershon, S. The role of dopamine in mood disorders. Compr. Psychiatry 1992, 33, 115–120. [Google Scholar] [CrossRef]
- Taylor, L.; Loerbroks, A.; Herr, R.M.; Lane, R.D.; Fischer, J.E.; Thayer, J.F. Depression and smoking: Mediating role of vagal tone and inflammation. Ann. Behav. Med. 2011, 42, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Vargas, H.O.; Nunes, S.O.; de Castro, M.R.; Vargas, M.M.; Barbosa, D.S.; Bortolasci, C.C.; Venugopal, K.; Dodd, S.; Berk, M. Oxidative stress and inflammatory markers are associated with depression and nicotine dependence. Neurosci. Lett. 2013, 544, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Miyata, M.; Ohba, T.; Ando, T.; Hatsushika, K.; Suenaga, F.; Shimokawa, N.; Ohnuma, Y.; Katoh, R.; Ogawa, H.; et al. Cigarette smoke extract induces thymic stromal lymphopoietin expression, leading to t(h)2-type immune responses and airway inflammation. J. Allergy Clin. Immunol. 2008, 122, 1208–1214. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.P.; Gundavarapu, S.; Pena-Philippides, J.C.; Rir-Sima-ah, J.; Mishra, N.C.; Wilder, J.A.; Langley, R.J.; Smith, K.R.; Sopori, M.L. Prenatal secondhand cigarette smoke promotes th2 polarization and impairs goblet cell differentiation and airway mucus formation. J. Immunol. 2011, 187, 4542–4552. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.P.; Mishra, N.C.; Rir-Sima-Ah, J.; Campen, M.; Kurup, V.; Razani-Boroujerdi, S.; Sopori, M.L. Maternal exposure to secondhand cigarette smoke primes the lung for induction of phosphodiesterase-4d5 isozyme and exacerbated th2 responses: Rolipram attenuates the airway hyperreactivity and muscarinic receptor expression but not lung inflammation and atopy. J. Immunol. 2009, 183, 2115–2121. [Google Scholar] [PubMed]
- Mishra, N.C.; Rir-Sima-Ah, J.; Langley, R.J.; Singh, S.P.; Pena-Philippides, J.C.; Koga, T.; Razani-Boroujerdi, S.; Hutt, J.; Campen, M.; Kim, K.C.; et al. Nicotine primarily suppresses lung th2 but not goblet cell and muscle cell responses to allergens. J. Immunol. 2008, 180, 7655–7663. [Google Scholar] [CrossRef] [PubMed]
- Kali, A. Human microbiome engineering: The future and beyond. J. Clin. Diagn. Res. 2015, 9, DE01–DE04. [Google Scholar] [CrossRef] [PubMed]
- Arthur, J.C.; Perez-Chanona, E.; Muhlbauer, M.; Tomkovich, S.; Uronis, J.M.; Fan, T.J.; Campbell, B.J.; Abujamel, T.; Dogan, B.; Rogers, A.B.; et al. Intestinal inflammation targets cancer-inducing activity of the microbiota. Science 2012, 338, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Solovyeva, I.A.; Sobko, E.A.; Ishchenko, O.P.; Kraposhina, A.Y.; Demko, I.V.; Eidemiller, N.S. Impact of tobacco smoking on the clinical and functional indicators and markers of systemic inflammation in patients with severe asthma. Ter. Arkh. 2015, 87, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Holownia, A.; Wielgat, P.; Rysiak, E.; Braszko, J.J. Intracellular and extracellular cytokines in a549 cells and thp1 cells exposed to cigarette smoke. Adv. Exp. Med. Biol. 2016, 910, 39–45. [Google Scholar] [PubMed]
- Zhao, J.; Li, X.; Xie, F.; Yang, Z.; Pan, X.; Zhu, M.; Shang, P.; Nie, C.; Liu, H.; Xie, J. Immunomodulatory effects of cigarette smoke condensate in mouse macrophage cell line. Int. J. Immunopathol. Pharmacol. 2017, 30, 315–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwivedi, S.; Goel, A.; Khattri, S.; Mandhani, A.; Sharma, P.; Pant, K.K. Tobacco exposure by various modes may alter proinflammatory (il-12) and anti-inflammatory (il-10) levels and affects the survival of prostate carcinoma patients: An explorative study in north Indian population. Biomed. Res. Int. 2014, 2014, 158530. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.; Goggel, R.; Chaudhary, N.; Wiedenmann, A.; Jung, B.; Weith, A.; Seither, P. Elevated expression of tarc (ccl17) and mdc (ccl22) in models of cigarette smoke-induced pulmonary inflammation. Biochem. Biophys. Res. Commun. 2005, 334, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Zier, K.S.; Leo, M.M.; Spielman, R.S.; Baker, L. Decreased synthesis of interleukin-2 (il-2) in insulin-dependent diabetes mellitus. Diabetes 1984, 33, 552–555. [Google Scholar] [CrossRef] [PubMed]
- Musselman, D.; Royster, E.B.; Wang, M.; Long, Q.; Trimble, L.M.; Mann, T.K.; Graciaa, D.S.; McNutt, M.D.; Auyeung, N.S.; Oliver, L.; et al. The impact of escitalopram on il-2-induced neuroendocrine, immune, and behavioral changes in patients with malignant melanoma: Preliminary findings. Neuropsychopharmacology 2013, 38, 1921–1928. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ouyang, J.; Liu, S.; Zhang, S.; Chen, P.; Jiang, T. The role of cytokines in the peripheral blood of major depressive patients. Clin. Lab. 2017, 63, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Molofsky, A.B.; Nussbaum, J.C.; Liang, H.E.; Van Dyken, S.J.; Cheng, L.E.; Mohapatra, A.; Chawla, A.; Locksley, R.M. Innate lymphoid type 2 cells sustain visceral adipose tissue eosinophils and alternatively activated macrophages. J. Exp. Med. 2013, 210, 535–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutierrez-Meza, J.M.; Jarillo-Luna, R.A.; Rivera-Aguilar, V.; Miliar-Garcia, A.; Campos-Rodriguez, R. Cytokine profile of nalt during acute stress and its possible effect on iga secretion. Immunol. Lett. 2017, 188, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Nakata, M.; Yamamoto, S.; Okada, T.; Yada, T. Aav-mediated il-10 gene transfer counteracts inflammation in the hypothalamic arcuate nucleus and obesity induced by high-fat diet. Neuropeptides 2017, 62, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Nakata, M.; Yamamoto, S.; Okada, T.; Gantulga, D.; Okano, H.; Ozawa, K.; Yada, T. Il-10 gene transfer upregulates arcuate pomc and ameliorates hyperphagia, obesity and diabetes by substituting for leptin. Int. J. Obes. 2016, 40, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Hu, Y.; Dong, F.; Xu, X.; Hu, A.; Gao, G. Hepatoma cell-derived leptin downregulates the immunosuppressive function of regulatory t-cells to enhance the anti-tumor activity of cd8+ t-cells. Immunol. Cell Biol. 2016, 94, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Filozof, C.; Fernandez Pinilla, M.C.; Fernandez-Cruz, A. Smoking cessation and weight gain. Obes. Rev. 2004, 5, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Rimm, E.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.A.; Willett, W.C.; Rosner, B.; Hennekens, C.H.; Speizer, F.E. Cigarette smoking and the risk of diabetes in women. Am. J. Public Health 1993, 83, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Perry, I.J.; Wannamethee, S.G.; Walker, M.K.; Thomson, A.G.; Whincup, P.H.; Shaper, A.G. Prospective study of risk factors for development of non-insulin dependent diabetes in middle aged British men. BMJ 1995, 310, 560–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawakami, N.; Takatsuka, N.; Shimizu, H.; Ishibashi, H. Effects of smoking on the incidence of non-insulin-dependent diabetes mellitus. Replication and extension in a Japanese cohort of male employees. Am. J. Epidemiol. 1997, 145, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Persson, P.G.; Carlsson, S.; Svanstrom, L.; Ostenson, C.G.; Efendic, S.; Grill, V. Cigarette smoking, oral moist snuff use and glucose intolerance. J. Intern. Med. 2000, 248, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, E.; Kawai, R. Significance of heart rate in the prevalence of metabolic syndrome and its related risk factors in japanese. Circ. J. 2009, 73, 1431–1436. [Google Scholar] [CrossRef] [PubMed]
- Cnop, M.; Landchild, M.J.; Vidal, J.; Havel, P.J.; Knowles, N.G.; Carr, D.R.; Wang, F.; Hull, R.L.; Boyko, E.J.; Retzlaff, B.M.; et al. The concurrent accumulation of intra-abdominal and subcutaneous fat explains the association between insulin resistance and plasma leptin concentrations: Distinct metabolic effects of two fat compartments. Diabetes 2002, 51, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.N.; Chang, W.T.; Chiu, Y.W.; Lee, C.Y.; Lin, K.D.; Cheng, Y.Y.; Su, Y.J.; Chung, H.F.; Huang, M.C. Relationships between changes in leptin and insulin resistance levels in obese individuals following weight loss. Kaohsiung J. Med. Sci. 2013, 29, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Purwar, P.; Khan, M.A.; Mahdi, A.A.; Pandey, S.; Singh, B.; Dixit, J.; Sareen, S. Salivary and serum leptin concentrations in patients with chronic periodontitis. J. Periodontol. 2015, 86, 588–594. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, B.; Smith, U. Leptin levels in smokers and long-term users of nicotine gum. Eur. J. Clin. Investig. 1999, 29, 145–152. [Google Scholar] [CrossRef]
- McKee, S.A.; Sinha, R.; Weinberger, A.H.; Sofuoglu, M.; Harrison, E.L.; Lavery, M.; Wanzer, J. Stress decreases the ability to resist smoking and potentiates smoking intensity and reward. J. Psychopharmacol. 2011, 25, 490–502. [Google Scholar] [CrossRef] [PubMed]
- Von der Goltz, C.; Koopmann, A.; Dinter, C.; Richter, A.; Rockenbach, C.; Grosshans, M.; Nakovics, H.; Wiedemann, K.; Mann, K.; Winterer, G.; et al. Orexin and leptin are associated with nicotine craving: A link between smoking, appetite and reward. Psychoneuroendocrinology 2010, 35, 570–577. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.D.; Walker, M.; Perkins, S.L.; Beyene, J.; Murphy, K.; Gibb, W.; Ohlsson, A. The effect of tobacco exposure on the fetal hypothalamic-pituitary-adrenal axis. BJOG 2006, 113, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.M.C.; Garcia, R.J.F.; Mangas, R.A.; Millan, J. Tobacco and arterial pressure (ii.). The acute effects on the angiotensin-converting enzyme. An. Med. Intern. 1990, 7, 392–395. [Google Scholar]
- Christensen, H.; Korczak, B.M.; Bojesen, A.M.; Kuhnert, P.; Frederiksen, W.; Bisgaard, M. Classification of organisms previously reported as the sp and stewart-letscher groups, with descriptions of necropsobacter gen. Nov. And of necropsobacter rosorum sp. Nov. For organisms of the sp group. Int. J. Syst. Evol. Microbiol. 2011, 61, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Myhrvold, V.; Brondz, I.; Olsen, I. Application of multivariate analyses of enzymic data to classification of members of the actinobacillus-haemophilus-pasteurella group. Int. J. Syst. Bacteriol. 1992, 42, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.Y.; Ng, L.S.; Eng, L.C. Five clinical cases of necropsobacter rosorum bacteremia. J. Clin. Microbiol. 2013, 51, 1337–1340. [Google Scholar] [CrossRef] [PubMed]
- Nonnenmacher, C.; Mutters, R.; de Jacoby, L.F. Microbiological characteristics of subgingival microbiota in adult periodontitis, localized juvenile periodontitis and rapidly progressive periodontitis subjects. Clin. Microbiol. Infect. 2001, 7, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Lehnerdt, G.; Senska, K.; Fischer, M.; Jahnke, K. smoking promotes the formation of peritonsillar abscesses. Laryngorhinootologie 2005, 84, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Schafer, P.; Furrer, C.; Mermillod, B. An association of cigarette smoking with recurrent subareolar breast abscess. Int. J. Epidemiol. 1988, 17, 810–813. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Nonsmokers | Smokers | p-Value * |
|---|---|---|---|
| Individuals (n) | 16 | 18 | - |
| Age in years (mean, range) | 34 (28–50) | 45 (33–49) | 0.109 |
| Sex (male/female) | 6/10 | 10/8 | 0.384 |
| Race | Hispanic | Hispanic | - |
| Education level (percentage) | 0.695 | ||
| ≤High school | 4 (25%) | 6 (33%) | |
| ≥College | 12 (75%) | 12 (67%) | |
| Total years smoking | - | ≤3 years = 2 >3 years = 15 NR a = 1 | - |
| Cigarettes per day (number) | |||
| Light/moderate (≤20 cigarettes) | - | 9 | - |
| Heavy (≥20 cigarettes) | - | 9 | - |
| Alcohol use (yes/no) | 11/5 | 7/11 | 0.721 |
| Assessment of depression symptoms mean ± standard deviation | 6.56 ± 7.36 | 10.89 ± 7.04 | 0.020 |
| Analyte | Nonsmokers Mean ± Standard Deviation (pg/mL) | Smokers Mean ± Standard Deviation Mean (pg/mL) | p-Value * |
|---|---|---|---|
| TNF-α | 28.3 ± 46.19 | 11.2 ± 11.33 | 0.646 |
| IL-12 (p70) | 8.4 ± 5.05 | 182.1 ± 749.43 | 0.281 |
| MDC ↓ | 311.8 ± 399.44 | 114.8 ± 246 | 0.007 |
| IL-10 ↓ | 7.7 ± 12.20 | 1.6 ± 0.23 | 4.28 × 10−4 |
| IFN-γ | 5.2 ± 3.50 | 6.9 ± 7.19 | 0.746 |
| TNF-β | 2.5 ± 1.12 | 1.8 ± 0.33 | 0.126 |
| IL-1 β | 443.1 ± 1358.49 | 214.4 ± 352.95 | 0.384 |
| IL-5 ↓ | 2.7 ± 1.05 | 1.7 ± 0.12 | 0.001 |
| IL-2 ↑ | 1.1 ± 0.02 | 2.4 ± 1.21 | 9.07 × 10−10 |
| IL-6 | 37.1 ± 92.94 | 26.1 ± 71.88 | 0.102 |
| IL-4 ↑ | 1.6 ± 1.48 | 15.6 ± 17.10 | 1.6E-4 |
| IL-1ra | 10,021 ± 2117.65 | 10,296 ± 4958.39 | 0.746 |
| IL-13 | 1.9 ± 1.13 | 1.3 ± 0.90 | 0.365 |
| IL-17 | 6.4 ± 10.95 | 8.5 ± 12.24 | 0.164 |
| IL-7 | 11.3 ± 8.83 | 7.4 ± 9.90 | 0.050 |
| GM-CSF | 30.9 ± 53.91 | 22.5 ± 16.64 | 0.721 |
| ACTH ↑ | 1.5 ± 0.80 | 9.2 ± 7.44 | 5.83 × 10−4 |
| Insulin ↓ | 364.7 ± 87.40 | 27.3 ± 22.23 | 3.66 × 10−4 |
| Leptin ↓ | 33.8 ± 16.03 | 19.3 ± 4.27 | 6.77 × 10−4 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Rabassa, M.; López, P.; Rodríguez-Santiago, R.E.; Cases, A.; Felici, M.; Sánchez, R.; Yamamura, Y.; Rivera-Amill, V. Cigarette Smoking Modulation of Saliva Microbial Composition and Cytokine Levels. Int. J. Environ. Res. Public Health 2018, 15, 2479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112479
Rodríguez-Rabassa M, López P, Rodríguez-Santiago RE, Cases A, Felici M, Sánchez R, Yamamura Y, Rivera-Amill V. Cigarette Smoking Modulation of Saliva Microbial Composition and Cytokine Levels. International Journal of Environmental Research and Public Health. 2018; 15(11):2479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112479
Chicago/Turabian StyleRodríguez-Rabassa, Mary, Pablo López, Ronald E. Rodríguez-Santiago, Antonio Cases, Marcos Felici, Raphael Sánchez, Yasuhiro Yamamura, and Vanessa Rivera-Amill. 2018. "Cigarette Smoking Modulation of Saliva Microbial Composition and Cytokine Levels" International Journal of Environmental Research and Public Health 15, no. 11: 2479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112479