Knowledge Management for Fostering Biostatistical Collaboration within a Research Network: The RTRN Case Study


 , ,
, ,  and
and 
Abstract
:1. Background
RTRN as the Environment of the Proposed Model
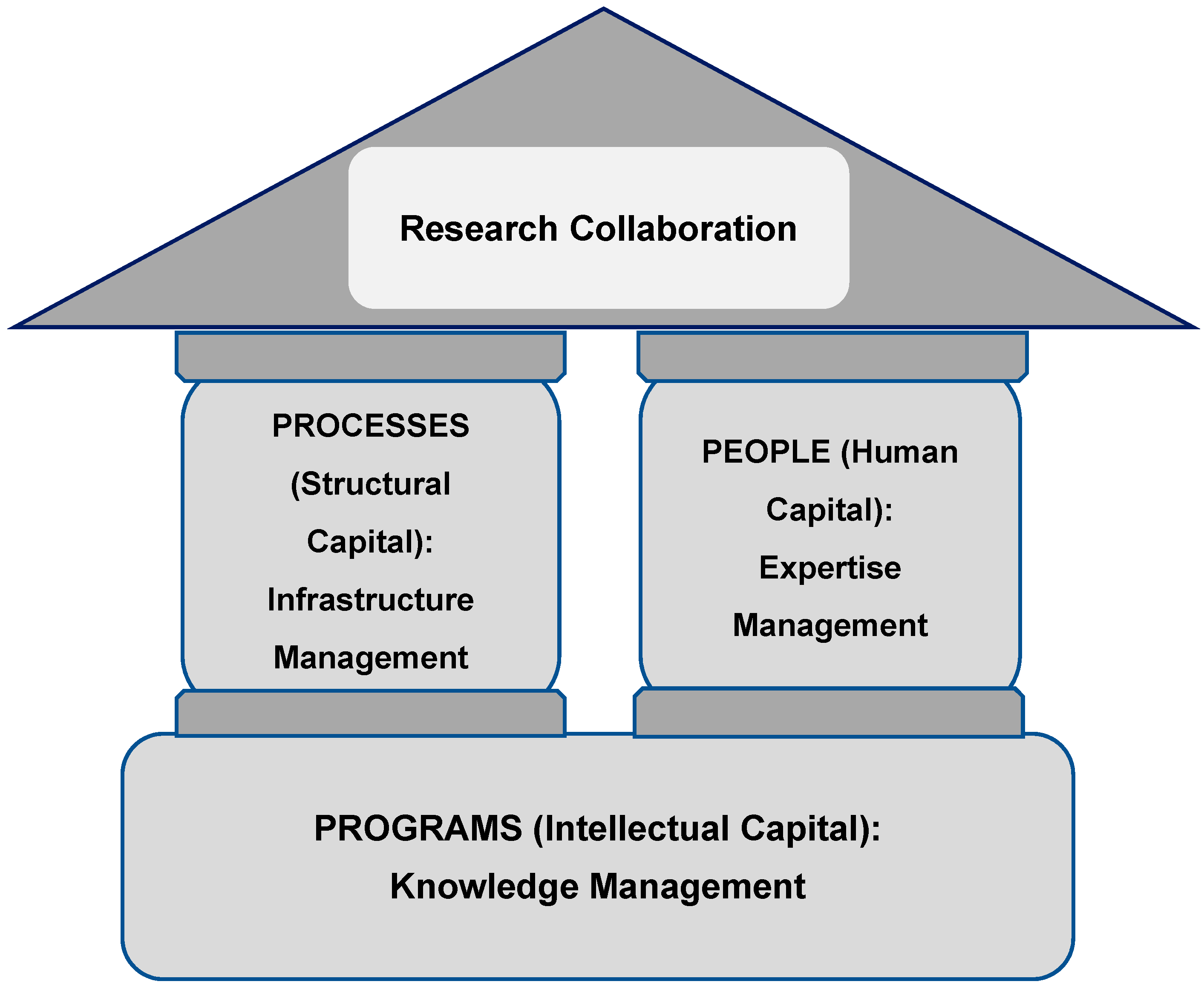
2. Components of the Proposed Model: 3 Ps
3. Strategic Approaches for Collaboration
3.1. Expertise Management
3.1.1. Capacity Assessment
3.1.2. Web Search
3.1.3. Key Research Team Meeting
3.2. Infrastructure Management (IM)
3.2.1. Research Networking (RN) Tools
3.2.2. Policies and Guidelines
3.2.3. GIS Data Capture App
3.2.4. Data Infrastructure
3.3. Knowledge Management
3.3.1. Biostatistical Mobile Clinic Collaborative Exchange Program
3.3.2. Webinar Series/Workshop/Consulting
3.3.3. Partnership
3.3.4. Adjunct Statistician Program
3.3.5. Jackson Heart Study Vanguard Center
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thargard, P. Collaborative knowledge. Noûs 1997, 31, 242–261. [Google Scholar] [CrossRef]
- Fleming, E.; Perkins, J.; Easa, D.; Conde, J.; Baker, R.; Southerland, W.; Dottin, R.; Benabe, J.; Ofili, E.; Bond, V.; et al. The role of translational research in addressing health disparities: A conceptual framework. Ethn. Dis. 2008, 18, S2-155-60. [Google Scholar]
- Vick, T.E.; Nagano, M.S. Preconditions for successful knowledge creation in the context of academic innovation projects. J. Inf. Knowl. Manag. 2018, 17, 1850004. [Google Scholar] [CrossRef]
- Ziman, J. Prometheus Bound: Science in a Dynamic Steady State; Cambridge University Press: Cambridge, UK, 1994. [Google Scholar]
- Gibbons, M.; Limoges, G.; Nowotny, H.; Schwartzman, S.; Scott, P.; Trow, M. The New Production of Knowledge: The Dynamics of Science and Research in Contemporary Societies; SAGE Publications: London, UK, 1994. [Google Scholar]
- Hudson, J. Trends in multi-authored papers in economics. J. Econ. Perspect. 1996, 10, 153–158. [Google Scholar] [CrossRef]
- Rosenblat, T.; Mobius, M. Getting closer or drifting apart? Q. J. Econ. 2004, 119, 971–1009. [Google Scholar] [CrossRef] [Green Version]
- Varda, D.; Shoup, J.A.; Miller, S. A systematic review of collaboration and network research in the public affairs literature: Implications for public health practice and research. Am. J. Public Health. 2012, 102, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Bozeman, B. The impact of research collaboration on scientific productivity. Soc. Stud. Sci. 2005, 35, 673–702. [Google Scholar] [CrossRef]
- Ribeiro, S.X.; Nagano, M.S. Elements influencing knowledge management in university–business–government collaboration: Case studies in National Institutes of Science and Technology. Knowl. Process Manag. 2018, 25, 207–219. [Google Scholar] [CrossRef]
- Ribeiro, S.X.; Nagano, M.S. Main dimensions that impact knowledge management and university-business-government collaboration in the Brazilian scenario. Rev. Gestão 2018, 25, 258–273. [Google Scholar] [CrossRef]
- De Castro, I.J.; Nagano, M.S.; Ribeiro, S.X. Elements That Influence Knowledge Sharing in the University-Industry-Government Collaboration: Case Studies in Brazil. Available online: https://0-www-emeraldinsight-com.brum.beds.ac.uk/doi/full/10.1108/REGE-04-2018-0061 (accessed on 12 November 2018).
- Stokols, D.; Hall, K.L.; Taylor, B.K.; Moser, R.P. The science of team science: Overview of the field and introduction to the supplement. Am. J. Prev. Med. 2008, 35, S77–S89. [Google Scholar] [CrossRef] [PubMed]
- Robinson, T.E.; Rankin, N.; Janssen, A.; Mcgregor, D.; Grieve, S.; Shaw, T. Collaborative research networks in health: A pragmatic scoping study for the development of an imaging network. Health Res. Policy Syst. 2015, 13, 76. [Google Scholar] [CrossRef] [PubMed]
- Gunn, J.M. Should Australia develop primary care research networks? Med. J. Aust. 2002, 177, 63–66. [Google Scholar] [PubMed]
- Lee, J.E.; Perkins, J.; Barnett, E.M.; Sarpong, D.; Sung, J. Importance of capacity assessment for an early staged-research network designed to eliminate health disparity: Lessons from RTRN. Ethn. Dis. 2010, 20, 5–8. [Google Scholar]
- Fleming, E.S.; Perkins, J.; Easa, D.; Conde, J.; Baker, R.; Southerland, W.; Dottin, R.; Benabe, J.; Ofili, E.; Bond, V.; et al. Addressing health disparities through multi-institutional, multidisciplinary collaboratories. Ethn. Dis. 2008, 18, S2-161-7. [Google Scholar]
- Naseer, A.; Stergioulas, L.K. Web-services-based resource discovery model and service deployment on HealthGrids. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Vasilevsky, N.; Johnson, T.; Corday, K.; Torniai, C.; Brush, M.; Segerdell, E.; Wilson, M.; Shaffer, C.; Robinson, D.; Haendel, M. Research resources: Curating the new eagle-i discovery system. Database 2012. [Google Scholar] [CrossRef] [PubMed]
- Fazel-Zarandi, M.; Devlin, H.J.; Huang, Y.; Contractor, N. Expert recommendation based on social drivers, social network analysis, and semantic data representation. In Proceedings of the 2nd International Workshop on Information Heterogeneity and Fusion in Recommender Systems, Chicago, IL, USA, 27 October 2011. [Google Scholar]
- Carey, J. Faculty of 1000 and VIVO: Invisible colleges and team science. Issues Sci. Technol. Libr. 2011. [Google Scholar] [CrossRef]
- Nyabawa, R.F. Technology in learning: Blackboard usage & its impact on academic performance; A case for Universities in Lesotho. Int. J. Humanit. Manag. Sci. 2016, 4, 455–461. [Google Scholar]
- Jones, A. Evaluation of Canvas-Based Online Homework for Engineering. Available online: https://peer.asee.org/evaluation-of-canvas-based-online-homework-for-engineering.pdf (accessed on 20 September 2018).[Green Version]
- Lee, J.E.; Sung, J.H.; Malouhi, M. Statistical validation of a web-based GIS application and its applicability to cardiovascular-related studies. Int. J. Environ. Res. Public Health 2016, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Rideout, C.; Tseng, W.; Islam, N.; Cook, W.K.; Ro, M.; Trinh-Shevrin, C. Developing the community empowered research training program: Building research capacity for community-initiated and community-driven research. Prog. Community Health Partnersh. 2012, 6, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Ramanadhan, S.; Kebede, S.; Mantopoulos, J.; Bradley, E.H. Network-based social capital and capacity-building programs: An example from Ethiopia. Hum. Res. Health 2010, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Sung, J.H.; Barnett, M.E.; Norris, K. User-friendly data-sharing practices for fostering collaboration within a research network: Roles of a vanguard center for a community-based study. Int. J. Environ. Res. Public Health 2016, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Hoadley, A.B.; Kettenring, J.R. Communications between statisticians and engineers/physical scientists. Technometrics 1990, 32, 243–247. [Google Scholar]
- Beckmann, M.J. Economic models of knowledge networks. In Networks in Action; Batten, D., Casti, J., Thord, R., Eds.; Springer: Berlin, Germany, 1995; pp. 159–174. [Google Scholar]
- Redon, R.; Ishikawa, S.; Fitch, K.R.; Feuk, L.; Perry, G.H.; Andrews, T.D.; Fiegler, H.; Shapero, M.H.; Carson, A.R.; Chen, W.; et al. Global variation in copy number in the human genome. Nature 2006, 444, 444–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.F.; Wuchty, S.; Uzzi, B. Multi-university research teams: Ahifting impact, geography, and stratification in science. Science 2008, 322, 1259–1262. [Google Scholar] [CrossRef] [PubMed]
- Bordons, M.; Gomez, I.; Fernandez, M.T.; Zulueta, M.A.; Mendez, A. Local, domestic and international scientific collaboration in biomedical research. Scientometrics 1996, 37, 279–295. [Google Scholar] [CrossRef]
- Lee, K.; Brownstein, J.S.; Mills, R.G.; Kohane, I.S. Does collocation inform the impact of collaboration? PLoS ONE 2010, 5, e14279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ried, K.; Farmer, E.A.; Weston, K.M. Setting directions for capacity building in primary health care: A survey of a research network. BMC Fam. Pract. 2006, 9, 7–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haizlip, J.; May, N.; Schorling, J.; Williams, A.; Plews-Ogan, M. Perspective: The negativity bias, medical education, and the culture of academic medicine: Why culture change is hard. Acad. Med. 2012, 87, 1205–1209. [Google Scholar] [CrossRef] [PubMed]
- Weiner, B.J.; Alexander, J.A.; Shortell, S.M. Leadership for quality improvement in health care; Empirical evidence on hospital boards, managers, and physicians. Med. Care Res. Rev. 1996, 53, 397–416. [Google Scholar] [CrossRef] [PubMed]
- Fos, P.; Lee, J.; Sung, J.; Zuniga, M.; Amy, B. The role of quality improvement in disease management: A state-wide tuberculosis control success story. J. Public Health Manag. Pract. 2005, 11, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Tinker, P.; Donatelli, D. Affecting culture change. Leadership involvement imperative to ensure paradigm shift. Mater Manag. Health Care 2009, 18, 20–22. [Google Scholar] [PubMed]
- Palmer, R.H.; Hargraves, J.L.; Orav, E.J.; Wright, E.A.; Louis, T.A. Leadership for quality improvement group practices. Med. Care 1996, 34, SS40–SS51. [Google Scholar] [CrossRef] [PubMed]
- Baren, J.M.; Middleton, M.K.; Kaji, A.H.; O’Conner, R.E.; Lindsell, C.; Weik, T.S.; Lewis, R.J. Evaluating emergency care research networks: What are the right metrics. Acad. Emerg. Med. 2009, 16, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.A.; Steiner, S.H.; Cook, R.J.; Farewell, V.T.; Morton, A.P. Monitoring the evolutionary process of quality: Risk-adjusted charting to track outcomes in intensive care. Crit. Care Med. 2003, 31, 1676–1682. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Components | Strategic Approaches | Available Plan | |
|---|---|---|---|
| People | Human capital | Expertise Management | Inventory, profile management, ongoing survey, match-making tool, etc. |
| Processes | Structural capital | Infrastructure Management | Networking infrastructure (internet, workspace, Wiki, listserv, etc.); policy and guideline infrastructure (MOU, SOP, leadership plan, etc.); data (repository system, data available, network based analytical tools/ |
| Programs | Intellectual capital | Knowledge Management | adjunct appointment, mobile workshop and clinics, webinar seminars, one-on-one consulting, online and on-site workshop, statistical programing course, certification program, etc. |
| Approach | Engagements |
|---|---|
| Expertise Management | Capacity Assessment: conducted survey for assessing the Networks biostatistical needs and capacities. RTRN biostatistical working group database created through the survey. |
| Web search: identified 235 RCMI investigators who will be user of the data that DCC possesses. | |
| Key Research Team Meeting: this outreach program allowed DCC to identify detailed expertise of key research teams in each member institution through dynamic interaction. | |
| Infrastructure Management | Research Networking (RN) Tools: to communicate with Network biostatisticians, share research related data, and post opinion/experience/knowledge in statistics related issues. |
| Policies and Guidelines: All procedures for the statistical collaboration were governed by DCC standard of process (SOPs). MOU, pre-specified written leadership plan/role assignment among Network biostatisticians for the specific research support, and SOP on collaboration among Network biostatisticians were developed. GIS Data Capture App: The RTRN DCC Web-based GIS application was developed to achieve the goal of procedural standardization for a multi-site study | |
| Data Infrastructure: Data-related infrastructure that the DCC has utilized for the collaboration with Network biostatisticians includes the data itself, data sharing tools, and data analysis software. | |
| Knowledge Management | Biostatistical Mobile Clinic Collaborative Exchange program: a total of 129 investigators participated in this program. The Mobile Biostatistical Clinics took “support” out into the scientific community and helped to minimize some the barriers of communication between statisticians and researchers. |
| Seminar Series/Workshop/Consulting: The DCC provided four webinar seminars, three on-site workshops and on- and off-site consulting programs. More than 520 RTRN investigators and students have attended these programs. | |
| Partnership: DCC has built a partnership with member institutions in organizing/implementing training programs. | |
| Jackson Heart Study Vanguard Center: As a Jackson Heart Study Vanguard Center, the DCC has helped Network investigators including biostatisticians generate scientific output by providing such customized services for secondary data as preliminary analyses for feasibility, data-mining, data workshops and idea sharing meetings, providing data information and query tools through the website, helping develop manuscript proposals, and providing data analyses for publication. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.E.; Sung, J.H.; Sarpong, D.; Efird, J.T.; Tchounwou, P.B.; Ofili, E.; Norris, K. Knowledge Management for Fostering Biostatistical Collaboration within a Research Network: The RTRN Case Study. Int. J. Environ. Res. Public Health 2018, 15, 2533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112533
Lee JE, Sung JH, Sarpong D, Efird JT, Tchounwou PB, Ofili E, Norris K. Knowledge Management for Fostering Biostatistical Collaboration within a Research Network: The RTRN Case Study. International Journal of Environmental Research and Public Health. 2018; 15(11):2533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112533
Chicago/Turabian StyleLee, Jae Eun, Jung Hye Sung, Daniel Sarpong, Jimmy T. Efird, Paul B. Tchounwou, Elizabeth Ofili, and Keith Norris. 2018. "Knowledge Management for Fostering Biostatistical Collaboration within a Research Network: The RTRN Case Study" International Journal of Environmental Research and Public Health 15, no. 11: 2533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112533