Challenges and Lessons Learned from Multi-Level Multi-Component Interventions to Prevent and Reduce Childhood Obesity

 ,
,
Abstract
:1. Introduction
2. Methods
3. Findings
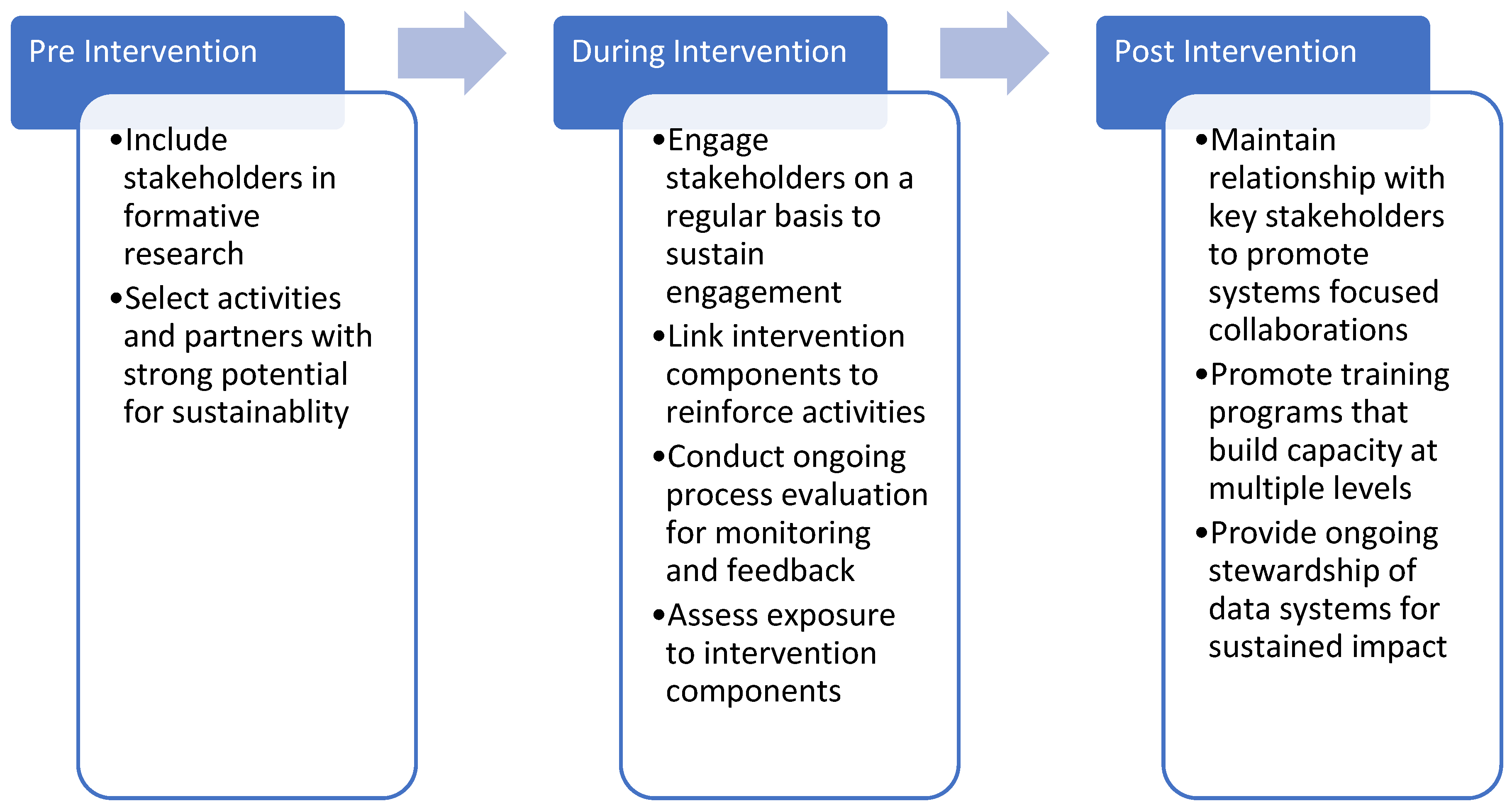
3.1. Design and Engagement (Pre-Intervention)
3.1.1. Lesson #1: Use Early Stage Formative Research Including Stakeholder Analysis to Select Intervention Levels and Components
3.1.2. Lesson #2: Select Intervention Activities and Partners that Have Strong Potential for Sustainability (e.g., Already Doing Similar Work, Capacity Building)
3.2. Building and Maintaining Intervention Intensity (During Intervention Implementation)
3.2.1. Lesson #3: Use Mid-Stage Process Research and Stakeholder Management and Coalition Development to Sustain Engagement
3.2.2. Lesson #4: Create Linkages between Intervention Components Based on Complementarity, Mutual Promotion and Mutual Reinforcement
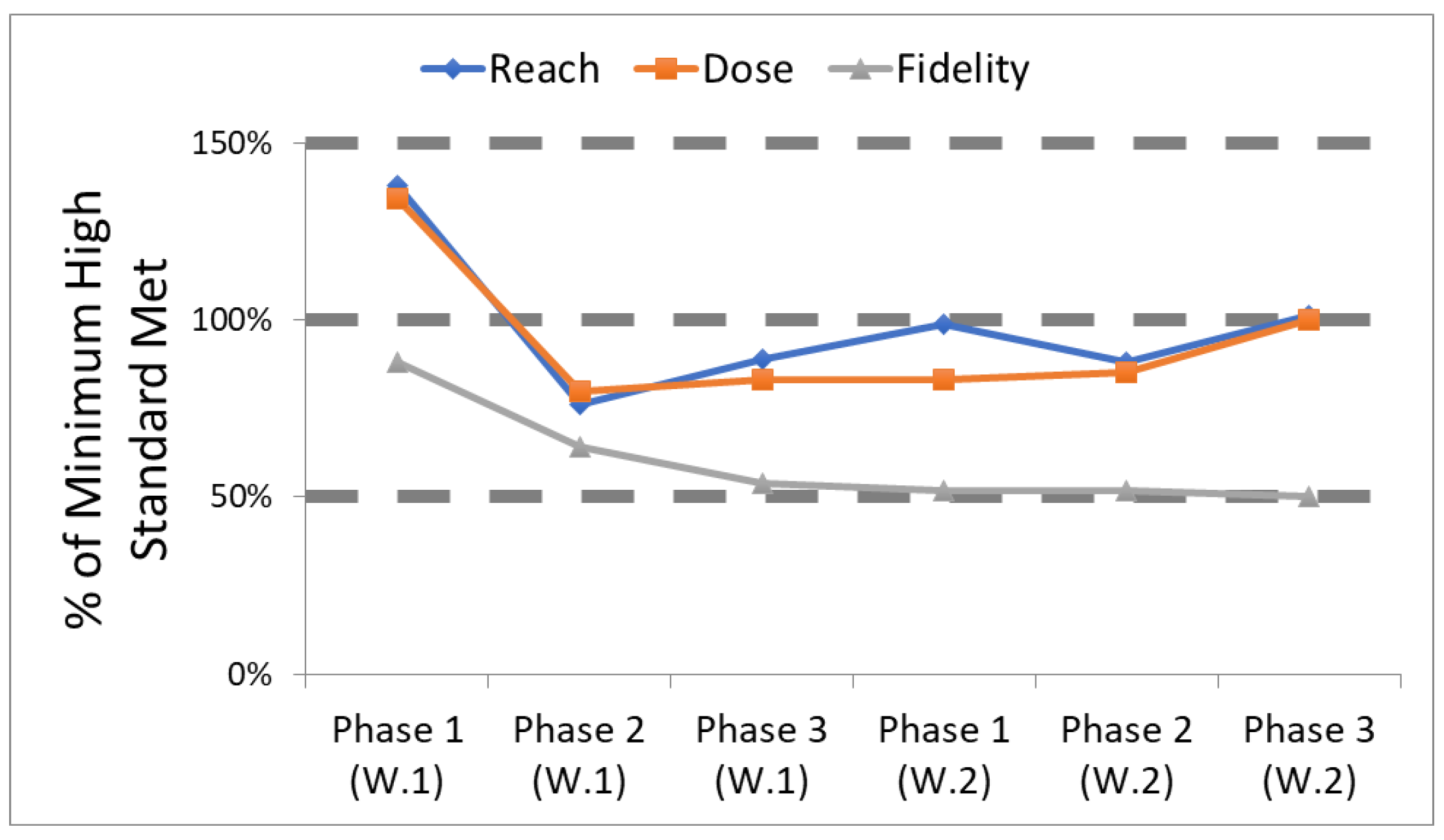
3.2.3. Lesson #5: Conduct Process Evaluation for Monitoring and Feedback
3.2.4. Lesson #6: Assess Exposure to Explain Findings
3.3. Sustaining MLMC Interventions (Post-Intervention Implementation)
3.3.1. Lesson #7: Form Enduring, Systems Focused Collaborations that Plan for Sustainability from the Beginning
3.3.2. Lesson #8: Require Ongoing Training Programs at Multiple Levels
3.3.3. Lesson #9: Ongoing Stewardship of Data Systems is Required for Sustainable Impacts
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfenden, L.; Wyse, R.; Nichols, M.; Allender, S.; Millar, L.; McElduff, P. A systematic review and meta-analysis of whole of community interventions to prevent excessive population weight gain. Prev. Med. 2014, 62, 193–200. [Google Scholar] [CrossRef]
- Ewart-Pierce, E.; Mejía Ruiz, M.J.; Gittelsohn, J. “Whole-of-Community” Obesity Prevention: A Review of Challenges and Opportunities in Multilevel, Multicomponent Interventions. Curr. Obes. Rep. 2016, 5, 361–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinhans, R.; Bolt, G. More than Just Fear: On the Intricate Interplay between Perceived Neighborhood Disorder, Collective Efficacy, and Action. J. Urban Aff. 2014, 36, 420–446. [Google Scholar] [CrossRef]
- Pratt, C.A.; Boyington, J.; Esposito, L.; Pemberton, V.L.; Bonds, D.; Kelley, M.; Yang, S.; Murray, D.; Stevens, J. Childhood Obesity Prevention and Treatment Research (COPTR): Interventions addressing multiple influences in childhood and adolescent obesity. Contemp. Clin. Trials 2013, 36, 406–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwood, N.E.; French, S.A.; Veblen-Mortenson, S.; Crain, A.L.; Berge, J.; Kunin-Batson, A.; Mitchell, N.; Senso, M. NET-Works: Linking families, communities and primary care to prevent obesity in preschool-age children. Contemp. Clin. Trials 2013, 36, 544–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Po’e, E.K.; Heerman, W.J.; Mistry, R.S.; Barkin, S.L. Growing Right Onto Wellness (GROW): A family-centered, community-based obesity prevention randomized controlled trial for preschool child-parent pairs. Contemp. Clin. Trials 2013, 36, 436–449. [Google Scholar] [CrossRef]
- Robinson, T.N.; Matheson, D.; Desai, M.; Wilson, D.M.; Weintraub, D.L.; Haskell, W.L.; McClain, A.; McClure, S.; Banda, J.A.; Sanders, L.M.; et al. Family, community and clinic collaboration to treat overweight and obese children: Stanford GOALS-A randomized controlled trial of a three-year, multi-component, multi-level, multi-setting intervention. Contemp. Clin. Trials 2013, 36, 421–435. [Google Scholar] [CrossRef]
- Moore, S.M.; Borawski, E.a.; Cuttler, L.; Ievers-Landis, C.E.; Love, T.E. IMPACT: A multi-level family and school intervention targeting obesity in urban youth. Contemp. Clin. Trials 2013, 36, 574–586. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wu, Y.; Wilson, R.F.; Bleich, S.; Cheskin, L.; Weston, C.; Showell, N.; Fawole, O.; Lau, B.; Segal, J. Childhood Obesity Prevention Programs: Comparative Effectiveness Review and Meta-Analysis. In Comparative Effectiveness Reviews No. 115; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013; Volume 13-EHC081-EF. [Google Scholar]
- Economos, C.D.; Hammond, R.A. Designing effective and sustainable multifaceted interventions for obesity prevention and healthy communities. Obesity 2017, 25, 1155–1156. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Mui, Y.; Adam, A.; Lin, S.; Kharmats, A.; Igusa, T.; Lee, B.Y. Incorporating Systems Science Principles into the Development of Obesity Prevention Interventions: Principles, Benefits, and Challenges. Curr. Obes. Rep. 2015, 4, 174–181. [Google Scholar] [CrossRef] [Green Version]
- Braun, K.L.; Nigg, C.R.; Fialkowski, M.K.; Butel, J.; Hollyer, J.R.; Barber, L.R.; Bersamin, A.; Coleman, P.; Teo-Martin, U.; Vargo, A.M.; et al. Using the ANGELO Model To Develop the Children’s Healthy Living Program Multilevel Intervention To Promote Obesity Preventing Behaviors for Young Children in the US-Affiliated Pacific Region. Child. Obes. 2014, 10, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Gittelsohn, J.; Anderson Steeves, E.; Mui, Y.; Kharmats, A.Y.; Hopkins, L.C.; Dennis, D. B’More Healthy Communities for Kids: Design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health 2014, 14, 942. [Google Scholar] [CrossRef] [PubMed]
- Fialkowski, M.K.; DeBaryshe, B.; Bersamin, A.; Nigg, C.; Leon Guerrero, R.; Rojas, G.; Areta, A.A.R.; Vargo, A.; Belyeu-Camacho, T.; Castro, R.; et al. A Community Engagement Process Identifies Environmental Priorities to Prevent Early Childhood Obesity: The Children’s Healthy Living (CHL) Program for Remote Underserved Populations in the US Affiliated Pacific Islands, Hawaii and Alaska. Matern. Child Health J. 2014, 18, 2261–2274. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, B.E.; Bloch, P.; Reinbach, H.C.; Buch-Andersen, T.; Lawaetz Winkler, L.; Toft, U.; Glumer, C.; Jensen, B.B.; Aagaard-Hansen, J. Project SoL-A Community-Based, Multi-Component Health Promotion Intervention to Improve Healthy Eating and Physical Activity Practices among Danish Families with Young Children Part 2: Evaluation. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Butel, J.; Braun, K.L.; Novotny, R.; Acosta, M.; Castro, R.; Fleming, T.; Powers, J.; Nigg, C.R. Assessing intervention fidelity in a multi-level, multi-component, multi-site program: The Children’s Healthy Living (CHL) program. Transl. Behav. Med. 2015, 5, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, C.F.; Poirier, L.; Trude, A.C.B.; Yang, T.; Schwendler, T.; Gunen, B.; Loh, I.H.; Perepezko, K.; Nam, C.S.; Sato, P.; et al. Implementation of B’More Healthy Communities for Kids: Process evaluation of a multi-level, multi-component obesity prevention intervention. Health Educ. Res. 2018. [Google Scholar] [CrossRef]
- Novotny, R.; Davis, J.; Butel, J.; et al. Effect of the children’s healthy living program on young child overweight, obesity, and acanthosis nigricans in the us-affiliated pacific region: A randomized clinical trial. JAMA Netw. Open 2018, 1, e183896. [Google Scholar] [CrossRef]
- Winkler, L.L.; Christensen, U.; Glumer, C.; Bloch, P.; Mikkelsen, B.E.; Wansink, B.; Toft, U. Substituting sugar confectionery with fruit and healthy snacks at checkout—A win-win strategy for consumers and food stores? a study on consumer attitudes and sales effects of a healthy supermarket intervention. BMC Public Health 2016, 16, 1184. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Trude, A.C.; Poirier, L.; Ross, A.; Ruggiero, C.; Schwendler, T.; Anderson Steeves, E. The Impact of a Multi-Level Multi-Component Childhood Obesity Prevention Intervention on Healthy Food Availability, Sales, and Purchasing in a Low-Income Urban Area. Int. J. Environ. Res. Public Health 2017, 14, 1371. [Google Scholar] [CrossRef]
- Trude, A.C.B.; Surkan, P.J.; Cheskin, L.J.; Gittelsohn, J. A multilevel, multicomponent childhood obesity prevention group-randomized controlled trial improves healthier food purchasing and reduces sweet-snack consumption among low-income African-American youth. Nutr. J. 2018, 17, 96. [Google Scholar] [CrossRef] [PubMed]
- Wilken, L.R.; Novotny, R.; Fialkowski, M.K.; Boushey, C.J.; Nigg, C.; Paulino, Y.; Leon Guerrero, R.; Bersamin, A.; Vargo, D.; Kim, J.; et al. Children’s Healthy Living (CHL) Program for remote underserved minority populations in the Pacific region: Rationale and design of a community randomized trial to prevent early childhood obesity. BMC Public Health 2013, 13, 944. [Google Scholar] [CrossRef] [PubMed]
- Novotny, R.; Fialkowski, M.K.; Areta, A.A.; Bersamin, A.; Braun, K.; DeBaryshe, B.; Deenik, J.; Dunn, M.; Hollyer, J.; Kim, J.; et al. University of Hawai’i Cancer Center Connection: The Pacific Way to Child Wellness: The Children’s Healthy Living Program for Remote Underserved Minority Populations of the Pacific Region (CHL). Hawaii J. Med. Public Health 2013, 72, 406–408. [Google Scholar] [PubMed]
- Gittelsohn, J.; Franceschini, M.C.T.; Rasooly, I.R.; Ries, A.V.; Ho, L.S.; Pavlovich, W.; Santos, V.T.; Jennings, S.M.; Frick, K.D. Understanding the Food Environment in a Low-Income Urban Setting: Implications for Food Store Interventions. J. Hunger Environ. Nutr. 2008, 2, 33–50. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Suratkar, S.; Song, H.; Sacher, S.; Rajan, R.; Rasooly, I.R.; Bednarek, E.; Sharma, S.; Anliker, J.A. Process evaluation of Baltimore Healthy Stores: A pilot health intervention program with supermarkets and corner stores in Baltimore City. Health Promot. Pract. 2010, 11, 723–732. [Google Scholar] [CrossRef]
- Lee-Kwan, S.H.; Bleich, S.N.; Kim, H.; Colantuoni, E.; Gittelsohn, J. Environmental Intervention in Carryout Restaurants Increases Sales of Healthy Menu Items in a Low-Income Urban Setting. Am. J. Health Promot. AJHP 2014. [Google Scholar] [CrossRef] [PubMed]
- Shin, A.; Surkan, P.J.; Coutinho, A.J.; Suratkar, S.R.; Campbell, R.K.; Rowan, M.; Sharma, S.; Dennisuk, L.A.; Karlsen, M.; Gass, A.; et al. Impact of Baltimore Healthy Eating Zones: An Environmental Intervention to Improve Diet Among African American Youth. Health Educ. Behav. 2015, 42, 97–105. [Google Scholar] [CrossRef]
- Budd, N.; Cuccia, A.; Jeffries, J.K.; Prasad, D.; Frick, K.D.; Powell, L.; Katz, F.A.; Gittelsohn, J. B’More healthy: Retail rewards–Design of a multi-level communications and pricing intervention to improve the food environment in Baltimore City. BMC Public Health 2015, 15, 283. [Google Scholar] [CrossRef]
- Seifu, L.; Ruggiero, C.; Ferguson, M.; Mui, Y.; Lee, B.Y.; Gittelsohn, J. Simulation modeling to assist with childhood obesity control: Perceptions of Baltimore City policymakers. J. Public Health Policy 2018. [Google Scholar] [CrossRef]
- Nam, C.S.; Ross, A.; Ruggiero, C.; Ferguson, M.; Mui, Y.; Lee, B.Y.; Gittelsohn, J. Process Evaluation and Lessons Learned From Engaging Local Policymakers in the B’More Healthy Communities for Kids Trial. Health Educ. Behav. 2018. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Mui, Y.; Lin, S.; Lee, B.Y.; Seiden, A.; Gorstein, A.; Welch, P.; Bleich, S.; Igusa, T. ‘’Simulating impact of an urban farm tax credit policy in a low income urban setting,” Harvard Health Policy Review. Available online: http://hhpronline.org/simulating-the-impact-of-an-urban-farm-tax-credit-policy-in-a-low-income-urban-setting-2/ (accessed on 9 November 2018).
- Toft, U.; Bloch, P.; Reinbach, C.H.; Winkler, L.L.; Buch-Andersen, T.; Aagaard-Hansen, J.; Mikkelsen, E.B.; Jensen, B.B.; Glümer, C. Project SoL—A Community-Based, Multi-Component Health Promotion Intervention to Improve Eating Habits and Physical Activity among Danish Families with Young Children. Part 1: Intervention Development and Implementation. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef]
- Perepezko, K.; Tingey, L.; Sato, P.; Rastatter, S.; Ruggiero, C.; Gittelsohn, J. Partnering with carryouts: Implementation of a food environment intervention targeting youth obesity. Health Educ. Res. 2018, 33, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Sato, P.M.; Steeves, E.A.; Carnell, S.; Cheskin, L.J.; Trude, A.C.; Shipley, C.; Mejía Ruiz, M.J.; Gittelsohn, J. A youth mentor-led nutritional intervention in urban recreation centers: A promising strategy for childhood obesity prevention in low-income neighborhoods. Health Educ. Res. 2016, 31, 195–206. [Google Scholar] [CrossRef]
- Schwendler, T.; Shipley, C.; Budd, N.; Trude, A.; Surkan, P.J.; Anderson Steeves, E.; Sato, P.d.M.; Eckmann, T.; Loh, H.; Gittelsohn, J. Development and Implementation: B’more Healthy Communities for Kids Store and Wholesaler Intervention. Health Promot. Pract. 2017. [Google Scholar] [CrossRef]
- Loh, I.H.; Schwendler, T.; Trude, A.C.B.; Anderson Steeves, E.T.; Cheskin, L.J.; Lange, S.; Gittelsohn, J. Implementation of Text-Messaging and Social Media Strategies in a Multilevel Childhood Obesity Prevention Intervention: Process Evaluation Results. Inquiry 2018, 55. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Klesges, L.M.; Dzewaltowski, D.A.; Bull, S.S.; Estabrooks, P. The future of health behavior change research: What is needed to improve translation of research into health promotion practice? Ann. Behav. Med. 2004, 27, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Trude, A.C.B.; Kharmats, A.Y.; Jones-Smith, J.C.; Gittelsohn, J. Exposure to a multi-level multi-component childhood obesity prevention community-randomized controlled trial: Patterns, determinants, and implications. Trials 2018, 19, 287. [Google Scholar] [CrossRef]
- Trude, A.C.; Surkan, P.J.; Anderson Steeves, E.; Pollack Porter, K.; Gittelsohn, J. The impact of a multilevel childhood obesity prevention intervention on healthful food acquisition, preparation, and fruit and vegetable consumption on African-American adult caregivers. Public Health Nutr. 2018. [Google Scholar] [CrossRef]
- Butel, J.; Wilkens, L.; Nigg, C.; Braun, K.L.; Hurwitz, E.; Bersamin, A.; Leon Guerroro, R.; Coleman, P.; Fleming, T.; Novotny, R. The Relationship between Multilevel, Multisite Intervention Activities Dose and Waist Circumference and Screen Time Outcomes in The Children’s Healthy Living (CHL) Program. Presented at the Hawaii Public Health Conference, Honolulu, HI, USA, 25 October 2016. [Google Scholar]
- Healthy People 2020. Disease Prevention and Health Promotion; U.S. Department of Health and Human Services: Washington, DC, USA, 2016. Available online: https://www.healthypeople.gov/2020/pp-office/office-of-disease-prevention-and-health-promotion (accessed on 31 March 2016).
- Gibbons, C.B.; Weiss, A.F. Creating and sustaining change: Early insights from Aligning Forces. Am. J. Manag. Care 2012, 18, s96–s98. [Google Scholar]
- Scanlon, D.P.; Beich, J.; Alexander, J.A.; Christianson, J.B.; Hasnain-Wynia, R.; McHugh, M.C.; Mittler, J.N. The Aligning Forces for Quality initiative: Background and evolution from 2005 to 2012. Am. J. Manag. Care 2012, 18, 115–125. [Google Scholar]
- Slater, M.D.; Edwards, R.W.; Plested, B.A. Using Community Readiness Key Informant Assessments in a Randomized Group Prevention Trial: Impact of a Participatory Community-Media Intervention. J. Community Health 2005, 30, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Kendall, E.; Muenchberger, H.; Sunderland, N.; Harris, M.; Cowan, D. Collaborative capacity building in complex community-based health partnerships: A model for translating knowledge into action. J. Public Health Manag. Pract. 2012, 18. [Google Scholar] [CrossRef] [PubMed]
- Hohmann, A.A.; Shear, M.K. Community-based intervention research: Coping with the “noise” of real life in study design. Am. J. Psychiatry 2002, 159, 201–207. [Google Scholar] [CrossRef] [PubMed]
- de Groot, F.P.; Robertson, N.M.; Swinburn, B.A.; de Silva-Sanigorski, A.M. Increasing community capacity to prevent childhood obesity: Challenges, lessons learned and results from the Romp & Chomp intervention. BMC Public Health 2010, 10, 522. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.D.; Dietz, W. Childhood obesity: The new tobacco. Health Aff. 2010, 29, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Mercer, S.L.; Green, L.W.; Rosenthal, A.C.; Husten, C.G.; Khan, L.K.; Dietz, W.H. Possible lessons from the tobacco experience for obesity control. Am. J. Clin. Nutr. 2003, 77, 1073S–1082S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Economos, C.D.; Hyatt, R.R.; Goldberg, J.P.; Must, A.; Naumova, E.N.; Collins, J.J.; Nelson, M.E. A community intervention reduces BMI z-score in children: Shape Up Somerville first year results. Obesity 2007, 15, 1325–1336. [Google Scholar] [CrossRef]
- De Silva-Sanigorski, A.M.; Bell, a.C.; Kremer, P.; Nichols, M.; Crellin, M.; Smith, M.; Sharp, S.; De Groot, F.; Carpenter, L.; Boak, R.; et al. Reducing obesity in early childhood: Results from Romp & Chomp, an Australian community-wide intervention program. Am. J. Clin. Nutr. 2010, 91, 831–840. [Google Scholar] [CrossRef]
- McGlashan, J.; Nichols, M.; Korn, A.; Millar, L.; Marks, J.; Sanigorski, A.; Pachucki, M.; Swinburn, B.; Allender, S.; Economos, C. Social network analysis of stakeholder networks from two community-based obesity prevention interventions. PLoS ONE 2018, 13, e0196211. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Recreation Center/Peer-leader Component | Set Standard (# for optimal) |
|---|---|
| Reach | |
| # of children per session (10–14) | 10+ |
| Dose Delivered | |
| # handouts distributed/session | 12+ |
| # giveaways distributed/session | 12+ |
| # food sampled per session | 12+ |
| # types of recipes distributed (phase 2) | 3+ |
| # posts featuring youth-leaders | 3+ |
| Fidelity | |
| # of YL attending each session | 5+ |
| # of visits to after-school center/ week | 3+ |
| # of YL in corner store session/phase | 10+ |
| # of posters up at after-school center/phase | 3+ |
| # of post made by YL per phase | 3+ |
| % of YL attendance to trainings | 90% |
| # of YL actively participating | 10 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gittelsohn, J.; Novotny, R.; Trude, A.C.B.; Butel, J.; Mikkelsen, B.E. Challenges and Lessons Learned from Multi-Level Multi-Component Interventions to Prevent and Reduce Childhood Obesity. Int. J. Environ. Res. Public Health 2019, 16, 30. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010030
Gittelsohn J, Novotny R, Trude ACB, Butel J, Mikkelsen BE. Challenges and Lessons Learned from Multi-Level Multi-Component Interventions to Prevent and Reduce Childhood Obesity. International Journal of Environmental Research and Public Health. 2019; 16(1):30. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010030
Chicago/Turabian StyleGittelsohn, Joel, Rachel Novotny, Angela Cristina Bizzotto Trude, Jean Butel, and Bent Egberg Mikkelsen. 2019. "Challenges and Lessons Learned from Multi-Level Multi-Component Interventions to Prevent and Reduce Childhood Obesity" International Journal of Environmental Research and Public Health 16, no. 1: 30. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16010030