1. Introduction
Internationally, access to primary healthcare services (e.g., family doctor) has long been widely accepted as one of the primary goals in fulfilling the health needs of individuals since these are often the first point of contact in the healthcare system; providing a wide range of services over time that focus on prevention and prognosis of diseases through early diagnosis, contrary to disease-oriented care [
1,
2,
3,
4]. Statistically, as of 2016, Canada has 2.6 physicians per 1000 people, which is significantly lower than the Organization for Economic Co-operation and Development (OECD) countries’ average of 3.3 physicians per 1000 population [
5]. Lower physician availability status in Canada, compared to the international standards, is escalated by uneven distribution of population and healthcare facilities over regions. As such, access to primary healthcare continues to be a pressing research and policy issue in Canada and globally.
Despite this, the term ‘access’ is still not well-defined [
6,
7,
8,
9,
10]. The reason behind the ambiguity in defining healthcare access is that it is a multidimensional term. Access can be defined both as a noun, referring to the potential for healthcare use; and, a verb, referring to the interaction between the provider and the patient [
3,
11]. In order to better interpret access, it has been presented in terms of stages and dimensions. The two stages are ‘potential’ for healthcare and ‘realized’ service utilization, which correspond to the noun and verb definitions, respectively, of access [
3].
The progression from potential to realized access can be impeded by the presence of a number of barriers. Penchansky and Thomas (1981) group the barriers according to five dimensions: availability, accessibility, affordability, acceptability, and accommodation. The last three aforementioned dimensions comprise the aspatial factors (independent of any geographic aspect), and refer to healthcare costs, cultural attributes and communication effectiveness, respectively. The first two dimensions (availability and accessibility) contain an inherent spatial component where the former refers to the capacity of the provider and the latter refers to the travel cost between the provider and the patient [
12]. Commonly, in urban areas, where there is a provision of multiple provider service locations, availability and accessibility dimensions of access are considered in coherence. This union is referred to as ‘spatial accessibility’ [
3].
Multiple methods, and combinations of methods, have been developed to derive an effective spatial accessibility measure, including traditional measures such as straight distance and supply-to-demand ratio [
13,
14], and advanced measures, such as two-step floating catchment area [
15], three-step floating catchment area [
10,
16], and kernel density and enhanced variable two-step floating catchment area method (EV2SFCA and KD2SFCA) [
14,
17], with many others still actively under development by the research community. These measures of spatial accessibility have been extensively applied to detect non-uniform distribution of healthcare [
10,
16,
18,
19,
20,
21,
22], and to optimize access to other services such as daycares, libraries, food stores, and district building energy plan [
13,
23,
24]. Despite this growth in spatial accessibility methods, there is limited research spatial accessibility to primary healthcare by mode of transit.
When it comes to spatial access to primary healthcare, the assumption that all populations have access to a car which enables them to access the primary healthcare is highly generalized in the current measures. Car ownership is not universal. In fact, fewer people are getting their driver’s license in the global south and north due to improved public and active transportation. A study led by the University of Michigan Transportation Research Institute showed that the number of young licensed drivers has decreased in half of the 15 countries they investigated, including Canada. Specifically, between the ages of 25 to 34, 92% percent of the people had a driver’s license in 1999 and in 2009, this number dropped to 87% [
25]. Further to this point, cities are encouraging citizens to employ greater use of active transportation networks, where an effective transition requires service and amenities that are accessible—by transit, and/or walking. To more accurately understand spatial access for non-drivers, it is crucial to measure the accessibility to primary healthcare facilities by alternative modes of travel.
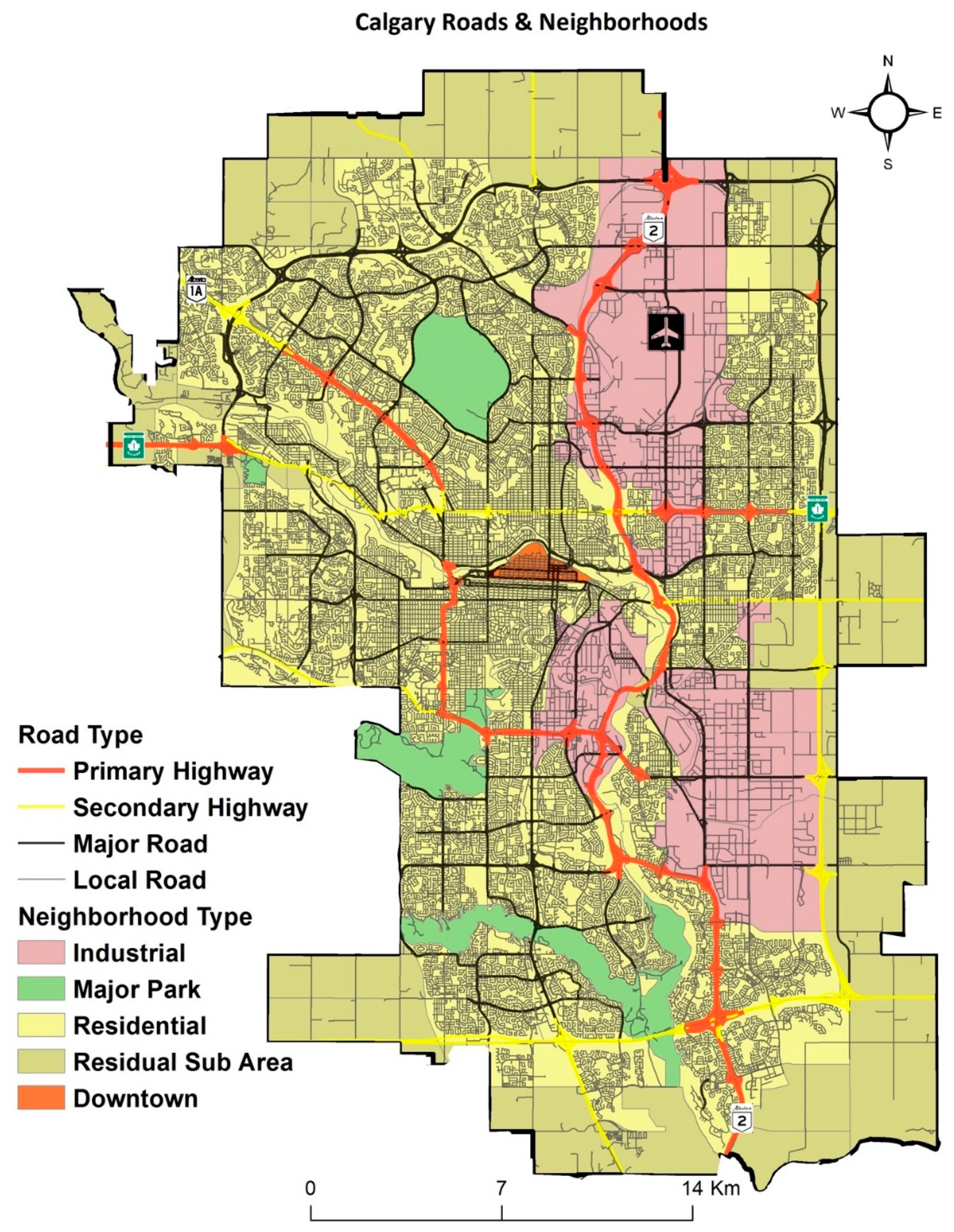
Collectively, the distribution of facilities and the spatial networks of transportation are two significant determinants of spatial accessibility of primary healthcare facilities. Realizing the importance of adequate primary healthcare and mode of transportation, this research analyzes multimodal access to primary care in the City of Calgary, Canada. First, we explore current methods of measuring access, before settling on the spatial access ratio (SPAR) method. Then, spatial accessibility to the primary healthcare facilities in the city is analyzed, using SPAR, at the community level by simulating travel on walking, multimodal, and driving-oriented networks.
3. Results
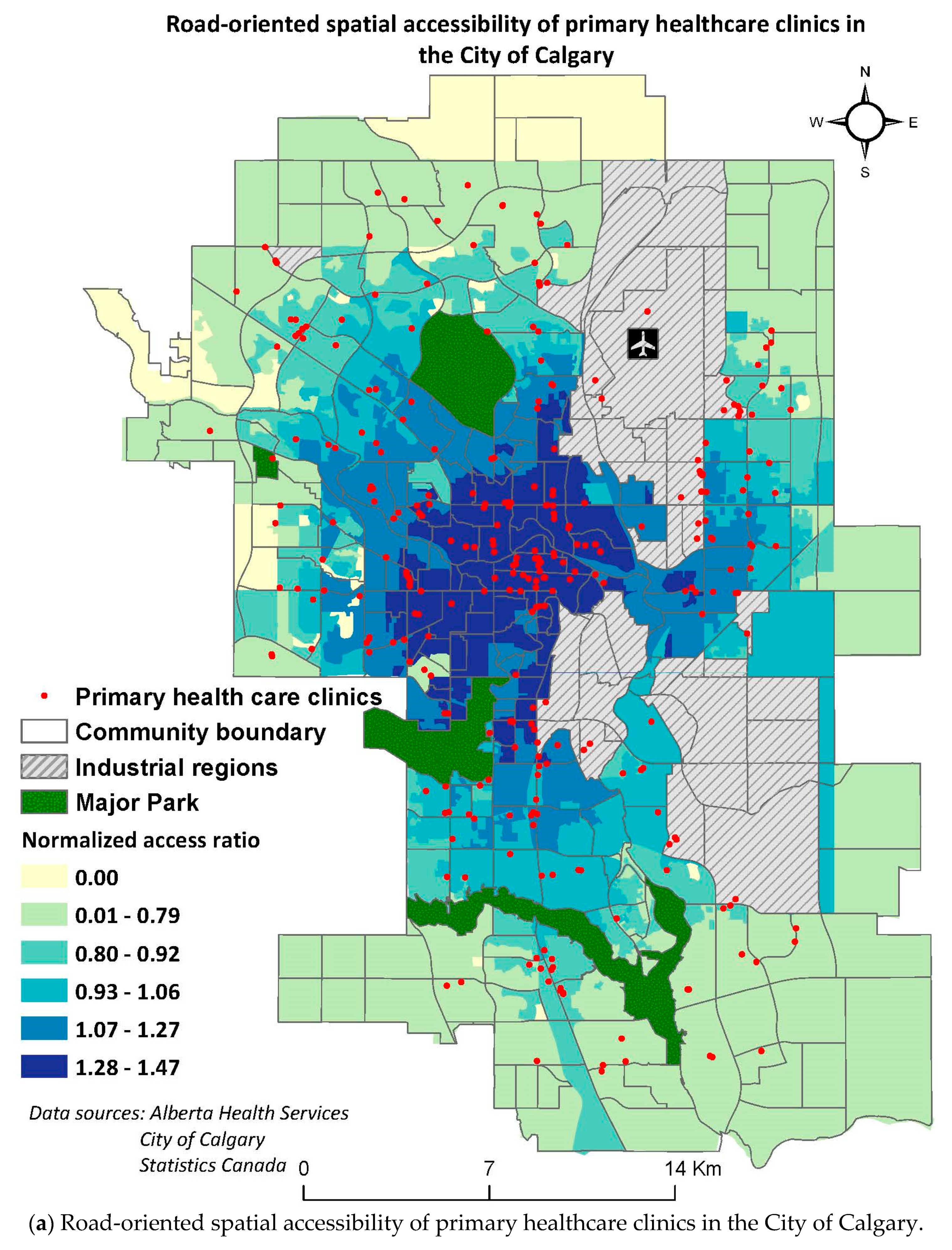
A general comparison between spatial accessibility trends by driving, multimodal means, and walking illustrate that there are higher accessibility values estimated in the urban (core) region as compared to suburban regions by all modes of travel (
Figure 5, a: road, b: multimodal, and c: walking). Additionally, the regions of high spatial accessibility are identified at the locations of the healthcare clinics for all analyses. In other words, the regions which were determined to have no accessibility were found to contain no healthcare facility in their proximity. A general comparison in travel by different modes revealed that spatial accessibility decreases when the mode of travel is changed from car to bus transit means, and reduced further by walking.
3.1. Accessibility by Driving
The greatest spatial accessibility to primary healthcare facilities in the City of Calgary was achieved by driving as compared to other modes of travel (
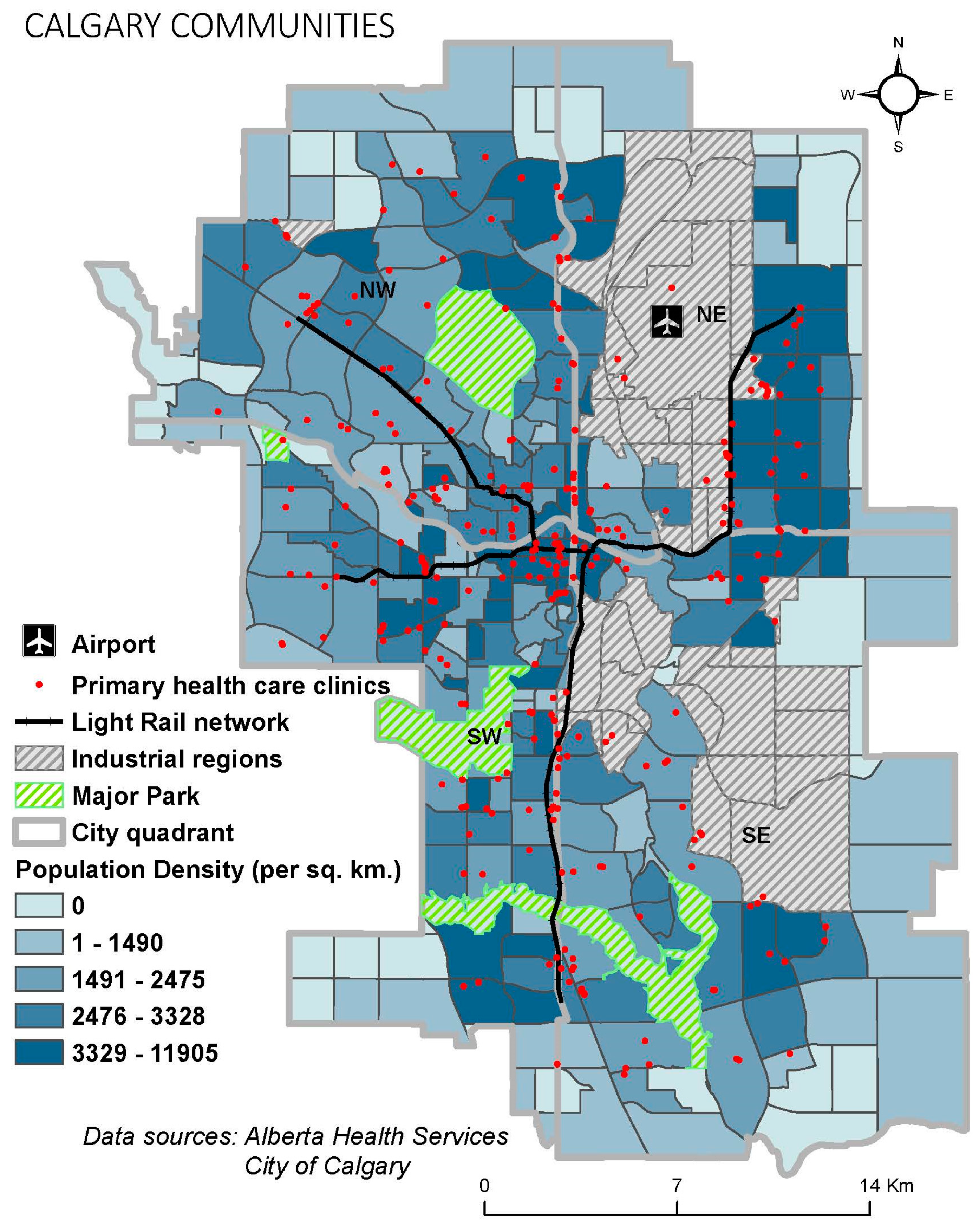
Figure 5a). The initial inspection of the access status through this mode points out the decreasing trend in accessibility as one moves from the central to the peripheral regions of the city. According to this model, precisely 24 out of 1594 DAs, with the cumulative population of 30,090 (2.4% of the total population), had no spatial accessibility to primary healthcare facilities. Most of the DAs with no accessibility were found to be located in the Northwest region of the city.
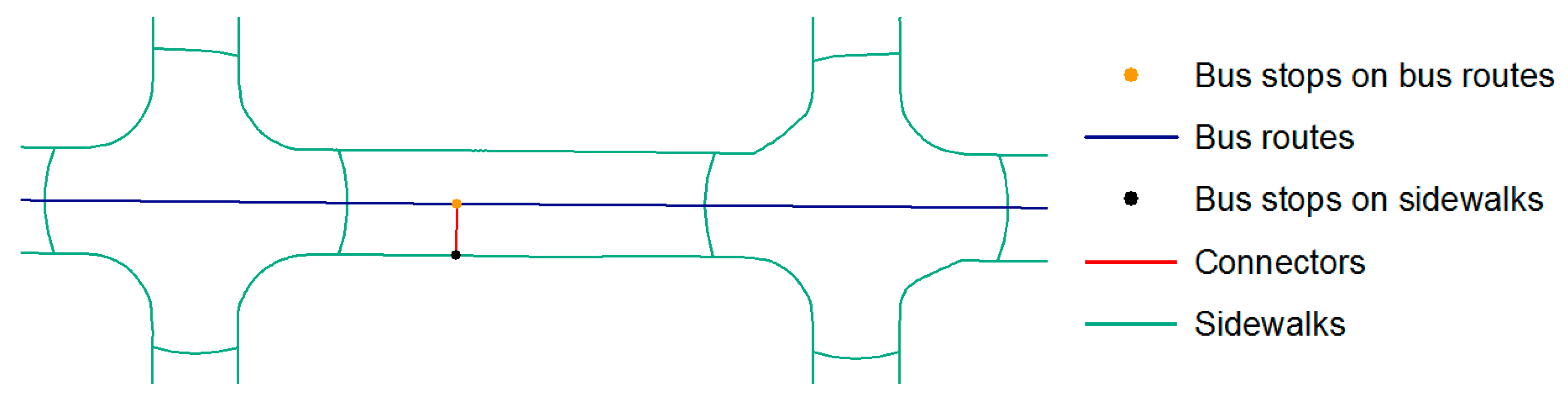
3.2. Accessibility by Multimodal Means of Travel (Sidewalks, Bus Routes and Train Lines)
As compared to driving mode, spatial accessibility by multimodal means exhibits more intra-community variations over the City of Calgary (
Figure 5b). Through this mode, the access status was observed to lie between the accessibility measured by driving and walking networks (
Figure 5a,c). Specifically, less intra-community variations are observed than measured through walking and higher intra-community variations are identified than analysis performed on driving. For the multimodal means of travel, 151 out of 1594 DAs were identified with no access to healthcare, which were dispersed in different sections of Calgary of cumulative population of 137,745 (11.1% of total population).
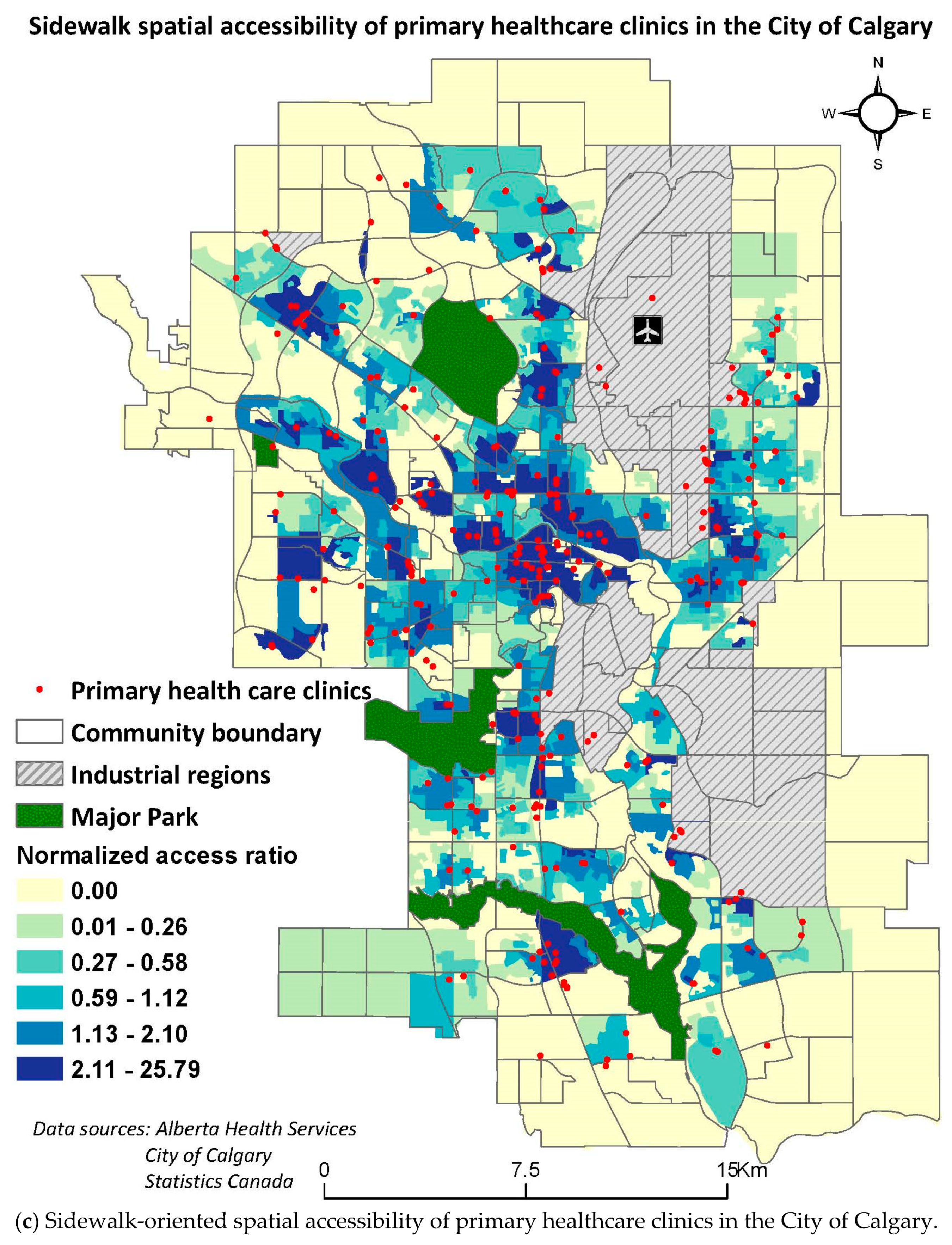
3.3. Accessibility by Walking
The spatial accessibility to the primary healthcare facilities in the City by walking (
Figure 5c), is substantially lower than that of driving or multimodal means. For this analysis, prominent intra-community variations in accessibility indices are observed. This implies that the access is not the same within the communities by walking, contradictory to the results obtained by other means. For this travel mode, 455 out of 1594 DAs were identified with no access to primary healthcare, which is home to 439,500 (35.5%) people in the city. Unlike access measured by driving mode, the regions with no accessibility can be found in all four quadrants of the city. Generally, regions with higher access are concentrated in the downtown section of the city.
3.4. Multiple Regression Analysis by Mode of Travel
The regression analysis for three modes of travel resulted in positively spatially auto-correlated residuals, implied by the high positive values of the Moran’s I statistic (
Table 4). This implies there is a spatial factor in determining the accessibility of primary healthcare facilities in the City of Calgary. This violated one of the assumptions of multiple regression. In other words, the residuals of the regression models should be independent of one another for the model to be considered valid. However, this was not the case in this research with positively auto-correlated residuals. Hence, the spatial regression analysis was performed to obtain regression results, while accounting for the spatial dependency of the nearby feature values.
For the spatial regression analysis for travel by car, four variables were determined to be significant with less than 0.05
p-value: proportion of the individuals separated, divorced, or widowed; proportion of the persons living alone; average income; and proportion of single-parent families (
Table 5).
The global spatial regression model (
Table 6) reveals that there is an inverse relationship between the spatial accessibility and the proportion of the individuals separated, divorced, or widowed. In other words, the regions with high proportion of separated, divorced, or widowed individuals have lower accessibility to primary healthcare. On the other hand, the variables which were found to have a positive relationship with the increased SPAR were found to be proportion of the persons living alone, average income, and the proportion of single-parent families. Specifically, there seems to be a mismatch between the needs and resources for primary healthcare provisions. People with higher income tend to make use of healthcare facilities more as compared to low income individuals. The possible explanations for these trends are presented in discussion.
In regards to the multimodal means analysis, variables identified to be significant were proportion of the individuals separated, divorced, or widowed; proportion of population living alone; average income; and employment-population ratio. According to the SPAR model, there is a direct relationship between the SPAR values and these variables except for proportion of the individuals separated, divorced, or widowed. As the regions of high proportion of population living alone, high average income, and high employment-population ratio increases, the SPAR value increases. On the other hand, the regions with high proportion of the individuals separated, divorced, or widowed were found to have the low SPAR values as seen in the driving mode of travel analysis. Again, possible explanations are provided in discussion.
When the mode of travel is changed to walking, the spatial regression results are different from the other two analyses. In this case, the significant variables were calculated to be proportion of the individuals separated, divorced, or widowed and proportion of people living alone. The trend between the SPAR values and these two variables is similar as observed for the SPAR analysis in other two modes of travel scenarios. The regions with high proportion of people living alone and low proportion of the individuals separated, divorced, or widowed were found in high spatial access areas (
Table 7). These trends are further discussed in the discussion section.
4. Discussion
4.1. Accessibility Status of the Primary Healthcare Facilities by Different Modes of Travel
In regard to spatial accessibility measured by all three different modes, the regions which were identified to have no spatial accessibility were found to contain no healthcare facilities in its vicinity. This implies that the spatial distribution of primary healthcare facilities is non-uniform and hence, points out the spatial disparity in terms of healthcare allocation in space. A general comparison for accessibility to primary healthcare facilities with different modes revealed that populations without access to a car have a significantly lower access ratio as compared to population who can drive (
Table 8). It is evident that both the shortage area and population served increased in number in the following order of travel mode considered: walking, multimodal (bus routes and train), and car. This implies that if the population does not have access to an automobile and relies on bus transit/train for mobility, the accessibility index of the travel to the primary healthcare facilities decreases; comparatively larger areas of the City of Calgary are found to have no accessibility to primary healthcare facilities. As a result, a higher proportion of the population of the City of Calgary is not served by the healthcare systems equally due to the distance barrier posed from limited access by public transit and walking.
Additionally, while comparing the results from different modes, it should be noted that the range of SPAR values differs among different modes. Specifically, the spatial accessibility range is lowest for the analysis by car travel (0.00–1.47). This analysis assumed that all of the population had access to a car, which resulted in the increasing ability to access the primary care overall. The small range implies that the assumption of universal access to a car smoothed the differences between the accessibility measures, resulting in the lower standard deviation (low variation in access in the City of Calgary). As the mode of travel is changed to multimodal (walking, bus routes, and train lines), the range increases (0.00–4.07). It can be deduced that more regional variability is identified with multi-modal network analysis as compared to the car analysis. This might have resulted from the kind of infrastructure in place that not all roads are bus routes, resulting in limiting choices of the primary healthcare facilities to the population to regions where bus service or the train lines are available. Another rationality behind this greater variation in access over space might be the unavailability of sidewalk infrastructure in non-core regions of the City of Calgary, resulting in limited access to the facilities. Further, the regional variability is highest for the walkability analysis (0.00–25.79). It is inferred that this would have resulted from the lower speed of pedestrians as compared to speeds in other travel models, concluding in higher spatial differences in the final output.
4.2. Relationship between Spatial Accessibility and Social Determinants of Health
The regression analysis between the accessibility index and the social determinants of health provided different results for each mode of travel. The aim of regression analysis was to detect any regions with low accessibility, where the vulnerable population is residing. There were two significant variables that were consistent among the three analyses: proportion of people living alone and proportion of the individuals separated, divorced, or widowed. This points out the mismatch between the needs and resources in primary healthcare provision. Specifically, it is important to determine the areas where there is a greater proportion of the individuals separated, divorced, or widowed, as these areas were found to have low access. Two key limitations were identified relating to the accuracy of travels speeds and actual car use, and employment status of the doctors. The same evaluation was used for all the features in travel networks; whereas, different elevation can result in travel at different speeds. Because of Calgary’s location in the foothills of the Rocky Mountains, the elevation varies from one place to another. We also did not consider time delays at intersections, leading to variations in travel speeds. Since the analyses were conducted on the travel time, not considering the elevation and delay times at intersections might not have truly captured the real-time spatial accessibility status of primary care in the city of Calgary. We also did not consider the status of access to a car through ownership, compared to new approaches to mobility such as car sharing, which in future studies, could be analyzed and paired with the access results. Another limitation is that the number of Full-Time Equivalent physicians, service hours, and days of clinics’ workings were not considered in the analysis. This information is crucial in determining whether the facility is capable of providing services. Ignoring these variables in the analysis might lead to inaccurate results regarding the availability of primary care in the city. There is also a lack of consideration of the general public’s perception on their accessibility status to primary healthcare facilities in this analysis. Qualitative data on the public’s perception of access and quantitative determination of access as performed in this analysis can be compared to obtain a holistic view of spatial accessibility to primary healthcare facilities in the City of Calgary.
Regardless of the limitations, it is important to consider the findings of this study to advocate for access for all populations regardless of socio-economic factors, such as access to a vehicle. The underlying purpose of this research was to examine the current situation of primary healthcare status in regards to clinic location, the population ability to access them, and the mode of travel used to travel to the healthcare services. An important next step would be to consider these factors to target future services to areas with the lowest (and in some cases nonexistent) access.
5. Conclusions
This research points out one of the biggest gaps in healthcare accessibility studies to date. The problem persists as most of the studies are conducted on the assumption of universal access to car. Specifically, in urban areas, a major proportion of people rely exclusively on public transportation for travel; serving as the motivation of this research. Specifically, we compared the effectiveness of different modes of travel in regard to accessibility to the primary healthcare facilities in the City of Calgary. People with access to a car were found to have the highest level of spatial accessibility to primary healthcare facilities in the city, with only 2.5% of the population in the shortage area. On the other hand, limited access was found for people relying on public transportation for accessing healthcare (11.1% of the population) and the lowest access was identified when the mode of travel was changed to walking only—over one third of the population (35.5%) reside in the shortage area. In other words, the social disparity in access to healthcare facilities was identified to be 14 times higher for people without access to a car. The regression analysis showed that the low-income regions corresponded to high access values. These were consistent with the previous research pointing out that people residing in low-income neighborhoods tend to utilize more healthcare services. Other variables were not consistent throughout different modes of travel analysis.
It is concluded that in the City of Calgary more primary healthcare facilities are required to be located in under-served areas or the pedestrian, or public transportation infrastructure needs to be improved—or ideally both. This study is important as it advocates for access without financial, environmental and ethical barriers as no person should have limited access to health due to not having an access to a private vehicle as everyone has an equal right to proper healthcare access. It can be deduced from the accessibility outputs that large portions of the City of Calgary have a low walking and public transit access. An effective solution to this problem might be to lessen the zoning restriction in certain communities to accommodate more primary healthcare facilities in the City of Calgary. Alternatively, walkability can be improved overall if the pedestrian infrastructure is enhanced in the City of Calgary. These changes are expected to improve the overall access to primary healthcare.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}