Public Facility Utility and Third-Hand Smoking Exposure without First and Second-Hand Smoking According to Urinary Cotinine Level


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Variables
2.3. UCC
2.4. Statistical Analysis
3. Results
4. Discussion
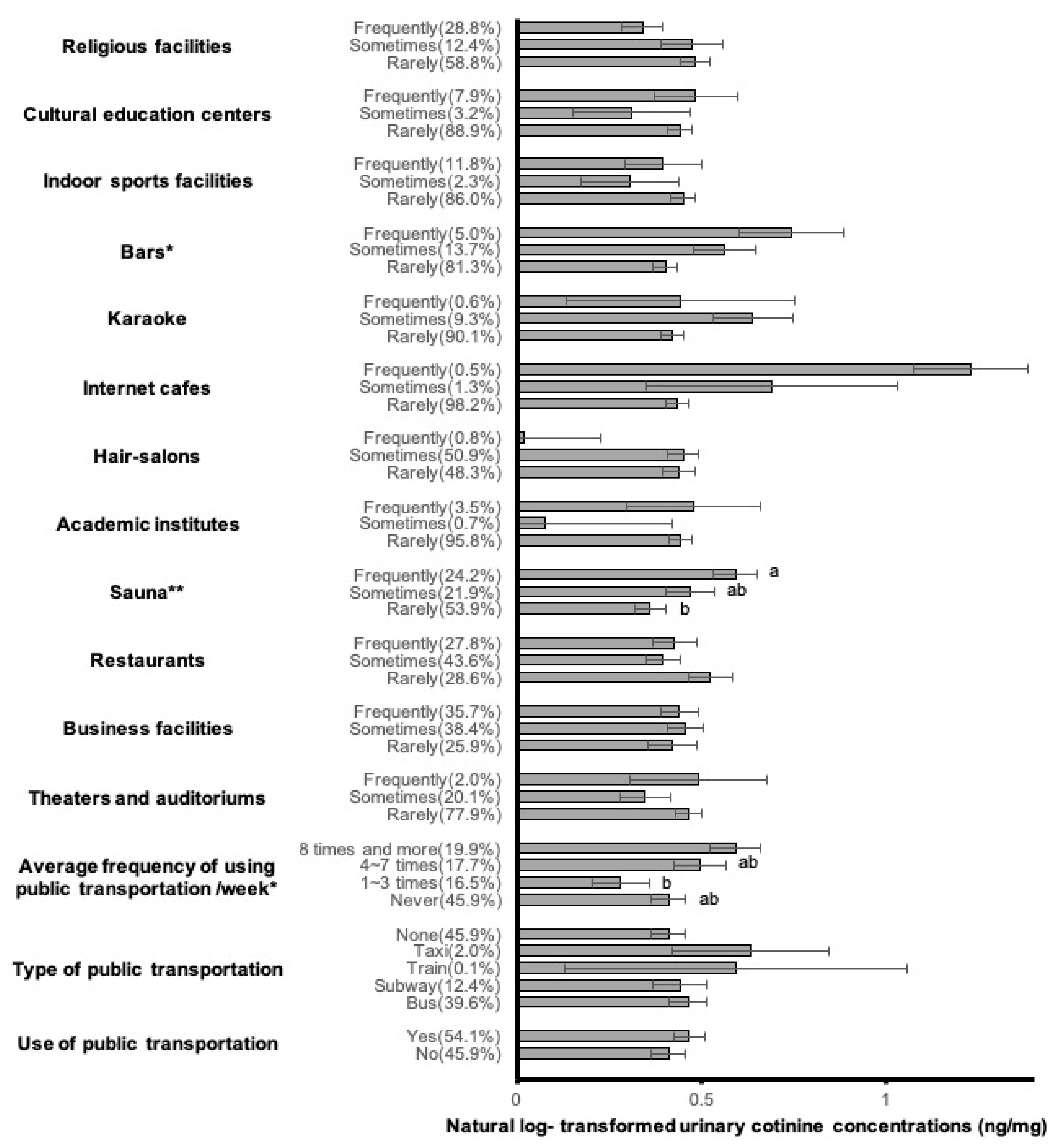
4.1. Frequencies of Public Facility Use
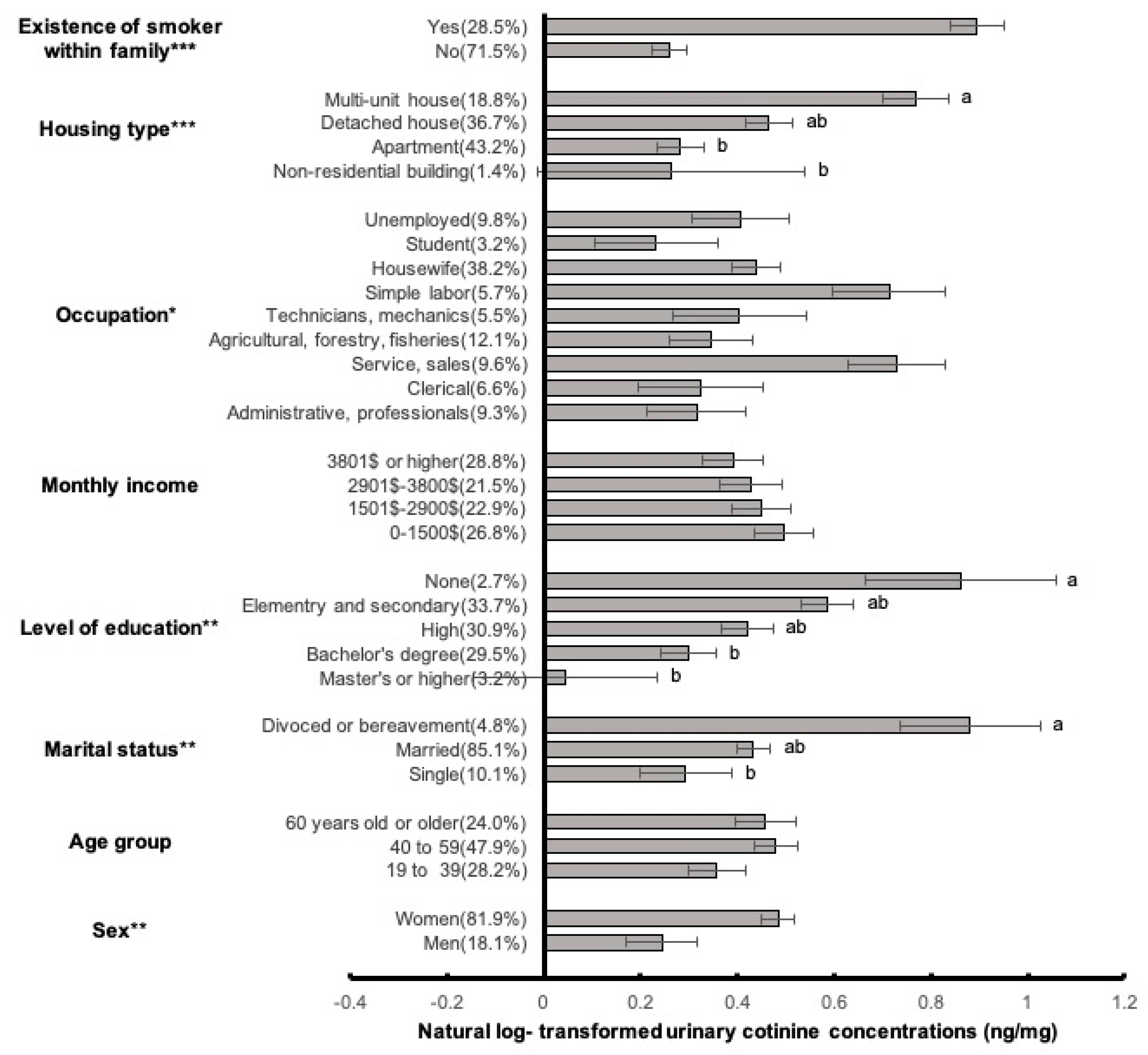
4.2. Socio-Demographic Factors
4.3. Limitations
4.4. Study Strengths
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rodgman, A.; Perfetti, T.A. The Chemical Components of Tobacco and Tobacco Smoke; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Swan, G.E.; Lessov-Schlaggar, C.N. The effects of tobacco smoke and nicotine on cognition and the brain. Neuropsychol. Rev. 2007, 17, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.E.; Zakarian, J.M.; Hoh, E.; Hovell, M.F.; Mahabee-Gittens, M.; Watanabe, K.; Datuin, K.; Vue, C.; Chatfield, D.A. When smokers quit: Exposure to nicotine and carcinogens persists from thirdhand smoke pollution. Tob. Control 2016, 26, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Health, U.D.o.; Services, H. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; US Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006; Volume 709.
- Acuff, L.; Fristoe, K.; Hamblen, J.; Smith, M.; Chen, J. Third-Hand Smoke: Old Smoke, New Concerns. J. Community Health 2016, 41, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, P., III; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand tobacco smoke: Emerging evidence and arguments for a multidisciplinary research agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Becquemin, M.H.; Bertholon, J.F.; Bentayeb, M.; Attoui, M.; Ledur, D.; Roy, F.; Roy, M.; Annesi-Maesano, I.; Dautzenberg, B. Third-hand smoking: Indoor measurements of concentration and sizes of cigarette smoke particles after resuspension. Tob. Control 2010, 19, 347–348. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, M.; Gundel, L.A.; Pankow, J.F.; Jacob, P.; Singer, B.C.; Destaillats, H. Formation of carcinogens indoors by surface-mediated reactions of nicotine with nitrous acid, leading to potential thirdhand smoke hazards. Proc. Natl. Acad. Sci. USA 2010, 107, 6576–6581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins-Green, M.; Adhami, N.; Frankos, M.; Valdez, M.; Goodwin, B.; Lyubovitsky, J.; Dhall, S.; Garcia, M.; Egiebor, I.; Martinez, B. Cigarette smoke toxins deposited on surfaces: Implications for human health. PLoS ONE 2014, 9, e86391. [Google Scholar] [CrossRef]
- Hang, B.; Wang, Y.; Huang, Y.; Wang, P.; Langley, S.A.; Bi, L.; Sarker, A.H.; Schick, S.F.; Havel, C.; Jacob, P.; et al. Short-term early exposure to thirdhand cigarette smoke increases lung cancer incidence in mice. Clin. Sci. 2018, 132, 475–488. [Google Scholar] [CrossRef]
- Jacob, P., 3rd; Benowitz, N.L.; Destaillats, H.; Gundel, L.; Hang, B.; Martins-Green, M.; Matt, G.E.; Quintana, P.J.; Samet, J.M.; Schick, S.F.; et al. Thirdhand Smoke: New Evidence, Challenges, and Future Directions. Chem. Res. Toxicol. 2017, 30, 270–294. [Google Scholar] [CrossRef]
- Sleiman, M.; Logue, J.M.; Luo, W.; Pankow, J.F.; Gundel, L.A.; Destaillats, H. Inhalable constituents of thirdhand tobacco smoke: Chemical characterization and health impact considerations. Environ. Sci. Technol. 2014, 48, 13093–13101. [Google Scholar] [CrossRef]
- Jung, J.W.; Ju, Y.S.; Kang, H.R. Association between parental smoking behavior and children’s respiratory morbidity: 5-year study in an urban city of South Korea. Pediatr. Pulmonol. 2012, 47, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Protano, C.; Andreoli, R.; Manini, P.; Vitali, M. How home-smoking habits affect children: A cross-sectional study using urinary cotinine measurement in Italy. Int. J. Public Health 2012, 57, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.; Quintana, P.; Hovell, M.; Bernert, J.; Song, S.; Novianti, N.; Juarez, T.; Floro, J.; Gehrman, C.; Garcia, M. Households contaminated by environmental tobacco smoke: Sources of infant exposures. Tob. Control 2004, 13, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.; Zakarian, J.M.; Fortmann, A.L.; Chatfield, D.A.; Hoh, E.; Uribe, A.M.; Hovell, M.F. When smokers move out and non-smokers move in: Residential thirdhand smoke pollution and exposure. Tob. Control 2011, 20, e1. [Google Scholar] [CrossRef] [PubMed]
- Quintana, P.J.; Matt, G.E.; Chatfield, D.; Zakarian, J.M.; Fortmann, A.L.; Hoh, E. Wipe sampling for nicotine as a marker of thirdhand tobacco smoke contamination on surfaces in homes, cars, and hotels. Nicotine Tob. Res. 2013, 15, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Syamlal, G.; Mazurek, J.M.; Hendricks, S.A.; Jamal, A. Cigarette smoking trends among US working adult by industry and occupation: Findings from the 2004–2012 National Health Interview Survey. Nicotine Tob. Res. 2014, 17, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.; Hovell, M.F.; Chatfield, D.; Ma, D.S.; Romero, R.; Uribe, A. Residual tobacco smoke pollution in used cars for sale: Air, dust, and surfaces. Nicotine Tob. Res. 2008, 10, 1467–1475. [Google Scholar] [CrossRef]
- Park, J.H.; Lee, C.K.; Kim, K.H.; Son, B.C.; Kim, J.H.; Suh, C.H.; Kim, S.Y.; Yu, S.D.; Kim, S.J.; Choi, W.H.; et al. Decrease in the urine cotinine concentrations of Korean non-smokers between 2009 and 2011 following implementation of stricter smoking regulations. Int. J. Hyg. Environ. Health 2016, 219, 123–128. [Google Scholar] [CrossRef]
- Kim, J.; Lee, K. Characterization of urinary cotinine in non-smoking residents in smoke-free homes in the Korean National Environmental Health Survey (KoNEHS). BMC Public Health 2016, 16, 538. [Google Scholar] [CrossRef]
- Guak, S.; Lee, K.; Kim, S.; Kim, S.; Yang, W.; Ha, K. Impact of the smoke-free law on secondhand smoke in computer game rooms. Korean J. Environ. Health Sci. 2015, 41, 11–16. [Google Scholar] [CrossRef]
- Lee, K.; Hahn, E.J.; Robertson, H.E.; Whitten, L.; Jones, L.K.; Zahn, B. Air quality in and around airport enclosed smoking rooms. Nicotine Tob. Res. 2010, 12, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Alevantis, L.E.; Offermann, F.J. A survey of environmental tobacco smoke controls in California office buildings. Indoor Air 2001, 11, 26–34. [Google Scholar] [PubMed]
- Jones, M.R.; Wipfli, H.; Shahrir, S.; Avila-Tang, E.; Samet, J.M.; Breysse, P.N.; Navas-Acien, A. Secondhand tobacco smoke: An occupational hazard for smoking and non-smoking bar and nightclub employees. Tob. Control 2013, 22, 308–314. [Google Scholar] [CrossRef] [PubMed]
- St. Helen, G.; Bernert, J.T.; Hall, D.B.; Sosnoff, C.S.; Xia, Y.; Balmes, J.R.; Vena, J.E.; Wang, J.-S.; Holland, N.T.; Naeher, L.P. Exposure to Secondhand Smoke Outside of a Bar and a Restaurant and Tobacco Exposure Biomarkers in Nonsmokers. Environ. Health Perspect. 2012, 120, 1010–1016. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.-J.; Khang, Y.-H.; Jun, H.-J.; Kawachi, I. Marital status and smoking in Korea: The influence of gender and age. Soc. Sci. Med. 2008, 66, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Nystedt, P. Marital life course events and smoking behaviour in Sweden 1980–2000. Soc. Sci. Med. 2006, 62, 1427–1442. [Google Scholar] [CrossRef] [Green Version]
- Altindag, D.; Cannonier, C.; Mocan, N. The impact of education on health knowledge. Econ. Educ. Rev. 2011, 30, 792–812. [Google Scholar] [CrossRef]
- King, B.A.; Travers, M.J.; Cummings, K.M.; Mahoney, M.C.; Hyland, A.J. Secondhand smoke transfer in multiunit housing. Nicotine Tob. Res. 2010, 12, 1133–1141. [Google Scholar] [CrossRef]
- MOLIT. A Survey on Residential Conditions; Ministry of Land, Infrastructure and Transport of South Korea: Sejong-si, Korea, 2017.
- Bonevski, B.; Regan, T.; Paul, C.; Baker, A.L.; Bisquera, A. Associations between alcohol, smoking, socioeconomic status and comorbidities: Evidence from the 45 and U p S tudy. Drug Alcohol Rev. 2014, 33, 169–176. [Google Scholar] [CrossRef]
- Syamlal, G.; Mazurek, J.M.; Dube, S.R. Gender Differences in Smoking among U.S. Working Adults. Am. J. Prev. Med. 2014, 47, 467–475. [Google Scholar] [CrossRef]
- Amos, A.; Greaves, L.; Nichter, M.; Bloch, M. Women and tobacco: A call for including gender in tobacco control research, policy and practice. Tob. Control 2012, 21, 236–243. [Google Scholar] [CrossRef]
- Bang, K.M.; Kim, J.H. Prevalence of cigarette smoking by occupation and industry in the United States. Am. J. Ind. Med. 2001, 40, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Protano, C.; Avino, P.; Manigrasso, M.; Vivaldi, V.; Perna, F.; Valeriani, F.; Vitali, M. Environmental Electronic Vape Exposure from Four Different Generations of Electronic Cigarettes: Airborne Particulate Matter Levels. Int. J. Environ. Res. Public. Health 2018, 15, 2172. [Google Scholar] [CrossRef] [PubMed]
- Protano, C.; Manigrasso, M.; Avino, P.; Vitali, M. Second-hand smoke generated by combustion and electronic smoking devices used in real scenarios: Ultrafine particle pollution and age-related dose assessment. Environ. Int. 2017, 107, 190–195. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Socio-Demographics | n (%) | GM (±SD) |
|---|---|---|
| Total | 1360 (100%) | 1.55 (±6.57) |
| Sex | ||
| Male | 246 (18.1%) | 1.28 (±4.90) |
| Female | 1114 (81.9%) | 1.62 (±6.88) |
| Age group | ||
| 19 to 39 | 383 (28.2%) | 1.43 (±5.44) |
| 40 to 59 | 651 (47.9%) | 1.62 (±7.33) |
| 60 years old or older | 326 (24.0%) | 1.58 (±6.17) |
| Marital status | ||
| Single | 138 (10.1%) | 1.34 (±4.05) |
| Married | 1157 (85.1%) | 1.54 (±6.83) |
| Divorced or bereaved | 65 (4.8%) | 2.41 (±5.99) |
| Level of education | ||
| Masters or higher | 44 (3.2%) | 1.04 (±5.52) |
| Bachelor’s degree | 401 (29.5%) | 1.35 (±5.79) |
| High school | 420 (30.9%) | 1.52 (±4.74) |
| Elementary and secondary | 458 (33.7%) | 1.80 (±8.42) |
| None | 37 (2.7%) | 2.37 (±6.99) |
| Monthly income | ||
| $0~$1500 | 364 (26.8%) | 1.64 (±4.81) |
| $1501~$2900 | 312 (22.9%) | 1.57 (±4.94) |
| $2901~$3800 | 292 (21.5%) | 1.53 (±10.24) |
| $3801 or higher | 392 (28.8%) | 1.48 (±5.56) |
| Occupation | ||
| Student | 43 (3.2%) | 1.26 (±1.64) |
| Administrative or professionals | 127 (9.3%) | 1.37 (±4.60) |
| Clerical | 90 (6.6%) | 1.38 (±6.97) |
| Agricultural, forestry, or fisheries | 165 (12.1%) | 1.41 (±4.18) |
| Technicians or mechanics | 75 (5.5%) | 1.50 (±5.05) |
| Unemployed | 133 (9.8%) | 1.50 (±3.37) |
| Housewife | 520 (38.2%) | 1.55 (±7.96) |
| Simple labor | 77 (5.7%) | 2.04 (±5.39) |
| Service and sales | 130 (9.6%) | 2.07 (±8.73) |
| Housing type | ||
| Non-residential building | 19 (1.4%) | 1.30 (±1.93) |
| Apartment | 587 (43.2%) | 1.33 (±5.59) |
| Detached house | 499 (36.7%) | 1.59 (±7.78) |
| Multiunit house | 255 (18.8%) | 2.16 (±6.04) |
| Existence of smoker within family | ||
| No | 973 (71.5%) | 1.30 (±6.32) |
| Yes | 387 (28.5%) | 2.45 (±6.96) |
| Public Facilities | n (%) | GM (±SD) |
|---|---|---|
| Use of public transportation | ||
| No | 624 (45.9%) | 1.51 (±6.30) |
| Yes | 736 (54.1%) | 1.59 (±6.80) |
| Type of public transportation | ||
| Bus | 539 (39.6%) | 1.59 (±7.59) |
| Subway | 168 (12.4%) | 1.55 (±3.84) |
| Train | 2 (0.1%) | 1.81 (±1.23) |
| Taxi | 27 (2.0%) | 1.88 (±3.78) |
| None | 624 (45.9%) | 1.51 (±6.30) |
| Average frequency of using public transportation per week | ||
| Never | 624 (45.9%) | 1.51 (±6.30) |
| 1~3 times | 225 (16.5%) | 1.32 (±3.88) |
| 4~7 times | 241 (17.7%) | 1.64 (±8.58) |
| 8 times and more | 270 (19.9%) | 1.81 (±6.88) |
| Theaters and auditoriums | ||
| Rarely | 1060 (77.9%) | 1.59 (±6.91) |
| Sometimes | 273 (20.1%) | 1.41 (±5.40) |
| Frequently | 27 (2.0%) | 1.63 (±2.41) |
| Business facilities | ||
| Rarely | 352 (25.9%) | 1.52 (±7.42) |
| Sometimes | 522 (38.4%) | 1.58 (±4.89) |
| Frequently | 486 (35.7%) | 1.55 (±7.44) |
| Restaurants | ||
| Rarely | 389 (28.6%) | 1.69 (±6.80) |
| Sometimes | 593 (43.6%) | 1.48 (±5.31) |
| Frequently | 378 (27.8%) | 1.53 (±7.97) |
| Sauna | ||
| Rarely | 733 (53.9%) | 1.43 (±6.90) |
| Sometimes | 298 (21.9%) | 1.60 (±5.84) |
| Frequently | 329 (24.2%) | 1.81 (±6.46) |
| Academic institutes | ||
| Rarely | 1303 (95.8%) | 1.55 (±5.80) |
| Sometimes | 9 (0.7%) | 1.08 (±2.06) |
| Frequently | 48 (3.5%) | 1.61 (±17.64) |
| Hair-salons | ||
| Rarely | 657 (48.3%) | 1.55 (±7.23) |
| Sometimes | 692 (50.9%) | 1.57 (±5.93) |
| Frequently | 11 (0.8%) | 1.02 (±0.76) |
| Internet cafes | ||
| Rarely | 1336 (98.2%) | 1.54 (±6.60) |
| Sometimes | 17 (1.3%) | 1.99 (±5.18) |
| Frequently | 7 (0.5%) | 3.41 (±1.44) |
| Karaoke | ||
| Rarely | 1226 (90.1%) | 1.52 (±5.69) |
| Sometimes | 126 (9.3%) | 1.89 (±12.26) |
| Frequently | 8 (0.6%) | 1.55 (±1.86) |
| Bars | ||
| Rarely | 1106 (81.3%) | 1.49 (±6.31) |
| Sometimes | 186 (13.7%) | 1.75 (±7.26) |
| Frequently | 68 (5.0%) | 2.10 (±8.36) |
| Indoor sports facilities | ||
| Rarely | 1169 (86.0%) | 1.57 (±5.73) |
| Sometimes | 31 (2.3%) | 1.36 (±1.25) |
| Frequently | 160 (11.8%) | 1.48 (±11.24) |
| Cultural education centers | ||
| Rarely | 1209 (88.9%) | 1.55 (±6.42) |
| Sometimes | 44 (3.2%) | 1.36 (±4.42) |
| Frequently | 107 (7.9%) | 1.62 (±8.70) |
| Religious facilities | ||
| Rarely | 799 (58.8%) | 1.62 (±7.11) |
| Sometimes | 169 (12.4%) | 1.61 (±8.29) |
| Frequently | 392 (28.8%) | 1.40 (±4.10) |
| Covariates | Exp. (β) | Exp (SE) | Exp CI (95%) | p-Value |
|---|---|---|---|---|
| Average frequency of using public transportation/week | ||||
| Never | 1.00 | |||
| 1–3 times | 0.89 | 0.08 | (0.75, 1.05) | 0.164 |
| 4–7 times | 1.07 | 0.08 | (0.91, 1.26) | 0.419 |
| 8 times and more | 1.25 | 0.08 | (1.07, 1.47) | 0.006 |
| Sauna | ||||
| Rarely | 1.00 | |||
| Sometimes (1–3 times per month) | 1.09 | 0.07 | (0.95, 1.27) | 0.231 |
| Frequently (1–7 times per week) | 1.16 | 0.07 | (1.00, 1.34) | 0.043 |
| Internet cafes | ||||
| Rarely | 1.00 | |||
| Sometimes (1–3 times per month) | 1.29 | 0.28 | (0.75, 2.21) | 0.358 |
| Frequently (1–7 times per week) | 2.87 | 0.42 | (1.26, 6.56) | 0.012 |
| Bar | ||||
| Rarely | 1.00 | |||
| Sometimes (1–3 times per month) | 1.23 | 0.09 | (1.03, 1.47) | 0.02 |
| Frequently (1–7 times per week) | 1.59 | 0.14 | (1.21, 2.10) | 0.001 |
| Marital status | ||||
| Single | 1.00 | |||
| Married | 1.26 | 0.12 | (1.00, 1.58) | 0.048 |
| Divorced or bereavement | 1.74 | 0.18 | (1.22, 2.47) | 0.002 |
| Level of education | ||||
| Masters or higher | 1.00 | |||
| Bachelor’s degree | 1.14 | 0.17 | (0.81, 1.60) | 0.451 |
| High school | 1.28 | 0.17 | (0.91, 1.79) | 0.154 |
| Elementary and secondary | 1.52 | 0.17 | (1.08, 2.13) | 0.016 |
| None | 1.99 | 0.24 | (1.24, 3.21) | 0.005 |
| Existence of smoker within family | ||||
| No | 1.00 | |||
| Yes | 1.82 | 0.07 | (1.60, 2.07) | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moon, S.Y.; Kim, T.W.; Kim, Y.-J.; Kim, Y.; Kim, S.Y.; Kang, D. Public Facility Utility and Third-Hand Smoking Exposure without First and Second-Hand Smoking According to Urinary Cotinine Level. Int. J. Environ. Res. Public Health 2019, 16, 855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050855
Moon SY, Kim TW, Kim Y-J, Kim Y, Kim SY, Kang D. Public Facility Utility and Third-Hand Smoking Exposure without First and Second-Hand Smoking According to Urinary Cotinine Level. International Journal of Environmental Research and Public Health. 2019; 16(5):855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050855
Chicago/Turabian StyleMoon, Si Yun, Tae Won Kim, Yoon-Ji Kim, Youngki Kim, Se Yeong Kim, and Dongmug Kang. 2019. "Public Facility Utility and Third-Hand Smoking Exposure without First and Second-Hand Smoking According to Urinary Cotinine Level" International Journal of Environmental Research and Public Health 16, no. 5: 855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16050855