Plasma Soluble Urokinase-Type Plasminogen Activator Receptor Level as a Predictor of the Severity of Community-Acquired Pneumonia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement of Plasma suPAR
2.3. Cell and Cell Culture
2.4. Western Blot Analysis
2.5. Immunofluorescence Staining
2.6. Statistical Analysis
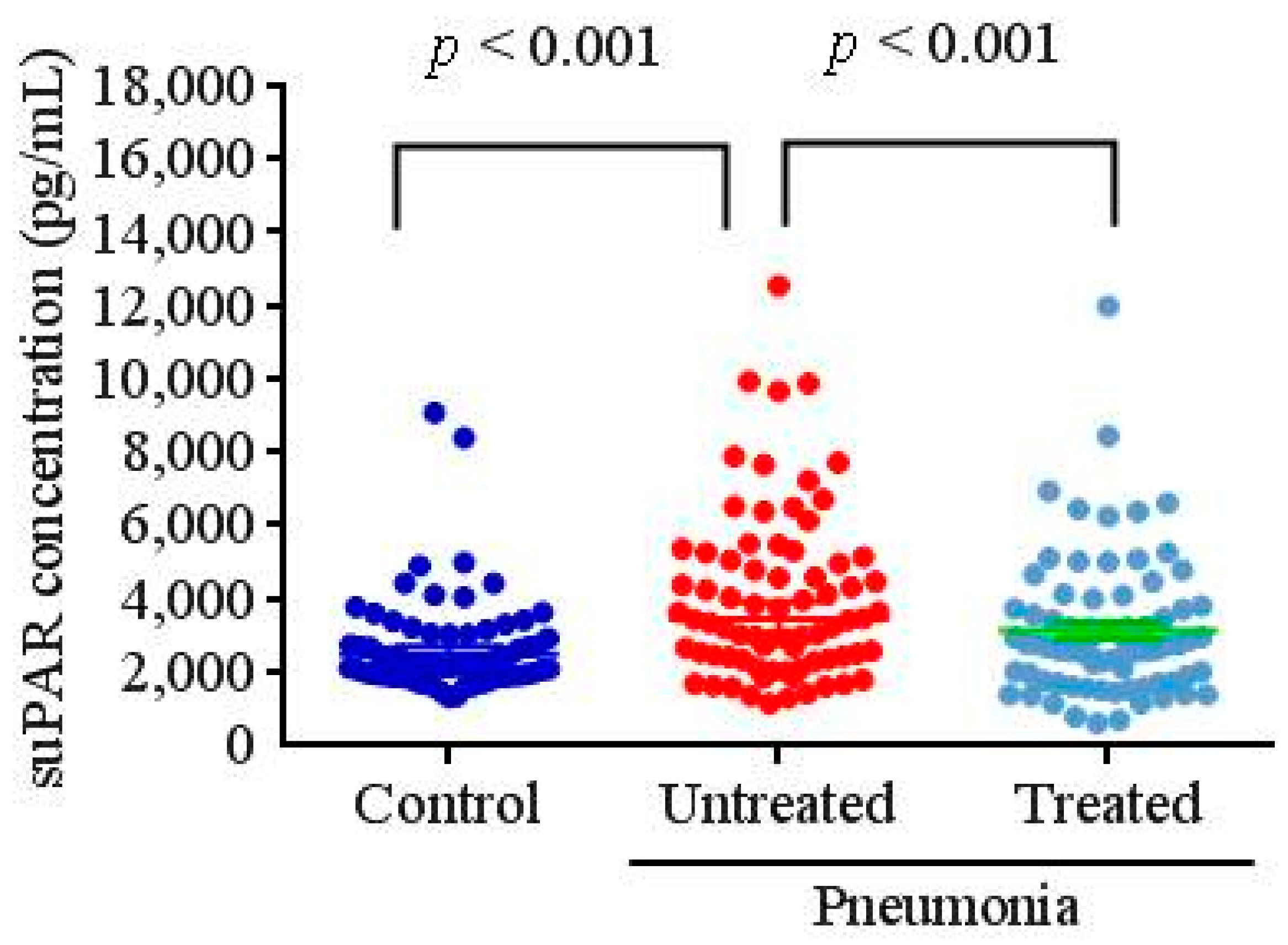
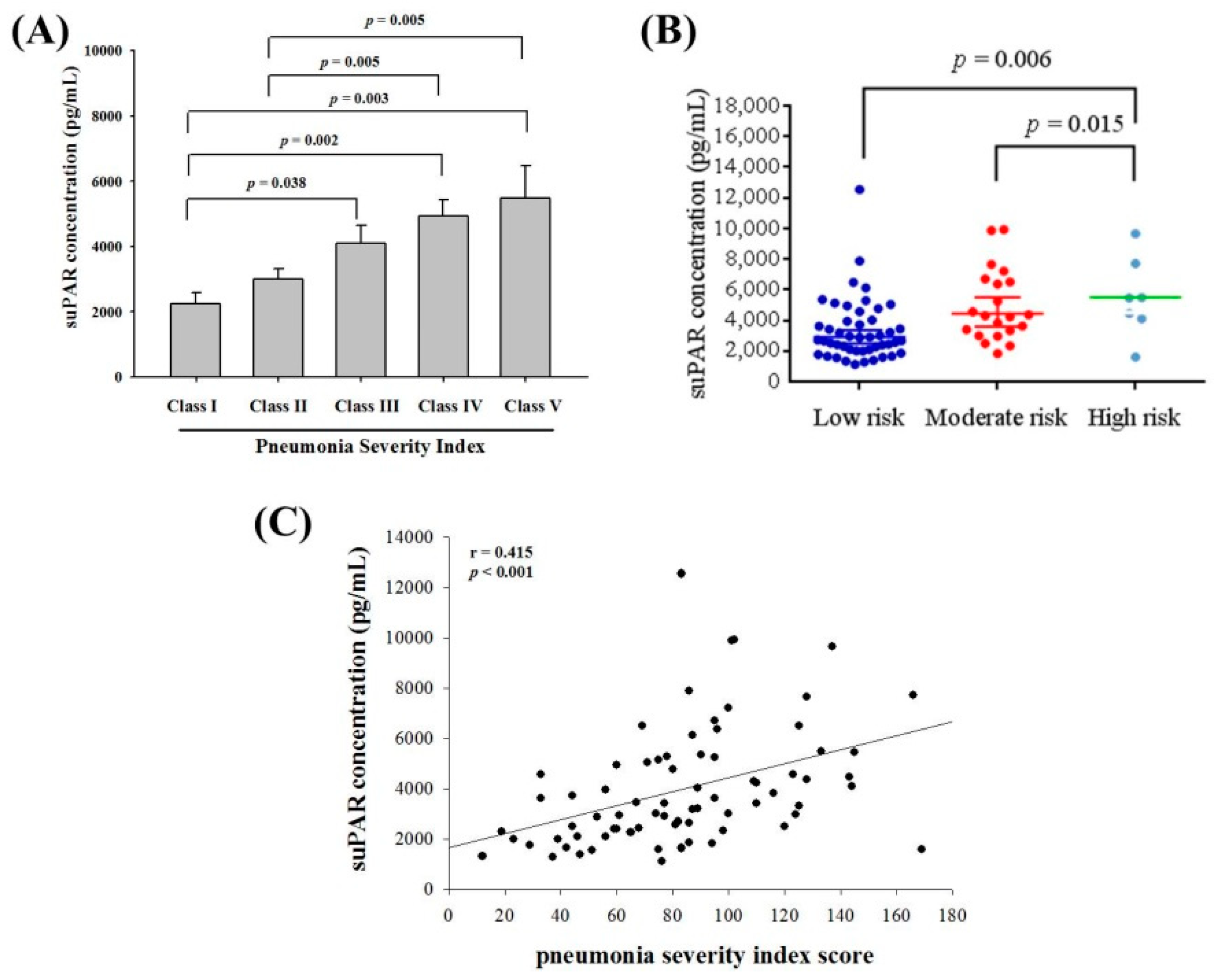
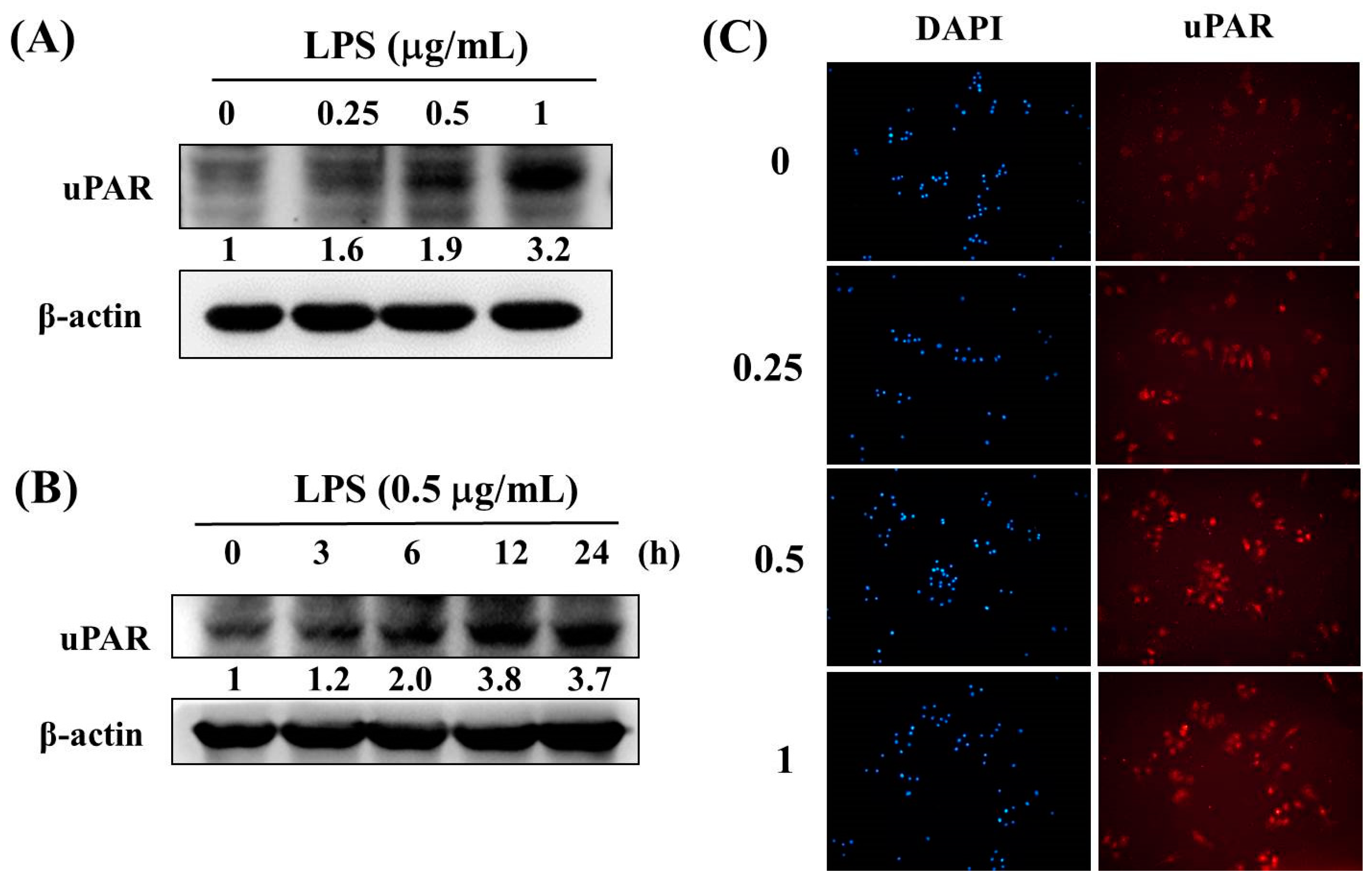
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Su, S.C.; Lin, C.W.; Yang, W.E.; Fan, W.L.; Yang, S.F. The urokinase-type plasminogen activator (upa) system as a biomarker and therapeutic target in human malignancies. Expert Opin. Ther. Targets 2016, 20, 551–566. [Google Scholar] [CrossRef]
- Chu, S.C.; Yang, S.F.; Lue, K.H.; Hsieh, Y.S.; Hsiao, T.Y.; Lu, K.H. Urokinase-type plasminogen activator, receptor, and inhibitor correlating with gelatinase-b (mmp-9) contribute to inflammation in gouty arthritis of the knee. J. Rheumatol. 2006, 33, 311–317. [Google Scholar] [PubMed]
- Weng, C.J.; Lin, C.W.; Chung, T.T.; Tsai, C.M.; Chen, M.K.; Yang, S.F. Impact of upa system gene polymorphisms on the susceptibility of environmental factors to carcinogenesis and the development of clinicopathology of oral cancer. Ann. Surg. Oncol. 2011, 18, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.H.; Wang, P.H.; Lin, L.Y.; Tee, Y.T.; Chou, M.C.; Yang, S.F.; Tsai, H.T. Significantly increased concentration of soluble urokinase-type plasminogen activator receptor in the blood of patients with pelvic inflammatory disease. Clin. Chim. Acta 2013, 415, 138–144. [Google Scholar] [CrossRef]
- Liu, K.L.; Fan, J.H.; Wu, J. Prognostic role of circulating soluble upar in various cancers: A systematic review and meta-analysis. Clin. Lab. 2017, 63, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Madunic, J. The urokinase plasminogen activator system in human cancers: An overview of its prognostic and predictive role. Thromb. Haemost. 2018, 118, 2020–2036. [Google Scholar] [CrossRef]
- Enocsson, H.; Sjowall, C.; Wettero, J. Soluble urokinase plasminogen activator receptor—A valuable biomarker in systemic lupus erythematosus? Clin. Chim. Acta 2015, 444, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Dande, R.R.; Peev, V.; Altintas, M.M.; Reiser, J. Soluble urokinase receptor and the kidney response in diabetes mellitus. J. Diabetes Res. 2017, 2017, 3232848. [Google Scholar] [CrossRef]
- Wrotek, A.; Jackowska, T. The role of the soluble urokinase plasminogen activator (supar) in children with pneumonia. Respir. Physiol. Neurobiol. 2015, 209, 120–123. [Google Scholar] [CrossRef]
- Savva, A.; Raftogiannis, M.; Baziaka, F.; Routsi, C.; Antonopoulou, A.; Koutoukas, P.; Tsaganos, T.; Kotanidou, A.; Apostolidou, E.; Giamarellos-Bourboulis, E.J.; et al. Soluble urokinase plasminogen activator receptor (supar) for assessment of disease severity in ventilator-associated pneumonia and sepsis. J. Infect. 2011, 63, 344–350. [Google Scholar] [CrossRef]
- Cilloniz, C.; Dominedo, C.; Garcia-Vidal, C.; Torres, A. Community-acquired pneumonia as an emergency condition. Curr. Opin. Crit. Care 2018, 24, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Prina, E.; Ceccato, A.; Torres, A. New aspects in the management of pneumonia. Crit. Care 2016, 20, 267. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Tsao, S.M.; Yeh, C.B.; Chou, Y.E.; Yang, S.F. Circulating level of high mobility group box1 predicts the severity of communityacquired pneumonia: Regulation of inflammatory responses via the cjun nterminal signaling pathway in macrophages. Mol. Med. Rep. 2017, 16, 2361–2366. [Google Scholar] [CrossRef]
- Lin, C.W.; Yang, W.E.; Lee, W.J.; Hua, K.T.; Hsieh, F.K.; Hsiao, M.; Chen, C.C.; Chow, J.M.; Chen, M.K.; Yang, S.F.; et al. Lipocalin 2 prevents oral cancer metastasis through carbonic anhydrase ix inhibition and is associated with favourable prognosis. Carcinogenesis 2016, 37, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Hsin, M.C.; Hsieh, Y.H.; Wang, P.H.; Ko, J.L.; Hsin, I.L.; Yang, S.F. Hispolon suppresses metastasis via autophagic degradation of cathepsin s in cervical cancer cells. Cell Death Dis. 2017, 8, e3089. [Google Scholar] [CrossRef] [PubMed]
- de Bock, C.E.; Wang, Y. Clinical significance of urokinase-type plasminogen activator receptor (upar) expression in cancer. Med. Res. Rev. 2004, 24, 13–39. [Google Scholar] [CrossRef]
- Kronbichler, A.; Saleem, M.A.; Meijers, B.; Shin, J.I. Soluble urokinase receptors in focal segmental glomerulosclerosis: A review on the scientific point of view. J. Immunol. Res. 2016, 2016, 2068691. [Google Scholar] [CrossRef] [PubMed]
- Montuori, N.; Selleri, C.; Ragno, P. The urokinase-receptor in infectious diseases. Infez. Med. 2012, 20 (Suppl. 6), 13–18. [Google Scholar]
- Falcone, M.; Corrao, S.; Venditti, M.; Serra, P.; Licata, G. Performance of psi, curb-65, and scap scores in predicting the outcome of patients with community-acquired and healthcare-associated pneumonia. Intern. Emerg. Med. 2011, 6, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Rello, J. Demographics, guidelines, and clinical experience in severe community-acquired pneumonia. Crit. Care 2008, 12 (Suppl. 6), S2. [Google Scholar] [CrossRef]
- Terraneo, S.; Polverino, E.; Cilloniz, C.; Amaro, R.; Vennera Mdel, C.; Gabarrus, A.; Montull, B.; Moreno, E.; Menendez, R.; Centanni, S.; et al. Severity and outcomes of community acquired pneumonia in asthmatic patients. Respir. Med. 2014, 108, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Varshochi, M.; Kianmehr, P.; Naghavi-Behzad, M.; Bayat-Makoo, Z. Correspondence between hospital admission and the pneumonia severity index (psi), curb-65 criteria and comparison of their predictive value in mortality and hospital stay. Infez. Med. 2013, 21, 103–110. [Google Scholar]
- Lee, M.; Snyder, A. The role of procalcitonin in community-acquired pneumonia: A literature review. Adv. Emerg. Nurs. J. 2012, 34, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Morley, D.; Torres, A.; Cilloniz, C.; Martin-Loeches, I. Predictors of treatment failure and clinical stability in patients with community acquired pneumonia. Ann. Transl. Med. 2017, 5, 443. [Google Scholar] [CrossRef]
- Viasus, D.; Del Rio-Pertuz, G.; Simonetti, A.F.; Garcia-Vidal, C.; Acosta-Reyes, J.; Garavito, A.; Carratala, J. Biomarkers for predicting short-term mortality in community-acquired pneumonia: A systematic review and meta-analysis. J. Infect. 2016, 72, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Li, H.; Qiu, J.; Feng, H. Betulin protects mice from bacterial pneumonia and acute lung injury. Microb. Pathog. 2014, 75, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Zhu, P.; Qi, S.; Li, C.; Zhao, K. Microrna-92a antagonism attenuates lipopolysaccharide (lps)-induced pulmonary inflammation and injury in mice through suppressing the pten/akt/nf-kappab signaling pathway. Biomed. Pharmacother. 2018, 107, 703–711. [Google Scholar] [CrossRef]
- Han, Y.K.; Kim, Y.S.; Natarajan, S.B.; Kim, W.S.; Hwang, J.W.; Jeon, N.J.; Jeong, J.H.; Moon, S.H.; Jeon, B.T.; Park, P.J. Antioxidant and anti-inflammatory effects of chaenomeles sinensis leaf extracts on lps-stimulated raw 264.7 cells. Molecules 2016, 21, 422. [Google Scholar] [CrossRef]
- Zhai, X.T.; Zhang, Z.Y.; Jiang, C.H.; Chen, J.Q.; Ye, J.Q.; Jia, X.B.; Yang, Y.; Ni, Q.; Wang, S.X.; Song, J.; et al. Nauclea officinalis inhibits inflammation in lps-mediated raw 264.7 macrophages by suppressing the nf-kappab signaling pathway. J. Ethnopharmacol. 2016, 183, 159–165. [Google Scholar] [CrossRef]
- Koch, A.; Zimmermann, H.W.; Gassler, N.; Jochum, C.; Weiskirchen, R.; Bruensing, J.; Buendgens, L.; Duckers, H.; Bruns, T.; Gerken, G.; et al. Clinical relevance and cellular source of elevated soluble urokinase plasminogen activator receptor (supar) in acute liver failure. Liver Int. 2014, 34, 1330–1339. [Google Scholar] [CrossRef]
- Gyetko, M.R.; Aizenberg, D.; Mayo-Bond, L. Urokinase-deficient and urokinase receptor-deficient mice have impaired neutrophil antimicrobial activation in vitro. J. Leukoc. Biol. 2004, 76, 648–656. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Variable | Controls (n = 67) | Before Antibiotic Treatment (n = 75) | After Antibiotic Treatment (n = 75) | p Value UT/C | p Value UT/T |
|---|---|---|---|---|---|
| Age | 61.10 ± 10.13 | 65.52 ± 17.71 | p = 0.075 | ||
| Gender | |||||
| Male | 45 (67.2%) | 52 (69.3%) | p = 0.782 | ||
| Female | 22 (32.8%) | 23 (30.7%) | |||
| CRP (mg/dL) | 0.49 ± 0.27 | 12.41 ± 7.85 | 3.84 ± 4.01 | p < 0.001 | p < 0.001 |
| WBCs (cells/mm3) | 6259.6 ± 2025.1 | 13211.2 ± 6375.4 | 10085.5 ± 5251.7 | p < 0.001 | p < 0.001 |
| Neutrophils (cells/mm3) | 3736.4 ± 1526.8 | 10505.3 ± 5248.8 | 7548.3 ± 4165.9 | p < 0.001 | p < 0.001 |
| PSI score | |||||
| I | 10 (13.3%) | ||||
| II | 16 (21.4%) | ||||
| III | 21 (28.0%) | ||||
| IV | 21 (28.0%) | ||||
| V | 7 (9.3%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, P.-K.; Tsao, S.-M.; Yang, W.-E.; Yeh, C.-B.; Wang, H.-L.; Yang, S.-F. Plasma Soluble Urokinase-Type Plasminogen Activator Receptor Level as a Predictor of the Severity of Community-Acquired Pneumonia. Int. J. Environ. Res. Public Health 2019, 16, 1035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061035
Tsai P-K, Tsao S-M, Yang W-E, Yeh C-B, Wang H-L, Yang S-F. Plasma Soluble Urokinase-Type Plasminogen Activator Receptor Level as a Predictor of the Severity of Community-Acquired Pneumonia. International Journal of Environmental Research and Public Health. 2019; 16(6):1035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061035
Chicago/Turabian StyleTsai, Ping-Kun, Shih-Ming Tsao, Wei-En Yang, Chao-Bin Yeh, Hsiang-Ling Wang, and Shun-Fa Yang. 2019. "Plasma Soluble Urokinase-Type Plasminogen Activator Receptor Level as a Predictor of the Severity of Community-Acquired Pneumonia" International Journal of Environmental Research and Public Health 16, no. 6: 1035. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16061035