Psycho-Physiological Stress Recovery in Outdoor Nature-Based Interventions: A Systematic Review of the Past Eight Years of Research

 , ,
, ,
Abstract
:1. Introduction
1.1. Psychological and Physiological Stress Recovery
1.2. Research Questions
2. Method
2.1. Eligibility Criteria
2.2. Information Source and Search Strategy
2.3. Inclusion and Assessment
3. Results
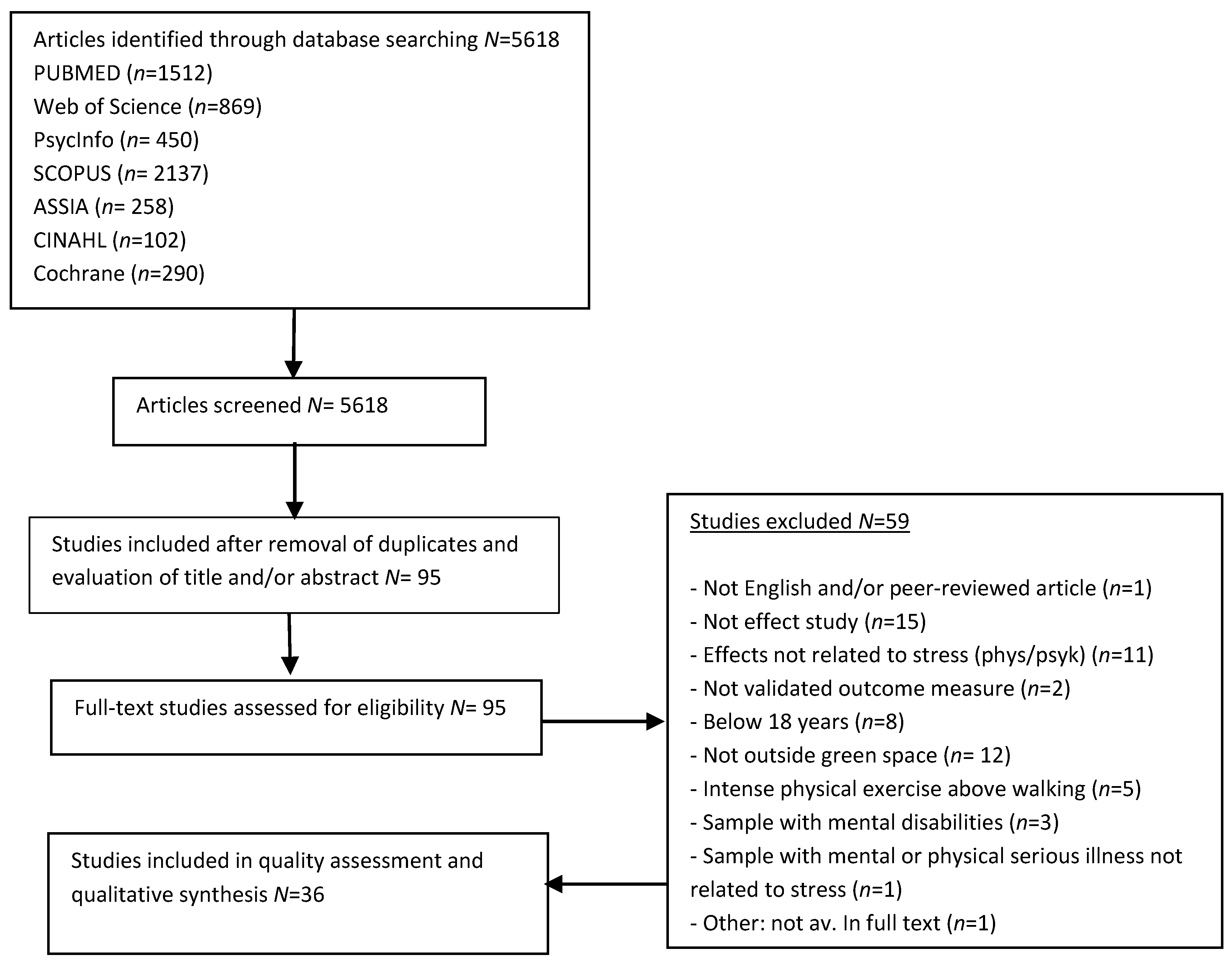
3.1. Article Selection Process
3.2. Characteristics of Included Studies
3.2.1. Study Design and Quality Assessment
3.2.2. Location
3.2.3. Sample Characteristics
3.2.4. Environments and Activities
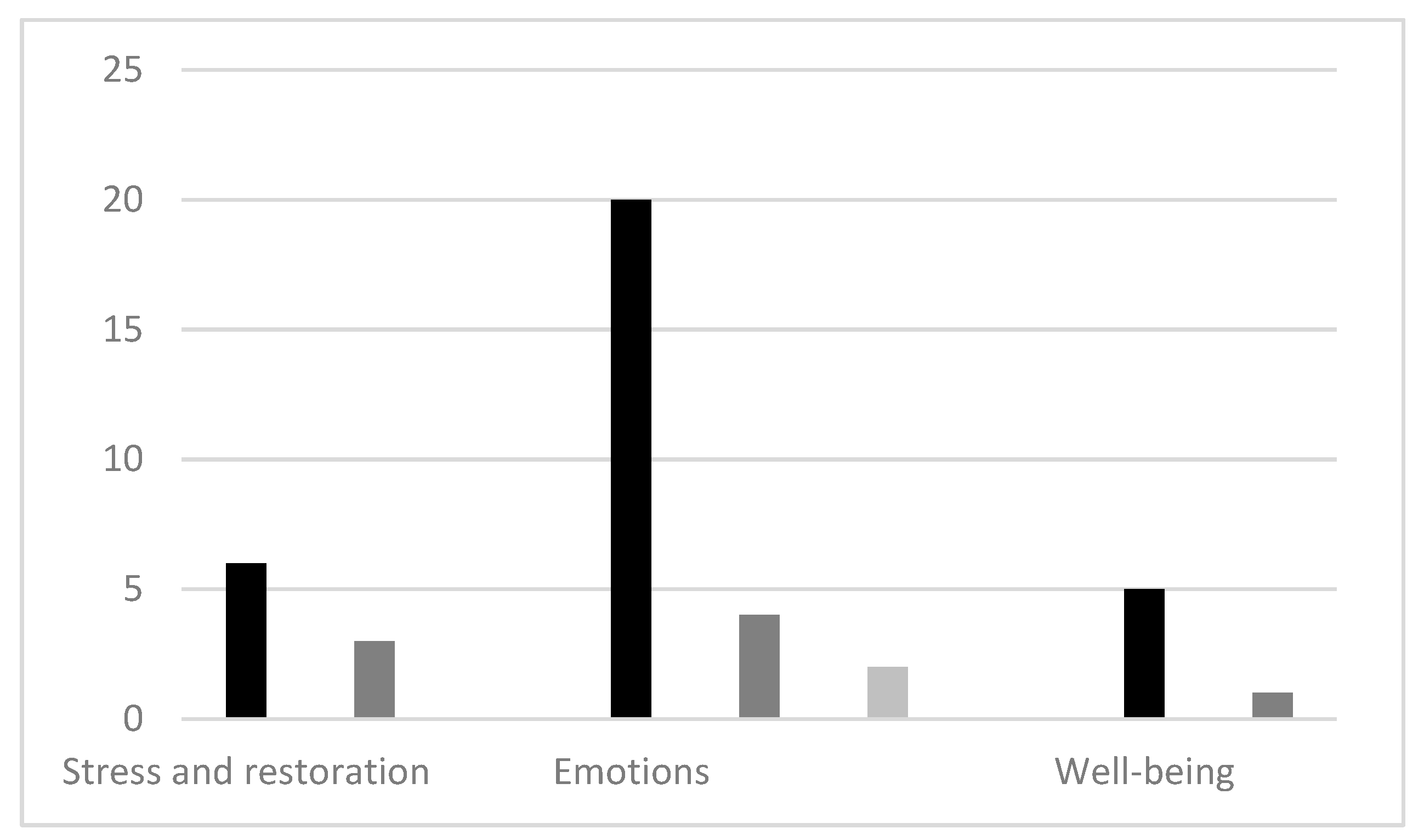
3.3. Summary and Synthesis of Psychological Outcomes
3.3.1. Stress, Burnout, and Recovery Outcomes
3.3.2. Emotional Outcomes
3.4. Well-Being, Quality of Life, and Mental Health Outcomes
3.4.1. Synthesis of Psychological Outcomes
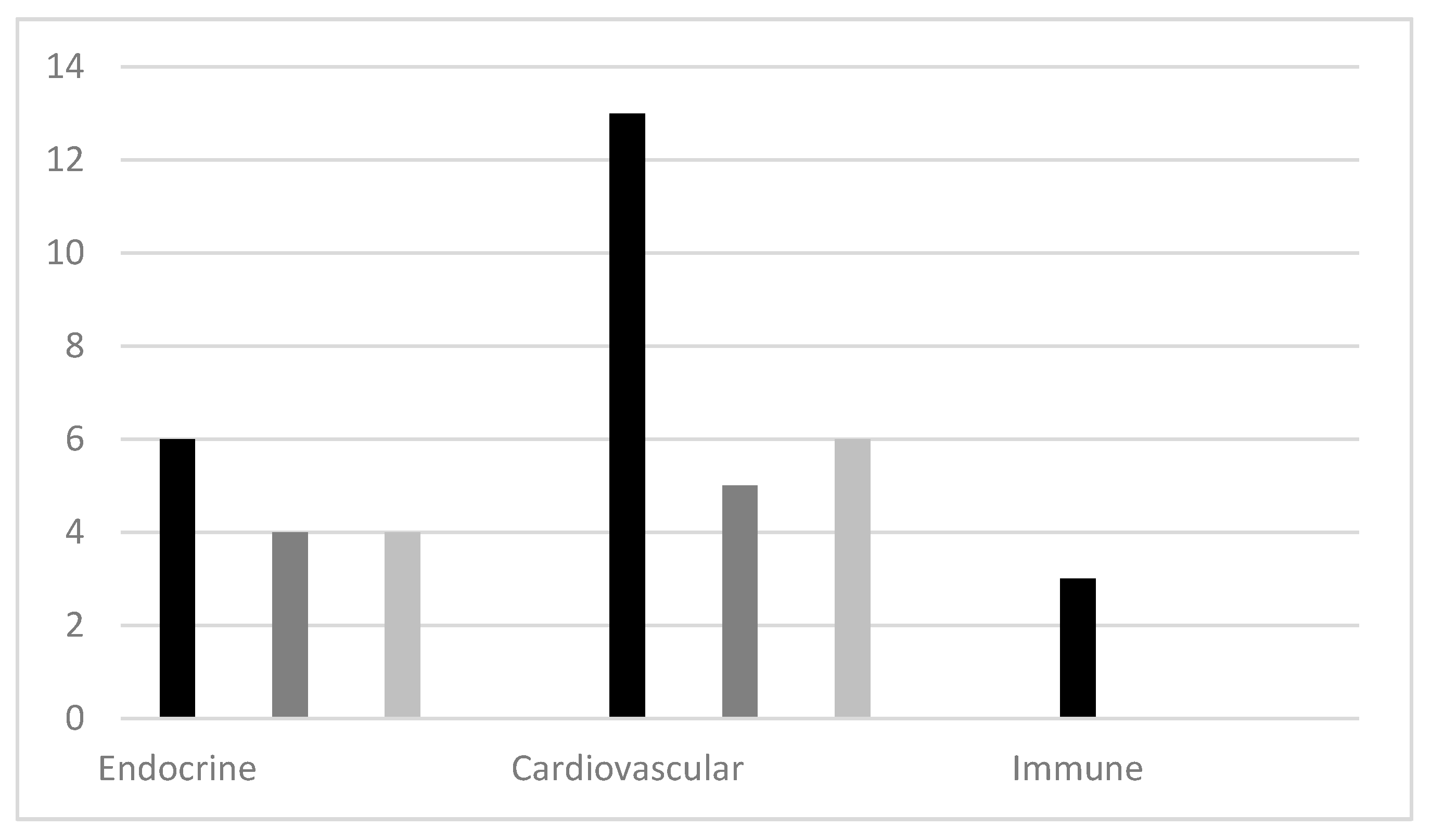
3.5. Summary and Synthesis of Physiological Outcomes
3.5.1. Endocrine Outcomes
3.5.2. Cardiovascular Outcomes
3.5.3. Immune Outcomes
3.5.4. Synthesis of Physiological Outcomes
4. Discussion
4.1. Quality of the Studies
4.2. Findings and Evidence Base
4.3. EPHPP as Quality Assessment Tool
4.4. “Nature-Positive” Bias
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. The Global Burden of Disease. In The Global Burden of Disease. A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries and Risk Factors in 1990 and Projected; Murray, C.J.L., Lopez, A.D., Eds.; Harvard School of Public Health: Cambridge, UK, 1996. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision, Online Edition. Available online: https://esa.un.org/unpd/wup/Publications (accessed on 13 May 2019).
- Towards an EU Research and Innovation Policy Agenda for Nature-Based Solutions & Re-Naturing Cities. Available online: https://ec.europa.eu/programmes/horizon2020/en/news/towards-eu-research-and-innovation-policy-agenda-nature-based-solutions-re-naturing-cities (accessed on 3 July 2015).
- World Health Organization. Urban Green Spaces and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Hansen, M.M.; Jones, R.; Tocchini, K. Shin-Yoku (Forest Bathing) and Nature Therapy: A State-Of-The-Art-Review. Int. J. Environ. Res. Public Health 2017, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- McMahan, E.A.; Estes, D. The effect of contact with natural environments on positive and negative affect: A meta-analysis. J. Posit. Psychol. 2015, 10, 507–519. [Google Scholar] [CrossRef]
- Haluza, D.; Schönbauer, R.; Cervinka, R. Green Perspective for Public Health: A Narrative Review on The Physiological Effects of Experiencing Outdoor Nature. Int. J. Environ. Res. Public Health 2014, 11, 5445–5461. [Google Scholar] [CrossRef]
- Kondo, M.C.; Jacoby, S.F.; South, E.C. Does spending time outdoors reduce stress? A review of real-time stress response to outdoor environments. Health Place 2018, 51, 136–150. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twohig-Bennet, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef]
- Lazarus, R.; Folksmann, S. Stress, Appraisal and Coping; Springer Publishing Company: New York, NY, USA, 1994. [Google Scholar]
- Murison, R. The neurobiology of stress. In Neuroscience of Pain, Stress, and Emotion: Psychological and Clinical Implications; Flaten, M., Absi, M.A., Eds.; Academic Press: Amsterdam, The Netherlands, 2016; pp. 20–49. [Google Scholar] [CrossRef]
- Ulrich, R.; Simons, R.F.; Lositot, B.D. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef] [Green Version]
- Ohly, H.; White, M.P.; Wheeler, B.W.; Bethel, A. A systematic review of the attention restoration potential of exposure to natural environments. J. Toxicol. Environ. Health 2016, 19, 305–343. [Google Scholar] [CrossRef]
- Stevenson, M.P.; Schilhab, T.S.S.; Bendtsen, P. Attention Restoration Theory II: A systematic review to clarify attention processes affected by exposure to natural environments. J. Toxicol. Environ. Health 2018, 21, 227–268. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Thuku, M.; Hamel, C.; Moran, J.; Henry, D.A. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, 1–9. [Google Scholar] [CrossRef]
- Rasmussen, L.N.; Montgomery, P. The prevalence of and factors associated with inclusion of non-English language studies in Campbell systematic reviews: A survey and meta-epidemiological study. Syst. Rev. 2018, 7, 129. [Google Scholar] [CrossRef] [PubMed]
- Gyllin, M.; Grahn, P. Semantic Assessments of Experienced Biodiversity from Photographs and on-Site Observations—A Comparison. Environ. Nat. Resour. Res. 2015, 5, 46–62. [Google Scholar] [CrossRef]
- Kahn, P.H.; Severson, R.L.; Ruckert, J.H. The human relation with nature and technological nature. Cur. Dir. Psychol. Sci. 2009, 18, 37–42. [Google Scholar] [CrossRef]
- Penedo, F.; Hahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Herosch-Herold, C. An Evidence-Based Approach to Choosing Outcome Measures: A Checklist for the Critical Appraisal of Validity, Reliability and Responsiveness Studies. Br. J. Occup. Ther. 2005, 68, 347–353. [Google Scholar] [CrossRef]
- Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies; Effective Public Health Practice Project: Hamilton, ON, USA, 1998; Available online: https://merst.ca/ephpp/ (accessed on 13 May 2019).
- Thomas, B.H.; Ciliske, R.N.; Dobbins, M.; Mucucci, B.A. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Grazuleviciene, R.; Vencloviene, J.; Kubilius, R.; Grizas, V.; Danileviciute, A.; Dedele, A.; Nieuwenhuijsen, M.J. Tracking Restoration of Park and Urban Street Settings in Coronary Artery Disease Patients. Int. J. Environ. Res. Public Health 2016, 13, 550. [Google Scholar] [CrossRef] [PubMed]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Niedermeier, M.; Einwanger, J.; Hartl, A.; Kopp, M. Affective responses in mountain hiking—A randomized crossover trial focusing on differences between indoor and outdoor activity. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef]
- Kjellgren, A.; Buhrkall, H. A comparison of the restorative effect of a natural environment with that of a simulated natural environment. J. Environ. Psych. 2010, 30, 464–472. [Google Scholar] [CrossRef]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang Province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar]
- Largo-Wight, E.; Wlyudka, P.S.; Merten, J.W.; Cuvelier, E.A. Effectiveness and feasibility of a 10 min employee stress intervention: Outdoor Booster Break. J. Work. Behav. Health 2017, 32, 159–171. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.-J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, G.; Cloke, P.; Vögele, C. Place, green exercise and stress: An exploration of lived experience and restorative effects. Health Place 2017, 46, 358–365. [Google Scholar] [CrossRef]
- Passmore, H.-A.; Howell, A.J. Nature involvement increases hedonic and eudaimonic well-being: A two-week experimental study. Ecopsychology 2014, 6, 148–154. [Google Scholar]
- Van Den Berg, A.E.; Custers, M.H.G. Gardening promotes neuroendocrine and affective restoration from stress. J. Health. Psychol. 2011, 16, 3–11. [Google Scholar] [CrossRef]
- Fuegen, K.; Breitenbecher, K.H. Walking and being outdoors in nature increase positive affect and energy. Ecopsychology 2018, 10, 14–25. [Google Scholar] [CrossRef]
- Gidlow, C.J.; Jones, M.V.; Hurst, G.; Masterson, D.; Clark-Carter, D.; Tarvainen, M.P.; Smith, G.; Nieuwenhuijsen, M. Where to put your best foot forward: Psycho-physiological responses to walking in natural and urban environments. J. Environ. Psychol. 2016, 45, 22–29. [Google Scholar] [CrossRef]
- Gladwell, V.F.; Kuoppa, P.; Tarvainen, M.P.; Rogerson, M. A Lunchtime Walk in Nature Enhances Restoration of Autonomic Control during Night-Time Sleep: Results from a Preliminary Study. Int. J. Environ. Res. Public Health 2016, 13, 280. [Google Scholar] [CrossRef]
- Horiuchi, M.; Endo, J.; Takayama, N.; Murase, K.; Nishiyama, N.; Saito, H.; Fujiwara, A. Impact of Viewing vs. Not Viewing a Real Forest on Physiological and Psychological Responses in the Same Setting. Int. J. Environ. Res. Public Health 2014, 11, 10883–10901. [Google Scholar] [CrossRef] [Green Version]
- Im, S.G.; Choi, H.; Jeon, Y.-H.; Song, M.-K.; Kim, W.; Woo, J.-M. Comparison of Effect of Two-Hour Exposure to Forest and Urban Environments on Cytokine, Anti-Oxidant, and Stress Levels in Young Adults. Int. J. Environ. Res. Public Health 2016, 13, 625. [Google Scholar] [CrossRef]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.-J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Population-based study on the effect of a forest environment on salivary cortisol concentration. Int. J. Environ. Res. Public Health 2017, 14, 931. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Igarashi, M.; Takagaki, M.; Miyazaki, Y. Physiological and Psychological Effects of a Walk in Urban Parks in Fall. Int. J. Environ. Res. Public Health 2015, 12, 14216–14228. [Google Scholar] [CrossRef] [Green Version]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Kristiansen, J.; Grahn, P. It is not all bad for the grey city—A crossover study on physiological and psychological restoration in a forest and an urban environment. Health Place 2017, 46, 145–154. [Google Scholar] [CrossRef]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Kobayashi, M.; Kumeda, S.; Ochiai, T.; Miura, T.; Kagawa, T.; Imai, M.; Wang, Z.; Otsuka, T.; Kawada, T. Effects of Forest Bathing on Cardiovascular and Metabolic Parameters in Middle-Aged Males. Evid. Based Complemt. Alternat. Med. 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Toda, M.; Den, R.; Hasegawa-Ohira, M.; Morimoto, K. Effects of woodland walking on salivary stress markers cortisol and chromogranin A. Complement. Ther. Med. 2013, 21, 29–34. [Google Scholar] [CrossRef]
- Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Warber, S.L. Examining group walks in nature and multiple aspects of well-being: A large-scale study. Ecopsychology 2014, 6, 134–147. [Google Scholar]
- Bird, K. Research evaluation of an Australian peer outdoor support therapy program for contemporary veterans’ wellbeing. Int. J. Ment. Health. 2015, 44, 46–79. [Google Scholar] [CrossRef]
- Duvall, J.; Kaplan, R. Enhancing the well-being of veterans using extended group-based nature recreation experiences. J. Rehabil. Res. Dev. 2014, 51, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, M.; Young, C.; Binz, T.M.; Baumgartner, M.R.; Bauer, N. Contact to Nature Benefits Health: Mixed Effectiveness of Different Mechanisms. Int. J. Environ. Res. Public Health 2018, 15, 31. [Google Scholar] [CrossRef]
- Iwata, Y.; Dhubháin, Á.N.; Brophy, J.; Roddy, D.; Burke, C.; Murphy, B. Benefits of group walking in forests for people with significant mental ill-health. Ecopsychology 2016, 8, 16–26. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Does perceived restorativeness mediate the effects of perceived biodiversity and perceived naturalness on emotional well-being following group walks in nature? J. Environ. Psych. 2016, 46, 217–232. [Google Scholar] [CrossRef]
- McCaffrey, R.; Liehr, P. The Effect of Reflective Garden Walking on Adults With Increased Levels of Psychological Stress. J. Holist. Nurs. 2016, 34, 177–184. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and Psychological Effects of Forest Therapy on Middle-Aged Males with High-Normal Blood Pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, H.; Ikei, H.; Song, C.R.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and Psychological Effects of a Forest Therapy Program on Middle-Aged Females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary approach. Tour. Manag. 2017, 62, 322–334. [Google Scholar] [CrossRef]
- Sahlin, E.; Ahrborg, G.; Tenenbaum, A.; Grahn, P. Using Nature-Based Rehabilitation to Restart a Stalled Process of Rehabilitation in Individuals with Stress-Related Mental Illness. Int. J. Environ. Res. Public Health 2015, 12, 1928–1951. [Google Scholar] [CrossRef] [Green Version]
- Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of Short Forest Bathing Program on Autonomic Nervous System Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Consumers and Communication Review Group: Data Synthesis and Analysis. Available online: http://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/Analysis.pdf (accessed on 13 May 2019).
- Nicolson, N.A. Measurement of Cortisol. In Handbook of Physiological Research—Methods in Health Psychology; Luecken, L.J., Gallo, L.G., Eds.; SAGE knowledge: Arizona, AZ, USA, 2008; pp. 37–73. [Google Scholar]
- Baker, M. Statisticians issue warning over misuse of p values. Nature 2016, 531, 151. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Miguel, A.C.; Hernán, A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Higgens, J.P. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 12, 4919. [Google Scholar] [CrossRef] [PubMed]
- Haga, A.; Halin, N.; Holmgreen, M.; Sörqvist, P. Psychological Restoration Can Depend on Stimulus-Source Attribution: A Challenge for the Evolutionary Account? Front. Psychol. 2016, 7, 1831. [Google Scholar] [CrossRef] [PubMed]
- Mlinarić, A.; Horvat, M.; Smolčić1, V.S. Dealing with the positive publication bias: Why you should really publish your negative results. Biochem. Med. 2017, 27. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.; Sadeghieh, T.; Adeli, K. Peer review in scientific publication: Benefits, critiques & a survival guide. EJIFCC 2014, 25, 227–243. [Google Scholar]

 Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention.  Number of studies with no significant difference found in pre-post measures of the nature intervention.
Number of studies with no significant difference found in pre-post measures of the nature intervention.  Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure. Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: Some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: Some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: Some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.
Number of studies with positive significant difference in pre-post measures of the nature intervention alone and/or effect of condition favoring the nature intervention. Number of studies with no significant difference found in pre-post measures of the nature intervention. Number of studies with positive significant difference in pre-post measures of both intervention and control and/or no significant difference between intervention and control. Note: Some of the studies have several different measurement instruments and are thus represented in multiple columns in the figure.

{kind=link}
{kind=link}
{kind=link}
| P | I | C | O |
|---|---|---|---|
| Population/Problem | Intervention | Comparison | Outcome |
| Adults (18+), all ethnicities, all countries, with or without stress-related issues/illness, without mental disabilities or other serious physical or mental illness. | Exposure to all types of outdoors natural green environments, with all types of sedentary and light exercise activities, in all time durations. From 2010–2018. | All kinds of comparisons or no comparison group. | Physiological (cardiovascular, endocrine, and immune) and psychological (mood, physiological stress, and well-being) outcomes related to stress prevention or stress treatment. |
| Main Author, Year | Country | Study Design | Sample Size | Characteristics | Age | Gender | Intervention | Control | Duration | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| (Control) | Assessment * | |||||||||
| [27] Grazuleviciene, 2016 | Lithuania | RCT | 10 (10) | Coronary artery disease | 45–75 y | Mixed | Park walks | Urban walks | 7 days | Weak (II) |
| [28] Razani, 2018 | USA | RCT 2:1 ratio | 50 (28) | Low-income parents | Mixed | Facilitated park tours | No facilitated tours | 3 months | Moderate (III) | |
| [29] Niedermeyer, 2017 | Austria | RCT crossover | 42 (42) | Healthy individuals | M:32 y | Mixed | Mountain hiking | Treadmill/sitting | 3 h | Weak (II) |
| [30] Han, 2016 | South Korea | CCT | 14 (14) | Elderly with poor mental health | NA | NA | Horticultural therapy | Passive control | 10 weeks | Weak (II) |
| [31] Kjellgren, 2010 | Sweden | CCT | 9 (9) | Individuals suffering from stress | 37 y | Mixed | Relaxation in nature | Slideshow of nature | 30 min | Moderate (II) |
| [32] Mao, 2011 | China | CCT | 10 (10) | University students | NA | Male | Stay/walk in forest | Stay walk in city | 2 days | Weak (I) |
| [33] Largo-Wight, 2017 | USA | CCT | 18 (19) | University office staff | M:49 y | Mixed | Daily outdoor break | Daily indoor break | 4 weeks | Moderate (III) |
| [34] Lee, 2010 | Japan | CCT | 12 (12) | University students | M:21 y | Male | Sitting in forest | Sitting in urban park | 15 min | Weak (I) |
| [35] Olafdottir, 2017 | Iceland | CCT | 20 (24) | Inactive university students | NA | NA | Nature walk | Treadmill/nature videos | 40 min | Weak (I) |
| [36] Passmore, 2014 | Canada | CCT | 43 (41) | Undergraduate students | NA | Mixed | Own choice nature activity | Own choice activity | 2 weeks | Weak (I) |
| [37] Van den Berg, 2011 | Netherlands | CCT | 14 (16) | Allotment gardeners | 38–79 y | Mixed | Gardening | Indoor reading | 30 min | Weak (II) |
| [38] Fuegen, 2018 | USA | CCT crossover | 181 (181) | University students | M:22 y | Mixed | Green walk/green rest | Treadmill/rest | 15 min | Weak (I) |
| [39] Gidlow, 2015 | UK | CCT crossover | 38 (38) | Unstressed adults | M:41 y | Mixed | Green walk/blue walk | Urban walk | 30 min | Weak (II) |
| [40] Gladwell, 2016 | UK | CCT crossover | 13 (13) | Healthy individuals | M:39 y | Mixed | Nature walk | Campus walk | 30 min | Weak (II) |
| [41] Horiuchi, 2014 | Japan | CCT crossover | 15 (15) | Healthy volunteers | M:36 y | Mixed | Sit and view in forest | View a curtain | 15 min | Weak (I) |
| [42] Im, 2016 | South Korea | CCT crossover | 41 (41) | Undergraduate students | 18–35 y | Mixed | Forest exposure | Urban exposure | 2 h | Weak (I) |
| [43] Kobayashi, 2017 | Japan | CCT crossover | 408 (408) | Young individuals | NA | Male | Forest viewing | Urban viewing | 15 min | Weak (I) |
| [44] Song, 2015 | Japan | CCT crossover | 23 (23) | University students | M:22 y | Male | Park walk | City walk | 15 min | Weak (I) |
| [45] Stigsdotter, 2017 | Denmark | CCT crossover | 51 (51) | University students | 20–36 y | Female | View and walk in arboretum | View and walk in city | 55 min | Weak (II) |
| [46] Tyrväinen, 2014 | Finland | CCT crossover | 77 (77) | Workers in Helsinki | 30–61 y | Mixed | View and walk in woodland | View and walk in city | 45 min | Moderate (III) |
| [47] Berman, 2012 | USA | pre/post crossover | 20 (20) | Depressive disorder | M:26 y | Mixed | Park walk | Urban walk | 50 min | Weak (I) |
| [48] Li, 2016 | Japan | pre/post crossover | 19 (19) | Middle-aged | 40–69 y | Male | Guided walks in forest park | Urban guided walks | 1 day | Weak (I) |
| [49] Toda, 2013 | Japan | pre/post crossover | 20 (20) | Volunteers | 64–74 y | Male | Woodland walk | Sitting in office | 45 min | Weak (I) |
| [50] Bang, 2017 | South Korea | pre/post crossover | 51 (48) | University students | M:26 y | Mixed | Forest walk in lunch break | Passive control | 6 weeks | Weak (II) |
| [51] Marselle, 2014 | UK | pre/post 2 groups | 15 (16) | Adults | NA | NA | Group walks in nature | Passive control | 13 weeks | Moderate (III) |
| [52] Bird, 2015 | Australia | pre/post | 20 | Veterans | 31–61 y | Male | Outdoor therapy program | 6 days | Weak (I) | |
| [53] Duvall, 2014 | USA | pre/post | 98 | Veterans | 20–49 y | Mixed | Nature-based recreation | 4–7 days | Weak (II) | |
| [54] Hofmann, 2017 | Germany | pre/post | 85 | Volunteer gardeners | 25–70 y | Mixed | Urban gardening | 6 months | Weak (II) | |
| [55] Iwata, 2016 | Ireland | pre/post | 15 | Mental ill health | 32–72 y | Mixed | Forest walk | 13 weeks | Weak (I) | |
| [56] Marselle, 2016 | UK | pre/post | 935 | Elderly | 55–74 y | Mixed | Walk in nature | 13 weeks | Weak (I) | |
| [57] McCaffrey, 2016 | USA | pre/post | 195 | Adults with stress | N/A | Mixed | Garden walks | 6 weeks | Weak (II) | |
| [58] Ochiai, 2015a | Japan | pre/post | 9 | Normal-to-high blood pressure | 40–72 y | Male | Relax and walk in forest | 1 day | Weak (I) | |
| [59] Ochiai, 2015b | Japan | pre/post | 17 | Middle aged | 40–73 y | Female | Forest therapy program | 2 days | Weak (I) | |
| [60] Ohe, 2017 | Japan | pre/post | 43 | Office workers | 20–70 y | Mixed | Forest therapy program | 2 days | Weak (I) | |
| [61] Sahlin, 2015 | Sweden | pre/post | 57 | On sick leave due to stress | 45 y | Mixed | Nature-based therapy | 16 weeks | Moderate (III) | |
| [62] Yu, 2017 | Taiwan | pre/post | 128 | Middle-aged and elderly | 45–86 y | Mixed | Forest bathing program | 2 h | Weak (I) |
| Main Author, Year | Measure | Intervention | p Value | Control | p Value | Comparison | p Value | Effect Size | Comments |
|---|---|---|---|---|---|---|---|---|---|
| Stress, burnout, and recovery | |||||||||
| Stress | |||||||||
| [31] Kjellgren, 2010 | Stress and energy test | NA | NA | Difference | <0.01 | NA | |||
| [31] Kjellgren, 2010 | Stress VAS | NA | NA | Difference | <0.05 | NA | |||
| [33] Largo-Wight, 2017 | Perceived stress scale | NA | NA | Difference | <0.05 | NA | |||
| [38] Razani, 2018 | Perceived stress scale | NA | NA | No difference | NA | ||||
| [42] Im, 2016 | Stress responsive inventory | NA | NA | Difference | <0.05 | NA | No baseline | ||
| [51] Marselle, 2014 | Perceived stress scale | NA | NA | Difference | <0.001 | 0.22 | |||
| [53] Duvall, 2014 | Perceived stress scale | NS | NA | ||||||
| [54] Hofmann, 2017 | Stress and coping inventory | NS | NA | ||||||
| Burnout | |||||||||
| [61] Sahlin, 2014 | Shirom-melamed burnout | Decrease | NA | NA | |||||
| Recovery | |||||||||
| [46] Tyrväinen, 2014 | Recovery outcome scale | NA | NA | Difference | <0.01 | 0.53 | |||
| Emotions | |||||||||
| Positive and negative affect | |||||||||
| [27] Grazuleviciene, 2016 | Positive and negative affect scale | NS | Decrease NA | <0.01 | NA | ||||
| [35] Olafdottir, 2017 | Positive and negative affect scale | NA | NA | NA | Results not reported | ||||
| [36] Passmore, 2014 | Positive and negative affect scale | NA | NA | Difference | <0.05 | NA | |||
| [37] Van den Berg, 2011 | Positive and negative affect scale | Increase PA | <0.05 | NS | NA | ||||
| [38] Fuegen, 2018 | Positive and negative affect scale | NA | NA | Difference | <0.01 | NA | |||
| [46] Tyrväinen, 2014 | Positive and negative affect scale | NA | NA | Difference | <0.01 | Pa 0.43/Na 0.15 | |||
| [47] Berman, 2012 | Positive and negative affect scale | improvement | <0.001 | Improvement | <0.005 | Difference | <0.001 | NA | |
| [51] Marselle, 2014 | Positive and negative affect scale | NA | NA | Difference | <0.001 | Pa 0.24/Na 0.22 | |||
| [53] Duvall, 2014 | Positive and negative affect scale | Improvement | <0.05–0.001 | NA | |||||
| [55] Iwata, 2016 | Positive and negative affect scale | NS | NA | NA | |||||
| [56] Marselle, 2016 | Positive and negative affect scale | NA | NA | Difference | <0.05 | NA | |||
| Mood | |||||||||
| [32] Mao, 2011 | Profile of mood states | NA | NA | Difference subscales | <0.05 | NA | No baseline | ||
| [29] Niedermeyer, 2017 | Mood survey scale | Improvement subscales | <0.001 | NS | NA | ||||
| [34] Lee, 2010 | Profile of mood states | Improvement | <0.01 | improvement subscales | <0.01 | NA | |||
| [39] Gidlow, 2010 | Profile of mood states | NA | NA | No difference | NA | ||||
| [41] Horiuchi, 2014 | Profile of mood states | Improvement subscales | <0.05-0.01 | improvement subscales | <0.01 | NA | |||
| [44] Song, 2015 | Profile of mood states | NA | NA | Difference subscales | <0.05 | NA | No baseline | ||
| [45] Stigsdotter, 2017 | Profile of mood states | Improvement | <0.05 | NS | NA | ||||
| [48] LI, 2016 | Profile of mood states | Improvement subscales | <0.05-0.01 | Recession subscales | <0.01 | NA | |||
| [54] Hofmann, 2017 | Profile of mood states | NS | NS | NA | |||||
| [58] Ochiai, 2015a | Profile of mood states | Improvement subscales | <0.05 | NA | |||||
| [59] Ochiai, 2015b | Profile of mood states | Improvement subscales | <0.01 | NA | |||||
| Anxiety | |||||||||
| [29] Niedermeyer, 2017 | State trait anxiety inventory | Decrease | <0.001 | NS | NA | ||||
| [44] Song, 2015 | State trait anxiety inventory | NA | NA | Difference | <0.01 | NA | No baseline | ||
| [61] Sahlin, 2015 | Beck anxiety inventory | Decrease | <0.005 | NA | |||||
| [62] Yu, 2017 | State trait anxiety inventory | Decrease | <0.01 | NA | |||||
| Depression | |||||||||
| [50] Bang, 2017 | Beck depression inventory | NA | NA | Difference | <0.001 | NA | |||
| [51] Marselle, 2014 | Major depressive Inventory | NA | NA | Difference | <0.001 | 0.21 | |||
| [55] Iwata, 2016 | Hamilton depression rating scale | NA | NA | NA | |||||
| [55] Iwata, 2016 | Beck depression inventory | NA | NA | NA | |||||
| [61] Sahlin, 2015 | Becks depression inventory | Decrease | <0.0001 | NA | |||||
| Combined measures | |||||||||
| [52] Bird, 2015 | Depression, anxiety, stress scale | Decrease | <0.001 | NA | |||||
| Well-being, quality of life, and mental health | |||||||||
| [51] Marselle, 2014 | Warwick Edinburgh mental well-being scale | NA | NA | Difference | <0.001 | 0.19 | |||
| [54] Hofmann, 2017 | Mental health (SF12) | NS | NS | NA | |||||
| [56] Marselle, 2016 | Single-item happiness scale | Increase | <0.001 | NA | |||||
| [57] McCaffrey, 2016 | Personal Growth Initiative Scale (PGIS) | Increase | <0.000 | NA | |||||
| [57] McCaffrey, 2016 | Quality of Life Scale | Increase | <0.001 | NA | |||||
| [61] Sahlin, 2015 | Psych. general well-being index | Increase | <0.0001 | NA | |||||
| Main Author, Year | Measure | Intervention | p Value | Control | p Value | Comparison | p Value | Comments |
|---|---|---|---|---|---|---|---|---|
| Endocrine | ||||||||
| Cortisol | ||||||||
| [27] Grazuleviciene, 2016 | Salivary cortisol | NS | NS | |||||
| [28] Razani, 2018 | Serum cortisol | NA | NA | Difference | <0.05 | |||
| [30] Han, 2016 | Salivary cortisol | Decrease | <0.05 | NS | ||||
| [32] Mao, 2011 | Hair cortisol | NS | NS | |||||
| [34] Lee, 2010 | Salivary cortisol | NS | NS | |||||
| [35] Olafdottir, 2017 | Salivary cortisol | NA | NA | No difference | ||||
| [37] Van den Berg, 2011 | Salivary cortisol | Decrease | <0.01 | Decrease | <0.05 | |||
| [39] Gidlow, 2015 | Salivary cortisol | Decrease | <0.01 | Decrease | <0.01 | No difference | ||
| [43] Kobayashi, 2017 | Salivary cortisol | NA | NA | Difference | <0.001 | No baseline | ||
| [46] Tyrväinen, 2014 | Salivary cortisol | Decrease | <0.01 | Decrease | <0.01 | No difference | ||
| [49] Toda, 2013 | Salivary cortisol | NS | NS | |||||
| [58] Ochiai, 2015a | Serum cortisol | Decrease | <0.01 | |||||
| [59] Ochiai, 2015b | Salivary cortisol | Decrease | <0.05 | |||||
| Other | ||||||||
| [48] Li, 2016 | Stress hormones | Decrease | <0.01 | Decrease | <0.01 | |||
| [41] Horiuchi, 2014 | Salivia amylases | NA | NA | Difference | <0.05 | |||
| Cardiovascular | ||||||||
| Heart rate variability | ||||||||
| [34] Lee, 2010 | HRV | Improved | p < 0.05 | NA | ||||
| [35] Olafdottir, 2017 | HRV | NA | NA | |||||
| [39] Gidlow, 2017 | HRV | NS | NS | |||||
| [40] Gladwell, 2016 | HRV | NA | NA | Difference | <0.05 | |||
| [41] Horiuchi, 2014 | HRV | Decrease HR | <0.05 | Decrease HR | <0.05 | No Difference | ||
| [44] Song, 2015 | HRV | NA | NA | Difference | <0.01 | |||
| [45] Stigsdotter, 2017 | HRV | Increase HF | <0.001 | Increase HF | <0.001 | No difference | ||
| [50] Bang, 2017 | HRV | NA | NA | Difference | <0.05 | |||
| [62] Yu, 2017 | HRV | NS | ||||||
| Blood pressure | ||||||||
| [27] Grazuleviciene, 2016 | Blood pressure | Decrease DBP | <0.05 | NS | ||||
| [31] Kjellgren, 2010 | Blood pressure | NA | NA | No difference | ||||
| [34] Lee, 2010 | Blood pressure | NS | NS | |||||
| [41] Huriuchi, 2014 | Blood pressure | Decrease | p < 0.05 | Decrease | p < 0.05 | No difference | ||
| [45] Stigsdotter, 2017 | Blood pressure | Decrease | p < 0.05 | Decease | p < 0.05 | No difference | ||
| [48] Li, 2016 | Blood pressure | NS | NS | |||||
| [49] Toda, 2013 | Blood pressure | Decrease | <0.05 | NS | ||||
| [58] Ochiai, 2015a | Blood pressure | Decrease | <0.05 | |||||
| [60] Ohe, 2017 | Blood pressure | Decrease | <0.05 | |||||
| [62] Yu, 2017 | Blood pressure | Decrease | <0.01 | |||||
| Pulse rate | ||||||||
| [31] Kjellgren, 2010 | Pulse rate | NA | NA | No difference | ||||
| [34] Lee, 2010 | Pulse rate | NA | NA | Difference | <0.01 | |||
| [48] Li, 2016 | Pulse rate | NA | NA | Difference | <0.01 | |||
| [58] Ochiai, 2015a | Pulse rate | Decrease | <0.01 | |||||
| [60] Ohe, 2017 | Pulse rate | NS | ||||||
| [62] Yu, 2017 | Pulse rate | Decrease | <0.01 | |||||
| Immune system | ||||||||
| [32] Mao, 2011 | Serum PI | NA | NA | Difference | <0.05 | |||
| [32] Mao, 2011 | Oxidative stress | NA | NA | Difference MDA | <0.001 | |||
| [42] Im, 2016 | Blood serum | NA | NA | Difference | <0.05–0.001 | No baseline | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corazon, S.S.; Sidenius, U.; Poulsen, D.V.; Gramkow, M.C.; Stigsdotter, U.K. Psycho-Physiological Stress Recovery in Outdoor Nature-Based Interventions: A Systematic Review of the Past Eight Years of Research. Int. J. Environ. Res. Public Health 2019, 16, 1711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101711
Corazon SS, Sidenius U, Poulsen DV, Gramkow MC, Stigsdotter UK. Psycho-Physiological Stress Recovery in Outdoor Nature-Based Interventions: A Systematic Review of the Past Eight Years of Research. International Journal of Environmental Research and Public Health. 2019; 16(10):1711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101711
Chicago/Turabian StyleCorazon, Sus Sola, Ulrik Sidenius, Dorthe Varning Poulsen, Marie Christoffersen Gramkow, and Ulrika Karlsson Stigsdotter. 2019. "Psycho-Physiological Stress Recovery in Outdoor Nature-Based Interventions: A Systematic Review of the Past Eight Years of Research" International Journal of Environmental Research and Public Health 16, no. 10: 1711. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16101711