New 20 m Progressive Shuttle Test Protocol and Equation for Predicting the Maximal Oxygen Uptake of Korean Adolescents Aged 13–18 Years

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Modified 20 m PST Protocol Development
2.3. Anthropometric Measurements
2.4. Laboratory Assessment of VO2max (GXT)
2.5. Field Assessment of VO2max (Modified 20 m PST)
2.6. Reliability Testing of the Modified 20 m PST Protocol
2.7. Statistical Analysis
3. Results
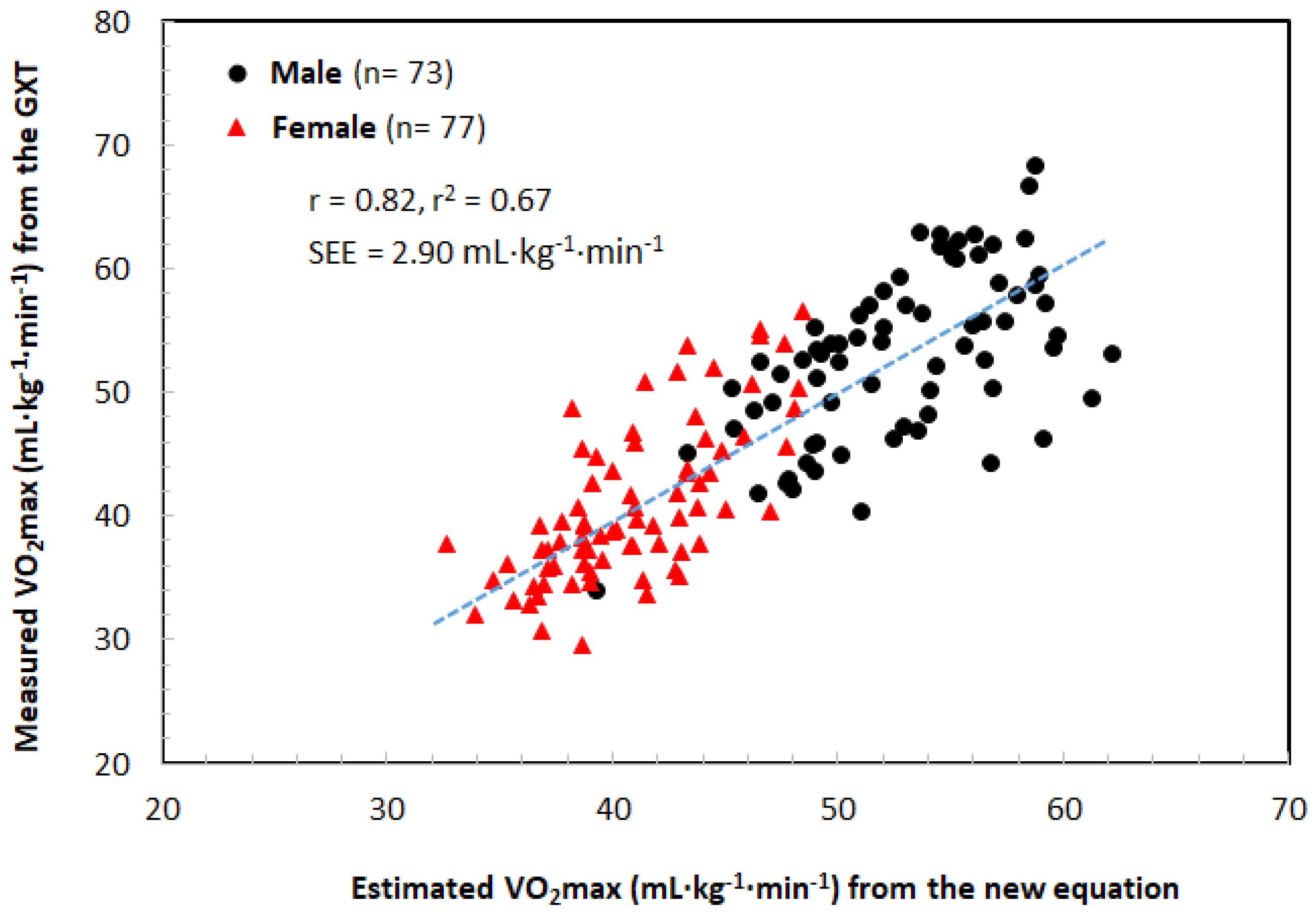
- with r = 0.82; r2 = 0.67; SEE = 2.90 mL·kg−1·min−1, n = 152.
- where “laps” are the number of laps in the modified 20 m PST and “age”, “G”, and “W” are the age, sex (boy = 1, girl = 2), and weight, respectively, of the participants performing the modified 20 m PST.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Korea Centers for Disease Control and Prevention (KCDC). The 12th Korea Youth Risk Behavior Survey; KCDC: Seoul, Korea, 2012. [Google Scholar]
- WHO. Global Health Observatory (GHO) Data. Prevalence of Insufficient Physical Activity. Available online: http://www.who.int/gho/ncd/risk_factors/physical_activity/en/ (accessed on 4 June 2019).
- Ko, B.G.; Kim, Y.R.; Sung, B.J.; Chung, D.S.; Youn, S.W.; Lee, J.K.; Shin, I.S.; Chang, G.J.; Park, I.G.; Kim, D.H. Development of Criteria for Korea Youth Fitness Award. Korean J. Sport Sci. 2005, 16, 44–63. [Google Scholar]
- Leite, S.A.; Monk, A.M.; Upham, P.A.; Bergenstal, R.M. Low cardiorespiratory fitness in people at risk for type 2 diabetes: Early marker for insulin resistance. Diabetol. Metab. Syndr. 2009, 1, 8. [Google Scholar] [CrossRef] [PubMed]
- Steell, L.; Ho, F.K.; Sillars, A.; Petermann-Rocha, F.; Li, H.; Lyall, D.M.; Iliodromiti, S.; Welsh, P.; Anderson, J.; MacKay, D.F.; et al. Dose-response associations of cardiorespiratory fitness with all-cause mortality and incidence and mortality of cancer and cardiovascular and respiratory diseases: The UK Biobank cohort study. Br. J. Sports Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.H.; Park, D.H.; Youn, S.W.; Chung, D.S. Analysis on the Heart Ratepesponses at LT and OBLA of Swimmers according to Graded Exercise Test Methods. Korean J. Sport Sci. 2003, 14, 88–96. [Google Scholar]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ko, B.G. Practical field aerobic fitness test, Shuttle run test. Sports Sci. 2006, 96, 31–38. [Google Scholar]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavón, D.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field based fitness assessment in young people: The ALPHA health related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Ghouri, N.; Purves, D.; McConnachie, A.; Wilson, J.; Gill, J.M.; Sattar, N. Lower cardiorespiratory fitness contributes to increased insulin resistance and fasting glycaemia in middle-aged South Asian compared with European men living in the UK. Diabetologia 2013, 56, 2238–2249. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.Y.; Kim, J.S.; Park, D.H. Assessing Agreement of Various 20 m PSRT Equations to Estimate VO2max in the Middle School Girls. Korean J. Sport Sci. 2012, 23, 254–264. [Google Scholar]
- Poole, D.C.; Ward, S.A.; Gardner, G.W.; Whipp, B.J. Metabolic and respiratory profile of the upper limit for prolonged exercise in man. Ergonomics 1988, 31, 1265–1279. [Google Scholar] [CrossRef] [PubMed]
- Saltin, B. Oxygen uptake during the first minutes of heavy muscular exercise. J. Appl. Physiol. 1961, 16, 971–976. [Google Scholar]
- Whipp, B.J. The slow component of O2 uptake kinetics during heavy exercise. Med. Sci. Sports Exerc. 1994, 26, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Whipp, B.J.; Wasserman, K. Oxygen uptake kinetics for various intensities of constant-load work. J. Appl. Physiol. 1972, 33, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.K.; Kravitz, L.; Robergs, R. VO2max, protocol duration, and the VO2 plateau. Med. Sci. Sports Exerc. 2007, 39, 1186–1192. [Google Scholar] [CrossRef]
- Park, D.H.; Song, J.R.; Lee, S.H.; Kim, C.S. The Development of Prediction Equation for Estimating VO2max from the 20 m PSRT in Korean Middle-School Girls. Exerc. Sci. 2014, 23, 1–11. [Google Scholar] [CrossRef]
- Incheon Metropolitan City Office of Education (IMCOE). General Report on Physical Activity Promotion System (PAPS); IMCOE: Seoul, Korea, 2007. [Google Scholar]
- Barnett, A.; Chan, L.Y.S.; Bruce, I.C. A preliminary study of the 20 m multistage shuttle run as a predictor of peak VO2 in Hong Kong Chinese students. Ped. Exer. Sci. 1993, 5, 42–50. [Google Scholar] [CrossRef]
- Gualteros, J.A.; Torres, J.A.; Umbarila-Espinosa, L.M.; Rodríguez-Valero, F.J.; Ramírez-Vélez, R. A lower cardiorespiratory fitness is associated to an unhealthy status among children and adolescents from Bogotá, Colombia. Endocrinol. Nutr. 2015, 62, 437–446. [Google Scholar] [CrossRef]
- Mahar, M.T.; Guerieri, A.M.; Hanna, M.S.; Kemble, C.D. Estimation of aerobic fitness from 20 m multistage shuttle run test performance. Am. J. Prev. Med. 2011, 41, S117–S123. [Google Scholar] [CrossRef]
- Matsuzaka, A.; Takahashi, Y.; Yamazoe, M.; Kumakura, N.; Ikeda, A.; Wilk, B. Validity of the multistage 20m shuttle run test for Japanese children, adolescents, and adults. Pediatr. Exer. Sci. 2004, 16, 113–125. [Google Scholar] [CrossRef]
- Melo, X.; Santa-Clara, H.; Almeida, J.P.; Carnero, E.A.; Sardinha, L.B.; Bruno, P.M.; Fernhall, B. Comparing several equations that predict peak VO2 using the 20 m multistage-shuttle run-test in 8–10-year-old children. Eur. J. Appl. Physiol. 2011, 111, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Mora-Gonzalez, J.; Cadenas-Sanchez, C.; Martinez-Tellez, B.; Sanchez-Delgado, G.; Ruiz, J.R.; Léger, L.; Ortega, F.B. Estimating VO2max in children aged 5–6 years through the preschool-adapted 20 m shuttle-run test (PREFIT). Eur. J. Appl. Physiol. 2017, 117, 2295–2307. [Google Scholar] [CrossRef] [PubMed]
- Quinart, S.; Mougin, F.; Simon-Rigaud, M.L.; Nicolet-Guenat, M.; Negre, V.; Regnard, J. Evaluation of cardiorespiratory fitness using three field tests in obese adolescents: Validity, sensitivity and prediction of peak VO2. J. Sci. Med. Sport 2014, 17, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Ramirez-Lechuga, J.; Ortega, F.B.; Castro-Pinero, J.; Benitez, J.M.; Arauzo-Azofra, A.; Sanchez, C.; Sjöström, M.; Castillo, M.J.; Gutierrez, A.; et al. Artificial neural network-based equation for estimating VO2max from the 20 m shuttle run test in adolescents. Artif. Intell. Med. 2008, 44, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Silva, G.; Oliveira, N.; Ribeiro, J.C.; Oliveira, J.F.; Mota, J. Criterion-related validity of the 20 m shuttle run test in youths aged 13–19 years. J. Sports Sci. 2009, 27, 899–906. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal modeling of the relationship between age and maximal heart rate. Med. Sci. Sports Exerc. 2007, 39, 822–829. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.E.; King, G.A.; Howley, E.T.; Bassett, D.R., Jr.; Ainsworth, B.E. Validation of the COSMED K4 b2 portable metabolic system. Int. J. Sports Med. 2001, 22, 280–284. [Google Scholar] [CrossRef]
- Flouris, A.D.; Metsios, G.S.; Koutedakis, Y. Enhancing the efficacy of the 20 m multistage shuttle run test. Br. J. Sports Med. 2005, 39, 166–170. [Google Scholar] [CrossRef] [Green Version]
- Paliczka, V.J.; Nichols, A.K.; Boreham, C.A. A multi-stage shuttle run as a predictor of running performance and maximal oxygen uptake in adults. Br. J. Sports Med. 1987, 21, 163–165. [Google Scholar] [CrossRef]
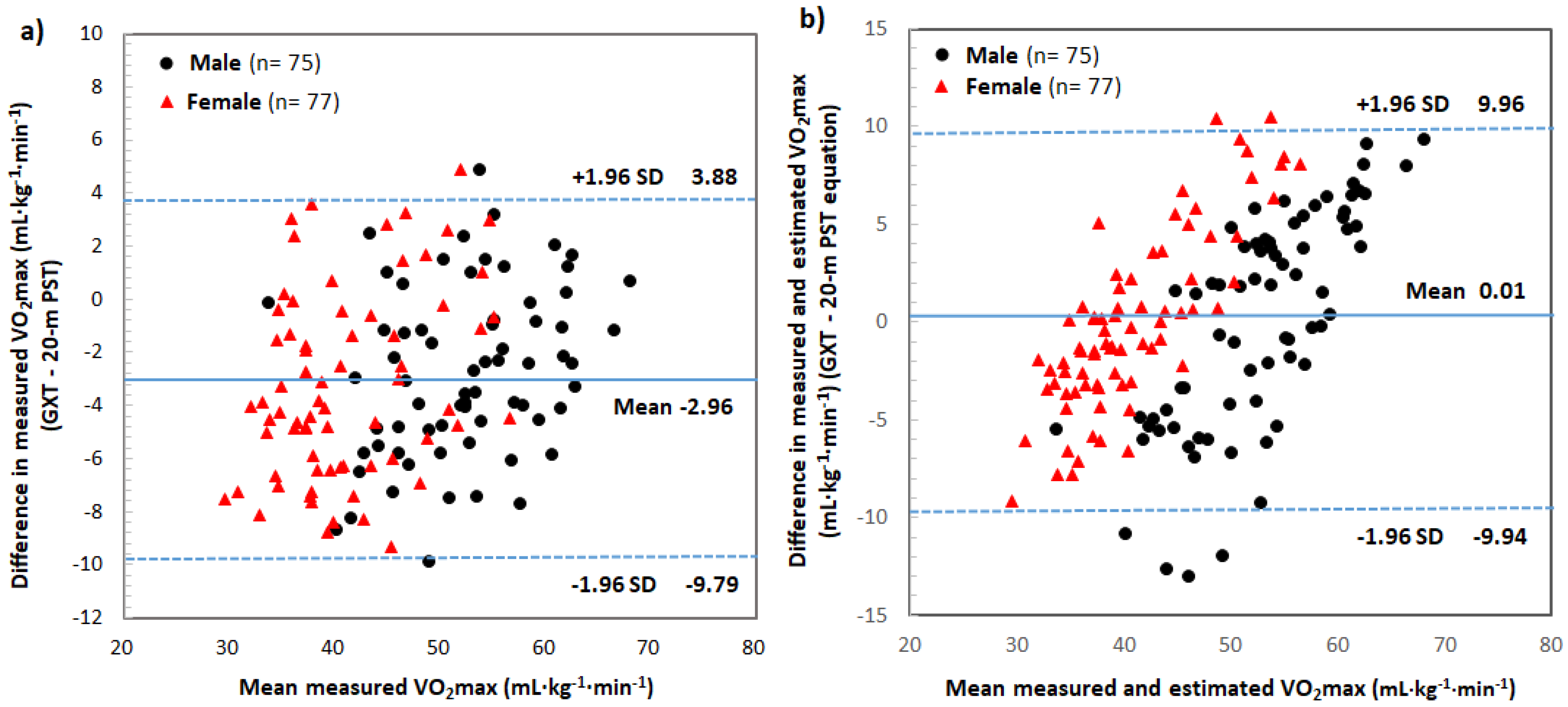
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Lepretre, P.M.; Koralsztein, J.P.; Billat, V.L. Effect of exercise intensity on relationship between VO2max and cardiac output. Med. Sci. Sports Exerc. 2004, 36, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- McCole, S.D.; Davis, A.M.; Fueger, P.T. Is there a disassociation of maximal oxygen consumption and maximal cardiac output? Med. Sci. Sports Exerc. 2001, 33, 1265–1269. [Google Scholar] [CrossRef] [PubMed]
- Buchfuhrer, M.J.; Hansen, J.E.; Robinson, T.E.; Sue, D.Y.; Wasserman, K.; Whipp, B.J. Optimizing the exercise protocol for cardiopulmonary assessment. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Doust, J.H. A 1% treadmill grade most accurately reflects the energetic cost of outdoor running. J. Sports Sci. 1996, 14, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Flouris, A.D.; Metsios, G.S.; Famisis, K.; Geladas, N.; Koutedakis, Y. Prediction of VO2max from a new field test based on portable indirect calorimetry. J. Sci. Med. Sport 2010, 13, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Ahmaidi, S.; Collomp, K.; Caillaud, C.; Prefaut, C. Maximal and functional aerobic capacity as assessed by two graduated field methods in comparison to laboratory exercise testing in moderately trained subjects. Int. J. Sports Med. 1992, 13, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.; Corbett, K.; Amjad, A.M.; Wilson, J.; Aitchison, T. A comparison of methods of predicting maximum oxygen uptake. Br. J. Sports Med. 1995, 29, 147–152. [Google Scholar] [CrossRef]
- Sproule, J.; Kunalan, C.; McNeill, M.; Wright, H. Validity of 20 mST for predicting VO2max of adult Singaporean athletes. Br. J. Sports Med. 1993, 27, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Léger, L.A.; Lambert, J. A maximal multistage 20 m shuttle run test to predict VO2 max. Eur. J. Appl. Physiol. Occup. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef]
- Mahar, M.T.; Welk, G.J.; Rowe, D.A. Estimation of aerobic fitness from PACER performance with and without body mass index. Meas. Phys. Educ. Exerc. Sci. 2018, 22, 239–249. [Google Scholar] [CrossRef]
- Lamb, K.L.; Rogers, L. A re-appraisal of the reliability of the 20 m multi-stage shuttle run test. Eur. J. Appl. Physiol. 2007, 100, 287–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GXT Protocol (Modified KISS Protocol) | Modified 20 m PST Protocol * | |||||||
|---|---|---|---|---|---|---|---|---|
| Stage (2 min, 3% Grade Stage) | Speed (km·h−1) | Speed (m·min−1) | Stage (1 min) | Speed (km·h−1) | Lap. | Cumulative Count | 20 m Reaching Time (Sec) | Expended Time·Stage −1 (Sec) |
| 2-min warm-up | 5.00 | 83.33 | 5.00 | 4 | 14.40 | 57.60 | ||
| 5.00 | 83.33 | 5.00 | 4 | 14.40 | 57.60 | |||
| 1 | 5.00 | 83.33 | 1 | 5.00 | 4 | 14.40 | 57.60 | |
| 2 | 5.75 | 5 | 9 | 12.50 | 62.60 | |||
| 2 | 6.50 | 108.33 | 3 | 5.75 | 5 | 14 | 12.50 | 62.60 |
| 4 | 7.25 | 6 | 20 | 9.90 | 59.60 | |||
| 3 | 8.00 | 133.33 | 5 | 7.25 | 6 | 26 | 9.90 | 59.60 |
| 6 | 8.75 | 7 | 33 | 8.20 | 57.60 | |||
| 4 | 9.50 | 158.33 | 7 | 9.50 | 8 | 41 | 7.60 | 60.60 |
| 8 | 9.50 | 8 | 49 | 7.60 | 60.60 | |||
| 5 | 11.00 | 183.33 | 9 | 11.00 | 9 | 58 | 6.50 | 58.90 |
| 10 | 11.75 | 10 | 68 | 6.10 | 61.30 | |||
| 6 | 12.50 | 208.33 | 11 | 11.75 | 10 | 78 | 6.10 | 61.30 |
| 12 | 13.25 | 11 | 89 | 5.40 | 59.80 | |||
| 7 | 14.00 | 233.33 | 13 | 14.00 | 12 | 101 | 5.10 | 61.70 |
| 14 | 14.00 | 12 | 113 | 5.10 | 61.70 | |||
| 8 | 15.50 | 258.33 | 15 | 15.50 | 13 | 126 | 4.60 | 60.40 |
| 16 | 15.50 | 13 | 139 | 4.60 | 60.40 | |||
| 9 | 17.00 | 283.33 | 17 | 17.00 | 14 | 153 | 4.20 | 59.30 |
| 18 | 17.75 | 15 | 168 | 4.10 | 60.80 | |||
| 10 | 18.50 | 308.33 | 19 | 17.75 | 15 | 183 | 4.10 | 60.80 |
| 20 | 19.25 | 16 | 199 | 3.70 | 59.80 | |||
| 11 | 20.00 | 333.33 | 21 | 20.00 | 17 | 216 | 3.60 | 61.20 |
| 22 | 20.00 | 17 | 233 | 3.60 | 61.20 | |||
| 12 | 21.50 | 358.33 | 23 | 21.25 | 18 | 251 | 3.40 | 61.00 |
| 24 | 21.25 | 18 | 269 | 3.40 | 61.00 | |||
| Variable | Boys (n = 80) | Girls (n = 81) | Total (N = 161) |
|---|---|---|---|
| Age (year) | 15.30 ± 1.86 | 15.50 ± 1.73 | 15.40 ± 1.79 |
| Height (cm) | 170.60 ± 6.20 * | 159.40 ± 5.4 | 164.99 ± 8.10 |
| Weight (kg) | 63.66 ± 9.95 * | 54.69 ± 8.59 | 59.14 ± 10.29 |
| BMI (kg·m−2) | 21.82 ± 3.03 | 21.49 ± 3.04 | 21.65 ± 3.03 |
| Body fat (%) | 16.10 ± 8.00 * | 25.40 ± 8.20 | 20.77 ± 9.32 |
| Waist-hip ratio | 0.79 ± 0.05 * | 0.75 ± 0.05 | 0.77 ± 0.05 |
| VO2max (mL·kg−1·min−1) # | 52.79 ± 6.80 * | 40.91 ± 6.33 | 46.77 ± 8.85 |
| Variable | n | Stationary | Portable | SEE | p | r # |
|---|---|---|---|---|---|---|
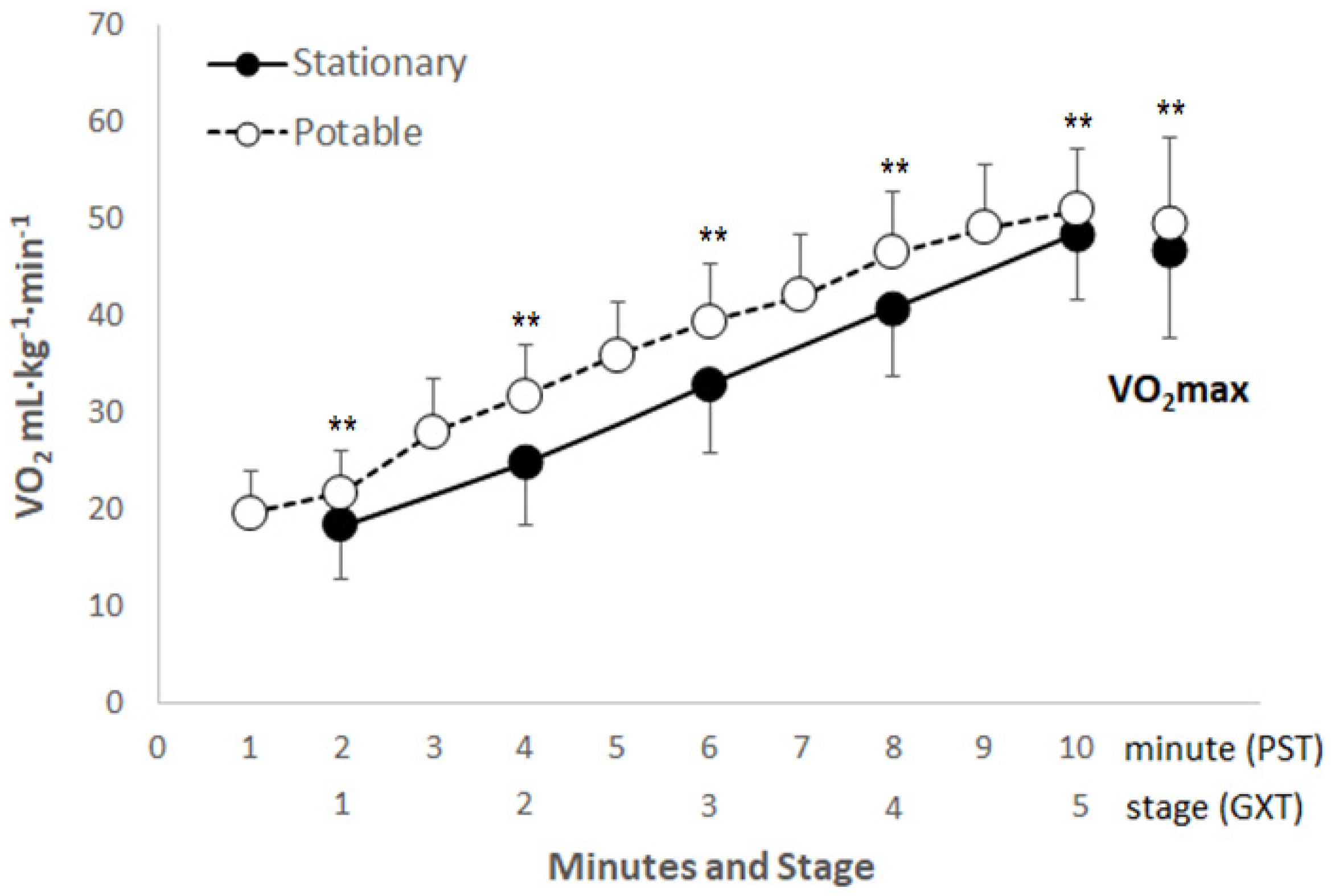
| VO2max (mL·kg−1·min−1) | 140 | 46.61 ± 8.92 | 49.56 ± 8.73 ** | 1.350 | 0.000 | 0.922 ** |
| Last speed (km·h−1) | 140 | 10.60 ± 1.65 | 10.95 ± 1.31 ** | 0.787 | 0.001 | 0.724 ** |
| Test duration (min. sec) | 142 | 8.10 ± 2.24 | 7.58 ± 1.47 | 1.262 | 0.169 | 0.689 ** |
| HRmax (bpm) | 142 | 195.74 ± 7.51 | 199.01 ± 6.82 ** | 5.991 | 0.000 | 0.578 ** |
| Variable | Trial | Male (n = 78) | Female (n = 81) | Total (n = 159) | p | r# |
|---|---|---|---|---|---|---|
| # of Laps (repetition) | 1st | 70.43 ± 14.64 a,** | 48.48 ± 9.18 | 59.25 ± 16.38 | T: 0.276 S: 0.000 T × S: 0.817 | 0.955 ** |
| 2nd | 69.62 ± 13.11 a,** | 48.15 ± 10.07 | 58.83 ± 15.95 | |||
| Last speed (km·h−1) | 1st | 12.24 ± 1.12 a,** | 10.49 ± 9.18 | 11.35 ± 1.30 | T: 0.447 S: 0.000 T × S: 0.447 | 0.932 ** |
| 2nd | 12.18 ± 1.00 a,** | 10.49 ± 10.07 | 11.32 ± 1.26 | |||
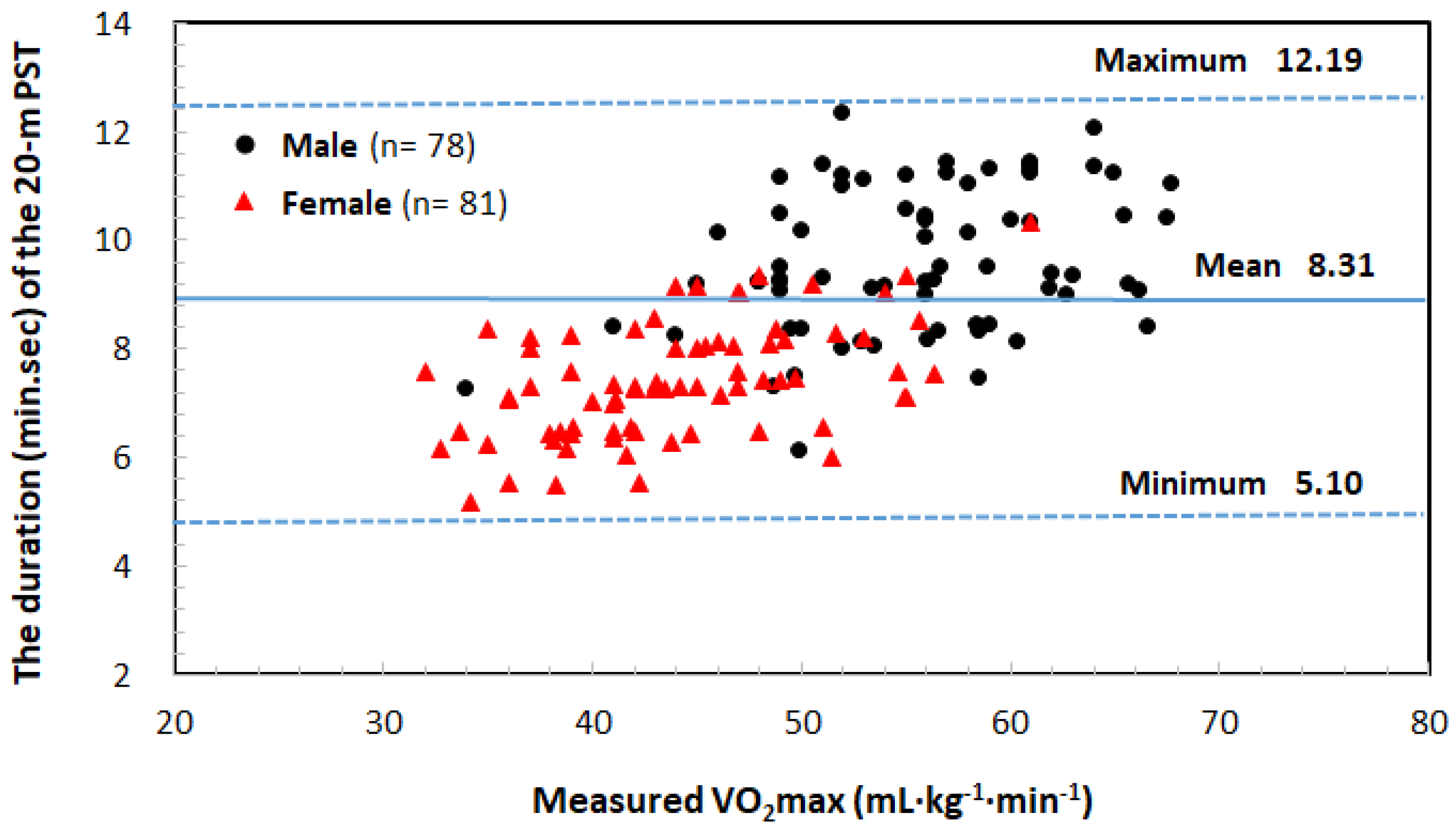
| Test duration (min.sec) | 1st | 9.40 ± 1.28 a,** | 7.25 ± 1:04 | 8.32 ± 1.42 | T: 0.628 S: 0.000 T × S: 0.475 | 0.944 ** |
| 2nd | 9.41 ± 1.19 a,** | 7.22 ± 1:11 | 8.30 ± 1.42 | |||
| HRmax (bpm) | 1st | 204.24 ± 7.90 a,*,b,** | 201.35 ± 7.05 b,** | 202.77 ± 7.59 | T: 0.000 S: 0.008 T × S: 0.809 | 0.795 ** |
| 2nd | 201.92 ± 7.53 a,** | 198.84 ± 7.05 | 200.35 ± 7.43 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Song, J.-R.; Kim, Y.-J.; Kim, S.-J.; Park, H.; Kim, C.-S.; Kwak, H.-B.; Kang, J.-H.; Park, D.-H. New 20 m Progressive Shuttle Test Protocol and Equation for Predicting the Maximal Oxygen Uptake of Korean Adolescents Aged 13–18 Years. Int. J. Environ. Res. Public Health 2019, 16, 2265. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132265
Lee S-H, Song J-R, Kim Y-J, Kim S-J, Park H, Kim C-S, Kwak H-B, Kang J-H, Park D-H. New 20 m Progressive Shuttle Test Protocol and Equation for Predicting the Maximal Oxygen Uptake of Korean Adolescents Aged 13–18 Years. International Journal of Environmental Research and Public Health. 2019; 16(13):2265. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132265
Chicago/Turabian StyleLee, Sang-Hyun, Jung-Ran Song, Yang-Jung Kim, Su-Jin Kim, Hyuk Park, Chang-Sun Kim, Hyo-Bum Kwak, Ju-Hee Kang, and Dong-Ho Park. 2019. "New 20 m Progressive Shuttle Test Protocol and Equation for Predicting the Maximal Oxygen Uptake of Korean Adolescents Aged 13–18 Years" International Journal of Environmental Research and Public Health 16, no. 13: 2265. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132265