Perceptions of Nature and Access to Green Space in Four Urban Neighborhoods

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Recruitment
2.3. Procedures
2.4. Coding and Data Analysis
2.5. Trustworthiness
3. Results
3.1. First Described are the Participant and Neighborhood Characteristics Followed by a Presentation of the Three Themes that Emerged and Findings Related to Perceptions of Physician Generated Nature Prescriptions
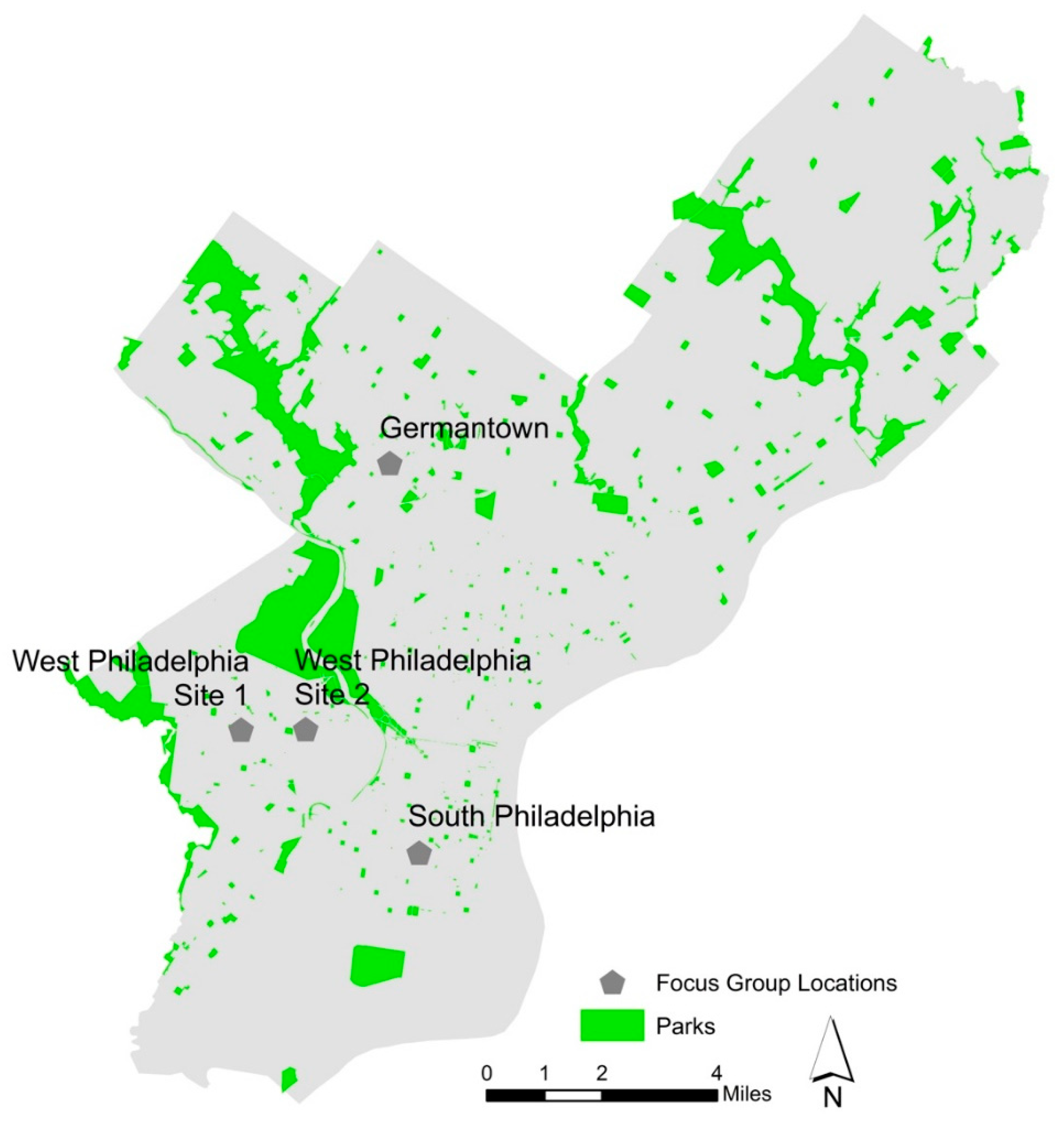
3.1.1. Participant and Neighborhood Characteristics
3.1.2. Access to Information
3.2. Themes
3.2.1. Perceived Benefits of Being in Nature
Being a mom of little ones, I spend at least four days a week in the park. I actually enjoy it…We could be out riding our bikes. I love picnics…The kids love the geese. We’ll take some pieces of bread. So I enjoy the outdoor life. I enjoy the park life. And it’s free, so I love it.
3.2.2. Barriers to Time Spent in Nature
“I know this is illegal, but there should be a park if you just want to do illegal stuff. For all of you who want to do illegal activity, this is your park. But the rest of us who just want to play cards or play checkers, or just want to have clean fun, this is ours.”
“That park was grimy for years. But with gentrification, then they want to fix it up. I’m like why didn’t you fix it up when my son was 3? Now you wait until…you’re trying to attract more Caucasians.”
“… [the city] can spend a lot of money and taxes in one section, and then in another section you’re only spending $ 1000 or $ 500–$ 800 in taxes. And it’s just not the same. And that’s the messed [up] part. It’s basically saying well, if you’re poor, then you don’t get to have a safe park. But if you can afford to pay this extra, then we’ll look out for you.”
3.2.3. Desired Features of Outdoor Green Spaces
“For me, my reason for driving the longer distance as opposed to staying local, it’s for number one, safety reasons. Number two, it’s cleaner. The atmosphere is better. Safety, the atmosphere is cleaner, the beauty of going far out. You would never catch me at some more local parks.”
“…a lot of people say to get outside more, especially to the young folks in our community, but there’s not technically a lot of things for us to do outside. So give us some activities…”Ideas generated included giveaways such as free Frisbees and passes for bike rentals which could provide youth with more structured play.
3.3. Perceptions of Physician Generated Nature Prescriptions
“If my pediatrician recommended that we spend more time outdoors, my response would be like ‘Wow, that’s interesting. Because we was planning to go to the park when we left here.’ So I would be excited to know that what I’ve been doing all along actually helps or should be done. And I would ask him, ‘Do you have any – a list of parks to share that I haven’t been to yet?’...I would be really enthused at the fact that what I’ve been doing all along is what needs to be done.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe-Nelson, C.; Kelly, S.; Kennedy, M.; Cherrie, J.W. A Scoping Review of Mapping Research on Green Space and Associated Mental Health Benefits. Int. J. Environ. Res. Public Health 2019, 16, 2081. [Google Scholar] [CrossRef] [PubMed]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through 2017. Curr. Environ. Health Reports 2018, 5, 77–87. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to greenness and mortality in a nationwide prospective cohort study of women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef] [PubMed]
- Christian, H.; Zubrick, S.R.; Foster, S.; Giles-Corti, B.; Bull, F.; Wood, L.; Knuiman, M.; Brinkman, S.; Houghton, S.; Boruff, B. The influence of the neighborhood physical environment on early child health and development: A review and call for research. Health Place 2015, 33, 25–36. [Google Scholar] [Green Version]
- Lovasi, G.S.; Jacobson, J.S.; Quinn, J.W.; Neckerman, K.M.; Ashby-Thompson, M.N.; Rundle, A. Is the environment near home and school associated with physical activity and adiposity of urban preschool children? J. Urban Health 2011, 88, 1143–1157. [Google Scholar] [CrossRef]
- Berman, M.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef]
- Beyer, K.M.; Kaltenbach, A.; Szabo, A.; Bogar, S.; Nieto, F.J.; Malecki, K.M. Exposure to neighborhood green space and mental health: Evidence from the survey of the health of Wisconsin. Int. J. Environ. Res. Public Health 2014, 11, 3453–3472. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [Green Version]
- Maas, J.; Van Dillen, S.M.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [Green Version]
- Hartig, T. Green space, psychological restoration, and health inequality. Lancet 2008, 372, 1614–1615. [Google Scholar] [CrossRef]
- Ward Thompson, C.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Kuo, F.E. Coping with poverty: Impacts of environment and attention in the inner city. Environ. Behav. 2001, 33, 5–34. [Google Scholar] [CrossRef]
- Kuo, F.E.; Sullivan, W.C. Aggression and Violence in the Inner City: Effects of Environment via Mental Fatigue. Environ. Behav. 2001, 33, 543–571. [Google Scholar] [CrossRef]
- Taylor, A.F.; Kuo, F.E. Children with attention deficits concentrate better after walk in the park. J. Attention. Disord. 2009, 12, 402–409. [Google Scholar] [CrossRef]
- Razani, N.; Morshed, S.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Alqassari, M.; Agodi, A.; Rutherford, G.W. Effect of park prescriptions with and without group visits to parks on stress reduction in low-income parents: SHINE randomized trial. PLoS ONE 2018, 13, e0192921. [Google Scholar] [CrossRef] [PubMed]
- Wells, N.M.; Evans, G.W. Nearby nature a buffer of life stress among rural children. Environ. Behav. 2003, 35, 311–330. [Google Scholar] [CrossRef]
- Fair, M.L.; Kaczynski, A.T.; Hughey, S.M.; Besenyi, G.M.; Powers, A.R. An Initiative to Facilitate Park Usage, Discovery, and Physical Activity Among Children and Adolescents in Greenville County, South Carolina, 2014. Prev. Chronic Dis. 2017, 14, E14. [Google Scholar] [CrossRef] [Green Version]
- Kuo, F.E.; Sullivan, W.C.; Coley, R.L.; Brunson, L. Fertile ground for community: Inner-city neighborhood common spaces. Am. J. Commun. Psychol. 1998, 26, 823–851. [Google Scholar] [CrossRef]
- Kweon, B.-S.; Sullivan, W.C.; Wiley, A.R. Green common spaces and the social integration of inner-city older adults. Environ. Behav. 1998, 30, 832–858. [Google Scholar] [CrossRef]
- Salvo, D.; Banda, J.A.; Sheats, J.L.; Winter, S.J.; Lopes dos Santos, D.; King, A.C. Impacts of a Temporary Urban Pop-Up Park on Physical Activity and Other Individual- and Community-Level Outcomes. J. Urban Health 2017, 94, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Tiesler, C.M.; Fuertes, E.; Romanos, M.; Dadvand, P.; Nieuwenhuijsen, M.J.; Berdel, D.; Koletzko, S.; Heinrich, J. Access to urban green spaces and behavioural problems in children: results from the GINIplus and LISAplus studies. Environ. Int. 2014, 71, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Amoly, E.; Dadvand, P.; Forns, J.; López-Vicente, M.; Basagaña, X.; Julvez, J.; Alvarez-Pedrerol, M.; Nieuwenhuijsen, M.J.; Sunyer, J. Green and blue spaces and behavioral development in Barcelona schoolchildren: the BREATHE project. Environ. Health Perspect. 2014, 122, 1351. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.F.; Kuo, F.E.; Sullivan, W.C. Coping with ADD: The surprising connection to green play settings. Environ. Behav. 2001, 33, 54–77. [Google Scholar] [CrossRef]
- Faber Taylor, A.; Kuo, F.E. Could Exposure to Everyday Green Spaces Help Treat ADHD? Evidence from Children’s Play Settings. Appl. Psychol. Health Well-Being 2011, 3, 281–303. [Google Scholar] [CrossRef]
- Yasuda, K. Priorities for 2019 focus on health of children and physicians. Letter from the President. AAP News, 2 January 2019. [Google Scholar]
- Chaput, J.-P.; Tremblay, M.S.; Katzmarzyk, P.T.; Fogelholm, M.; Mikkilä, V.; Hu, G.; Lambert, E.V.; Maher, C.; Maia, J.; Olds, T.; et al. Outdoor time and dietary patterns in children around the world. J. Public Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Aggio, D.; Gardner, B.; Roberts, J.; Johnstone, J.; Stubbs, B.; Williams, G.; López Sánchez, G.F.; Smith, L. Correlates of children’s independent outdoor play: Cross-sectional analyses from the Millennium Cohort Study. Prev. Med. Rep. 2017, 8, 10–14. [Google Scholar] [CrossRef]
- Larouche, R.; Garriguet, D.; Tremblay, M.S. Outdoor time, physical activity and sedentary time among young children: The 2012–2013 Canadian Health Measures Survey. Can. J. Public Health 2017, 107, 500–506. [Google Scholar] [CrossRef]
- Moran, M.R.; Plaut, P.; Merom, D. Is the Grass Always Greener in Suburban Neighborhoods? Outdoors Play in Suburban and Inner-City Neighborhoods. Int. J. Environ. Res. Public Health 2017, 14, 759. [Google Scholar] [CrossRef]
- Boone, C.G.; Buckley, G.L.; Grove, J.M.; Sister, C. Parks and people: An environmental justice inquiry in Baltimore, Maryland. Ann. Assoc. Am. Geogr. 2009, 99, 767–787. [Google Scholar] [CrossRef]
- Sister, C.; Wolch, J.; Wilson, J. Got green? Addressing environmental justice in park provision. GeoJournal 2010, 75, 229–248. [Google Scholar] [CrossRef]
- Das, K.V.; Fan, Y.; French, S.A. Park-use behavior and perceptions by race, Hispanic origin, and immigrant status in Minneapolis, MN: implications on park strategies for addressing health disparities. J. Immigr. Minor. Health 2017, 19, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; Rudick, J.; McKenzie, T.L. Neighborhood poverty, park use, and park-based physical activity in a Southern California city. Soc. Sci. Med. 2012, 75, 2317–2325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Han, B.; Cohen, D.A.; Derose, K.P. Contributions of Neighborhood Parks to Physical Activity in High-Poverty Urban Neighborhoods. J. Urban Health 2018, 95, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Derose, K.P.; Han, B.; Williamson, S.; Cohen, D.A. Gender Disparities in Park Use and Physical Activity among Residents of High-Poverty Neighborhoods in Los Angeles. Womens Health Issues 2018, 28, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Cohen, D.A.; Lapham, S.; Evenson, K.R.; Williamson, S.; Golinelli, D.; Ward, P.; Hillier, A.; McKenzie, T.L. Use of neighbourhood parks: does socio-economic status matter? A four-city study. Public Health 2013, 127, 325–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groff, E.; McCord, E.S. The role of neighborhood parks as crime generators. Secur. J. 2012, 25, 1–24. [Google Scholar] [CrossRef]
- Han, B.; Cohen, D.A.; Derose, K.P.; Li, J.; Williamson, S. Violent crime and park use in low-income urban neighborhoods. Am. J. Prev. Med. 2018, 54, 352–358. [Google Scholar] [CrossRef]
- Groshong, L.; Wilhelm Stanis, S.A.; Kaczynski, A.T.; Hipp, J.A. Attitudes About Perceived Park Safety Among Residents in Low-Income and High Minority Kansas City, Missouri, Neighborhoods. Environ. Behav. 2018, 0013916518814291. [Google Scholar] [CrossRef]
- Cohen, D.A.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; Raaen, L.; McKenzie, T.L. The paradox of parks in low-income areas: Park use and perceived threats. Environ. Behav. 2016, 48, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Dolash, K.; He, M.; Yin, Z.; Sosa, E.T. Factors that influence park use and physical activity in predominantly Hispanic and low-income neighborhoods. J. Phys. Act. Health 2015, 12, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Greer, A.E.; Castrogivanni, B.; Marcello, R. Park use and physical activity among mostly low-to-middle income, minority parents and their children. J. Phys. Act. Health 2017, 14, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak, A. The contribution of local parks to neighbourhood social ties. Landsc. Urban Plan. 2013, 109, 31–44. [Google Scholar] [CrossRef]
- Broyles, S.T.; Mowen, A.J.; Theall, K.P.; Gustat, J.; Rung, A.L. Integrating social capital into a park-use and active-living framework. Am. J. Prev. Med. 2011, 40, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Sturm, R.; Cohen, D. Proximity to urban parks and mental health. J. Ment. Health Policy Econ. 2014, 17, 19. [Google Scholar]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- South, E.C.; Hohl, B.C.; Kondo, M.C.; MacDonald, J.M.; Branas, C.C. Effect of Greening Vacant Land on Mental Health of Community-Dwelling Adults: A Cluster Randomized Trial. JAMA Netw. Open 2018, 1, e180298. [Google Scholar] [CrossRef]
- Institute at the Golden Gate. National ParkRx Initiative Website. Available online: https://parkrx.org (accessed on 27 June 2019).
- National Recreation and Park Association. Prescribing Parks for Better Health Success Stories. Available online: http://parkrx.org/sites/default/files/final-prescribing-parks-for-better-health-success-stories.pdf (accessed on 28 June 2019).
- Groshong, L.; Stanis, S.A.W.; Kaczynski, A.T.; Hipp, J.A.; Besenyi, G.M. Exploring Attitudes, Perceived Norms, and Personal Agency: Insights Into Theory-Based Messages to Encourage Park-Based Physical Activity in Low-Income Urban Neighborhoods. J. Phys. Act. Health 2017, 14, 108–116. [Google Scholar] [CrossRef]
- Cohen, D.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; Raaen, L.; McKenzie, T.L. Promoting Physical Activity in High-Poverty Neighborhood Parks. Soc. Sci. Med. 2017, 186, 130–138. [Google Scholar] [CrossRef]
- Uijtdewilligen, L.; Waters, C.N.-H.; Aw, S.; Wong, M.L.; Sia, A.; Ramiah, A.; Wong, M.; Müller-Riemenschneider, F. The Park Prescription Study: Development of a community-based physical activity intervention for a multi-ethnic Asian population. PLoS ONE 2019, 14, e0218247. [Google Scholar] [CrossRef]
- Kim, H.; Sefcik, J.S.; Bradway, C. Characteristics of qualitative descriptive studies: A systematic review. Res. Nurs. Health 2017, 40, 23–42. [Google Scholar]
- Sandelowski, M. Focus on research methods-whatever happened to qualitative description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Hennink, M.M. Focus Group Discussion: Understanding Qualitative Research; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Lincoln, Y.; Guba, E. Naturalistic Inquiry; Sage: Thousands Oaks, CA, USA, 1985. [Google Scholar]
- Razani, N.; Kohn, M.A.; Wells, N.M.; Thompson, D.; Flores, H.H.; Rutherford, G.W. Design and evaluation of a park prescription program for stress reduction and health promotion in low-income families: The Stay Healthy in Nature Everyday (SHINE) study protocol. Contemp. Clin. Trials 2016, 51, 8–14. [Google Scholar] [CrossRef]
- Razani, N.; Niknam, K.; Wells, N.M.; Thompson, D.; Hills, N.K.; Kennedy, G.; Gilgoff, R.; Rutherford, G.W. Clinic and park partnerships for childhood resilience: A prospective study of park prescriptions. Health Place 2019, 57, 179–185. [Google Scholar] [CrossRef]


{kind=link}
| Demographics | N (%) |
|---|---|
| Gender | |
| Female | 30 (71.4%) |
| Male | 9 (21.4%) |
| Missing | 3 (7.1%) |
| Age | |
| 18–24 | 4 (9.5%) |
| 25–34 | 5 (12%) |
| 35–44 | 11 (26.2%) |
| 45–54 | 9 (21.4%) |
| 55–64 | 6 (14.2%) |
| 65–74 | 2 (4.8%) |
| Missing | 5 (12%) |
| Race (self-defined) | |
| Black | 31 (73.8%) |
| Biracial | 1 (2.4%) |
| White | 1 (2.4%) |
| Mediterranean/MidEastern | 1 (2.4%) |
| Puerto Rican | 1 (2.4%) |
| Missing | 7 (16.7%) |
| Neighborhood Characteristics | Focus Group Location | |||
|---|---|---|---|---|
| South Philadelphia | West Philadelphia Site 1 | West Philadelphia Site 2 | Germantown | |
| Racial makeup, % | ||||
| White | 36 | 1 | 4 | 7 |
| Black/African American | 19 | 98 | 91 | 92 |
| Asian | 43 | 0 | 0 | 1 |
| Family Households, % | ||||
| Male Householder, No Wife Present | 8 | 12 | 12 | 8 |
| Female Householder, No Husband Present | 17 | 25 | 32 | 25 |
| Median Household Income (In 2016 Inflation Adjusted Dollars) | $42,903 | $26,814 | $20,840 | $31,299 |
| Renter Occupied Housing Units, % | 43 | 52 | 74 | 52 |
| Population Living Below Poverty, % | 23 | 28 | 41 | 34 |
| Category | Resource |
|---|---|
| • Internet resources | • MeetUp.com; • Social Media outlets; • Facebook; • Facebook groups; • Twitter; • LinkedIn; • Township websites; • Using Google. |
| • Postings in the community | • Fliers; • At the library; • At community centers. |
| • Advertisements | • Local TV stations; • Community newspapers. |
| • Personal networks | • Word-of-mouth. |
| Barriers | Specific Concerns |
|---|---|
| Safety concerns |
|
| Dislike of things associated with nature environments |
|
| Financial hardship |
|
| Medical conditions affecting physical function |
|
| Outdoor conditions |
|
| Physical conditions of spaces |
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sefcik, J.S.; Kondo, M.C.; Klusaritz, H.; Sarantschin, E.; Solomon, S.; Roepke, A.; South, E.C.; Jacoby, S.F. Perceptions of Nature and Access to Green Space in Four Urban Neighborhoods. Int. J. Environ. Res. Public Health 2019, 16, 2313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132313
Sefcik JS, Kondo MC, Klusaritz H, Sarantschin E, Solomon S, Roepke A, South EC, Jacoby SF. Perceptions of Nature and Access to Green Space in Four Urban Neighborhoods. International Journal of Environmental Research and Public Health. 2019; 16(13):2313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132313
Chicago/Turabian StyleSefcik, Justine S., Michelle C. Kondo, Heather Klusaritz, Elisa Sarantschin, Sara Solomon, Abbey Roepke, Eugenia C. South, and Sara F. Jacoby. 2019. "Perceptions of Nature and Access to Green Space in Four Urban Neighborhoods" International Journal of Environmental Research and Public Health 16, no. 13: 2313. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16132313