Insights Following Implementation of an Exercise Intervention in Older Veterans with PTSD

Abstract
:1. Introduction
2. Materials and Methods
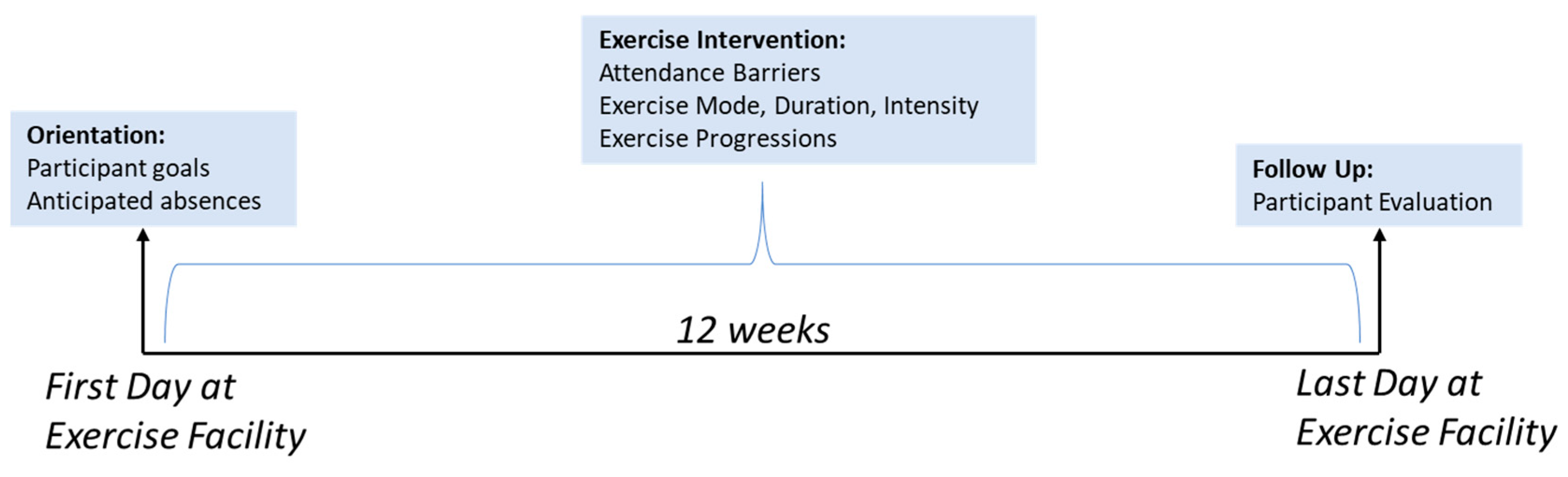
2.1. Exercise Intervention
2.2. Setting and Participants
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Participant Goals
3.3. Exercise Prescription
3.4. Adherance and Attendance Barriers
3.5. Program Evaluations
4. Discussion
4.1. Participant Goals
4.2. Participation Barriers
4.3. Tailoring
4.4. Additional Future Considerations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

References
- Windle, G.; Hughes, D.; Linck, P.; Russell, I.; Woods, B. Is exercise effective in promoting mental well-being in older age? A systematic review. Aging Ment. Health 2010, 14, 652–669. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Wetherell, J.L.; Petkus, A.J.; Thorp, S.R.; Stein, M.B.; Chavira, D.A.; Campbell-Sills, L.; Craske, M.G.; Sherbourne, C.; Bystritsky, A.; Sullivan, G.; et al. Age differences in treatment response to a collaborative care intervention for anxiety disorders. Br. J. Psychiatry 2013, 203, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopra, M.P.; Zhang, H.; Pless Kaiser, A.; Moye, J.A.; Llorente, M.D.; Oslin, D.W.; Spiro, A. PTSD is a chronic, fluctuating disorder affecting the mental quality of life in older adults. Am. J. Geriatr. Psychiat. 2014, 22, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Marmar, C.R.; Schlenger, W.; Henn-Haase, C.; Qian, M.; Purchia, E.; Li, M.; Corry, N.; Williams, C.S.; Ho, C.L.; Horesh, D.; et al. Course of posttraumatic stress disorder 40 years after the Vietnam war: Findings from the National Vietnam Veterans Longitudinal Study. JAMA Psychiat 2015, 72, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Dedert, E.A.; Calhoun, P.S.; Watkins, L.L.; Sherwood, A.; Beckham, J.C. Posttraumatic stress disorder, cardiovascular, and metabolic disease: A review of the evidence. Ann. Behav. Med. 2010, 39, 61–78. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.S.; Beckham, J.C.; Bosworth, H.B.; Sloane, R.; Pieper, C.F.; Morey, M.C. PTSD is negatively associated with physical performance and physical function in older overweight military Veterans. J. Rehabil. Res. Dev. 2014, 51, 285–295. [Google Scholar] [CrossRef]
- Levine, A.B.; Levine, L.M.; Levine, T.B. Posttraumatic stress disorder and cardiometabolic disease. Cardiology 2014, 127, 1–19. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Goldstein, R.B.; Southwick, S.M.; Grant, B.F. Physical health conditions associated with posttraumatic stress disorder in U.S. older adults: Results from wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Am. Geriatr. Soc. 2012, 60, 296–303. [Google Scholar] [CrossRef]
- van den Berk-Clark, C.; Secrest, S.; Walls, J.; Hallberg, E.; Lustman, P.J.; Schneider, F.D.; Scherrer, J.F. Association between posttraumatic stress disorder and lack of exercise, poor diet, obesity, and co-occuring smoking: A systematic review and meta-analysis. Health Psychol. 2018, 37, 407–416. [Google Scholar] [CrossRef]
- Whitworth, J.W.; Ciccolo, J.T. Exercise and Post-Traumatic Stress Disorder in Military Veterans: A Systematic Review. Mil. Med. 2016, 181, 953–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouldin, E.D.; Reiber, G.E. Physical Activity among Veterans and Nonveterans with Diabetes. J. Aging. Res. 2012, 2012, 135–192. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, S.; Vancampfort, D.; Steel, Z.; Newby, J.; Ward, P.B.; Stubbs, B. Physical activity in the treatment of Post-traumatic stress disorder: A systematic review and meta-analysis. Psychiatry Res. 2015, 230, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, S.; Sherrington, C.; Tiedemann, A. Exercise augmentation compared with usual care for post-traumatic stress disorder: A randomized controlled trial. Acta Psychiatr. Scand. 2015, 131, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Davidson, C.L.; Babson, K.A.; Bonn-Miller, M.O.; Souter, T.; Vannoy, S. The impact of exercise on suicide risk: Examining pathways through depression, PTSD, and sleep in an inpatient sample of veterans. Suicide Life Threat Behav. 2013, 43, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, J.W.; Craft, L.L.; Dunsiger, S.I.; Ciccolo, J.T. Direct and indirect effects of exercise on posttraumatic stress disorder symptoms: A longitudinal study. Gen. Hosp. Psychiat. 2017, 49, 56–62. [Google Scholar] [CrossRef]
- Lu, M.W.; Carlson, K.F.; Duckart, J.P.; Dobscha, S.K. The effects of age on initiation of mental health treatment after positive PTSD screens among Veterans Affairs primary care patients. Gen. Hosp. Psychiat. 2012, 34, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Crombie, K.; Leitzelar, B.; Brellenthin, A.; Hilliard, C.; Koltyn, K. Loss of exercise- and stress-induced increases in circulating 2-arachidonoylglycerol concentrations in adults with chronic PTSD. Biol. Psychol. 2019, 145, 1–7. [Google Scholar] [CrossRef]
- Crombie, K.; Brellenthin, A.; Hillard, C.; Koltyn, K. Psychobiological Responses to Aerobic Exercise in Individuals with Posttraumatic Stress Disorder. J. Trauma. Stress. 2018, 31, 134–135. [Google Scholar] [CrossRef]
- Maguen, S.; Hoerster, K.D.; Littman, A.J.; Klingaman, E.A.; Evans-Hudnall, G.; Holleman, R.; Kim, H.M.; Goodrich, D.E. Iraq and Afghanistan veterans with PTSD participate less in VA’s weight loss program than those without PTSD. J. Affect. Disord. 2016, 193, 289–294. [Google Scholar] [CrossRef]
- Hall, K.S.; Gregg, J.; Bosworth, H.B.; Beckham, J.C.; Hoerster, K.D.; Sloane, R.; Morey, M.C. Physical activity counseling promotes physical and psychological resilience in older veterans with posttraumatic stress disorder. Ment. Health Phys. Act. 2016, 11, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babson, K.A.; Heinz, A.J.; Ramirez, G.; Puckett, M.; Irons, J.G.; Bonn-Miller, M.O.; Woodward, S.H. The interactive role of exercise and sleep on veteran recovery from symptoms of PTSD. Ment. Health Phys. Act. 2015, 8, 15–20. [Google Scholar] [CrossRef]
- Manger, T.A.; Motta, R.W. The impact of an exercise program on posttraumatic stress disorder, anxiety, and depression. Int. J. Emerg. Ment. Health. 2005, 7, 49–57. [Google Scholar] [PubMed]
- Pratt, S.I.; Jerome, G.J.; Schneider, K.L.; Craft, L.L.; Buman, M.P.; Stoutenberg, M.; Daumit, G.L.; Bartels, S.J.; Goodrich, D.E. Increasing US health plan coverage for exercise programming in community mental health settings for people with serious mental illness: A position statement from the Society of Behavior Medicine and the American College of Sports Medicine. Transl. Behav. Med. 2016, 6, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.S.; Hoerster, K.D.; Yancy, W.S., Jr. Post-traumatic stress disorder, physical activity, and eating behaviors. Epidemiol. Rev. 2015, 37, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Harada, N.D.; Wilkins, S.S.; Schneider, B.; Elrod, M.; Hahn, T.J.; Kleinman, L.; Fang, M.; Dhanani, S. The influence of depression and PTSD on exercise adherence in older veterans. Mil. Behav. Health 2013, 1, 146–151. [Google Scholar] [CrossRef]
- Slade, S.; Dionne, C.; Underwood, M.; Buchbinder, R. Consensus on Exercise Reporting Template (CERT): Explanation and Elaboration Statement. Br. J. Sports Med. 2016, 50, 1425. [Google Scholar] [CrossRef]
- Hall, K.S.; Morey, M.C.; Beckham, J.C.; Bosworth, H.B.; Pebole, M.M.; Pieper, C.F.; Sloane, R. The Warrior Wellness Study: A Randomized Controlled Exercise Trial for Older Veterans with PTSD. Transl. J. Am. Coll. Sports Med. 2018, 3, 43–51. [Google Scholar]
- Hall, K.S.; Morey, M.C.; Bosworth, H.B.; Beckham, J.C.; Pebole, M.M.; Sloane, R.; Pieper, C.F. Pilot Randomized Controlled Trial of Exercise Training for Older Veterans with PTSD. Available online: https://0-link-springer-com.brum.beds.ac.uk/article/10.1007/s10865-019-00073-w (accessed on 23 July 2019).
- USA Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Physical Activity Guidelines for Americans; Department of Health and Human Services: Washington, DC, USA, 2008.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM–5 (CAPS-5): Development and initial psychometric evaluation in military veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Wortmann, J.H.; Jordan, A.H.; Weathers, F.W.; Resick, P.A.; Dondanville, K.A.; Hall-Clark, B.; Foa, E.B.; Young-McCaughan, S.; Yarvis, J.S.; Hembree, E.A.; et al. Psychometric analysis of the PTSD Checklist-5 (PCL-5) among treatment-seeking military service members. Psychol. Assess. 2016, 28, 1392–1403. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Rosenbaum, S.; Stubbs, B.; Gorczynski, P.; Yung, A.; Vancampfort, D. Motivating factors and barriers towards exercise in severe mental illness: A systematic review and meta-analysis. Psychol. Med. 2016, 46, 2869–2881. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.; I-Min, L.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health: Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 38, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Foster, D.; Wadden, T.A.; Phelan, S.; Sarwer, D.B.; Sanderson, R.S. Obese Patients’ Perceptions of Treatment Outcomes and the Factors That Influence Them. Arch. Intern. Med. 2001, 161, 2133–2139. [Google Scholar] [CrossRef] [PubMed]
- Foster, D.; Wadden, T.A.; Vogt, R.A.; Brewer, G. What is a reasonable weight loss? Patients’ expectations and evaluations of obesity treatment outcomes. J. Consult. Clin. Psychol. 1997, 65, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Crone, D.; Guy, H. I know it is only exercise, but to me it is something that keeps me going; A qualitative approach to understanding mental health service users’ experiences of sports therapy. Int. J. Ment. Health. Nurs. 2008, 17, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Soundy, A.; Faulkner, A.; Taylor, A. Exploring Variability and Perceptions of Lifestyle Physical Activity among Individuals with Severe and Enduring Mental Health Problems; A Qualitative Study. J. Men. Health 2007, 16, 493–503. [Google Scholar] [CrossRef]
- Ussher, M.; Stanbury, L.; Cheeseman, V.; Faulkner, G. Physical activity preferences and perceived barriers to activity among persons with severe mental illness in the United Kingdom. Psychiatr. Serv. 2007, 58, 405–408. [Google Scholar] [CrossRef] [PubMed]
- McDevitt, J.; Snyder, M.; Miller, A.; Wilbur, J. Perceptions of Barriers and Benefits to Physical Activity Among Outpatients in Psychiatric Rehabilitation. J. Nurs. Scholarsh. 2006, 38, 50–55. [Google Scholar] [CrossRef]
- Fogarty, M.; Happell, B. Exploring the benefits of an exercise program for people with schizophrenia: A qualitative study. Issues Ment. Health Nurs. 2005, 26, 341–351. [Google Scholar] [CrossRef]
- Vancampfort, D.; Madou, T.; Moens, H.; De Backer, T.; Vanhalst, P.; Helon, C.; Naert, P.; Rosenbaum, S.; Stubbs, B.; Probst, M. Could autonomous motivation hole the key to successfully implementing lifestyle changes in affective disorders? A multicenter cross sectional study. Psychiatry Res. 2015, 228, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Stubbs, B.; Venigalla, S.; Probst, M. Adopting and maintaining physical activity behaviours in people with severe mental illness: The importance of autonomous motivation. Prev. Med. 2015, 81, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Rosenbaum, S.; Schuch, F.; Ward, B.; Probst, M.; Stubbs, B. Prevalence and predictors of treatment dropout from physical activity interventions in schizophrenia: A meta-analysis. Gen. Hosp. Psychiatry 2016, 39, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Rosenbaum, S.; Schuch, F.; Ward, P.B.; Richards, J.; Mugisha, J.; Probst, M.; Stubbs, B. Cardiorespiratory fitness in severe mental illness: A systematic review and meta-analysis. Sports Medic. 2017, 47, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Shiner, B.; Whitley, R.; Van Vitters, A.; Pratt, S.; Bartels, S. Learning What Matters for Patients: Qualitative Evaluation of a Health Promotion Program for Those with Serious Mental Illness. Health Promot. Int. 2008, 23, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Raine, P.; Truman, C.; Southerst, A. The development of a community gym for people with mental health problems: Influences on psychological accessibility. J. Ment. Health 2002, 11, 43–53. [Google Scholar] [CrossRef]
- Soundy, A.; Freeman, P.; Stubbs, B.; Probst, M.; Coffee, P.; Vancampfort, D. The transcending benefits of physical activity for individuals with schizophrenia: A systematic review and meta-ethnography. Psychiatry Res. 2014, 220, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Kulka, R.A.; Schlenger, W.E.; Fairbank, J.A.; Hough, R.L.; Jordan, B.K.; Marmar, C.R.; Weiss, D.S. Trauma and the Vietnam War Generation; Brunner/Manzel: New York, NY, USA, 1990. [Google Scholar]
- Roberts, A.L.; Gilman, S.E.; Breslau, J.; Breslau, N.; Koenen, K.C. Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychol. Med. 2011, 41, 71–83. [Google Scholar] [CrossRef]
- Pebole, M.M.; Hall, K.S. Physical Activity Promotion in Women with PTSD: What we need for progress. Psychol. Sport Exerc. 2019, 41, 127–129. [Google Scholar] [CrossRef]
- Bucham, D.; Ollis, S.; Thomas, N.; Naker, J. Physical Activity Behavior: An overview of current and emergent theoretical practices. J. Obes. 2012, 2012, 11. [Google Scholar]


{kind=link}
| Variable | * M(SD) |
|---|---|
| Age (yrs) | 67.5 (3.3) Range: 60–76 |
| Sex (male), n (%) | 41 (91.1%) |
| Race (AA), n (%) | 40 (88.9%) |
| Comorbidities | 3.9 (1.7) |
| Overweight / Obese, n (%) | 37 (82.2%) |
| BMI (kg/m2) | 30.0 (5.6) Range: 21–47 |
| Education, ≥some college, n (%) | 28 (62.2%) |
| Depression (PHQ9; 0–24) [33] | 10.2 (5.2) 49% ≥ 10 score |
| PTSD symptoms (PCL-5; 0–80) [34] | 41.3 (14.5) Range: 13–70 |
| Item | Mean (SD) | Median (Min–Max) | N (%) * |
|---|---|---|---|
| Overall Review | |||
| ** Please circle your overall reaction to Warrior Wellness (1 = excellent; 4 = poor) | 1.1 (0.4) | 1 (1–2) | 37 (100%) |
| ** Please circle your overall reaction to the instructors (1 = excellent; 4 = poor) | 1 (0.2) | 1 (1–2) | 37 (100%) |
| ** Overall, how do you feel physically after completing the Warrior Wellness exercise program (1 = excellent; 4 = poor) | 1.6 (0.6) | 2 (1–3) | 35 (95%) |
| ** Overall, how do you feel mentally after completing the Warrior Wellness program (1 = excellent; 4 = poor) | 1.6 (0.6) | 2 (1–3) | 34 (92%) |
| Additional Comments | |||
| I plan to continue doing the exercises on my own (1 = strongly disagree; 4 = strongly agree) | 3.4 (0.7) | 4 (2–4) | 32 (86%) |
| I would recommend Warrior Wellness to other Veterans with PTSD (1 = strongly disagree; 4 = strongly agree) | 3.8 (0.4) | 4 (3–4) | 37 (100%) |
| Exercise Program | |||
| The exercises were too hard given my physical condition (1 = strongly disagree; 4 = strongly agree) | 1.6 (0.9) | 1 (1–4) | 3 (8%) |
| The exercise intensity progressed at an appropriate pace for me (1 = strongly disagree; 4 = strongly agree) | 3.6 (0.6) | 4 (2–4) | 36 (97%) |
| I enjoyed the selected exercises (1 = strongly disagree; 4 = strongly agree) | 3.6 (0.5) | 4 (3–4) | 37 (100%) |
| Exercise Environment | |||
| The time Warrior Wellness was held was convenient (1 = strongly disagree; 4 = strongly agree) | 3.7 (0.5) | 4 (2–4) | 36 (97%) |
| I felt comfortable in the exercise setting (1 = strongly disagree; 4 = strongly agree) | 3.7 (0.5) | 4 (2–4) | 36 (97%) |
| I feel emotionally close to others in the exercise group (1 = strongly disagree; 4 = strongly agree) | 3.2 (0.7) | 3 (1–4) | 26 (87%) |
| Instructors | |||
| The instructors helped me adapt the exercises to fit my level of ability (1 = strongly disagree; 4 = strongly agree) | 3.9 (0.3) | 4 (3–4) | 37 (100%) |
| I feel emotionally close to the instructors (1 = strongly disagree; 4 = strongly agree) | 3.5 (0.8) | 4 (1–4) | 28 (93%) |
| Future Study Considerations | |||
| I wish the program would have addressed diet/eating habits (1 = strongly disagree; 4 = strongly agree) | 3.2 (0.7) | 3 (2–4) | 30 (81%) |
| I wish my spouse or significant other could have participated in the program (1 = strongly disagree; 4 = strongly agree) | 3.4 (0.7) | 3 (2–4) | 30 (81%) |
| What type of exercise setting do you prefer | (54%) Mix of home- and facility-based (46%) Facility-based (0%) Home-based | ||
| How do you like to exercise? | (46%) In a group, doing my own routine (22%) Alone (16%) In a group, instructor-led class | ||
| Is the Warrior Wellness program length adequate? (12 weeks) | (40%) Not long enough (60%) Yes, 12 wks was adequate | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pebole, M.M.; Hall, K.S. Insights Following Implementation of an Exercise Intervention in Older Veterans with PTSD. Int. J. Environ. Res. Public Health 2019, 16, 2630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142630
Pebole MM, Hall KS. Insights Following Implementation of an Exercise Intervention in Older Veterans with PTSD. International Journal of Environmental Research and Public Health. 2019; 16(14):2630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142630
Chicago/Turabian StylePebole, Michelle M., and Katherine S. Hall. 2019. "Insights Following Implementation of an Exercise Intervention in Older Veterans with PTSD" International Journal of Environmental Research and Public Health 16, no. 14: 2630. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16142630