The Impact of Particulate Matter on Outdoor Activity and Mental Health: A Matching Approach


Abstract
:1. Introduction
2. Influence of Particulate Matter on Outdoor Activity and Mental Health
2.1. Particulate Matter and Outdoor Activity
2.2. Particulate Matter and Mental Health
3. Method
3.1. Data Source and Descriptions
3.2. Dependent Variables: Mental Health and Outdoor Walking Activity
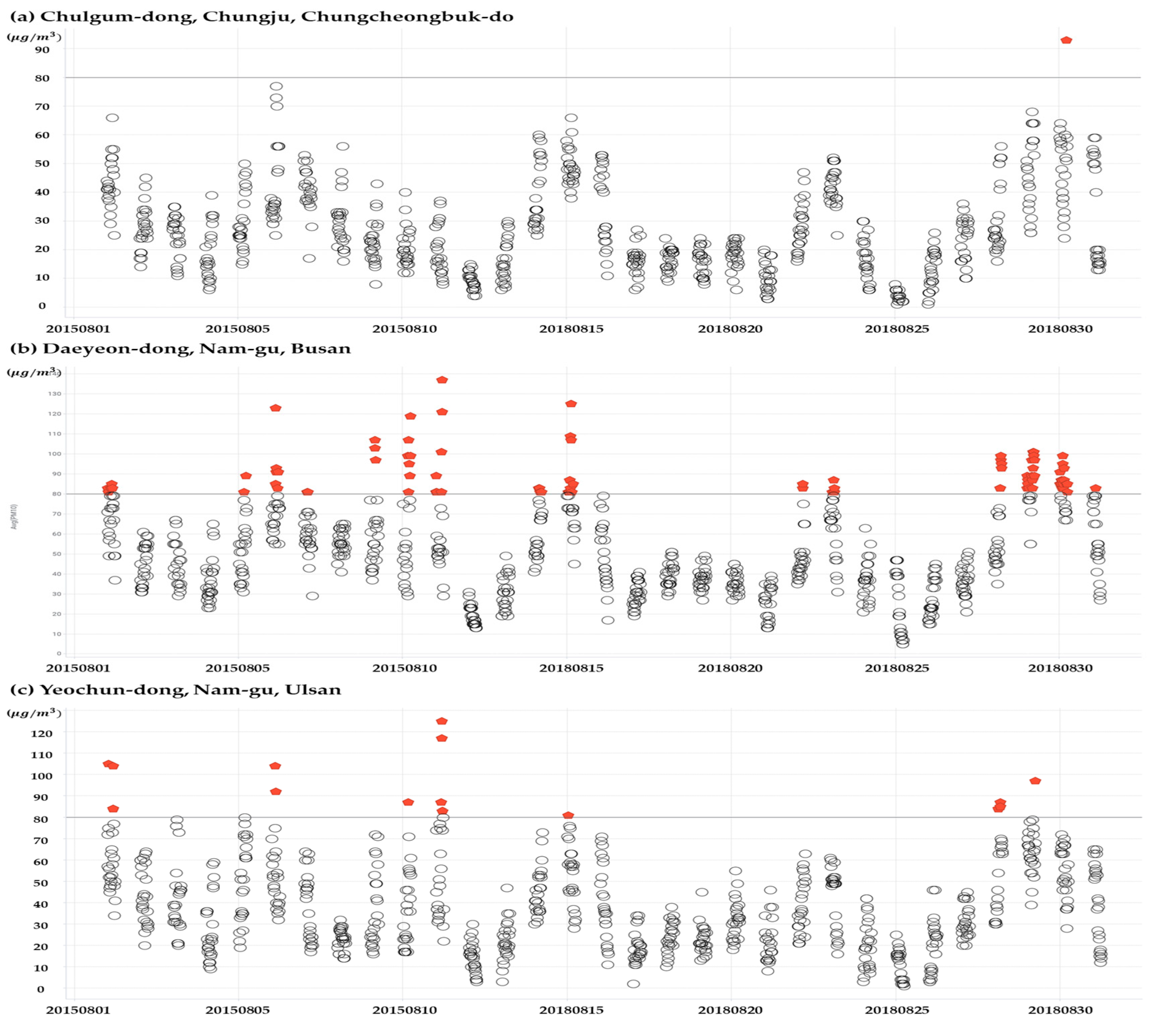
3.3. Exposure Levels of High PM10
3.4. Statistical Analysis
4. Results
4.1. Matching Variables of the Study Population and the PM10 Exposure Level
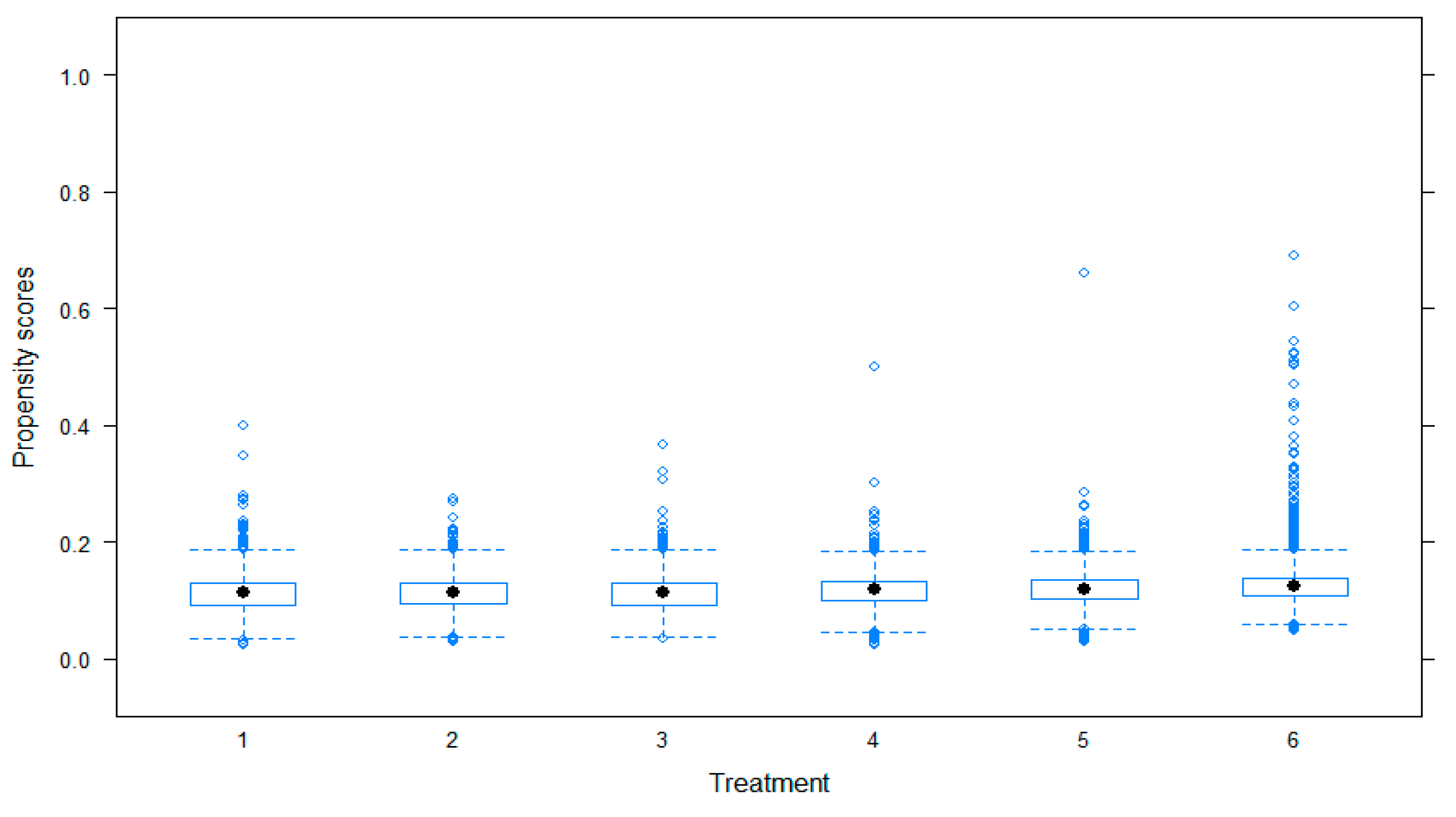
4.2. Assessment of Balance with Multiple Exposure Groups
4.3. Effects on Mental Health and Outdoor Walking Activity
4.4. Robustness Checks
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cohen, A.J.; Anderson, H.R.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Künzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; et al. The Global Burden of Disease due to Outdoor Air Pollution. J. Toxicol. Env. Health Part A 2005, 68, 1301–1307. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Christiani, D.; Ren, J. The global contribution of outdoor air pollution to the incidence, prevalence, mortality and hospital admission for chronic obstructive pulmonary disease: A systematic review and meta-analysis. Int. J. Env. Res. Public Health 2014, 11, 11822–11832. [Google Scholar] [CrossRef] [PubMed]
- Gurjar, B.R.; Butler, T.M.; Lawrence, M.G.; Lelieveld, J. Evaluation of emissions and air quality in megacities. Atmos. Environ. 2008, 42, 1593–1606. [Google Scholar] [CrossRef]
- Cohen, B. Urbanization in Developing Countries: Current Trends, Future Projections, and Key Challenges for Sustainability. Technol. Soc. 2006, 28, 63–80. [Google Scholar] [CrossRef]
- Viana, M.; Kuhlbusch, T.A.J.; Querol, X.; Alastuey, A.; Harrison, R.M.; Hopke, P.K.; Hueglin, C. Source apportionment of particulate matter in Europe: A review of methods and results. J. Aerosol Sci. 2008, 39, 827–849. [Google Scholar] [CrossRef]
- Xie, Y.; Dai, H.; Xu, X.; Fujimori, S.; Hasegawa, T.; Yi, K.; Masui, T.; Kurata, G. Co-benefits of climate mitigation on air quality and human health in Asian countries. Environ. Int. 2018, 119, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Guan, D.; Jiang, X.; Peng, L.; Schroeder, H.; Zhang, Q. Assessment of socioeconomic costs to China’s air pollution. Atmos. Environ. 2016, 139, 147–156. [Google Scholar] [CrossRef]
- Zhang, Y.L.; Cao, F. Fine particulate matter (PM 2.5) in China at a city level. Sci. Rep. 2015, 5, 14884. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010; a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Deutsche Bank. China: Big Bang Measures to Fight Air Pollution; Deutsche Bank: Frankfurt, Germany, 2013. [Google Scholar]
- Lee, S. Korea’s New Comprehensive Plan on Fine Dust and Its Implications for Policy and Research. Res. Brief 2018, 29, 1–7. [Google Scholar]
- Chung, A. Korea’s Policy towards Pollution and Fine Particle. Korea Anal. 2014, 2, 1–2. [Google Scholar]
- Penedo, F.J.; Dahn, J.R. Exercise and Well-Being: A Review of Mental and Physical Health Benefits Associated with Physical Activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Rothman, A.J.; Detweiler, J.B.; Steward, W.T. Emotional States and Physical Health. Am. Psychol. 2000, 55, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R. Racial Differences in Physical and Mental Health. J. Health Psychol. 1997, 2, 335–351. [Google Scholar] [CrossRef] [Green Version]
- Maté, T.; Guaita, R.; Pichiule, M.; Linares, C.; Díaz, J. Short-term effect of fine particulate matter (PM 2.5) on daily mortality due to diseases of the circulatory system in Madrid (Spain). Sci. Total Environ. 2010, 408, 5750–5757. [Google Scholar]
- Lavy, V.; Ebenstein, A.; Roth, S. The impact of short term exposure to ambient air pollution on cognitive performance and human capital formation (No. w20648). Natl. Bur. Econ. Res. 2014. [Google Scholar] [CrossRef]
- Weuve, J.; Puett, R.C.R.; Schwartz, J.; Yanosky, J.D.; Laden, F.; Grodstein, F. Exposure to Particulate Air Pollution and Cognitive Decline in Older Women. Arch. Intern. Med. 2012, 172, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szyszkowicz, M.; Rowe, B.; Colman, I. Air pollution and daily emergency department visits for depression. Int. J. Occup. Med. Environ. Health 2009, 22, 355–362. [Google Scholar] [CrossRef]
- Lim, Y.H.; Kim, H.; Kim, J.H.; Bae, S.; Park, H.Y.; Hong, Y.C. Air Pollution and Symptoms of Depression in Elderly Adults. Environ. Health Perspect. 2012, 120, 1023–1028. [Google Scholar] [CrossRef] [Green Version]
- Szyszkowicz, M.; Stieb, D.M.; Rowe, B.H. Air pollution and daily ED visits for migraine and headache in Edmonton, Canada. Am. J. Emerg. Med. 2009, 27, 391–396. [Google Scholar] [CrossRef]
- Szyszkowicz, M.; Willey, J.B.; Grafstein, E.; Rowe, B.H.; Colman, I. Air pollution and emergency department visits for suicide attempts in Vancouver, Canada. Environ. Health Insights 2010, 4, EHI-S5662. [Google Scholar] [CrossRef]
- Baum, A.; Fleming, R.; Singer, J.E. Stress at Three Mile Island: Applying psychological impact analysis. Appl. Soc. Psychol. Annu. 1982, 3, 217–248. [Google Scholar]
- Graff Zivin, J.; Neidell, M. The Impact of Pollution on Worker Productivity. Am. Econ. Rev. 2012, 102, 3652–3673. [Google Scholar] [CrossRef] [Green Version]
- Andersen, Z.J.; de Nazelle, A.; Mendez, M.A.; Garcia-Aymerich, J.; Hertel, O.; Tjonneland, A.; Overvad, K.; Raaschou-Nielsen, O.; Nieuwenhuijsen, M.J. A Study of the Combined Effects of Physical Activity and Air Pollution on Mortality in Elderly Urban Residents: The Danish Diet, Cancer, and Health Cohort. Environ. Health Perspect. 2015, 123, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, R.W.; Anderson, H.R.; Sunyer, J.; Ayres, J.; Baccini, M.; Vonk, J.M.; Boumghar, A.; Forastiere, F.; Forsberg, B.; Touloumi, G.; et al. Acute Effects of Particulate Air Pollution on Respiratory Admissions: Results from APHEA 2 Project. Am. J. Respir Crit. Care Med. 2001, 164, 1860–1866. [Google Scholar] [CrossRef]
- Schwartz, J. Air Pollution and Daily Mortality: A Review and Meta Analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef]
- Dominici, F.; Zeger, S.L.; Samet, J.M. A Measurement Error Model for Time-Series Studies of Air Pollution and Mortality. Biostatistics 2000, 1, 157–175. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef]
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 2012, 8, 166–175. [Google Scholar] [CrossRef]
- Jones, R.R.; Hogrefe, C.; Fitzgerald, E.F.; Hwang, S.A.; Özkaynak, H.; Garcia, V.C.; Lin, S. Respiratory hospitalizations in association with fine PM and its components in New York State. J. Air Waste Manag. Assoc. 2015, 65, 559–569. [Google Scholar] [CrossRef]
- Sarnat, J.A.; Schwartz, J.; Catalano, P.J.; Suh, H.H. Gaseous Pollutants in Particulate Matter Epidemiology: Confounders or Surrogates? Environ. Health Perspect. 2001, 109, 1053–1061. [Google Scholar] [CrossRef]
- Schlesinger, R.B.; Kunzli, N.; Hidy, G.M.; Gotschi, T.; Jerrett, M. The Health Relevance of Ambient Particulate Matter Characteristics: Coherence of Toxicological and Epidemiological Inferences. Inhal. Toxicol. 2006, 18, 95–125. [Google Scholar] [CrossRef]
- Schwarze, P.E.; Øvrevik, J.; Låg, M.; Refsnes, M.; Nafstad, P.; Hetland, R.B.; Dybing, E. Particulate Matter Properties and Health Effects: Consistency of Epidemiological and Toxicological Studies. Hum. Exp. Toxicol. 2006, 25, 559–579. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef]
- McCreanor, J.; Cullinan, P.; Nieuwenhuijsen, M.J.; Stewart-Evans, J.; Malliarou, E.; Jarup, L.; Harrington, R.; Svartengren, M.; Han, I.K.; Ohman-Strickland, P.; et al. Respiratory Effects of Exposure to Diesel Traffic in Persons with Asthma. N. Engl. J. Med. 2007, 357, 2348–2358. [Google Scholar] [CrossRef] [Green Version]
- Neidell, M.J. Air Pollution, Health, and Socio-Economic Status: The Effect of Outdoor Air Quality on Childhood Asthma. J. Health Econ. 2004, 23, 1209–1236. [Google Scholar] [CrossRef]
- Schwartz, J. Air Pollution and Hospital Admissions for Respiratory Disease. Epidemiology 1995, 7, 20–28. [Google Scholar] [CrossRef]
- Kim, H.; Kim, H.; Park, Y.H.; Lee, J.T. Assessment of Temporal Variation for the Risk of Particulate Matters on Asthma Hospitalization. Environ. Res. 2017, 156, 542–550. [Google Scholar] [CrossRef]
- Kim, O. Association between Long-Term Exposure to Particulate Matter Air Pollution and Mortality in a South Korean National Cohort: Comparison across Different Exposure Assessment Approaches. Int. J. Environ. Res. Public Health 2017, 14, 1103. [Google Scholar] [CrossRef]
- Li, P.; Xin, J.; Wang, Y.; Li, G.; Pan, X.; Wang, S.; Cheng, M.; Wen, T.; Wang, G.; Liu, Z. Association between Particulate Matter and Its Chemical Constituents of Urban Air Pollution and Daily Mortality or Morbidity in Beijing City. Environ. Sci. Pollut. Res. 2014, 22, 358–368. [Google Scholar] [CrossRef]
- Lin, H.; Liu, T.; Xiao, J.; Zeng, W.; Guo, L.; Li, X.; Xu, Y.; Zhang, Y.; Chang, J.J.; Vaughn, M.G.; et al. Hourly Peak PM 2.5 Concentration Associated with Increased Cardiovascular Mortality in Guangzhou, China. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 333–338. [Google Scholar] [CrossRef]
- Baccini, M.; Mattei, A.; Mealli, F.; Bertazzi, P.A.; Carugno, M. Assessing the Short Term Impact of Air Pollution on Mortality: A Matching Approach. Environ. Health 2017, 6, 7. [Google Scholar] [CrossRef]
- Di Novi, C. The Indirect Effect of Fine Particulate Matter on Health through Individuals’ Life-Style. J. Socio Econ. 2013, 44, 27–36. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. Assessing sensitivity to an unobserved binary covariate in an observational study with binary outcome. J. R. Stat. Soc. Ser. B 1983, 45, 212–218. [Google Scholar] [CrossRef]
- Wooldridge, J.M. Inverse Probability Weighted M-estimators for Sample Selection, Attrition, and Stratification. Port. Econ. J. 2002, 1, 117–139. [Google Scholar] [CrossRef]
- Wooldridge, J.M. Inverse probability weighted estimation for general missing data problems. J. Econ. 2007, 141, 1281–1301. [Google Scholar] [CrossRef] [Green Version]
- McCaffrey, D.F.; Ridgeway, G.; Morral, A.R. Propensity Score Estimation with Boosted Regression for Evaluating Causal Effects in Observational Studies. Psychol. Methods 2004, 9, 403. [Google Scholar] [CrossRef]
- Burgette, L.; Griffin, B.A.; McCaffrey, D. Propensity Scores for Multiple Treatments: A Tutorial for the Mnps Function in the Twang Package; R Package; Rand Corporation: Santa Monica, CA, USA, 2017. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Definition | ||
|---|---|---|---|
| Dependent variables | Number of walking days | Number of days when he or she walked at least 10 minutes in the past week (from 0 to 7 days, including for commuting) | |
| Mental stress | The level of stress in daily life. (I feel very much a lot:1, I feel a lot:2, I feel a little:3, I hardly feel it:4) | ||
| Independent variables | Exposure level of PM | Six group indicators (1-6) divided by percent quintiles based on number of hours when PM10 concentration is higher than 80 μg/m3 | |
| Matching variables | Physical factors | Age | Age based on resident identification number (19–110 years old) |
| Sex | Male:1, Female:2 | ||
| Height | The value of height in cm | ||
| Weight | The value of weight in kg | ||
| Ability to exercise | Exercise ability (1: I do not mind walking; 2: I have a little trouble walking; 3: I should be lying all day) | ||
| Habitual factors | Number of days of intense physical activity | The number of days when he or she had at least 10 minutes of intense physical activity in the past week (from 0 to 7 days, such as running, hiking and cycling) | |
| Number of days of eating breakfast | Number of days when he or she had a breakfast in the past week (from 0 to 7 days) | ||
| Average time of sleeping | Average time of sleeping per day (hour) | ||
| Drinking or not up to now | Experience of drinking while living so far (Yes: 1, No: 0) | ||
| Current drinking habit | Experience of drinking last one year (Yes: 1, No: 0) | ||
| Socio-economic factors | Basic living support | Receiving basic living income or not (Yes: 1, Not now, but past recipients:2, No:3) | |
| Living together with dementia patients | Whether household is currently living with a dementia patient or not (Yes:1, No:0) | ||
| Number of household members | Number of household members currently living together | ||
| Family income | Average monthly income of household including wages, real estate income, interest, government supports in recent years (ask on 8 point scale) | ||
| Economic activity | Whether he or she worked more than one hour with salary or worked for more than 18 hours as unpaid family workers in the past week (Yes:1, No:0) | ||
| Owned car or not | Whether driving a car (Yes:1, No:0) | ||
| Psychological factors | Perceived health condition | Think about her or his health (very good: 1, Good: 2, Usually: 3, Poor: 4, Very bad: 5) | |
| Characteristics | Number of Subjects | Exposure Level of High PM10 Concentration | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total | Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | Quintile 6 | |||
| (0–177) | (0–3) | (4–12) | (13–20) | (21–30) | (31–53) | (60–177) | |||
| Total | 93,694 | 100.0 (%) | 15.4 | 16.1 | 17.9 | 20.2 | 14.2 | 16.1 | |
| 14,451 | 15,073 | 16,783 | 18,918 | 13,350 | 15,119 | ||||
| Age | 19–25 | 8864 | 9.5 | 8.4 | 9.1 | 9.9 | 9.8 | 9.7 | 9.7 |
| 26–35 | 14,677 | 15.7 | 13.3 | 14.3 | 17.0 | 16.4 | 16.2 | 16.4 | |
| 36–45 | 19,200 | 20.5 | 19.8 | 19.8 | 20.4 | 20.6 | 20.8 | 21.6 | |
| 46–55 | 20,057 | 21.4 | 22.5 | 20.9 | 20.2 | 21.5 | 21.5 | 22.0 | |
| 56–65 | 15,968 | 17.0 | 17.9 | 18.1 | 17.4 | 16.2 | 17.4 | 15.6 | |
| 66–93 | 14,928 | 15.9 | 18.2 | 17.8 | 15.1 | 15.5 | 14.4 | 14.7 | |
| Sex | Male | 47,211 | 50.4 | 51.9 | 49.4 | 50.3 | 49.9 | 50.8 | 50.2 |
| Female | 46,483 | 49.6 | 48.1 | 50.6 | 49.7 | 50.1 | 49.2 | 49.8 | |
| Family Income | <500,000 won | 4055 | 4.3 | 5.6 | 4.7 | 3.6 | 3.9 | 4.8 | 3.7 |
| 500,000–1,000,000 | 8366 | 8.9 | 10.6 | 10.8 | 7.9 | 7.7 | 8.8 | 8.3 | |
| 1,000,000–2,000,000 | 13,988 | 14.9 | 16.9 | 16.7 | 14.5 | 13.8 | 14.4 | 13.7 | |
| 2,000,000–3,000,000 | 18,012 | 19.2 | 19.2 | 20.1 | 19.3 | 18.2 | 20.1 | 18.8 | |
| 3,000,000–4,000,000 | 17,676 | 18.9 | 18.0 | 17.8 | 20.4 | 18.1 | 18.7 | 20.2 | |
| 4,000,000–5,000,000 | 12,513 | 13.4 | 12.4 | 12.9 | 14.7 | 13.0 | 12.9 | 14.2 | |
| 5,000,000–6,000,000 | 7,707 | 8.2 | 6.9 | 7.8 | 8.0 | 8.8 | 8.3 | 9.4 | |
| >6,000,000 won | 11,377 | 12.1 | 10.4 | 9.2 | 11.7 | 16.6 | 12.0 | 11.8 | |
| Alcohol use (Drinking at least once in a year) | 79,292 | 84.6 | 84.3 | 84.0 | 85.2 | 85.2 | 84.4 | 84.4 | |
| Vigorous Exercise (<3 days/week ) | 78,977 | 84.3 | 84.8 | 84.5 | 83.0 | 84.3 | 84.0 | 85.3 | |
| Height | ≤150 cm | 4163 | 4.4 | 4.7 | 4.9 | 4.0 | 4.5 | 4.5 | 4.1 |
| ≤160 cm | 28,029 | 29.9 | 30.1 | 30.9 | 29.7 | 29.4 | 29.7 | 29.9 | |
| ≤170 cm | 36,058 | 38.5 | 38.8 | 38.4 | 38.2 | 38.5 | 38.6 | 38.4 | |
| ≤180 cm | 22,622 | 24.1 | 23.5 | 23.1 | 25.0 | 24.4 | 24.2 | 24.5 | |
| >180 cm | 2822 | 3.0 | 2.8 | 2.7 | 3.1 | 3.2 | 3.0 | 3.2 | |
| Weight | ≤50 kg | 11,371 | 12.1 | 11.8 | 12.5 | 12.2 | 12.5 | 11.7 | 12.0 |
| ≤60 kg | 30,707 | 32.8 | 32.5 | 33.4 | 32.7 | 33.0 | 32.6 | 32.3 | |
| ≤70 kg | 28,291 | 30.2 | 30.6 | 30.6 | 30.2 | 29.5 | 30.1 | 30.4 | |
| ≤80 kg | 16,184 | 17.3 | 17.5 | 16.4 | 17.3 | 17.2 | 17.8 | 17.5 | |
| >80 kg | 7141 | 7.6 | 7.6 | 7.2 | 7.5 | 7.8 | 7.7 | 7.9 | |
| Ability to exercise | I do not mind walking | 83,747 | 89.4 | 88.0 | 87.8 | 90.3 | 90.3 | 89.9 | 89.5 |
| I have a little trouble walking | 9650 | 10.3 | 11.7 | 11.8 | 9.4 | 9.4 | 9.7 | 10.1 | |
| I should be lying all day | 297 | 0.3 | 0.3 | 0.3 | 0.3 | 0.3 | 0.4 | 0.3 | |
| Number of days of eating breakfast | 0 | 12,745 | 13.6 | 11.6 | 12.6 | 13.5 | 14.2 | 15.2 | 14.5 |
| 1 | 1842 | 2.0 | 1.6 | 1.9 | 2.3 | 2.0 | 2.2 | 1.8 | |
| 2 | 4129 | 4.4 | 3.8 | 4.1 | 4.9 | 4.6 | 4.3 | 4.6 | |
| 3 | 5446 | 5.8 | 4.9 | 5.8 | 6.2 | 5.8 | 5.7 | 6.6 | |
| 4 | 3101 | 3.3 | 3.0 | 3.4 | 3.6 | 3.2 | 3.2 | 3.4 | |
| 5 | 4060 | 4.3 | 3.7 | 4.3 | 4.5 | 4.6 | 4.4 | 4.5 | |
| 6 | 1524 | 1.6 | 1.2 | 1.7 | 1.9 | 1.9 | 1.4 | 1.5 | |
| 7 | 60,847 | 64.9 | 70.2 | 66.3 | 63.2 | 63.7 | 63.7 | 63.2 | |
| Average time of sleeping | one hour to 5 hours | 15,610 | 16.7 | 16.0 | 16.7 | 16.8 | 16.8 | 16.9 | 16.7 |
| 6 hours to 10 hours | 77,932 | 83.2 | 83.8 | 83.2 | 83.0 | 83.0 | 83.0 | 83.1 | |
| 11 hours to 15 hours | 149 | 0.2 | 0.2 | 0.1 | 0.2 | 0.2 | 0.2 | 0.2 | |
| Basic living support (Yes, or Having in the past, but not now) | 3155 | 3.4 | 4.0 | 3.7 | 3.1 | 2.9 | 3.3 | 3.4 | |
| Living together with dementia patient | 749 | 0.8 | 0.8 | 0.8 | 0.8 | 0.9 | 0.6 | 0.8 | |
| Number of household members | One person | 9343 | 10.0 | 10.7 | 10.3 | 9.8 | 9.8 | 10.2 | 9.3 |
| Two persons | 27,073 | 28.9 | 32.6 | 30.8 | 28.1 | 27.6 | 27.8 | 26.9 | |
| 3–4 persons household | 47,570 | 50.8 | 47.0 | 49.4 | 51.7 | 52.0 | 51.0 | 53.1 | |
| >4 persons | 9708 | 10.4 | 9.7 | 9.5 | 10.5 | 10.7 | 11.1 | 10.7 | |
| Economic activity | 61,558 | 65.7 | 65.4 | 65.3 | 65.1 | 65.0 | 67.1 | 66.6 | |
| Having a car | 53,581 | 57.2 | 60.9 | 54.7 | 55.1 | 56.4 | 59.2 | 57.6 | |
| Perceived health condition | Very good | 6756 | 7.2 | 6.2 | 6.4 | 7.4 | 8.2 | 7.3 | 7.5 |
| Good | 32,491 | 34.7 | 34.1 | 34.6 | 35.8 | 35.5 | 33.8 | 33.8 | |
| Moderate | 40,569 | 43.3 | 43.0 | 43.1 | 43.2 | 42.5 | 44.5 | 43.8 | |
| Poor | 11,063 | 11.8 | 13.0 | 12.6 | 11.1 | 11.2 | 11.5 | 11.6 | |
| Very bad | 2815 | 3.0 | 3.7 | 3.3 | 2.5 | 2.6 | 2.8 | 3.2 | |
| Variable | Average Number of Walking Days Per Week | |
|---|---|---|
| Coefficient | Standard Deviation | |
| Group 2 | 0.5118 *** | 0.0314 |
| Group 3 | 0.6312 *** | 0.0302 |
| Group 4 | 0.5681 *** | 0.0295 |
| Group 5 | 0.34 *** | 0.0326 |
| Group 6 | 0.2623 *** | 0.0315 |
| Constants | 3.9192 *** | 0.0229 |
| Observations | 93,694 | |
| Variable | Perceived Mental Stress Level (Likert 4 Scale: 1, Strong to 4, Less Likely) | |
|---|---|---|
| Coefficient | Standard Deviation | |
| Group 2 | −0.0224 ** | 0.0086 |
| Group 3 | −0.022 ** | 0.0094 |
| Group 4 | −0.0425 *** | 0.0082 |
| Group 5 | 0.0023 | 0.0089 |
| Group 6 | −0.0344 *** | 0.0087 |
| Constants | 2.8812 | 0.0061 |
| Observations | 93,694 | |
| Threshold | Hours with > 80 μg/m3 | Hours with > 100 μg/m3 | ||
|---|---|---|---|---|
| Variable | (1) Perceived Mental Stress Level | (2) Number of Walking Days | (3) Perceived Mental Stress Level | (4) Number of Walking Days |
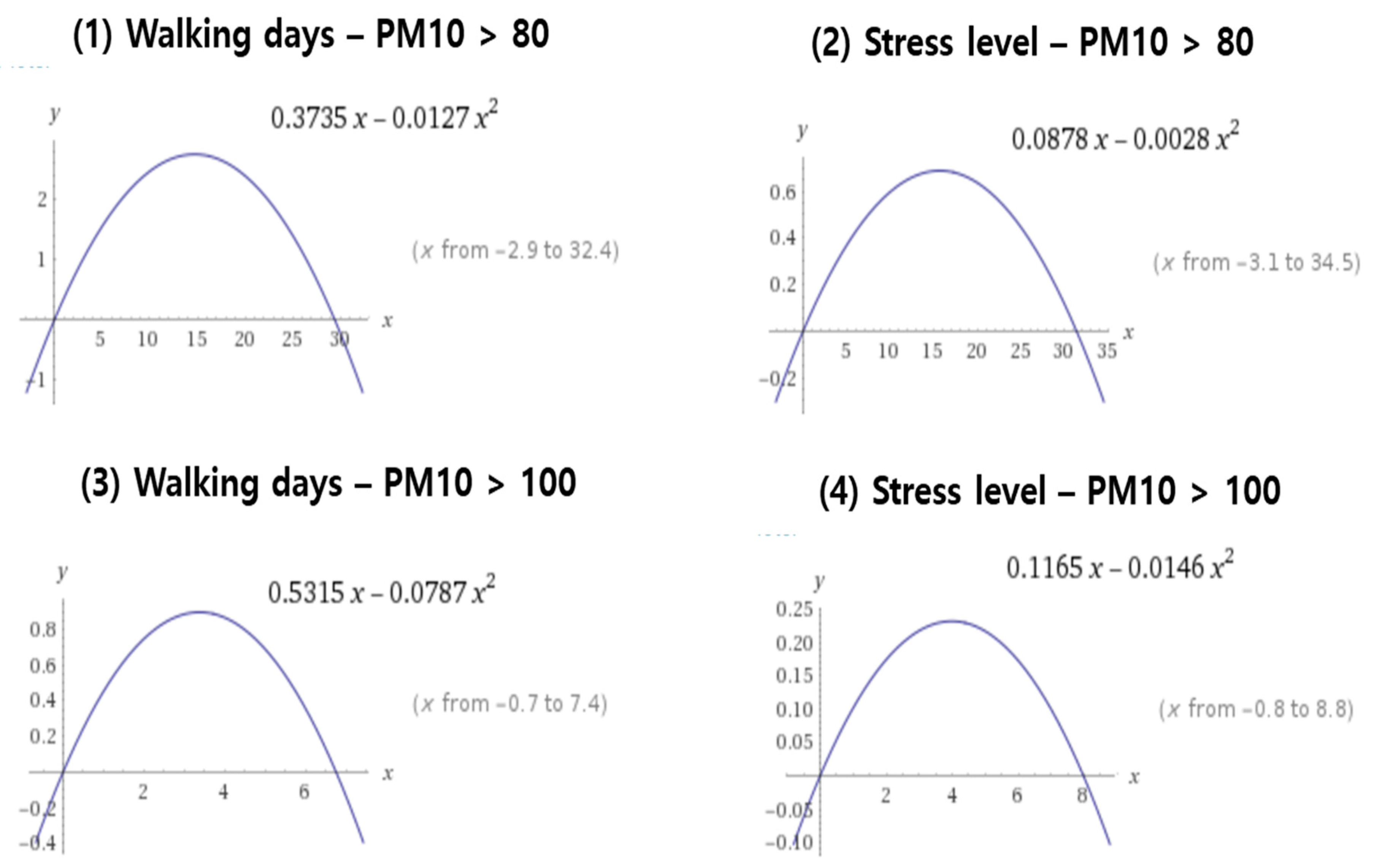
| high PM10 hours | 0.3735 *** | 0.0878 ** | 0.5315 *** | 0.1165 ** |
| (0.0420) | (0.0431) | (0.0563) | (0.0579) | |
| high PM10 hours^2 | −0.0127 *** | −0.0028 ** | −0.0787 *** | −0.0146 * |
| (0.0013) | (0.0014) | (0.0076) | (0.0078) | |
| Observations | 93,694 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, M.; Cho, D.; Shin, K. The Impact of Particulate Matter on Outdoor Activity and Mental Health: A Matching Approach. Int. J. Environ. Res. Public Health 2019, 16, 2983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162983
Jung M, Cho D, Shin K. The Impact of Particulate Matter on Outdoor Activity and Mental Health: A Matching Approach. International Journal of Environmental Research and Public Health. 2019; 16(16):2983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162983
Chicago/Turabian StyleJung, Miyeon, Daegon Cho, and Kwangsoo Shin. 2019. "The Impact of Particulate Matter on Outdoor Activity and Mental Health: A Matching Approach" International Journal of Environmental Research and Public Health 16, no. 16: 2983. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16162983