Equity-Specific Effects of Interventions to Promote Physical Activity among Middle-Aged and Older Adults: Development of a Collaborative Equity-Specific Re-Analysis Strategy

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Context
2.2. Establishment of the Collaboration
2.2.1. Search Strategy
2.2.2. Study Selection Criteria
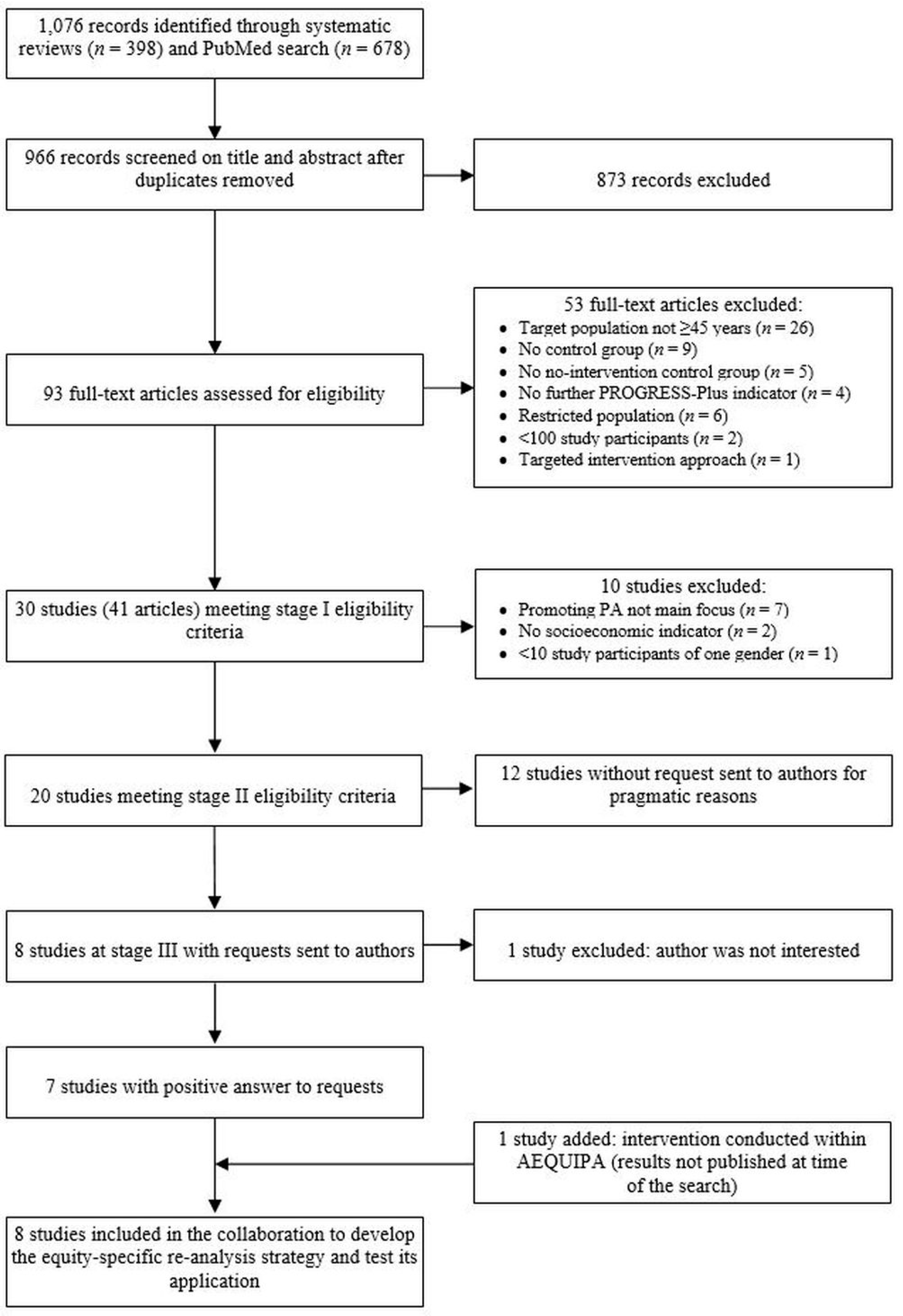
2.2.3. Search Results
2.3. Characteristics of the Collaboration and Development of the Joint Equity-Specific Re-Analysis Strategy
3. Results: The Joint Equity-Specific Re-Analysis Strategy
3.1. Definition of Exposure and Outcome Measures
3.2. Choice and Definition of Indicators of Social Inequalities
3.3. Statistical Analyses
3.3.1. Social Inequalities in Adherence and Dropout
3.3.2. Equity-Specific Intervention Effects
3.3.3. Secondary Analyses
3.4. Risk of Bias Assessment of Included Studies
3.5. Data Synthesis
3.6. Timeline
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Dalstra, J.A.A.; Kunst, A.E.; Borrell, C.; Breeze, E.; Cambois, E.; Costa, G.; Geurts, J.J.; Lahelma, E.; Van Oyen, H.; Rasmussen, N.K.; et al. Socioeconomic differences in the prevalence of common chronic diseases: An overview of eight European countries. Int. J. Epidemiol. 2005, 34, 316–326. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Physical Activity Promotion in Socially Disadvantaged Groups: Principles for Action; Phan Work Package 4 Final Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/185954/E96817eng.pdf (accessed on 11 July 2019).
- Gidlow, C.; Johnston, L.H.; Crone, D.; Ellis, N.; James, D. A systematic review of the relationship between socio-economic position and physical activity. Health Educ. J. 2006, 65, 338–367. [Google Scholar] [CrossRef]
- Hillsdon, M.; Lawlor, D.A.; Ebrahim, S.; Morris, J.N. Physical activity in older women: Associations with area deprivation and with socioeconomic position over the life course: Observations in the British Women’s Heart and Health Study. J. Epidemiol. Community Health 2008, 62, 344–350. [Google Scholar] [CrossRef] [PubMed]
- van Stralen, M.M.; De Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. Determinants of initiation and maintenance of physical activity among older adults: A literature review. Health Psychol. Rev. 2009, 3, 147–207. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef]
- Lear, S.A.; Hu, W.; Rangarajan, S.; Gasevic, D.; Leong, D.; Iqbal, R.; Casanova, A.; Swaminathan, S.; Anjana, R.M.; Kumar, R.; et al. The effect of physical activity on mortality and cardiovascular disease in 130,000 people from 17 high-income, middle-income, and low-income countries: The pure study. Lancet 2017, 390, 2643–2654. [Google Scholar] [CrossRef]
- Petrovic, D.; de Mestral, C.; Bochud, M.; Bartley, M.; Kivimäki, M.; Vineis, P.; Mackenbach, J.; Stringhini, S. The contribution of health behaviors to socioeconomic inequalities in health: A systematic review. Prev. Med. 2018, 113, 15–31. [Google Scholar] [CrossRef] [Green Version]
- Cleland, C.L.; Tully, M.A.; Kee, F.; Cupples, M.E. The effectiveness of physical activity interventions in socio-economically disadvantaged communities: A systematic review. Prev. Med. 2012, 54, 371–380. [Google Scholar] [CrossRef]
- Conn, V.S.; Coon Sells, T.G. Effectiveness of interventions to increase physical activity among minority populations: An umbrella review. J. Natl. Med. Assoc. 2016, 108, 54–68. [Google Scholar] [CrossRef]
- Kavanagh, J.; Oliver, S.; Lorenc, T.; Caird, J.; Tucker, H.; Harden, A.; Greaves, A.; Thomas, J.; Oakley, A. School-based cognitive-behavioural interventions: A systematic review of effects and inequalities. Health Sociol. Rev. 2009, 18, 61–78. [Google Scholar] [CrossRef]
- Frohlich, K.L.; Potvin, L. Transcending the known in public health practice: The inequality paradox: The population approach and vulnerable populations. Am. J. Public Health 2008, 98, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef] [PubMed]
- McLaren, L.; McIntyre, L.; Kirkpatrick, S. Rose’s population strategy of prevention need not increase social inequalities in health. Int. J. Epidemiol. 2010, 39, 372–377. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Adams, J.; Heywood, P. How and why do interventions that increase health overall widen inequalities within populations? In Social Inequality and Public Health; Babones, S.J., Ed.; The Policy Press: Bristol, UK, 2009; pp. 65–81. [Google Scholar]
- Backholer, K.; Beauchamp, A.; Ball, K.; Turrell, G.; Martin, J.; Woods, J.; Peeters, A. A framework for evaluating the impact of obesity prevention strategies on socioeconomic inequalities in weight. Am. J. Public Health 2014, 104, e43–e50. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.; Mytton, O.; White, M.; Monsivais, P. Why Are Some Population Interventions for Diet and Obesity More Equitable and Effective than Others? The Role of Individual Agency. PLoS Med. 2016, 13, e1001990. [Google Scholar] [CrossRef]
- Schüz, B.; Brick, C.; Wilding, S.; Conner, M. Socioeconomic status moderates the effects of health cognitions on health behaviors within participants: Two multibehavior studies. Ann. Behav. Med. 2019, kaz023. [Google Scholar] [CrossRef]
- Hilz, L.K.; Conner, M.; Schüz, B. Social inequality, health behaviour determinants and health behaviour: A Systematic Review. J. Psychol. Health 2019. [Google Scholar] [CrossRef] [Green Version]
- Bukman, A.J.; Teuscher, D.; Feskens, E.J.; van Baak, M.A.; Meershoek, A.; Renes, R.J. Perceptions on healthy eating, physical activity and lifestyle advice: Opportunities for adapting lifestyle interventions to individuals with low socioeconomic status. BMC Public Health 2014, 14, 1036. [Google Scholar] [CrossRef]
- Whitehead, M. A typology of actions to tackle social inequalities in health. J. Epidemiol. Community Health 2007, 61, 473–478. [Google Scholar] [CrossRef]
- Luten, K.A.; Dijkstra, A.; Reijneveld, S.A.; de Winter, A.F. Moderators of physical activity and healthy eating in an integrated community-based intervention for older adults. Eur. J. Public Health 2016, 26, 645–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Uffelen, J.G.Z.; Khan, A.; Burton, N.W. Gender differences in physical activity motivators and context preferences: A population-based study in people in their sixties. BMC Public Health 2017, 17, 624. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, D.K.; Ogilvie, D. Synthesising evidence for equity impacts of population-based physical activity interventions: A pilot study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 76. [Google Scholar] [CrossRef] [PubMed]
- Attwood, S.; van Sluijs, E.; Sutton, S. Exploring equity in primary-care-based physical activity interventions using progress-plus: A systematic review and evidence synthesis. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 60. [Google Scholar] [CrossRef] [PubMed]
- Lehne, G.; Bolte, G. Impact of universal interventions on social inequalities in physical activity among older adults: An equity-focused systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 20. [Google Scholar] [CrossRef] [PubMed]
- Petticrew, M.; Tugwell, P.; Kristjansson, E.; Oliver, S.; Ueffing, E.; Welch, V. Damned if you do, damned if you don’t: Subgroup analysis and equity. J. Epidemiol. Community Health 2012, 66, 95–98. [Google Scholar] [CrossRef]
- De Bourdeaudhuij, I.; Simon, C.; De Meester, F.; Van Lenthe, F.; Spittaels, H.; Lien, N.; Faggiano, F.; Mercken, L.; Moore, L.; Haerens, L. Are physical activity interventions equally effective in adolescents of low and high socio-economic status (SES): Results from the European Teenage project. Health Educ. Res. 2011, 26, 119–130. [Google Scholar] [CrossRef]
- Magnée, T.; Burdorf, A.; Brug, J.; Kremers, S.P.; Oenema, A.; van Assema, P.; Ezendam, N.P.; van Genugten, L.; Hendriksen, I.J.; Hopman-Rock, M.; et al. Equity-specific effects of 26 Dutch obesity-related lifestyle interventions. Am. J. Prev. Med. 2013, 44, e57–e66. [Google Scholar] [CrossRef]
- Lien, N.; Haerens, L.; Te Velde, S.J.; Mercken, L.; Klepp, K.I.; Moore, L.; de Bourdeaudhuij, I.; Faggiano, F.; van Lenthe, F.J. Exploring subgroup effects by socioeconomic position of three effective school-based dietary interventions: The European TEENAGE project. Int. J. Public Health 2014, 59, 493–502. [Google Scholar] [CrossRef]
- Tinner, L.; Caldwell, D.; Hickman, M.; MacArthur, G.J.; Gottfredson, D.; Lana Perez, A.; Moberg, D.P.; Wolfe, D.; Campbell, R. Examining subgroup effects by socioeconomic status of public health interventions targeting multiple risk behaviour in adolescence. BMC Public Health 2018, 18, 1180. [Google Scholar] [CrossRef]
- Love, R.; Adams, J.; van Sluijs, E.M.F. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef] [PubMed]
- TNS Opinion & Social. Special Eurobarometer 472: Sport and Physical Activity; Survey conducted by TNS Opinion & Social at the Request of the European Commission, Directorate-General for Education, Youth, Sport and Culture; Survey Co-Ordinated by the European Commission, Directorate-General for Communication (DG COMM “Media Monitoring, Media Analysis and Eurobarometer” Unit); TNS Opinion & Social: Brussels, Belgium, 2018. [Google Scholar]
- King, A.C.; King, D.K. Physical activity for an aging population. Public Health Rev. 2010, 32, 401–426. [Google Scholar] [CrossRef]
- Forberger, S.; Bammann, K.; Bauer, J.; Boll, S.; Bolte, G.; Brand, T.; Hein, A.; Koppelin, F.; Lippke, S.; Meyer, J.; et al. How to tackle key challenges in the promotion of physical activity among older adults (65+): The aequipa network approach. Int. J. Environ. Res. Public Health 2017, 14, 379. [Google Scholar] [CrossRef] [PubMed]
- Muellmann, S.; Bragina, I.; Voelcker-Rehage, C.; Rost, E.; Lippke, S.; Meyer, J.; Schnauber, J.; Wasmann, M.; Toborg, M.; Koppelin, F.; et al. Development and evaluation of two web-based interventions for the promotion of physical activity in older adults: Study protocol for a community-based controlled intervention trial. BMC Public Health 2017, 17, 512. [Google Scholar] [CrossRef] [PubMed]
- Muellmann, S.; Buck, C.; Voelcker-Rehage, C.; Bragina, I.; Lippke, S.; Meyer, J.; Peters, M.; Pischke, C.R. Effects of two web-based interventions promoting physical activity among older adults compared to a delayed intervention control group in Northwestern Germany: Results of the PROMOTE community-based intervention trial. Prev. Med. Rep. 2019, 100958. [Google Scholar] [CrossRef] [PubMed]
- Oude Hengel, K.M.; Coenen, P.; Robtoek, S.J.W.; Boot, C.R.L.; van der Beek, A.J.; Van Lenthe, F.J.; Burdorf, A. Socioeconomic inequalities in reach, compliance and effectiveness of lifestyle interventions among workers: Protocol for an individual participant data metaanalysis and equity-specific reanalysis. BMJ Open 2019, 9, e025463. [Google Scholar] [CrossRef]
- Lee, W.C.; Ory, M.G. The engagement in physical activity for middle-aged and older adults with multiple chronic conditions: Findings from a community health assessment. J. Aging Res. 2013, 2013, 152868. [Google Scholar] [CrossRef]
- Caban-Martinez, A.J.; Courtney, T.K.; Chang, W.R.; Lombardi, D.A.; Huang, Y.H.; Brennan, M.J.; Perry, M.J.; Katz, J.N.; Christiani, D.C.; Verma, S.K. Leisure-time physical activity, falls, and fall injuries in middle-aged adults. Am. J. Prev. Med. 2015, 49, 888–901. [Google Scholar] [CrossRef]
- Baxter, S.; Johnson, M.; Payne, N.; Buckley-Woods, H.; Blank, L.; Hock, E.; Daley, A.; Taylor, A.; Pavey, T.; Mountain, G.; et al. Promoting and maintaining physical activity in the transition to retirement: A systematic review of interventions for adults around retirement age. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 12. [Google Scholar] [CrossRef]
- Müller, A.M.; Khoo, S. Non-face-to-face physical activity interventions in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 35. [Google Scholar] [CrossRef]
- Chase, J.A. Interventions to Increase Physical Activity among Older Adults: A Meta-Analysis. Gerontologist 2015, 55, 706–718. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using progress ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Evans, T.; Brown, H. Road traffic crashes: Operationalizing equity in the context of health sector reform. Inj. Control Saf. Promot. 2003, 10, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S.; Kavanagh, J.; Caird, J.; Lorenc, T.; Oliver, K.; Harden, A.; Thomas, J.; Greaves, A.; Oakley, A. Health Promotion, Inequalities and Young People’s Health: A Systematic Review of Research; EPPI-Centre, Social Science Research Unit, Institute of Education, University of London: London, UK, 2008. [Google Scholar]
- Estabrooks, P.A.; Lee, R.E.; Gyurcsik, N.C. Resources for physical activity participation: Does availability and accessibility differ by neighborhood socioeconomic status? Ann. Behav. Med. 2003, 25, 100–104. [Google Scholar] [CrossRef] [PubMed]
- van Stralen, M.M.; de Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. Efficacy of two tailored interventions promoting physical activity in older adults. Am. J. Prev. Med. 2009, 37, 405–417. [Google Scholar] [CrossRef] [PubMed]
- van Stralen, M.M.; de Vries, H.; Bolman, C.; Mudde, A.N.; Lechner, L. Exploring the Efficacy and Moderators of Two Computer-Tailored Physical Activity Interventions for Older Adults: A Randomized Controlled Trial. Ann. Behav. Med. 2010, 39, 139–150. [Google Scholar] [CrossRef] [Green Version]
- van Stralen, M.M.; de Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. The working mechanisms of an environmentally tailored physical activity intervention for older adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 83. [Google Scholar] [CrossRef]
- van Stralen, M.M.; de Vries, H.; Mudde, A.N.; Bolman, C.; Lechner, L. The long-term efficacy of two computer-tailored physical activity interventions for older adults: Main effects and mediators. Health Psychol. 2011, 30, 442–452. [Google Scholar] [CrossRef]
- Peels, D.A.; van Stralen, M.M.; Bolman, C.; Golsteijn, R.H.; de Vries, H.; Mudde, A.N.; Lechner, L. The differentiated effectiveness of a printed versus a Web-based tailored physical activity intervention among adults aged over 50. Health Educ. Res. 2014, 29, 870–882. [Google Scholar] [CrossRef] [Green Version]
- Peels, D.A.; Hoogenveen, R.R.; Feenstra, T.L.; Golsteijn, R.H.; Bolman, C.; Mudde, A.N.; Wendel-Vos, G.C.W.; De Vries, H.; Lechner, L. Long-term health outcomes and cost-effectiveness of a computer-tailored physical activity intervention among people aged over fifty: Modelling the results of a randomized controlled trial. BMC Public Health 2014, 14, 1099. [Google Scholar] [CrossRef]
- Peels, D.A.; Bolman, C.; Golsteijn, R.H.; de Vries, H.; Mudde, A.N.; van Stralen, M.M.; Lechner, L. Long-term efficacy of a printed or a Web-based tailored physical activity intervention among older adults. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 104. [Google Scholar] [CrossRef] [PubMed]
- Pelssers, J.; Delecluse, C.; Opdenacker, J.; Kennis, E.; Van Roie, E.; Boen, F. “Every Step Counts!”: Effects of a Structured Walking Intervention in a Community-Based Senior Organization. J. Aging Phys. Act. 2013, 21, 167–185. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.; Lemmink, K.A.; Stevens, M.; de Greef, M.H.; Rispens, P.; King, A.C.; Mulder, T. Six-month effects of the Groningen active living model (GALM) on physical activity, health and fitness outcomes in sedentary and underactive older adults aged 55–65. Patient Educ. Couns. 2006, 62, 132–141. [Google Scholar] [CrossRef] [PubMed]
- de Jong, J.; Lemmink, K.A.; King, A.C.; Huisman, M.; Stevens, M. Twelve-month effects of the Groningen active living model (GALM) on physical activity, health and fitness outcomes in sedentary and underactive older adults aged 55–65. Patient Educ. Couns. 2007, 66, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.; Kerry, S.M.; Victor, C.R.; Ekelund, U.; Woodcock, A.; Iliffe, S.; Whincup, P.H.; Beighton, C.; Ussher, M.; Limb, E.S.; et al. A primary care nurse-delivered walking intervention in older adults: PACE (pedometer accelerometer consultation evaluation)-Lift cluster randomised controlled trial. PLoS Med. 2015, 12, e1001783. [Google Scholar] [CrossRef]
- Harris, T.; Kerry, S.M.; Limb, E.S.; Victor, C.R.; Iliffe, S.; Ussher, M.; Whincup, P.H.; Ekelund, U.; Fox-Rushby, J.; Furness, C.; et al. Effect of a Primary Care Walking Intervention with and without Nurse Support on Physical Activity Levels in 45- to 75-Year-Olds: The Pedometer and Consultation Evaluation (PACE-UP) Cluster Randomised Clinical Trial. PLoS Med. 2017, 14, e1002210. [Google Scholar] [CrossRef] [PubMed]
- Iliffe, S.; Kendrick, D.; Morris, R.; Griffin, M.; Haworth, D.; Carpenter, H.; Masud, T.; Skelton, D.A.; Dinan-Young, S.; Bowling, A.; et al. Promoting physical activity in older people in general practice: ProAct65+ cluster randomised controlled trial. Br. J. Gen. Pract. 2015, 65, e731–738. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Deeks, J.J.; Altman, D.G.; on behalf of the Cochrane Statistical Methods Group. Chapter 16: Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration; 2011; Available online: www.handbook.cochrane.org (accessed on 23 August 2019).
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the american college of sports medicine and the american heart association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the computer science and applications, inc. Accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Hill, S.; Amos, A.; Clifford, D.; Platt, S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: Review of the evidence. Tob. Control. 2014, 23, e89–e97. [Google Scholar] [CrossRef]
- Beauchamp, A.; Backholer, K.; Magliano, D.; Peeters, A. The effect of obesity prevention interventions according to socioeconomic position: A systematic review. Obes. Rev. 2014, 5, 541–554. [Google Scholar] [CrossRef] [PubMed]
- McGill, R.; Anwar, E.; Orton, L.; Bromley, H.; Lloyd-Williams, F.; O’Flaherty, M.; Taylor-Robinson, D.; Guzman-Castillo, M.; Gillespie, D.; Moreira, P.; et al. Are interventions to promote healthy eating equally effective for all? Systematic review of socioeconomic inequalities in impact. BMC Public Health 2015, 15, 457. [Google Scholar] [CrossRef]
- UNESCO Institute for Statistics. International Standard Classification of Education: ISCED 2011; UNESCO Institute for Statistics: Montreal, QC, Canada, 2012. Available online: http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf (accessed on 19 June 2019).
- Krieger, N. Genders, sexes, and health: What are the connections—And why does it matter? Int. J. Epidemiol. 2003, 32, 652–657. [Google Scholar] [CrossRef]
- Hammarström, A.; Johansson, K.; Annandale, E.; Ahlgren, C.; Aléx, L.; Christianson, M.; Elwér, S.; Eriksson, C.; Fjellman-Wiklund, A.; Gilenstam, K.; et al. Central gender theoretical concepts in health research: The state of the art. J. Epidemiol. Community Health 2014, 68, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Kerry, S.M.; Morgan, K.E.; Limb, E.; Cook, D.G.; Furness, C.; Carey, I.; DeWilde, S.; Victor, C.R.; Iliffe, S.; Whincup, P.; et al. Interpreting population reach of a large, successful physical activity trial delivered through primary care. BMC Public Health 2018, 18, 170. [Google Scholar] [CrossRef] [PubMed]
- Bayley, A.; Stahl, D.; Ashworth, M.; Cook, D.G.; Whincup, P.H.; Treasure, J.; Greenough, A.; Ridge, K.; Winkley, K.; Ismail, K. Response bias to a randomised controlled trial of a lifestyle intervention in people at high risk of cardiovascular disease: A cross-sectional analysis. BMC Public Health 2018, 18, 1092. [Google Scholar] [CrossRef] [PubMed]
- Lehne, G.; Voelcker-Rehage, C.; Meyer, J.; Bammann, K.; Gansefort, D.; Bruchert, T.; Bolte, G. Equity Impact Assessment of Interventions to Promote Physical Activity among Older Adults: A Logic Model Framework. Int. J. Environ. Res. Public Health 2019, 16, 420. [Google Scholar] [CrossRef]
- Harper, S.; King, N.B.; Young, M.E. Impact of selective evidence presentation on judgments of health inequality trends: An experimental study. PLoS ONE 2013, 8, e63362. [Google Scholar] [CrossRef]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Chideya, S.; Marchi, K.S.; Metzler, M.; Posner, S. Socioeconomic Status in Health Research. One Size Does Not Fit All. JAMA 2005, 294, 2879–2888. [Google Scholar] [CrossRef]
- Galobardes, B.; Shaw, B.A.; Lawlor, D.A.; Lynch, J.W.; Smith, G.D. Indicators of socioeconomic position (part1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Smith, G.D. Indicators of socioeconomic position (part 2). J. Epidemiol. Community Health 2006, 60, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzoli, L.; Villari, P.; Pirone, G.M.; Boccia, A. Marital status and mortality in the elderly: A systematic review and meta-analysis. Soc. Sci. Med. 2007, 64, 77–94. [Google Scholar] [CrossRef] [PubMed]
- Pettee, K.K.; Brach, J.S.; Kriska, A.M.; Boudreau, R.; Richardson, C.R.; Colbert, L.H.; Satterfield, S.; Visser, M.; Harris, T.B.; Ayonayon, H.N.; et al. Influence of marital status on physical activity levels among older adults. Med. Sci. Sports Exerc. 2006, 38, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 9: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (Updated March 2011); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration; 2011; Available online: www.handbook.cochrane.org (accessed on 23 August 2019).
- Ogilvie, D.; Fayter, D.; Petticrew, M.; Sowden, A.; Thomas, S.; Whitehead, M.; Worthy, G. The harvest plot: A method for synthesising evidence about the differential effects of interventions. BMC Med. Res. Methodol. 2008, 8, 8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Intervention Study | Location | Study Design, n * | Intervention | PA Outcome | Social Indicators |
|---|---|---|---|---|---|
| Active Plus (first version) [49,50,51,52] | The Netherlands | Cluster RCT, IG1 (2 MHC) n = 652, IG2 (2 MHC) n = 733, CG (2 MHC) n = 586 Follow-up = 2 and 8 months after end of intervention | IG1: Three tailored letters; personalized PA advice targeting psychosocial determinants during 4 months IG2: Intervention of IG1 plus tailored environmental information CG: Wait-listed | Self-report: Dutch SQUASH (weekly minutes of total PA, transport walking and cycling, leisure walking, gardening doing odd jobs and cycling, sports) | Gender, education, age, marital status |
| Active Plus (revised version) [53,54,55] | The Netherlands | Cluster RCT, IG1 (1 MHC) n = 439, IG2 (2 MHC) n = 423, IG3 (1 MHC) n = 435, IG4 (1 MHC) n = 432, CG (1 MHC) n = 411 Follow-up = 2 and 8 months after end of intervention | IG1: Three tailored letters; personalized PA advice targeting psychosocial determinants during 4 months IG2: Web-based version of intervention of IG1 IG3: Intervention of IG1 plus tailored environmental information IG4: Web-based version of intervention of IG3 CG: Wait-listed | Self-report: Dutch SQUASH (weekly days and minutes of total PA, transport walking and cycling, leisure walking, gardening doing odd jobs and cycling, sports) | Occupation, gender, education, income, age, marital status |
| Every step counts! [56] | Belgium | Controlled before and after study, IG (32 meeting points) n = 469, CG (12 meeting points) n = 154 Follow-up = end of intervention | IG: 10-week pedometer-defined walks in weekly walking schedules (fitness tailored and structured in walking load) CG: Wait-listed | Self-report: adapted version of GLTEQ (scores for low-, moderate-, and vigorous-intensity PA, total PA score) | Gender, education, social capital **, age, marital status |
| GALM [57,58] | The Netherlands | Cluster-randomized trial, IG (6 neighborhoods) n = 163, CG (6 neighborhoods) n = 152 Follow-up = end of intervention | IG: Weekly sessions emphasizing tailored moderate-intensity recreational sports activities over 15 weeks CG: Wait-listed | Self-report: Voorrips PA questionnaire, compendium of physical activities by Ainsworth et al. (energy expenditure for recreational sports activities, gardening, doing odd jobs, transport walking and cycling) | Gender, education, age, marital status, living situation |
| PACE-Lift [59] | UK | Cluster RCT, IG (118 households) n = 150, CG (117 households) n = 148 Follow-up = end of intervention, 9 and 45 months after end of intervention | IG: Four tailored primary care nurse-delivered PA consultations over 3 months, pedometer and accelerometer feedback, individual PA diary and plan CG: Usual care | Objective: Accelerometer (average daily step-count, weekly minutes of MVPA) Self-report: GPPAQ (being inactive, moderately inactive, moderately active), short IPAQ (time in MVPA weekly, time spend walking weekly) | Area-level deprivation, race/ethnicity, occupation, gender, education, social capital **, age, marital status, living situation |
| PACE-UP [60] | UK | Cluster RCT, IG1 (307 households) n = 339, IG2 (310 households) n = 346, CG (305 households) n = 338 Follow-up = end of intervention, 9 and 33 months after end of intervention | IG1: Pedometers, patient handbook, PA diary including individual walking plan over 3 months IG2: Intervention of IG1 plus 3 tailored practice nurse PA consultations CG: Usual care | Objective: Accelerometer (average daily step-count, weekly minutes of MVPA) Self-report: GPPAQ (being inactive, moderately inactive, moderately active), short IPAQ (time in MVPA weekly, time spend walking weekly) | Area-level deprivation, race/ethnicity, occupation, gender, education, social capital **, age, marital status, living situation |
| ProAct65+ [61] | UK | Cluster RCT, IG1 (14 practices) n = 410, IG2 (14 practices) n = 387, CG (14 practices) n = 457 Follow-up = end of intervention, 6, 12, 18 and 24 months after end of intervention | IG1: Home-based exercise program over 6 months comprising exercises, walking plan, visits of trained peer mentors IG2: Community-based exercise program over 6 months comprising instructor-delivered group exercise class, home exercise, advice to walk CG: Usual care | Self-report: CHAMPS, Phone-FITT, PASE (weekly minutes and days of MVPA) | Area-level deprivation, race/ethnicity, occupation, gender, education, income, age, marital status, living situation |
| PROMOTE [37,38] | Germany | RCT, IG1 n = 211, IG2 n = 198, CG n = 180 Follow-up = end of intervention | IG1: Tailored exercise plan; website with PA diary, online-forum, social features; weekly group meetings over 10 weeks IG2: Intervention of IG1 plus PA tracker CG: Wait-listed | Objective: Accelerometer (e.g., average daily step-count, weekly minutes of MVPA) Self-report: IPAQ | Race/ethnicity, occupation, gender, education, income, social capital **, age, marital status, living situation |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czwikla, G.; Boen, F.; Cook, D.G.; de Jong, J.; Harris, T.; Hilz, L.K.; Iliffe, S.; Morris, R.; Muellmann, S.; Peels, D.A.; et al. Equity-Specific Effects of Interventions to Promote Physical Activity among Middle-Aged and Older Adults: Development of a Collaborative Equity-Specific Re-Analysis Strategy. Int. J. Environ. Res. Public Health 2019, 16, 3195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173195
Czwikla G, Boen F, Cook DG, de Jong J, Harris T, Hilz LK, Iliffe S, Morris R, Muellmann S, Peels DA, et al. Equity-Specific Effects of Interventions to Promote Physical Activity among Middle-Aged and Older Adults: Development of a Collaborative Equity-Specific Re-Analysis Strategy. International Journal of Environmental Research and Public Health. 2019; 16(17):3195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173195
Chicago/Turabian StyleCzwikla, Gesa, Filip Boen, Derek G. Cook, Johan de Jong, Tess Harris, Lisa K. Hilz, Steve Iliffe, Richard Morris, Saskia Muellmann, Denise A. Peels, and et al. 2019. "Equity-Specific Effects of Interventions to Promote Physical Activity among Middle-Aged and Older Adults: Development of a Collaborative Equity-Specific Re-Analysis Strategy" International Journal of Environmental Research and Public Health 16, no. 17: 3195. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173195