Smoke-Free Policies and Smoking Cessation in the United States, 2003–2015

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Analytic Sample
2.3. Smoking Cessation
2.4. Smoke-Free Laws and Self-Reported Workplace Smoke-Free Policies
2.5. Key Sociodemographic Variables
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Association Between Smoke-Free Measures and Cessation
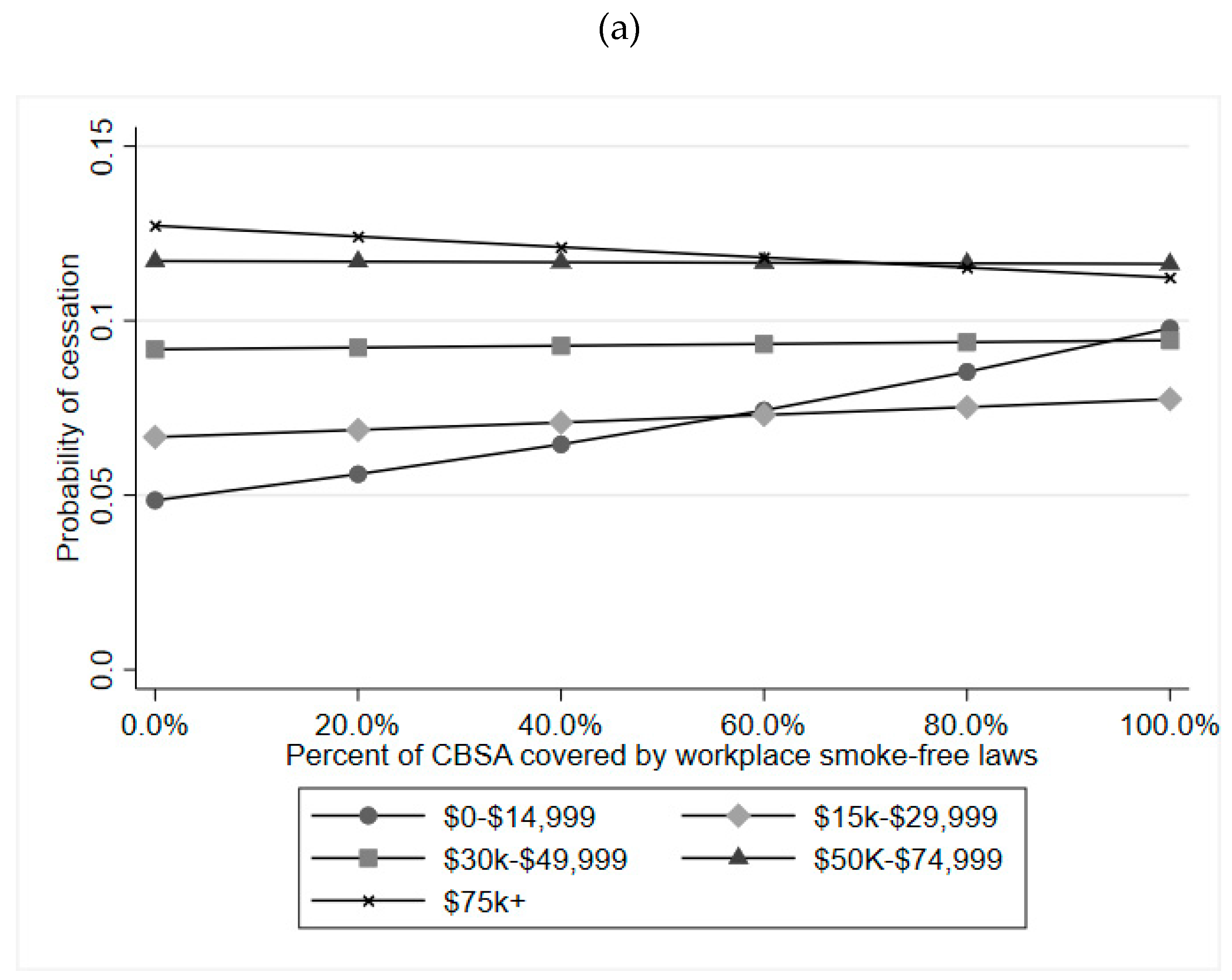
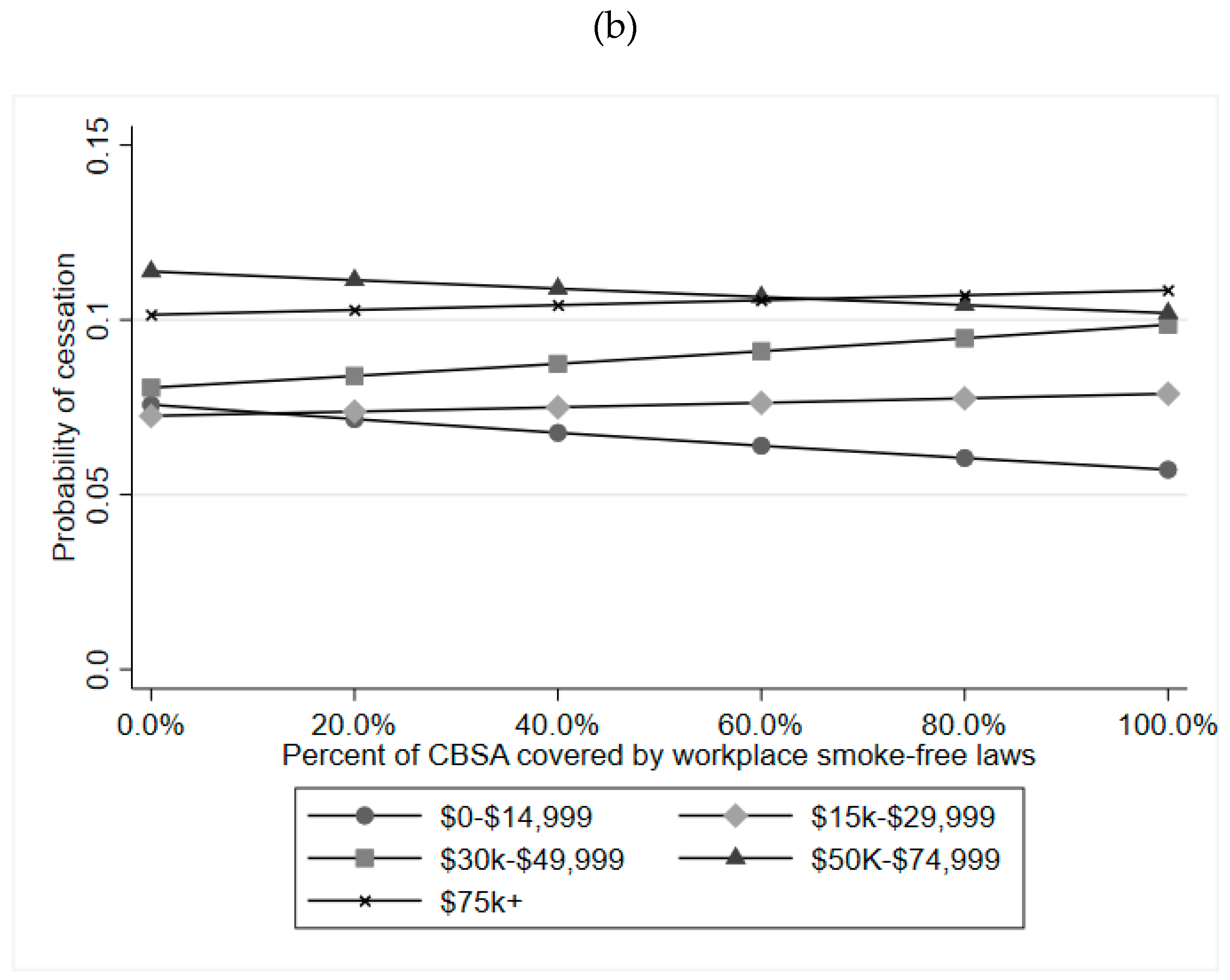
3.3. Effect Modification by Sociodemographic Factors
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smoking and Tobacco Use: Data and Statistics. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/tobacco/data_statistics/index.htm (accessed on 8 July 2019).
- Frazer, K.; Callinan, J.E.; McHugh, J.; van Baarsel, S.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2016. [Google Scholar]
- Fichtenberg, C.M.; Glantz, S.A. Effect of smoke-free workplaces on smoking behaviour: Systematic review. BMJ 2002, 325, 188. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.J.; Tan, C. Overview of systematic reviews on the health-related effects of government tobacco control policies. BMC Public Health 2015, 15, 744. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, D.P.; Razi, S.; Leeks, K.D.; Priya Kalra, G.; Chattopadhyay, S.K.; Soler, R.E. Task Force on Community Preventive Services Smokefree policies to reduce tobacco use. A systematic review. Am. J. Prev. Med. 2010, 38, S275–S289. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Afshin, A.; Benowitz, N.L.; Bittner, V.; Daniels, S.R.; Franch, H.A.; Jacobs, D.R.; Kraus, W.E.; Kris-Etherton, P.M.; Krummel, D.A.; et al. AHA Scientific Statement Population Approaches to Improve Diet, Physical Activity, and Smoking Habits A Scientific Statement From the American Heart Association. Circulation 2012, 126, 1514–1563. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Gonzalez, M.; Ling, P.M.; Glantz, S.A. Relationship of Smokefree Laws and Alcohol Use with Light and Intermittent Smoking and Quit Attempts among US Adults and Alcohol Users. PLoS ONE 2015, 10, e0137023. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.L.; Auchincloss, A.H.; Tabb, L.P.; Stehr, M.; Shikany, J.M.; Schreiner, P.J.; Widome, R.; Gordon-Larsen, P. Associations of Bar and Restaurant Smoking Bans With Smoking Behavior in the CARDIA Study: A 25-Year Study. Am. J. Epidemiol. 2018, 187, 1250–1258. [Google Scholar] [CrossRef] [PubMed]
- Shavers, V.L.; Fagan, P.; Alexander, L.A.J.; Clayton, R.; Doucet, J.; Baezconde-Garbanati, L. Workplace and home smoking restrictions and racial/ethnic variation in the prevalence and intensity of current cigarette smoking among women by poverty status, TUS-CPS 1998–1999 and 2001–2002. J. Epidemiol. Community Health 2006, 60, ii34–ii43. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R.; Mostashari, F.; Kerker, B.D.; Miller, N.; Hajat, A.; Frankel, M. Adult tobacco use levels after intensive tobacco control measures: New York City, 2002–2003. Am. J. Public Health 2005, 95, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.; Amos, A.; Clifford, D.; Platt, S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: Review of the evidence. Tob. Control 2014, 23, e89–e97. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Fayter, D.; Misso, K.; Ogilvie, D.; Petticrew, M.; Sowden, A.; Whitehead, M.; Worthy, G. Population tobacco control interventions and their effects on social inequalities in smoking: Systematic review. Tob. Control 2008, 17, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Platt, S.; Amos, A. Equity impact of population-level interventions and policies to reduce smoking in adults: A systematic review. Drug Alcohol Depend. 2014, 138, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Tobacco Use Supplement-Current Population Survey. Healthy People 2020. Available online: https://www.healthypeople.gov/2020/data-source/tobacco-use-supplement-current-population-survey (accessed on 18 June 2018).
- Flood, S.; King, M.; Ruggles, S.; Warren, J.R. Integrated Public Use Microdata Series, Current Population Survey: Version 5.0. Available online: https://ipums.org/projects/ipums-cps/d030.v5.0 (accessed on 26 July 2019).
- US Census Bureau Imputation of Unreported Data Items. Available online: https://www.census.gov/programs-surveys/cps/technical-documentation/methodology/imputation-of-unreported-data-items.html (accessed on 18 June 2019).
- IVEware: Imputation and Variance Estimation Software, Version 0.3. Available online: https://www.src.isr.umich.edu/software/ (accessed on 29 August 2018).
- US Census Bureau Geography 2010 Geographic Terms and Concepts—Core Based Statistical Areas and Related Statistical Areas. Available online: https://www.census.gov/geo/reference/gtc/gtc_cbsa.html (accessed on 5 June 2018).
- Tobacco Control Laws Database: A Tool for Researchers. Available online: https://no-smoke.org/tobacco-control-laws-database-tool-researchers/ (accessed on 18 June 2019).
- Gonzalez, M.; Sanders-Jackson, A.; Song, A.V.; Cheng, K.; Glantz, S.A. Strong Smoke-Free Law Coverage in the United States by Race/Ethnicity: 2000–2009. Am. J. Public Health 2013, 103, e62–e66. [Google Scholar] [CrossRef] [PubMed]
- US Census Bureau Population and Housing Unit Estimates. Available online: https://www.census.gov/popest (accessed on 18 June 2019).
- The Tax Burden on Tobacco Volume 51, 1970–2016. HealthData.gov. Available online: https://www.healthdata.gov/dataset/tax-burden-tobacco-volume-51-1970-2016-0 (accessed on 28 February 2018).
- Broken Promises to Our Children: A State-by-State Look at the 1998 Tobacco Settlement 19 Years Later. Campaign for Tobacco-Free Kids. 13 December 2017. Available online: https://www.tobaccofreekids.org/assets/content/what_we_do/state_local_issues/settlement/FY2018/FY2018_state_settlement_report.pdf (accessed on 28 February 2018).
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Series B. Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Callinan, J.E.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2010, 4, CD005992. [Google Scholar]
- Office on Smoking and Health (US). The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Publications and Reports of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2006.
- Syamlal, G.; King, B.A.; Mazurek, J.M. Workplace Smoke-Free Policies and Cessation Programs Among U.S. Working Adults. Am. J. Prev. Med. 2019, 56, 548–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moskowitz, J.M.; Lin, Z.; Hudes, E.S. The impact of workplace smoking ordinances in California on smoking cessation. Am. J. Public Health 2000, 90, 757–761. [Google Scholar] [PubMed] [Green Version]
- Dinno, A.; Glantz, S. Tobacco control policies are egalitarian: A vulnerabilities perspective on clean indoor air laws, cigarette prices, and tobacco use disparities. Soc. Sci. Med. 2009, 68, 1439–1447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smokefree Policies Result in High Levels of Compliance. CDC. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/secondhand_smoke/protection/compliance/index.htm (accessed on 8 August 2019).
- Lindquist, M.A.; Mejia, A. Zen and the art of multiple comparisons. Psychosom. Med. 2015, 77, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Pramesh, C.S.; Buyse, M. Common pitfalls in statistical analysis: The perils of multiple testing. Perspect. Clin. Res. 2016, 7, 106–107. [Google Scholar] [CrossRef] [PubMed]
- Pesko, M.F.; Bains, J.; Maclean, C.; Cook, B.L. Nearly Half Of Small Employers Using Tobacco Surcharges Do Not Provide Tobacco Cessation Wellness Programs. Health Aff. 2018, 37, 473–481. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | 2003 | 2006–2007 | 2010–2011 | 2014–2015 | |
|---|---|---|---|---|---|
| Total N | 102,834 | 28,026 | 28,807 | 25,302 | 20,699 |
| Age Categories | |||||
| % 25–39 | 39.4% | 40.4% | 39.4% | 38.8% | 39.0% |
| % 40–54 | 41.0% | 43.4% | 42.5% | 40.6% | 36.6% |
| % 55–65 | 19.6% | 16.1% | 18.0% | 20.5% | 24.4% |
| Age (mean and s.d.) | 43.4 (7.3) | 42.6 (7.4) | 43.1 (7.2) | 43.6 (7.3) | 44.3 (7.3) |
| % Male | 54.2% | 54.4% | 54.2% | 54.2% | 54.2% |
| Race/Ethnicity | |||||
| % Non-Hispanic White | 73.6% | 74.5% | 75.0% | 73.4% | 70.8% |
| % Non-Hispanic Black | 11.5% | 11.2% | 10.7% | 11.7% | 12.4% |
| % Hispanic | 9.7% | 9.3% | 9.4% | 9.6% | 10.8% |
| % Other Non-Hispanic | 5.2% | 5.1% | 4.8% | 5.2% | 6.0% |
| Education | |||||
| % Less than High School | 15.9% | 16.2% | 16.4% | 15.2% | 15.6% |
| % HS Graduate | 38.5% | 39.0% | 38.8% | 38.9% | 37.3% |
| % Some College | 31.0% | 29.7% | 30.0% | 31.7% | 32.9% |
| % College+ | 14.6% | 15.1% | 14.8% | 14.2% | 14.2% |
| Income | |||||
| % $0–14,999 | 19.4% | 20.0% | 17.2% | 19.9% | 20.9% |
| % $15,000–29,999 | 20.2% | 20.8% | 19.3% | 21.3% | 19.6% |
| % $30,000–49,999 | 23.7% | 24.0% | 24.5% | 23.3% | 22.6% |
| % $50,000–74,999 | 18.3% | 18.5% | 20.0% | 17.3% | 17.4% |
| % $75,000+ | 18.4% | 16.8% | 19.0% | 18.2% | 19.5% |
| % Recent Cessation (90-days) | 7.4% | 6.4% | 7.2% | 7.4% | 8.9% |
| Average % CBSA coverage–workplace laws | 40.3% | 9.7% | 29.6% | 60.6% | 63.8% |
| Average % CBSA coverage–hospitality laws | 48.5% | 17.2% | 38.4% | 68.6% | 72.4% |
| Average % self-reported–workplace policies a | 72.1% | 69.8% | 67.0% | 77.8% | 74.7% |
| Model 1 a | Model 2 b | Model 3 c | ||
|---|---|---|---|---|
| Smoke-free workplace law | Ages 25–39 | 1.20 * (1.03–1.40) | 1.06 (0.86–1.32) | |
| Ages 40–54 | 1.12 (0.94–1.33) | 1.27 * (1.00–1.62) | ||
| Ages 55–65 | 1.19 (0.95–1.50) | 0.98 (0.71–1.34) | ||
| Smoke-free hospitality law | Ages 25–39 | 1.20 * (1.02–1.40) | 1.07 (0.86–1.34) | |
| Ages 40–54 | 0.99 (0.83–1.19) | 0.85 (0.66–1.10) | ||
| Ages 55–65 | 1.30 * (1.03–1.63) | 1.26 (0.91–1.75) | ||
| Smoke-free workplace policy (self-report) | Ages 25–39 | 1.05 (0.93–1.19) | 1.00 (0.88–1.13) | |
| Ages 40–54 | 1.30 ** (1.10–1.55) | 1.22 * (1.02–1.45) | ||
| Ages 55–65 | 0.84 (0.65–1.09) | 0.80 (0.62–1.04) | ||
| Ages 25–39 | Ages 40–54 | Ages 55–65 | |
|---|---|---|---|
| Workplace law interactions | |||
| Gender | 0.717 | 0.553 | 0.965 |
| Education | 0.969 | 0.712 | 0.815 |
| Education×gender | 0.412 | 0.230 | 0.378 |
| Race/ethnicity | 0.223 | 0.989 | 0.530 |
| Race/ethnicity×gender | 0.680 | 0.202 | 0.688 |
| Family income | 0.264 | 0.898 | 0.758 |
| Family income×gender | 0.004 † | 0.846 | 0.427 |
| Hospitality law interactions | |||
| Gender | 0.934 | 0.940 | 0.539 |
| Education | 0.161 | 0.782 | 0.849 |
| Education×gender | 0.727 | 0.039 | 0.557 |
| Race/ethnicity | 0.234 | 0.377 | 0.054 |
| Race/ethnicity×gender | 0.643 | 0.477 | 0.611 |
| Family income | 0.284 | 0.207 | 0.374 |
| Family income×gender | 0.184 | 0.483 | 0.441 |
| Self-reported workplace policy interactions | |||
| Gender | 0.922 | 0.751 | 0.810 |
| Education | 0.861 | 0.722 | 0.569 |
| Education×gender | 0.913 | 0.114 | 0.224 |
| Race/ethnicity | 0.155 | 0.934 | 0.578 |
| Race/ethnicity×gender | 0.581 | 0.456 | 0.601 |
| Family income | 0.888 | 0.278 | 0.553 |
| Family income×gender | 0.964 | 0.810 | 0.279 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Titus, A.R.; Kalousova, L.; Meza, R.; Levy, D.T.; Thrasher, J.F.; Elliott, M.R.; Lantz, P.M.; Fleischer, N.L. Smoke-Free Policies and Smoking Cessation in the United States, 2003–2015. Int. J. Environ. Res. Public Health 2019, 16, 3200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173200
Titus AR, Kalousova L, Meza R, Levy DT, Thrasher JF, Elliott MR, Lantz PM, Fleischer NL. Smoke-Free Policies and Smoking Cessation in the United States, 2003–2015. International Journal of Environmental Research and Public Health. 2019; 16(17):3200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173200
Chicago/Turabian StyleTitus, Andrea R., Lucie Kalousova, Rafael Meza, David T. Levy, James F. Thrasher, Michael R. Elliott, Paula M. Lantz, and Nancy L. Fleischer. 2019. "Smoke-Free Policies and Smoking Cessation in the United States, 2003–2015" International Journal of Environmental Research and Public Health 16, no. 17: 3200. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16173200