Home Blood Pressure Monitoring by a Mobile-Based Model in Chongqing, China: A Feasibility Study

Abstract
:1. Introduction
2. Methods
2.1. Study Sites and Sampling
2.2. Monitoring Details
2.3. Intervention, Data Collection and Analysis
3. Results
3.1. Baseline Characteristics
3.2. Interview Results
3.2.1. User Experience and Feasibility of Home Blood Pressure Monitoring by a Mobile-Based Model in Patients
“In less than five minutes. After the machine was tied to my hand all I needed to do was press it. Maybe it just (took me) two minutes.”(Nan’an, female, 48 years old)
“It took (me) less than ten minutes to measure my blood pressure three times and average the values.”(Yangjiaping, female, 54 years old)
“It’s easy enough (for me to complete the measurement).”(Nan’an, female, 68 years old)
“It’s easy to use the instrument. I just think the less trouble, the better. The process is a bit boring for me.”(Nan’an, male, 56)
“Every time I received the reminder, I felt grateful.”(Yangjiaping, male, 61 years old)
“I am impressed with the message, (referring to the information on the phone), ‘You measured your blood pressure very positively yesterday, please stick with it tomorrow.’”(Yangjiaping, male, 64 years old)
“It had me insisting to take the measurement. I had forgotten to measure my blood pressure at the set time somedays, and felt even a little guilty when I received the reminder again one hour later.”(Yangjiaping, female, 64 years old)
“Well, I felt pretty satisfied. I think it was a concern for the elderly. The message wasn’t too long. No matter what you sent me, it was a motivation to us, which wasn’t annoying.”(Nan’an, female, 68 years old)
“I was in a better mood (with the measurement during the study), I also recorded my own blood pressure every day. I was really satisfied that my blood pressure was quite normal at this age.”(Nan’an, female, 75 years old)
“At the very least, I knew more about my own blood pressure.”(Yangjiaping, female, 64 years old)
“It had little effect on me. In fact, I used to measure blood pressure myself (before this study).”(Yangjiaping, male, 54 years old)
3.2.2. Factors Affecting Patients’ Compliance with Home Blood Pressure Monitoring
“It’s not entirely because of the benefits, I also like the measurement.”(Yangjiaping, female, 64 years old)
“Actually, I don’t think it is necessary to measure the blood pressure. I never felt uncomfortable even when my blood pressure was 160 or 170.”(Nan’an, male, 53 years old)
“I prefer to measure my blood pressure at six o’clock am every day, I usually begin to exercise at 6:30, so I have to take the sphygmomanometer with me every morning to ensure my blood pressure value could be fed back at the specified time these days.”(Nan’an, female, 75 years old)
“I am more willing to measure my blood pressure from ten to eleven o’clock am, because I need to buy food earlier than this period, and then prepare lunch for my grandchildren.”(Yangjiaping, female, 72 years old)
“I would like to measure earlier in the morning if I need to go out in the afternoon, but I prefer to measure my blood pressure in the afternoon if I am busy doing housework in the morning.”(Yangjiaping, female, 54 years old)
“I think it’s better to measure blood pressure every day. The value can be different after two minutes.”(Nan’an, female, 75 years old)
“In fact, I think it (blood pressure) should be measured every day. Since you gave me this instrument I have measured my blood pressure twice a day.”(Yangjiaping, female, 64 years old)
3.2.3. Patients’ Willingness to Use an App to Monitor Blood Pressure in the Future
“It will be more labor-saving to receive feedback automatically by an application, and it’ll be nice if we do not need to input our blood pressure ourselves.”(Yangjiaping, female, 54 years old)
“Both (application or WeChat) works for me. Although I could not input my blood pressure values manually by typing, I could use voice to feed back the values through WeChat.”(Yangjiaping, female, 64 years old)
“I’d like to (measure blood pressure in the future), since I have developed the habit during these days.”(Nan’an, female, 75 years old)
“Sure, I think it’s a good thing and a responsibility for our health.”(Nan’an, female, 68 years old)
3.2.4. Health Care Provider Experience with Home Blood Pressure Monitoring Using a Mobile-Phone Model
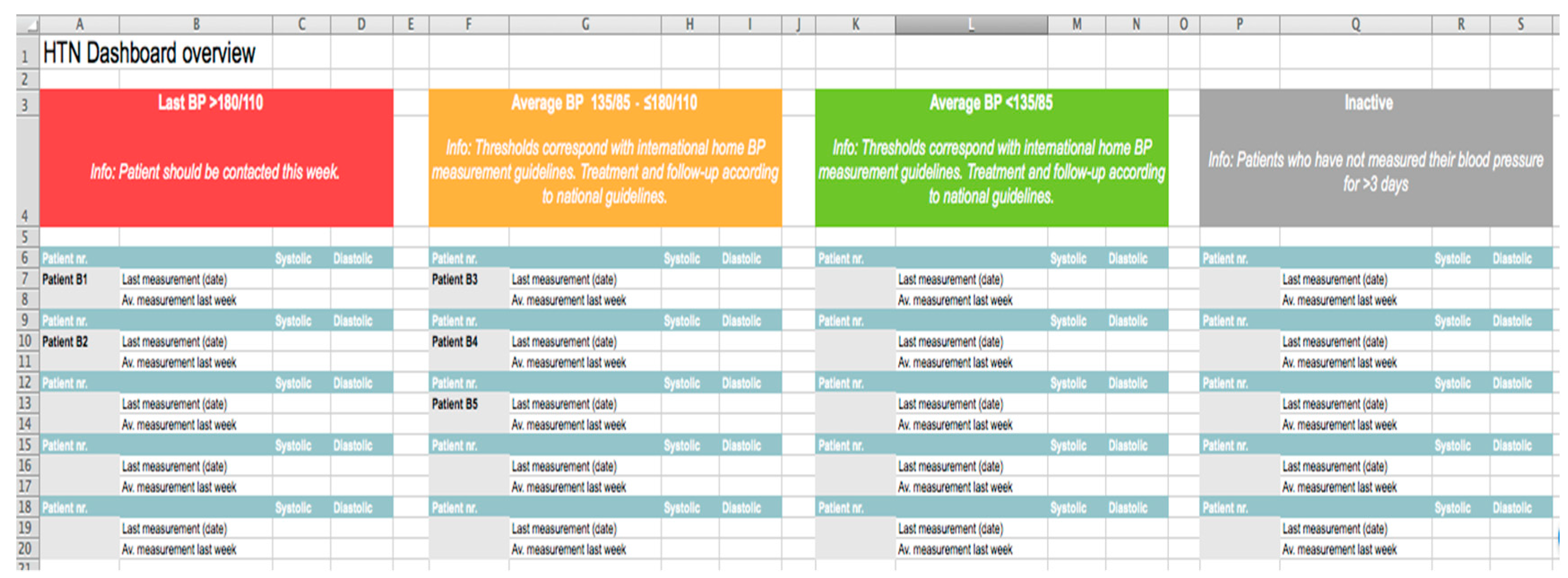
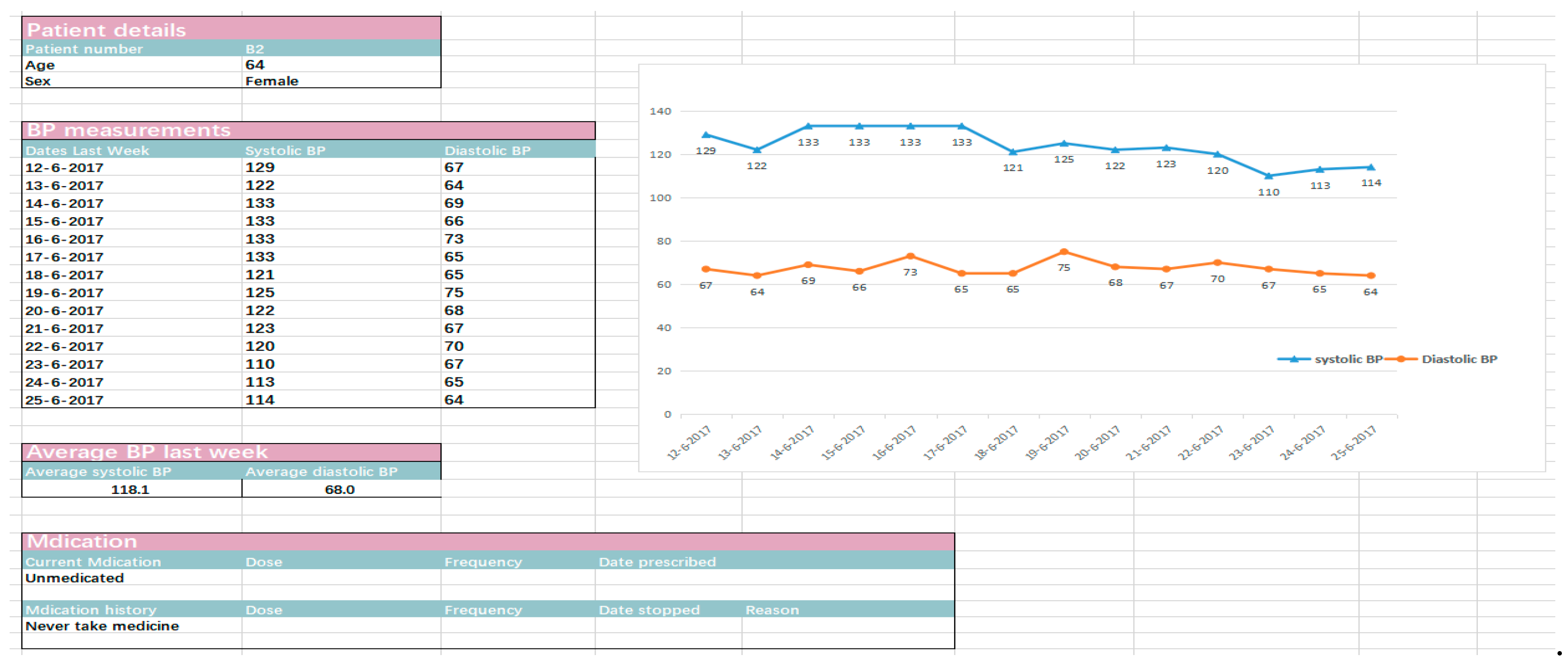
“Patients in the orange category were those whose blood pressure was not well controlled, so I mainly paid attention to this area. There were also a few patients in the red category. I tended to use the fluctuation of the blood pressure over one week (Figure 1) as the basis for treatment, rather than a single value.”(Care provider, Nan’an, female)
“I started with the red category and especially cared about the details of those unusual values; I would look at their mean values and fluctuations of blood pressure, so that I could determine whether the high value was caused by improper measurement methods or exercise prior to measurement.”(Care provider, Yangjiaping, female)
“If patients appeared in the red category, they would be called into the clinic for the treatment; otherwise, patients would be observed for another period of time, and would be notified to come into the clinic if the value was still abnormal.”(Care provider, Yangjiaping, female)
“The management model of daily monitoring increased the communication time between the patients and I, particularly for patients with uncontrolled blood pressure. It would be quicker (to check the dashboard) if their blood pressure was well controlled.”(Care provider, Nan’an, female)
“It would be better if a weekly average of patients in the orange category and daily high-risk situations (red category) of patients were reported in the dashboard, and I preferred patients’ blood pressure values be ranked from high to low.”(Care provider, Yangjiaping, female)
“During this study, we did not provide feedback to patients in the green category (those with controlled hypertension), but they actually also hoped to receive the provider’s feedback, otherwise they may think it’s useless for them.”(Care provider, Yangjiaping, female)
“It would be better if patients’ medication, lifestyle, and complications could be added to the received dashboard.”(Care provider, Yangjiaping, female)
4. Discussion
5. Strengths and limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lackland, D.T.; Weber, M.A. Global Burden of Cardiovascular Disease and Stroke: Hypertension at the Core. Can. J. Cardiol. 2015, 31, 569–571. [Google Scholar] [CrossRef]
- Datta, B.K.; Husain, M.J.; Fatehin, S.; Kostova, D. Consumption displacement in households with noncommunicable diseases in Bangladesh. PLoS ONE 2018, 13, e0208504. [Google Scholar] [CrossRef]
- Tang, S.; Ehiri, J.; Long, Q. China’s biggest, most neglected health challenge: Non-communicable diseases. Infect. Dis. Poverty 2013, 2, 7. [Google Scholar] [CrossRef]
- Yan, L.D.; Chirwa, C.; Chi, B.H.; Bosomprah, S.; Sindano, N.; Mwanza, M.; Musatwe, D.; Mulenga, M.; Chilengi, R. Hypertension management in rural primary care facilities in Zambia: A mixed methods study. BMC Health Serv. Res. 2017, 17, 111. [Google Scholar] [CrossRef]
- Shahaj, O.; Denneny, D.; Schwappach, A.; Pearce, G.; Epiphaniou, E.; Parke, H.L.; Taylor, S.J.C.; Pinnock, H. Supporting self-management for people with hypertension: A meta-review of quantitative and qualitative systematic reviews. J. Hypertens. 2019, 37, 264–279. [Google Scholar] [CrossRef]
- Still, C.H.; Jones, L.M.; Moss, K.O.; Variath, M.; Wright, K.D. African American Older Adults’ Perceived Use of Technology for Hypertension Self-Management. Res. Gerontol. Nurs. 2018, 11, 249–256. [Google Scholar] [CrossRef]
- The SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2016, 42, e141–e143. [Google Scholar]
- Tatiana, D.; John, M.G.; Martina, M.; Brunner-Jackson, B.; Favella, A.; Anderson, A.; Torres, M.; Ruggiero, K.J.; Treiber, F.A. Evaluation of an mHealth Medication Regimen, Self-Management Program for African American and, Hispanic Uncontrolled Hypertensives. J. Pers. Med. 2015, 5, 389–405. [Google Scholar]
- Mao, A.Y. A Mobile Phone-Based Health Coaching Intervention for Weight Loss and Blood Pressure Reduction in a National Payer Population: A Retrospective Study. JMIR Mhealth Uhealth 2017, 5, e80. [Google Scholar] [CrossRef]
- Whitehead, L. The Effectiveness of Self-Management Mobile Phone and Tablet Apps in Long-term Condition Management: A Systematic Review. J. Med. Internet Res. 2016, 18, e97. [Google Scholar] [CrossRef]
- Tencent Inc. Wechat Data Report 2018 [E/OL]; Tencent Inc.: Shenzhen, China, 2018; Available online: https://support.weixin.qq.com/cgi-bin/mmsupport-bin/getopendays (accessed on 16 August 2019).
- National Institute for Health and Care Excellence. 2019. Available online: https://www.nice.org.uk/guidance/ng136/chapter/Recommendations (accessed on 3 September 2019).
- Clarke, M.; Fursse, J.; Jones, R.W. Early experiences of the use of remote patient monitoring for the long term management of chronic disease. In Proceedings of the International Conference of the IEEE Engineering in Medicine & Biology Society, Vancouver, BC, Canada, 20–24 August 2008; IEEE: Piscataway, NJ, USA, 2008. [Google Scholar]
- Revision Committee of the Guidelines for the Prevention and Treatment of Hypertension in China. Guidelines for the Prevention and Treatment of Hypertension in China(2019 Revision). Chin. J. Cardiovasc. Med. 2019, 24, 25. (In Chinese) [Google Scholar]
- Beratarrechea, A.; Lee, A.G.; Willner, J.M.; Jahangir, E.; Ciapponi, A.; Rubinstein, A. The impact of mobile health interventions on chronic disease outcomes in developing countries: A systematic review. Telemed. E-Health 2014, 20, 75–82. [Google Scholar] [CrossRef]
- Márquez, E.C.; Márquez, S.R.; Rodríguez, E.G.; López-García-Ramos, L.; Pastoriza, J.V.; Baldonedo, A.S.; Gracia, C.D.; Gil, V.G.; Martell, N.C. Specific hypertension smartphone app to improve medication adherence in hypertension: A cluster-randomized trial. Curr. Med. Res. Opin. 2018, 35, 1–15. [Google Scholar]
- Project Reaction. Remote Accessibility to Diabetes Management and Therapy in Operational Healthcare Networks [E/OL]. 2014. Available online: https://www.reaction-project.eu/downloads.php?cat_id=4 (accessed on 3 September 2019).
- Debon, R.; Coleone, J.D.; Bellei, E.A.; De Marchi, A.C.B. Mobile health applications for chronic diseases: A systematic review of features for lifestyle improvement. Diabetes Metab. Syndr. 2019, 13, 2507–2512. [Google Scholar] [CrossRef]
- Gao, C.; Zhou, L.; Liu, Z.; Wang, H.; Bowers, B. Mobile application for diabetes self-management in China: Do they fit for older adults? Int. J. Med. Inf. 2017, 101, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Ebert, L.; Liu, X.; Chan, S.W. A mobile application of breast cancer e-support program versus routine Care in the treatment of Chinese women with breast cancer undergoing chemotherapy: Study protocol for a randomized controlled trial. BMC Cancer 2017, 17, 291. [Google Scholar] [CrossRef]
- Shimamoto, K.; Ando, K.; Fujita, T.; Hasebe, N.; Higaki, J.; Horiuchi, M.; Imai, Y.; Imaizumi, T.; Ishimitsu, T.; Ito, M.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2014). Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2014, 37, 253–390. [Google Scholar]
- Feng, X.L.; Pang, M.; Beard, J. Health system strengthening and hypertension awareness, treatment and control: Data from the China Health and Retirement Longitudinal Study. Bull. World Health Organ. 2014, 92, 29. [Google Scholar] [CrossRef]
- Tocci, G.; Nati, G.; Cricelli, C.; Parretti, D.; Lapi, F.; Ferrucci, A.; Borghi, C.; Volpe, M. Prevalence and Control of Hypertension in Different Macro-Areas in Italy: Analysis of a Large Database by the General Practice. High Blood Press. Cardiovasc. Prev. 2016, 23, 1–7. [Google Scholar] [CrossRef]
- Merck, S.F. Chronic Disease and Mobile Technology: An Innovative Tool for Clinicians. Nurs. Forum. 2017, 52, 298–305. [Google Scholar] [CrossRef]
- Adler, A.J.; Martin, N.; Mariani, J.; Tajer, C.D.; Owolabi, O.O.; Free, C.; Serrano, N.C.; Casas, J.P.; Perel, P. Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. In The Cochrane Library; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2017. [Google Scholar]
- Gandhi, S.; Chen, S.; Hong, L.; Sun, K.; Gong, E.; Li, C.; Yan, L.L.; Schwalm, J.D. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can. J. Cardiol. 2016, 33, 219–231. [Google Scholar]
- Haricharan, H.J.; Heap, M.; Hacking, D.; Lau, Y.K. Health promotion via SMS improves hypertension knowledge for deaf South Africans. BMC Public Health 2017, 17, 663. [Google Scholar] [CrossRef]
- Kannisto, K.A.; Koivunen, M.H.; Välimäki, M.A. Use of mobile phone text message reminders in health care services: A narrative literature review. J. Med. Internet Res. 2014, 16, e222. [Google Scholar] [CrossRef]
- CDC. High Blood Pressure Fact Sheet [EB/OL]; CDC: Atlanta, GA, USA, 2016. Available online: https://www.cdc.gov/DHDSP/data_statistics/fact_sheets/fs_bloodpressure.htm (accessed on 16 August 2019).
- Akoko, B.M.; Fon, P.N.; Ngu, R.C.; Ngu, K.B. Knowledge of Hypertension and Compliance with Therapy Among Hypertensive Patients in the Bamenda Health District of Cameroon: A Cross-sectional Study. Cardiol. Ther. 2017, 6, 53–67. [Google Scholar]
- Albini, F.; Liu, X.; Torlasco, C.; Soranna, D.; Faini, A.; Ciminaghi, R.; Celsi, A.; Benedetti, M.; Zambon, A.; Di Rienzo, M.; et al. An ICT and mobile health integrated approach to optimize patients’ education on hypertension and its management by physicians: The Patients Optimal Strategy of Treatment(POST) pilot study. In Proceedings of the Engineering in Medicine & Biology Society, Orlando, FL, USA, 16–20 August 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Smith, R.; Menon, J.; Rajeev, J.G.; Feinberg, L.; Kumar, R.K.; Banerjee, A. Potential for the use of mHealth in the management of cardiovascular disease in Kerala: A qualitative study. BMJ Open 2015, 5, e009367. [Google Scholar] [CrossRef]
- Toro-Ramos, T.; Lee, D.H.; Kim, Y.; Michaelides, A.; Oh, T.J.; Kim, K.M.; Jang, H.C.; Lim, S. Effectiveness of a Smartphone Application for the Management of Metabolic Syndrome Components Focusing on Weight Loss: A Preliminary Study. Metab. Syndr. Relat. Disord. 2017, 15, 465–473. [Google Scholar] [CrossRef]
- Ashoorkhani, M.; Bozorgi, A.; Majdzadeh, R.; Hosseini, H.; Yoonessi, A.; Ramezankhani, A.; Eftekhar, H. Comparing the effectiveness of the BPMAP (Blood Pressure Management Application) and usual care in self-management of primary hypertension and adherence to treatment in patients aged 30–60 years: Study protocol for a randomized controlled trial. Trials 2016, 17, 511. [Google Scholar] [CrossRef]
- Toro-Ramos, T.; Kim, Y.; Wood, M.; Rajda, J.; Niejadlik, K.; Honcz, J.; Marrero, D.; Fawer, A.; Michaelides, A. Efficacy of a mobile hypertension prevention delivery platform with human coaching. J. Hum. Hypertens. 2017, 31, 795. [Google Scholar]
- Doocy, S.; Paik, K.E.; Lyles, E.; Tam, H.H.; Fahed, Z.; Winkler, E.; Kontunen, K.; Mkanna, A.; Burnham, G. Guidelines and mHealth to Improve Quality of Hypertension and Type 2 Diabetes Care for Vulnerable Populations in Lebanon: Longitudinal Cohort Study. JMIR Mhealth Uhealth 2017, 5, e158. [Google Scholar] [Green Version]



{kind=link}
{kind=link}
| Themes | Questions |
|---|---|
| 1. Operational feasibility of blood pressure measurement | How long do you need to measure your blood pressure every day? |
| Do you feel the process of measuring or use of the instrument difficult for you? | |
| 2. Personal experience of home blood pressure monitoring in the past two weeks | What was the most impressive or favorite reminder that you received during the past two weeks and why? |
| How did you feel during the past two-week measurement? | |
| 3. Factors affecting patients’ compliance with home blood pressure monitoring | What time of day do you usually measure your blood pressure? |
| What are the reasons for why you persist in blood pressure measurement? | |
| Would it be easier for you to keep on measuring at the time chosen by yourself? | |
| Do you prefer a daily or weekly measurement? | |
| 4. Patients’ willingness to use an app to monitor blood pressure in the future | would it be better to use an app to automatically feedback blood pressure in the future? |
| Would you like to measure your blood pressure every day in the future? |
| Basic Characteristics | Total | Nan’an | Yangjiaping | P Value |
|---|---|---|---|---|
| Gender | 0.4076 | |||
| Female (%) | 10 | 6 (60%) | 4 (40%) | |
| Male (%) | 10 | 4 (40%) | 6 (60%) | |
| Age, mean (SD) | 59.55 (8.91) | 59.90 (10.06) | 59.20 (7.57) | 0.8694 |
| Systolic blood pressure at entry, mean (SD) | 140.50 (17.57) | 142.50 (20.96) | 138.50 (13.05) | 0.6328 |
| Diastolic blood pressure at entry, mean (SD) | 83.25 (10.98) | 81.30 (9.55) | 85.20 (11.92) | 0.4537 |
| Frequency of self-measurements before this study (n) | 0.1079 | |||
| Never | 6 (60%) | 4 (40%) | 2 (20%) | |
| Once every two weeks | 6 (60%) | 4 (40%) | 2 (20%) | |
| Once a week on average | 3 (30%) | 1 (10%) | 2 (20%) | |
| Once/day | 5 (50%) | 1 (10%) | 4 (40%) |
| Variables | At Entry, Mean (SD) | After One-Week Measurement, Mean (SD) | P Value | At Entry, Mean (SD) | After Two-Week Measurement, Mean (SD) | P Value |
|---|---|---|---|---|---|---|
| Systolic blood pressure | ||||||
| Nan’an | 142.50(20.96) | 130.80(13.66) | 0.3022 | 142.50(20.96) | 131.60(15.84) | 0.3465 |
| Yangjiaping | 138.50(13.05) | 124.20(5.89) | 0.0470* | 138.50(13.05) | 126.60(13.11) | 0.1005 |
| Total | 140.50(17.57) | 127.50(10.51) | 0.0451* | 140.50(17.57) | 129.10(13.96) | 0.0746 |
| Diastolic blood pressure | ||||||
| Nan’an | 81.30(9.55) | 78.60(11.26) | 0.6499 | 81.30(9.55) | 79.40(9.86) | 0.7344 |
| Yangjiaping | 85.20(11.92) | 76.60(9.34) | 0.2015 | 85.20(11.92) | 77.60(13.79) | 0.3037 |
| Total | 83.25(10.98) | 77.60(9.81) | 0.1883 | 83.25(10.98) | 78.50(11.35) | 0.2866 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiao, M.; Lei, X.; Zhang, F.; Sun, Z.; Harris, V.C.; Tang, X.; Yan, L. Home Blood Pressure Monitoring by a Mobile-Based Model in Chongqing, China: A Feasibility Study. Int. J. Environ. Res. Public Health 2019, 16, 3325. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183325
Xiao M, Lei X, Zhang F, Sun Z, Harris VC, Tang X, Yan L. Home Blood Pressure Monitoring by a Mobile-Based Model in Chongqing, China: A Feasibility Study. International Journal of Environmental Research and Public Health. 2019; 16(18):3325. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183325
Chicago/Turabian StyleXiao, Meng, Xun Lei, Fan Zhang, Zhenxing Sun, Vanessa Catherine Harris, Xiaojun Tang, and Lijing Yan. 2019. "Home Blood Pressure Monitoring by a Mobile-Based Model in Chongqing, China: A Feasibility Study" International Journal of Environmental Research and Public Health 16, no. 18: 3325. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183325