Practical Guidance for Interventions in Adults with Metabolic Syndrome: Diet and Exercise vs. Changes in Body Composition

 , and
, and
Abstract
:1. Introduction
1.1. Metabolic Syndrome (MS): Concept, Prevalence and Diagnostic Criteria
1.2. MS: Causes, Diet, Exercise and Anthropometric Parameters
2. Materials and Methods
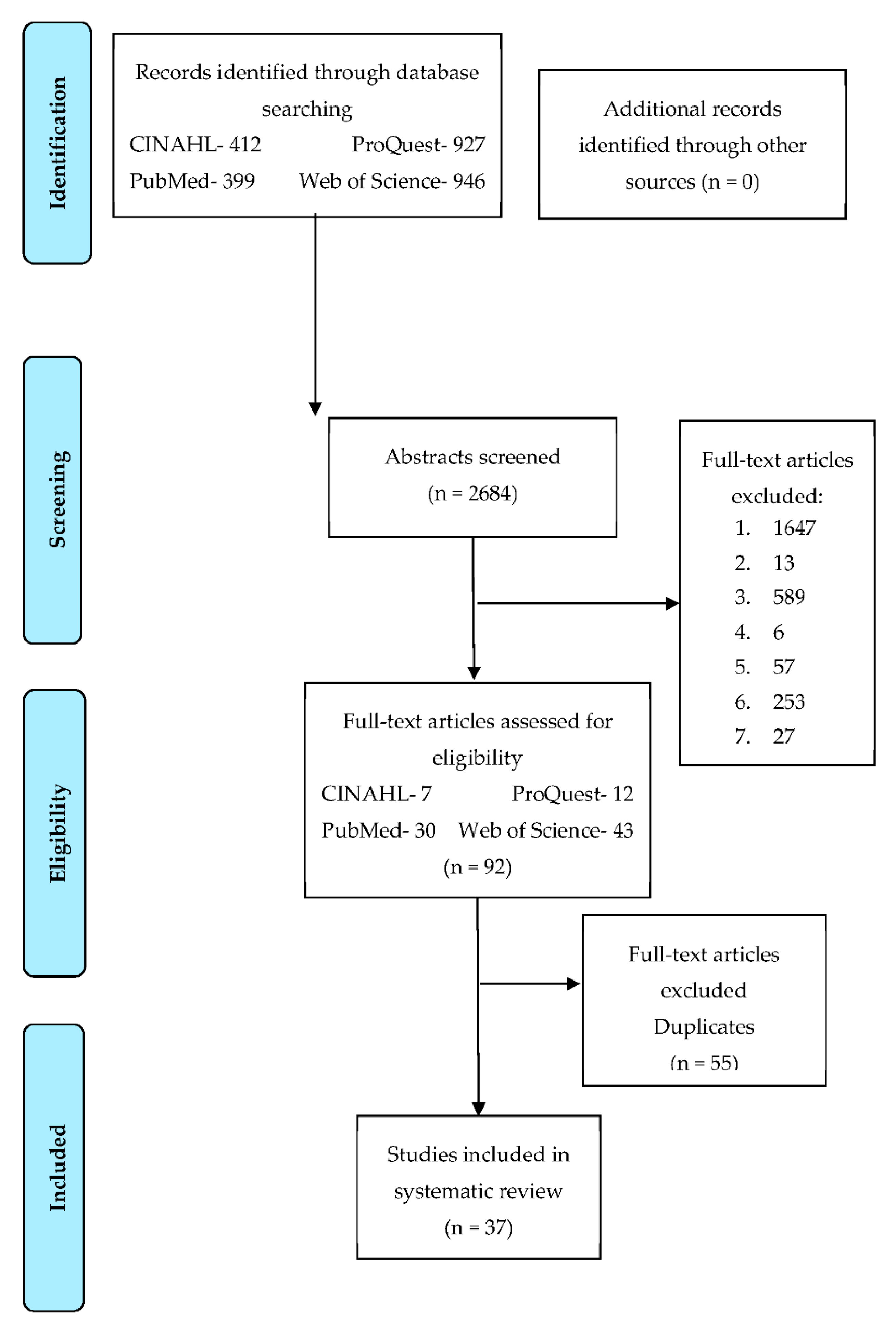
2.1. Search Strategy and Information Processing
2.2. Selection of the Articles Previously Identify
- Population: characteristics of the population studied (country of origin, type of diagnostic criteria, number, age and gender), inclusion and exclusion criteria.
- Interventions: exclusive and multidisciplinary as therapeutic treatments.
- Comparators: inclusion of randomized clinical trials, control and intervention groups are identified. In principle, only the intervention groups receive the therapeutic treatment that should cause changes in body composition.
- Results: identified as variation in body composition, presenting significant and not significant variations.
- Characteristics of clinical trials: authors, year of publication, type of randomized clinical trial, duration of intervention, instrument of analysis of body composition, type of intervention used (exclusive or multidisciplinary) and body composition variation (measured with different anthropometric parameters and units of measurement).
2.3. Data Analysis, Identification of Information Loss Risks
3. Results
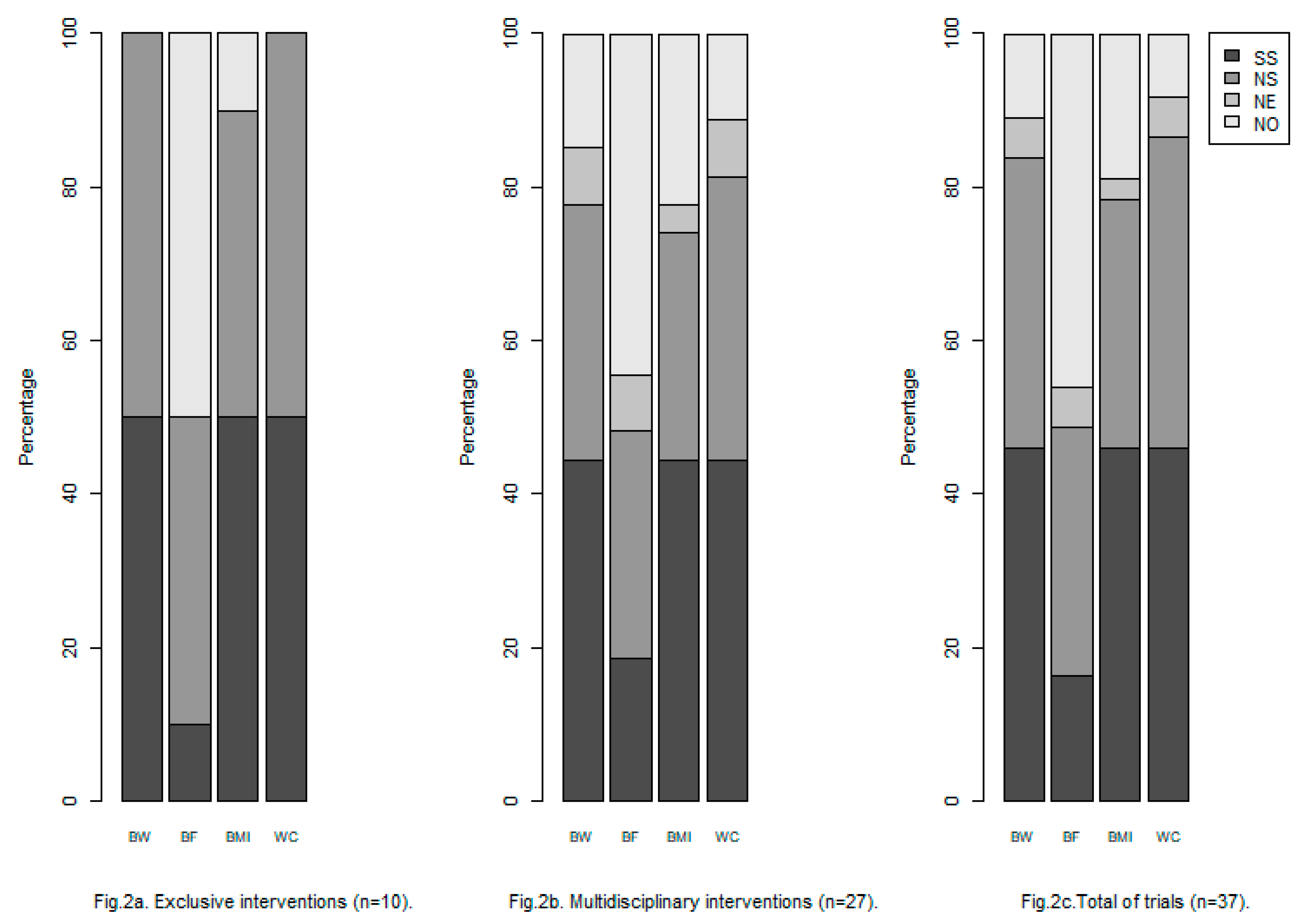
3.1. Search Features and Types of Interventions Identified
3.2. The Most Significant Body Composition Changes in MS (Table 2 and Table 3)
3.3. Anthropometric Parameters and Units of MS Changes in Body Composition Measurements (Table 2 and Table 3)
4. Discussion
- The available procedures must be identified to recognize in what type of patients and in what moment they must be applied. The variation in the use of the procedures can be due to factors as: ethnic groups, age, gender and physical limitations (in case of the use of crutches, prothesis and/or wheelchair or even in patients without toes due to amputations because of the diabetes) [71,86].
- The use of distance or remote health care is recommendable: (i) when the patient does not reside in the same population of the center of health and/or hospital [86]; (ii) in case of older people or specific cases in which the patients find hard to attend themselves to the center [86]; (iii) in coaching strategy [90,91].
- Monitoring of physical exercise and/or daily physical activity is recommended (triaxial accelerometers) [92].
- It is recommended to extrapolate the concept “obesogenic” for MS patients. This concept was firstly used in 1996 (“obese” means excess of corporal fat and “genic” refers to production or synthesis) [93]. Currently, the obesogenic environmental is defined as “the addition of the influences that have the environments, the opportunities or the living conditions to promote the obesity in individuals or populations” [94]. These influences promote the consumption of high levels or energy as well as diets based on non-healthy food (fast food, take away meals, etc.) [95].
- Coaching is highly recommended as part of the design of further clinical trials with MS patients. In the coaching per pairs approach during interventions of overweight, obesity and diabetes patients, several instructed patients are selected to accompany and monitor to other patients suffering the same pathology. Some recent studies have revealed that thanks to the coaching per pairs approach, the levels of glycosylated hemoglobin, cholesterol, LDL, blood pressure, corporal mass index (CMI), relation waist—hip, selfcare activities in the case of diabetes, depression and other quality life factors are positively modified [90,91,96,97].
- The nutritionist should be focused on “how” the patient or the family can apply the recommendations given by professionals. The intervention must be considered not only for the professional but also for the patient as a dynamic process, in which it will be necessary to overcome unforeseen challenges [86,98].
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaur, J. A Comprehensive Review on Metabolic Syndrome. Cardiol. Res. Pract. 2014, 2014, 943162. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M. Metabolic syndrome update. Trends Cardiovasc. Med. 2016, 26, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Duprez, D.; Toleuova, A. Prehypertension and the cardiometabolic syndrome: Pathological and clinical consequences. Expert Rev. Cardiovasc. Ther. 2013, 11, 1725–1733. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Pucci, G.; Alcidi, R.; Tap, L.; Battista, F.; Mattace-Raso, F.; Schillaci, G. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: A review of the literature. Pharmacol. Res. 2017, 120, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Bekkouche, L.; Bouchenak, M.; Malaisse, W.; Yahia, D. The Mediterranean Diet Adoption Improves Metabolic, Oxidative, and Inflammatory Abnormalities in Algerian Metabolic Syndrome Patients. Horm. Metab. Res. 2014, 46, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Jonsdottir, S.E.; Brader, L.; Gunnarsdottir, I.; Kally Magnusdottir, O.; Schwab, U.; Kolehmainen, M.; Risérus, U.; Herzig, K.H.; Cloetens, L.; Helgegren, H.; et al. Adherence to the Nordic Nutrition Recommendations in a Nordic population with metabolic syndrome: High salt consumption and low dietary fibre intake (The SYSDIET study). Food Nutr. Res. 2013, 57. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Martín-Calvo, N. The major European dietary patterns and metabolic syndrome. Rev. Endocr. Metab. Disord. 2013, 14, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Bremer, A.A.; Lustig, R.H. What is metabolic syndrome, and why are children getting it? Ann. N. Y. Acad. Sci. 2013, 1281, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Pérez, E.A.; Olivares, V.M.; Martínez-Espinosa, R.M.; Vila, M.D.M.; García-Galbis, M.R. New Insights about How to Make an Intervention in Children and Adolescents with Metabolic Syndrome: Diet, Exercise vs. Changes in Body Composition. A Systematic Review of RCT. Nutrients 2018, 10, 878. [Google Scholar] [CrossRef]
- Alicka, M.; Marycz, K. The Effect of Chronic Inflammation and Oxidative and Endoplasmic Reticulum Stress in the Course of Metabolic Syndrome and Its Therapy. Stem Cells Int. 2018, 2018, 4274361. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Barbagallo, M. The biology of the metabolic syndrome and aging. Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 5–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Monforte, M.; Sánchez, E.; Barrio, F.; Costa, B.; Flores-Mateo, G. Metabolic syndrome and dietary patterns: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2016, 56, 925–947. [Google Scholar] [CrossRef] [PubMed]
- Hong, A.R.; Lim, S. Clinical characteristics of metabolic syndrome in Korea, and its comparison with other Asian countries. J. Diabetes Investig. 2015, 6, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Calton, E.K.; James, A.P.; Pannu, P.K.; Soares, M.J. Certain dietary patterns are beneficial for the metabolic syndrome: Reviewing the evidence. Nutr. Res. 2014, 34, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhang, X.; Xiang, Y.-B.; Yang, G.; Li, H.; Gao, Y.-T.; Zheng, W.; Shu, X.-O. Adherence to dietary guidelines and mortality: A report from prospective cohort studies of 134,000 Chinese adults in urban Shanghai. Am. J. Clin. Nutr. 2014, 100, 693–700. [Google Scholar] [CrossRef]
- Golbidi, S.; Laher, I. Exercise Induced Adipokine Changes and the Metabolic Syndrome. J. Diabetes Res. 2014, 2014, 726861. [Google Scholar] [CrossRef] [PubMed]
- Jukarainen, S.; Holst, R.; Dalgård, C.; Piirilä, P.; Lundbom, J.; Hakkarainen, A.; Lundbom, N.; Rissanen, A.; Kaprio, J.; Kyvik, K.O.; et al. Cardiorespiratory Fitness and Adiposity as Determinants of Metabolic Health-Pooled Analysis of Two Twin Cohorts. J. Clin. Endocrinol. Metab. 2017, 102, 1520–1528. [Google Scholar] [CrossRef]
- Smith, U. Abdominal obesity: A marker of ectopic fat accumulation. J. Clin. Investig. 2015, 125, 1790–1792. [Google Scholar] [CrossRef]
- Vasques, A.C.J.; Cassani, R.S.L.; E Forti, A.C.; Vilela, B.S.; Pareja, J.C.; Tambascia, M.A.; Geloneze, B.; BRAMS Investigators. Sagittal Abdominal Diameter as a Surrogate Marker of Insulin Resistance in an Admixtured Population—Brazilian Metabolic Syndrome Study (BRAMS). PLoS ONE 2015, 10, e0125365. [Google Scholar] [CrossRef] [PubMed]
- Kroeger, C.M.; Hoddy, K.K.; Varady, K.A. Impact of Weight Regain on Metabolic Disease Risk: A Review of Human Trials. J. Obes. 2014, 2014, 614519. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Wiesman, F.; Hasman, A.; Herik, H.V.D. Information retrieval: An overview of system characteristics. Int. J. Med Inform. 1997, 47, 5–26. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Rubio, M.A.; Barbany, M.; Moreno, B. SEEDO 2007 Consensus for the evaluation of overweight and obesity and the establishment of therapeutic intervention criteria. Med. Clín. 2007, 128, 184–196. [Google Scholar]
- Mohammadi-Sartang, M.; Bellissimo, N.; De Zepetnek, J.O.T.; Brett, N.R.; Mazloomi, S.M.; Fararouie, M.; Bedeltavana, A.; Famouri, M.; Mazloom, Z. The effect of daily fortified yogurt consumption on weight loss in adults with metabolic syndrome: A 10-week randomized controlled trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 565–574. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Casas-Agustench, P.; López-Uriarte, P.; Bulló, M.; Ros, E.; Cabré-Vila, J.; Salas-Salvadó, J. Effects of one serving of mixed nuts on serum lipids, insulin resistance and inflammatory markers in patients with the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 126–135. [Google Scholar] [CrossRef]
- Muzio, F.; Mondazzi, L.; Harris, W.S.; Sommariva, D.; Branchi, A. Effects of moderate variations in the macronutrient content of the diet on cardiovascular disease risk factors in obese patients with the metabolic syndrome. Am. J. Clin. Nutr. 2007, 86, 946–951. [Google Scholar] [CrossRef] [Green Version]
- Mora-Rodriguez, R.; Ortega, J.F.; Morales-Palomo, F.; Ramirez-Jimenez, M. Weight loss but not gains in cardiorespiratory fitness after exercise-training predicts improved health risk factors in metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1267–1274. [Google Scholar] [CrossRef]
- Irving, B.A.; Weltman, J.Y.; Patrie, J.T.; Davis, C.K.; Brock, D.W.; Swift, D.; Barrett, E.J.; Gaesser, G.A.; Weltman, A. Effects of Exercise Training Intensity on Nocturnal Growth Hormone Secretion in Obese Adults with the Metabolic Syndrome. J. Clin. Endocrinol. Metab. 2009, 94, 1979–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irving, B.A.; Davis, C.K.; Brock, D.W.; Weltman, J.Y.; Swift, D.; Barrett, E.J.; Gaesser, G.A.; Weltman, A. Effect of exercise training intensity on abdominal visceral fat and body composition. Med. Sci. Sports Exerc. 2008, 40, 1863–1872. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Chair, S.Y.; Wong, E.M.-L. The effects of a lifestyle intervention program on physical outcomes, depression, and quality of life in adults with metabolic syndrome: A randomized clinical trial. Int. J. Cardiol. 2017, 230, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Weinstock, R.S.; Trief, P.M.; Cibula, D.; Morin, P.C.; Delahanty, L.M. Weight Loss Success in Metabolic Syndrome by Telephone Interventions: Results from the SHINE Study. J. Gen. Intern. Med. 2013, 28, 1620–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanri, A.; Tomita, K.; Matsushita, Y.; Ichikawa, F.; Yamamoto, M.; Nagafuchi, Y.; Kakumoto, Y.; Mizoue, T. Effect of Six Months Lifestyle Intervention in Japanese Men with Metabolic Syndrome: Randomized Controlled Trial. J. Occup. Health 2012, 54, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.; Sorkin, J.D.; Mastella, L.; Sutherland, A.; Rhyne, J.; Donnelly, P.; Simpson, K.; Goldberg, A.P. Poly is more effective than monounsaturated fat for dietary management in the metabolic syndrome: The muffin study. J. Clin. Lipidol. 2016, 10, 996–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora-Rodríguez, R.; Ortega, J.F.; Guio de Prada, V.; Fernández-Elías, V.E.; Hamouti, N.; Morales-Palomo, F.; Martinez-Vizcaino, V.; Nelson, R.K. Effects of Simultaneous or Sequential Weight Loss Diet and Aerobic Interval Training on Metabolic Syndrome. Int. J. Sports Med. 2016, 37, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.M.; Jackson, K.A.H.; Roussell, M.A.; West, S.G.; Kris-Etherton, P.M. Type and amount of dietary protein in the treatment of metabolic syndrome: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Bonfanti, N.; Fernández, J.M.; Gomez-Delgado, F.; Pérez-Jiménez, F. Effect of two hypocaloric diets and their combination with physical exercise on basal metabolic rate and body composition. Nutr. Hosp. 2014, 29, 635–643. [Google Scholar]
- Neumayr, G.; Fries, D.; Mittermayer, M.; Humpeler, E.; Klingler, A.; Schobersberger, W.; Spiesberger, R.; Pokan, R.; Schmid, P.; Berent, R. Effects of hiking at moderate and low altitude on cardiovascular parameters in male patients with metabolic syndrome: Austrian Moderate Altitude Study. Wilderness Environ. Med. 2014, 25, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Lac, G.; LeSourd, B.; Chapier, R.; Walther, G.; Vinet, A.; Sapin, V.; Verney, J.; Ouchchane, L.; Duclos, M.; et al. Different modalities of exercise to reduce visceral fat mass and cardiovascular risk in metabolic syndrome: The RESOLVE randomized trial. Int. J. Cardiol. 2013, 168, 3634–3642. [Google Scholar] [CrossRef] [PubMed]
- Landaeta-Díaz, L.; Fernández, J.M.; Da Silva-Grigoletto, M.; Rosado-Alvarez, D.; Gómez-Garduño, A.; Gómez-Delgado, F.; López-Miranda, J.; Pérez-Jiménez, F.; Fuentes-Jiménez, F. Mediterranean diet, moderate-to-high intensity training, and health-related quality of life in adults with metabolic syndrome. Eur. J. Prev. Cardiol. 2013, 20, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Malin, S.K.; Niemi, N.; Solomon, T.P.; Haus, J.M.; Kelly, K.R.; Filion, J.; Rocco, M.; Kashyap, S.R.; Barkoukis, H.; Kirwan, J.P. Exercise training with weight loss and either a high or low glycemic diet reduces metabolic syndrome severity in older adults. Ann. Nutr. Metab. 2012, 61, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Straznicky, N.E.; Lambert, E.A.; Grima, M.T.; Eikelis, N.; Nestel, P.J.; Dawood, T.; Schlaich, M.P.; Masuo, K.; Chopra, R.; Sari, C.I.; et al. The effects of dietary weight loss with or without exercise training on liver enzymes in obese metabolic syndrome subjects. Diabetes Obes. Metab. 2012, 14, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Wood, R.J.; Gregory, S.M.; Sawyer, J.; Milch, C.M.; Matthews, T.D.; Headley, S.A. Preservation of Fat-Free Mass after Two Distinct Weight Loss Diets with and without Progressive Resistance Exercise. Metab. Syndr. Relat. Disord. 2012, 10, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Seligman, B.G.; Polanczyk, C.A.; Santos, A.S.; Foppa, M.; Junges, M.; Bonzanini, L.; Nicolaidis, G.; Camey, S.; Lopes, A.L.; Sehl, P.; et al. Intensive practical lifestyle intervention improves endothelial function in metabolic syndrome independent of weight loss: A randomized controlled trial. Metabolism 2011, 60, 1736–1740. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Grima, M.T.; Lambert, E.A.; Eikelis, N.; Dawood, T.; Lambert, E.; Nestel, P.J.; Masuo, K.; Sari, C.I.; Chopra, R.; et al. Exercise augments weight loss induced improvement in renal function in obese metabolic syndrome individuals. J. Hypertens. 2011, 29, 553–564. [Google Scholar] [CrossRef]
- Lerman, R.H.; Minich, D.M.; Darland, G.; Lamb, J.J.; Chang, J.-L.; Hsi, A.; Bland, J.S.; Tripp, M.L. Subjects with elevated LDL cholesterol and metabolic syndrome benefit from supplementation with soy protein, phytosterols, hops rho iso-alpha acids, and Acacia nilotica proanthocyanidins. J. Clin. Lipidol. 2010, 4, 59–68. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, E.A.; Nestel, P.J.; McGrane, M.T.; Dawood, T.; Schlaich, M.P.; Masuo, K.; Eikelis, N.; de Courten, B.; Mariani, J.A.; et al. Sympathetic neural adaptation to hypocaloric diet with or without exercise training in obese metabolic syndrome subjects. Diabetes 2010, 59, 71–79. [Google Scholar] [CrossRef]
- Straznicky, N.E.; Lambert, G.W.; McGrane, M.T.; Masuo, K.; Dawood, T.; Nestel, P.J.; Eikelis, N.; Schlaich, M.P.; Esler, M.D.; Socratous, F.; et al. Weight Loss May Reverse Blunted Sympathetic Neural Responsiveness to Glucose Ingestion in Obese Subjects with Metabolic Syndrome. Diabetes 2009, 58, 1126–1132. [Google Scholar] [CrossRef]
- Yassine, H.N.; Marchetti, C.M.; Krishnan, R.K.; Vrobel, T.R.; Gonzalez, F.; Kirwan, J.P. Effects of Exercise and Caloric Restriction on Insulin Resistance and Cardiometabolic Risk Factors in Older Obese Adults—A Randomized Clinical Trial. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2009, 64, 90–95. [Google Scholar] [CrossRef]
- Katcher, H.I.; Legro, R.S.; Kunselman, A.R.; Gillies, P.J.; Demers, L.M.; Bagshaw, D.M.; Kris-Etherton, P.M. The effects of a whole grain-enriched hypocaloric diet on cardiovascular disease risk factors in men and women with metabolic syndrome. Am. J. Clin. Nutr. 2008, 87, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Chaiyasoot, K.; Sarasak, R.; Pheungruang, B.; Dawilai, S.; Pramyothin, P.; Boonyasiri, A.; Supapueng, O.; Jassil, F.C.; Yamwong, P.; Batterham, R.L. Evaluation of a 12-week lifestyle education intervention with or without partial meal replacement in Thai adults with obesity and metabolic syndrome: A randomised trial. Nutr. Diabetes 2018, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Jahangiry, L.; Montazeri, A.; Najafi, M.; Yaseri, M.; Farhangi, M.A. An interactive web-based intervention on nutritional status, physical activity and health-related quality of life in patient with metabolic syndrome: A randomized-controlled trial (The Red Ruby Study). Nutr. Diabetes 2017, 7, e240. [Google Scholar] [CrossRef]
- Fappa, E.; Yannakoulia, M.; Ioannidou, M.; Skoumas, Y.; Pitsavos, C.; Stefanadis, C. Telephone counselling intervention improves dietary habits and metabolic parameters of patients with the metabolic syndrome: A randomized controlled trial. Rev. Diabet. Stud. 2012, 9, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Saboya, P.P.; Bodanese, L.C.; Zimmermann, P.R.; Gustavo, A.D.; Macagnan, F.E.; Feoli, A.P.; Oliveira, M.D. Lifestyle Intervention on Metabolic Syndrome and its Impact on Quality of Life: A Randomized Controlled Trial. Arq. Bras. Cardiol. 2017, 108, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Huelgas, R.; Jansen-Chaparro, S.; Baca-Osorio, A.; Mancera-Romero, J.; Tinahones, F.; Bernal-Lopez, M. Effects of a long-term lifestyle intervention program with Mediterranean diet and exercise for the management of patients with metabolic syndrome in a primary care setting. Eur. J. Intern. Med. 2015, 26, 317–323. [Google Scholar] [CrossRef]
- Luley, C.; Blaik, A.; Götz, A.; Kicherer, F.; Kropf, S.; Isermann, B.; Stumm, G.; Westphal, S. Weight Loss by Telemonitoring of Nutrition and Physical Activity in Patients with Metabolic Syndrome for 1 Year. J. Am. Coll. Nutr. 2014, 33, 363–374. [Google Scholar] [CrossRef]
- Fuller, N.R.; Pearson, S.; Lau, N.S.; Wlodarczyk, J.; Halstead, M.B.; Tee, H.-P.; Chettiar, R.; Kaffes, A.J.; Tee, H. An intragastric balloon in the treatment of obese individuals with metabolic syndrome: A randomized controlled study. Obesity 2013, 21, 1561–1570. [Google Scholar] [CrossRef]
- Fappa, E.; Yannakoulia, M.; Skoumas, Y.; Valourdou, S.; Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Promoting only the consumption of healthy foods may be an alternative strategy for treating patients with the metabolic syndrome. Metabolism 2012, 61, 1361–1369. [Google Scholar] [CrossRef]
- Oh, E.G.; Bang, S.Y.; Hyun, S.S.; Kim, S.H.; Chu, S.H.; Jeon, J.Y.; Im, J.-A.; Lee, M.K.; Lee, J.E. Effects of a 6-month lifestyle modification intervention on the cardiometabolic risk factors and health-related qualities of life in women with metabolic syndrome. Metabolism 2010, 59, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.-G.; Hyun, S.S.; Kim, S.H.; Bang, S.-Y.; Chu, S.H.; Jeon, J.Y.; Kang, M.S. A randomized controlled trial of therapeutic lifestyle modification in rural women with metabolic syndrome: A pilot study. Metabolism 2008, 57, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. Int. J. Surg. 2012, 10, 28–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Royall, D.; Brauer, P.; Bjorklund, L.; O’Young, O.; Tremblay, A.; Jeejeebhoy, K.; Heyland, D.; Dhaliwal, R.; Klein, D.; Mutch, D.M. Development of a Dietary Management Care Map for Metabolic Syndrome. Can. J. Diet. Pract. Res. 2014, 75, 132–139. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M. Commentary on the clinical management of metabolic syndrome: Why a healthy lifestyle is important. BMC Med. 2012, 10, 139. [Google Scholar] [CrossRef] [PubMed]
- Garvey, W.T.; Mechanick, J.I.; Brett, E.M.; Garber, A.J.; Hurley, D.L.; Jastreboff, A.M.; Nadolsky, K.; Pessah-Pollack, R.; Plodkowski, R. Reviewers of the AACE/ACE Obesity Clinical Practice Guidelines. American Association of Clinical Endocrinologist and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with obesity. Endocr. Pract. 2016, 22, 1–203. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Camacho, P.M.; Cobin, R.H.; Garber, A.J.; Garber, J.R.; Gharib, H.; Petak, S.M.; Rodbard, H.W.; Trence, D.L. American Association of Clinical Endocrinologists Protocol for Standardized Production of Clinical Practice Guidelines—2010 Update. Endocr. Pract. 2010, 16, 270–283. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network. Obesity in Scotland. Integrating Prevention with Weight Management. A National Clinical Guideline Recommended for Use in Scotland; Scottish Intercollegiate Guidelines Network: Edinburgh, Scotland, 1996. [Google Scholar]
- American Diabetes Association. 4. Lifestyle Management. Diabetes Care 2017, 40, 33–43. [Google Scholar] [CrossRef]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; DeFronzo, R.A.; Einhorn, D.; Fonseca, V.A.; et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm—2018 Executive Summary. Endocr. Pract. 2018, 24, 91–120. [Google Scholar] [CrossRef]
- Coulston, A.M.; Rosen, C. American health care reform: Implications for medical nutrition therapy. Am. J. Clin. Nutr. 1994, 59, 1275–1276. [Google Scholar] [CrossRef] [PubMed]
- Champagne, C.M.; Bray, G.A. Dietary management of the metabolic syndrome—One size fits all? Proc. Nutr. Soc. 2013, 72, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Soares, M.J.; Mohan, V.; Anoop, S.; Abhishek, V.; Vaidya, R.; Pradeepa, R. Body fat, metabolic syndrome and hyperglycemia in South Asians. J. Diabetes Complicat. 2018, 32, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Armani, A.; Berry, A.; Cirulli, F.; Caprio, M. Molecular mechanisms underlying metabolic syndrome: The expanding role of the adipocyte. FASEB J. 2017, 31, 4240–4255. [Google Scholar] [CrossRef] [PubMed]
- Engin, A. The Definition and Prevalence of Obesity and Metabolic Syndrome. Adv. Exp. Med. Biol. 2017, 960, 1–17. [Google Scholar] [PubMed]
- Grundy, S.M. Adipose tissue and metabolic syndrome: Too much, too little or neither. Eur. J. Clin. Investig. 2015, 45, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.L.; Soeters, M.R.; Wüst, R.C.I.; Houtkooper, R.H. Metabolic Flexibility as an Adaptation to Energy Resources and Requirements in Health and Disease. Endocr. Rev. 2018, 39, 489–517. [Google Scholar] [CrossRef] [Green Version]
- Kahlhöfer, J.; Lagerpusch, M.; Skurk, T.; Müller, M.J.; Bosy-Westphal, A.; Bosy-Westphal, A. Deep body composition phenotyping during weight cycling: Relevance to metabolic efficiency and metabolic risk. Obes. Rev. 2015, 16, 36–44. [Google Scholar]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle Weight-Loss Intervention Outcomes in Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- García-Galbis, M.R.; Baeza, M.R.; Castell, E.C. Indicators of success in the dietary management of overweight and obesity: Weight, body fat loss and quality. Nutr. Hosp. 2015, 32, 1009–1016. [Google Scholar]
- Argimon, J.M.; Jimenéz, J. Métodos de Investigación Clínica y Epidemiológica, 4th ed.; Elsevier: Barcelona, Spain, 2013. [Google Scholar]
- Raynor, H.A.; Davidson, P.G.; Burns, H.; Nadelson, M.D.H.; Mesznik, S.; Uhley, V.; Moloney, L. Medical Nutrition Therapy and Weight Loss Questions for the Evidence Analysis Library Prevention of Type 2 Diabetes Project: Systematic Reviews. J. Acad. Nutr. Diet. 2017, 117, 1578–1611. [Google Scholar] [CrossRef] [PubMed]
- García-Galbis, M.R. The management of qualitative and quantitative dietary treatment for overweight and obesity: Methodology and a new perspective on individualised assessment. Nutr. Hosp. 2015, 32, 2019–2029. [Google Scholar]
- Müller, M.J.; Braun, W.; Pourhassan, M.; Geisler, C.; Bosy-Westphal, A. Application of standards and models in body composition analysis. Proc. Nutr. Soc. 2016, 75, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X. Changes in body composition and metabolic disease risk. Eur. J. Clin. Nutr. 2019, 73, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.V.; Murthy, V.L.; Abbasi, S.A.; Blankstein, R.; Kwong, R.Y.; Goldfine, A.B.; Jerosch-Herold, M.; Lima, J.A.; Ding, J.; Allison, M.A. Visceral Adiposity and the Risk of Metabolic Syndrome Across Body Mass Index. JACC Cardiovasc. Imaging 2014, 7, 1221–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aalaa, M.; Sanjari, M.; Aghaei Meybodi, H.R.; Amini, M.R.; Qorbani, M.; Adibi, H.; Mehrdad, N. The Effectiveness of a Peer Coaching Education on Control and Management of Type 2 Diabetes in Women: A Protocol for a Randomized Controlled Trial. Int. J. Community Based Nurs. Midwifery 2017, 5, 153–164. [Google Scholar]
- Rogers, E.A.; Hessler, D.M.; Bodenheimer, T.S.; Ghorob, A.; Vittinghoff, E.; Thom, D.H. Diabetes peer coaching: Do “better patients” make better coaches? Diabetes Educ. 2014, 40, 107–115. [Google Scholar] [CrossRef] [PubMed]
- De Toro-Martín, J.; Arsenault, B.J.; Després, J.-P.; Vohl, M.-C. Precision Nutrition: A Review of Personalized Nutritional Approaches for the Prevention and Management of Metabolic Syndrome. Nutrients 2017, 9, 913. [Google Scholar] [CrossRef]
- Gauthier, K.I.; Krajicek, M.J. Obesogenic environment: A concept analysis and pediatric perspective. J. Spéc. Pediatr. Nurs. 2013, 18, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Cauchi, D.; Rutter, H.; Knai, C. An obesogenic island in the Mediterranean: Mapping potential drivers of obesity in Malta. Public Health Nutr. 2015, 18, 3211–3223. [Google Scholar] [CrossRef] [PubMed]
- Giskes, K.; van Lenthe, F.; Avendano-Pabon, M.; Brug, J. A systematic review of environmental factors and obesogenic dietary intakes among adults: Are we getting closer to understanding obesogenic environments? Obes. Rev. 2011, 12, e95–e106. [Google Scholar] [CrossRef] [PubMed]
- Pirbaglou, M.; Katz, J.; Motamed, M.; Pludwinski, S.; Walker, K.; Ritvo, P. Personal Health Coaching as a Type 2 Diabetes Mellitus Self-Management Strategy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Health Promot. 2018, 32, 1613–1626. [Google Scholar] [CrossRef] [PubMed]
- Van Rinsum, C.; Gerards, S.; Rutten, G.; Philippens, N.; Janssen, E.; Winkens, B.; Van De Goor, I.; Kremers, S. The Coaching on Lifestyle (CooL) Intervention for Overweight and Obesity: A Longitudinal Study into Participants’ Lifestyle Changes. Int. J. Environ. Res. Public Health 2018, 15, 680. [Google Scholar] [CrossRef] [PubMed]
- Reig García-Galbis, M.; Rizo Baeza, M.M.; Cortés Castell, E. Predictors of weight loss and fat in the dietary management: Sex, age, BMI and consulting assistance. Nutr. Hosp. 2015, 32, 1028–1035. [Google Scholar] [CrossRef]
- Issurin, V.B. Benefits and Limitations of Block Periodized Training Approaches to Athletes’ Preparation: A Review. Sports Med. 2016, 46, 329–338. [Google Scholar] [CrossRef]
- Issurin, V.B. New Horizons for the Methodology and Physiology of Training Periodization. Sports Med. 2010, 40, 189–206. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Vanderlee, L.; Raffoul, A.; Stapleton, J.; Csizmadi, I.; Boucher, B.A.; Massarelli, I.; Rondeau, I.; Robson, P.J. Self-Report Dietary Assessment Tools Used in Canadian Research: A Scoping Review. Adv. Nutr. 2017, 8, 276–289. [Google Scholar] [CrossRef] [Green Version]
- Ortega, R.; Requejo, A.M. Nutriguía. Manuel de Nutrición Clínica, 2nd ed.; Editorial Panamericana: Madrid, España, 2015; pp. 137–152. [Google Scholar]
- Pan American Health Organization. International Guide to Monitor Alcohol Consumption and Its Health Consequences; World Health Organization: Geneva, Switzerland, 2000; pp. 159–167. Available online: https://apps.who.int/iris/bitstream/handle/10665/66529/WHO_MSD_MSB_00.4.pdf;jsessionid=0F2662BB866105AC29BBB1B42A990576?sequence=1 (accessed on 4 September 2019).



{kind=link}
{kind=link}
| Search Strategy | CINAHL Identified/Included | ProQuest Identified/Included | PubMed Identified/Included | Web of Science Identified/Included |
|---|---|---|---|---|
| “metabolic syndrome” AND “weight loss” OR “weight reduction” OR “fat loss” OR “fat reduction” OR “lifestyle” AND “exercise” OR “physical activity” OR “sport” OR “weightlifting” | 222/5 | 532/7 | 187/22 | 303/29 |
| “metabolic syndrome” AND “weight loss” OR “weight reduction” OR “fat loss” OR “fat reduction” OR “lifestyle” AND “diet” OR “dietary treatment” AND “feeding” OR “nutrition” OR “nutritional counselling” | 27/1 | 87/2 | 18/2 | 149/6 |
| “type II diabetes” OR “insulin resistance” AND “weight ls” OR “weight reduction” OR “fat loss” OR “fat reduction” AND “diet” OR “dietary treatment” OR “feeding” AND “nutrition” OR “nutritional counselling” OR “lifestyle” | 44/0 | 77/0 | 42/2 | 155/3 |
| “type II diabetes” OR “insulin resistance” AND “weight loss” OR “weight reduction” OR “fat loss” OR “fat reduction” AND “exercise” OR “physical activity” OR “sport” OR “weightlifting” | 119/1 | 231/3 | 152/4 | 339/5 |
| Author (s) [26,27,28,29,30,31,32,33,34,35] | Location | Study Design | MS Diagnosis Criteria [1] | Sample/Groups/Characteristics Studied | Duration (Months) | Body Composition Measurement Instrument | Intervention Method Characteristics Studied/Comparative Statistical Analysis of BC | Anthropometric Parameters and Measurement Unit Analyzed (Statistical Results) | Decreases in Body Composition Mean ± SD or Mean ± (SE) or Mean (CI, 95%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BW (kg/%) | BF (kg or %) | BMI (kg/m2/%) | WC (cm/%) | |||||||||
| [26] | Asia (Iran) | RCT | ATPIII | n = 87 IG1: 43 IG2: 44 Women: 60.95% Age: 45.5 | 2.5 | Body composition indices were measured via bioelectric impedance analysis (BIA; In Body s10; Korea). Height was measured bar using a stadiometer | Diet - Within groups: IG1: low fat plain yogurt IG2: fortified yogurt - Between groups | YES/NO p < 0.001 p < 0.001 NS | YES/YES p < 0.0001 p < 0.05 p < 0.05 | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 p < 0.05 | BW: IG1: 4.3 ± 1.9 kg IG2: 5.1 ± 3.0 kg BF: IG1: 1.7 ± 2.4 kg and 1.7 ± 3.2% IG2: 3.4 ± 4.7 kg and 3.0 ± 2.8% BMI: IG1: 1.6± 0.1 kg IG2: 1.8 ± 1.16 kg WC: IG1: 4.4 ± 1.7 cm IG2: 5.8 ± 2.0 cm |
| [27] | Asia (Israel) | RCT (parallel-arm) | ATPIII | n = 74 IG1: 38 IG2: 36 Women: 100% Age: 30–57 | 3 | BW and WC were measured by using a scale model Detector Physician Beam Scale (HOSPEQ, Inc., Miami, FL) vs. the same person according to the guidelines of the National Heart, Lung, and Blood Institute respectively | Diet- Within groups: IG1 (high breakfast kcal content) IG2 (high dinner kcal content) - Between groups | YES/NO p < 0.0001 p < 0.05 p < 0.0001 | NO/NO | YES/NO p < 0.0001 p < 0.05 p < 0.0001 | YES/NO p < 0.0001 p < 0.05 p < 0.0001 | BW: IG1: 8.7 ± (1.4) kg IG2: 3.6 ± (1.5) kg BMI: IG1: 3.1± (0.4) kg/m2 IG2: 1.3± (0.4) kg/m2 WC: IG1: 8.7 ± (0.9) cm IG2: 3.6 ± (0.9) cm |
| [28] | Europe (Spain) | RCT (parallel-group) | ATP III | n = 50 IG1: 25 IG2: 25 Men (56%) Age: 18–65 | 3 | Height and BC was measured using a wall-mounted stadiometer vs. Tanita TBF-300 (Tanita Corp., Tokyo, Japan) bioimpedance analysis device respectively | Diet - Within groups: IG1 (nut diet) IG2 - Between groups | YES/NO p < 0.05 p < 0.05 NS | YES (%)/NO p < 0.05 p < 0.05 NS | NO/NO | YES/NO p < 0.05 p < 0.05 NS | BW: IG1: 2.2 kg (0.9–3.4) IG2: 1.5 kg (0.6–2.4) BF: IG1: 1.9% (0.9–2.5) IG2: 1.1% (0.3–1.9) WC: IG1: 3.8 cm (1.9–5.8) IG2: 2.7 cm (1.0–4.4) |
| [29] | Europe (Italy) | RCT | ATP III | n = 100 IG1: 50 IG2: 50 Women: 73% Age: >18 | 5 | Height was measured using a stadiometer and WC, to the measurement of the narrowest circumference between the bottom of the rib cage and the iliac crest by using an unstretched tape measure | Diet - Within groups: IG1 (high CH diet) IG2 (low CH diet) - Between groups | YES/YES p < 0.001 p < 0.001 NS | NO/NO | YES/NO p < 0.001 p < 0.001 NS | YES/YES p < 0.001 p < 0.001 NS | BW: IG1: NE (kg) IG1: 10% IG2: NE (kg) IG2: 10% BMI: IG1: NE IG2: NE WC: IG1: NE (cm) IG1: 8% IG2: NE (cm) IG2: % |
| [30] | Europe (Spain) | RCT (Randomized-block) | IDF | n = 160 IG: 138 CG: 22 Women: 50% Age: 54 ± 8 | 4 | Body weight was assessed in an electronic scale (Hawk, Mettler Toledo, USA) body composition was determined by dual energy X-ray absorptiometry (DXA Hologic Series Discovery Wi QDR, Bedford, USA). WC was measured in a horizontal plane 2 cm above the iliac crest | Exercise Within groups: IG: aerobic interval training CG: sedentary Between groups | YES/NO p < 0.05 NE p < 0.05 | YES/NO NS NE NS | YES/NO p < 0.05 NE p < 0.05 | YES/NO p < 0.05 NE p < 0.05 | BW: IG: 1.2 kg CG: increase BF: IG: 0.7 kg CG: increase BMI: IG: 0.4 kg CG: increase WC: IG: 2.6 cm CG: increase |
| [31] | North America (USA) | RCT | IDF | n = 34 CG: 10 IG1:13 IG2: 11 Women: 75% Age: 49.1 ± 1.8 | 4 | Air displacement plethysmography (Bod-Pod; Life Measurement Instruments, Concord, CA) | Exercise - Within groups: IG1 (low intensity exercise) IG2 (high intensity) - Between groups | YES/NO p < 0.01 p < 0.01 NS | YES (%)/NO p < 0.01 p < 0.01 NS | YES/NO p < 0.01 p < 0.01 NS | YES/NO NS p < 0.01 NS | BW: IG1: 2.7 kg IG2: 2.7 kg BF: IG1: 0.7% IG2: 1.6% BMI: IG1: 0.9 kg/m2 IG2: 0.9 kg/m2 WC: IG1: 2 cm IG2: 4.9 cm |
| [32] | North America (USA) | RCT | IDF | n = 27 CG: 7 IG1: 11 IG2: 9 Women: 100% Age: 51 ± 9 | 4 | Air displacement plethysmography (Bod-Pod, Life Measurement Instruments, Concord, CA) | Exercise - Within groups: IG1 (low-intensity aerobic) IG2 (moderate-to-high intensity aerobic) - Between groups: IG1 vs. IG2 IG1 vs. CG IG2 vs. CG | YES/NO NS p < 0.05 NS NS NS | YES (%)/NO NS p < 0.05 NS NS NS | YES/NO NS p < 0.05 NS NS NS | YES/NO NS p < 0.05 p < 0.05 NS p < 0.05 | BW: IG1: 2.1 kg IG2: 3.5 kg BF: IG1: 0.4% IG2: 1.7% BMI: IG1: 0.8 kg/m2 IG2: 1.3 kg/m2 WC: IG1: 1.2 cm IG2: 5.6 cm |
| [33] | Asia (China) | RCT | IDF | n = 173 IG: 86 CG: 87 Women: 50.8% Age: 24–78 | 3 | NE | Intervention in lifestyle - Within groups: IG (Lifestyle intervention program) - Between groups | YES/NO NE p < 0.01 | NO/NO | YES/NO NE p < 0.01 | YES/NO NE NS | BW: IG: 1.77 kg CG: increase BMI: IG: 0.58 kg/m2 CG: 0.01 kg/m2 WC: IG: 3.69 (male)/1.37 (female) CG: 1.61 (male)/1.34 (female) |
| [34] | North America (USA) | RCT | IDF | n = 135 IG1: 72 IG2: 63 Women: 75% Age: 52 | 24 | The International Diabetes Federation definition requires central obesity, measured by WC with ethnicity-based cutoffs | Intervention in lifestyle - Within groups: IG1 (individual counselling) IG2 (group counselling) - Between groups | YES/YES p < 0.05 p < 0.05 p < 0.001 | NO/NO | YES/NO p < 0.001 p < 0.05 p < 0.05 | YES/NO p < 0.05 p < 0.05 NS | BW: IG1: 2.2 ± 14.2 kg IG1: 1.8 ± 18.6% IG2: 6.2 ± 14.3 kg IG2: 5.6 ± 26.8% BMI: IG1: 0.8 kg/m2 IG2: 2.1 kg/m2 WC: IG1: 2.4 ± 15.5 cm IG2: 3.1 ± 15.5 cm |
| [35] | Asia (East Asia) | RCT | The Examination Committee of Criteria for “Metabolic Syndrome” in Japan | n = 102 IG:49 CG:53 Men: 100% Age: 53.2 ± 6.8 | 6 | Body height and body weight were measured using an automated scale (AD-6225A; A&D, Tokyo, Japan) | Intervention in lifestyle CG (standard healthy recommendations) - Within groups: IG (intervention in lifestyle) - Between groups | YES/NO p < 0.001 p < 0.001 | NO/NO | YES/NO p < 0.001 p < 0.01 | YES/NO p < 0.001 p < 0.05 | BW: IG: 2.01 kg BMI: IG: 0.6 kg/m2 WC: IG: 2.51 cm |
| Author(s) [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] | Location | Study Design | MS Diagnosis Criteria [1] | Sample/Groups/Characteristics Studied | Duration (months) | Body Composition Measurement Instrument | Intervention Method/Comparative Statistical Analysis of the BC | Anthropometric Parameters and Measurement Unit Analyzed (Statistical results) | Decreases in Body Composition Mean ± SD or Mean ± (SE) or Mean (CI, 95%) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BW (kg/%) | BF (kg or %) | BMI (kg/m2/%) | WC (cm/%) | |||||||||
| [36] | North America (USA) | RCT | NE | n = 39 IG1:23 IG2:16 Women: 60% Age: 38–76 | 6 | NE | Diet, exercise - Within groups: IG1 (hypocaloric diet + MUFA) IG2 (hypocaloric diet + PUFA) - Between groups | YES/NO NS p < 0.01 NE | NO/NO | NO/NO | NO/NO | BW: IG1: 2.3 kg ± (1) IG2: 4.6 kg ± (2) |
| [37] | Europe (Spain) | RCT | NE | n = 36 CG: 12 IG1:12 IG2: 12 Men: 75% Age: 54 ± 9 | 4 | Dual Energy X-ray absorptiometry scans (Hologic Discovery DXA Series Wi QDR, Bedford, USA) | Diet, exercise - Within groups: IG1 (EXER-then-DIET) IG2 (EXER+DIET) - Between groups: IG1 vs. CG IG2 vs. CG IG2 vs. IG1 | YES/YES NS p < 0.05 NE NE NE | YES/NO NS p < 0.05 NE NE NE | YES/NO NS p < 0.05 NE NE NE | YES/NO p < 0.05 p < 0.05 NS p < 0.05 NS | BW: IG1: NE kg IG1: NE% IG2: NE kg IG2: 5.5 ± 0.8% BF: IG1: NE (kg) IG2: NE (kg) BMI: IG1: increase IG2: 1.8 kg/m2 WC: IG1: NE (cm) IG2: NE (cm) |
| [38] | Oceania (Australia) | RCT | ATPIII | n = 62 IG1: 21 IG2: 20 IG3: 21 Women: 55% Age: 30–60 | 6 | The participants weighing < 157 kg was measured with Hologic DXA (QDR-4500W; Hologic Corporation), and those weighing > 157 kg were measured with a GE Lunar iDXA (General Electric) | Diet, exercise - Within groups: IG1 (M-DASH diet) IG2 (BOLD diet) IG3 (BOLD + diet) - Between groups | YES/NO p < 0.001 p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 p < 0.001 NS | BW: IG1: 5.1 kg IG2: 4.8 kg IG3: 4.8 kg BF: NE BMI: IG1: 1.8 kg/m2 IG2: 0.5 kg/m2 IG2: 1.7 kg/m2 WC: IG1: 5.5 cm IG2: 7.6 cm IG3: 6.2 cm |
| [39] | Europe (Spain) | RCT | ATP III | n = 36 IG1: 8 IG2: 8 IG3: 10 IG4: 10 Women and Men: NE Age: 50–70 | 3 | The anthropometric study stated by the International Society for the Advancement of Kit anthropometry (method ISAK); to evaluate BW and height rods were used (MB 201T Bonus); the cutaneous folds were valued by means of the Harpenden calibrator | Diet, exercise Within groups: IG1 (Hypocaloric Med diet) IG2 (Low fat-high CH diet) IG3 (Hypocaloric Med diet and exercise) IG4 (Low fat-high diet and exercise) - Between groups: IG2 vs. IG1 IG2 vs. IG3 IG2 vs. IG4 IG4 vs. IG1 IG4 vs. IG3 | NO/YES NS p < 0.05 NS p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 | NO/YES p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 | NO/NO | NO/NO | BW: IG1: ~ 7% IG2: ~ 8% IG3: ~ 5% IG4: ~ 10% BF: IG1: ~ 7% IG2: ~ 10% IG3: ~ 9% IG4: ~ 12% |
| [40] | Europe (Austria) | RCT | ATPIII | n = 71 IG1: 36 IG2: 35 Men: 100% Age: 36–66 | 0.75 | NE | Diet, exercise - Within groups: IG1 (moderate altitude exercise) IG2 (sea level exercise) - Between groups | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NE | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NE | BW: IG1: 3.22 ± 1.91 kg IG2: 3.04 ± 2.16 kg BF: NE BMI: IG1: 0.81 kg/m2 IG2: 0.69 kg/m2 WC: NE |
| [41] | Europe (France) | RCT | OMS | n = 78 IG1: 24 IG2: 24 IG3: 30 Women: 56% Age: 50–70 | 12 | DXA (Hologic QDR 4500 series; Waltham, USA) | Diet, exercise - Within groups: IG1 (moderate-resistance and moderate-endurance) IG2 (high-resistance and moderate-endurance) IG3 (moderate-resistance and high-endurance) - Between groups | NO/YES p < 0.001 p < 0.001 p < 0.001 NS | NO/YES p < 0.001 p < 0.001 p < 0.001 NS | NO/NO | NO/YES p < 0.001 p < 0.001 p < 0.001 NS | BW: All: 6.3 ± 7.2% IG1: 5.9 ± 5.8% IG2: 8.4 ± 8.9% IG3: 4.7 ± 6.7% BF: All: 1.7 ± 1.7% IG1: 1.8 ± 1.5% IG2: 2.1 ± 2.3% IG3: 1.3 ± 1.3% WC: All: 7.7 ± 6.2% IG1: 7.7 ± 6.6% IG2: 9.5 ± 6.8% IG3: 6.3 ± 5% |
| [42] | Europe (Spain) | RCT | ATPIII | n = 40 IG1: 20 IG2: 20 Women: 67% Age: 50–66 | 3 | NE | Diet, exercise - Within groups: IG1 IG2 (exercise) - Between groups | YES/YES p < 0.05 p < 0.05 p < 0.05 | YES (%)/NO p < 0.05 p < 0.05 p < 0.05 | YES/NO p < 0.05 p < 0.05 p < 0.05 | YES/NO p < 0.05 p < 0.05 NS | BW: IG1: 5.38 kg IG1: 6.23 ± (0.83)% IG2: 8.38 kg IG2: 8.45 ± (0.76)% BF: IG1: 2.76% IG2: 4.5% BMI: IG1: 2.09 kg/m2 IG2: 3.26 kg/m2 WC: IG1: 3.72 cm IG2: 4.18 cm |
| [43] | North America (USA) | RCT | ATP III | n = 21 IG1: 11 IG2: 10 Men: 52% Age: 66.2 ± 1.1 | 3 | Dual-x-ray absorptiometry (DEXA; Lunar Prodigy, Madison, WI); Height was measured with a wall-mounted stadiometer and weight was recorded on a digital scale in a hospital gown | Diet, exercise - Within groups: IG1 (high glycemic diet) IG2 (low glycemic diet) - Between groups | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | NO/YES p < 0.05 p < 0.05 p < 0.05 | BW: IG1: 11 kg IG2: 6.8 kg BF: IG1: 8.9 kg IG2: 5.7 kg BMI: IG1: 3.6 kg/m2 IG2: 2.7 kg/m2 WC: IG1: ~10% IG2: ~6% |
| [44] | Oceania (Australia) | RCT | IDF | n = 58 IG1: 20 IG2: 19 CG: 19 Men: 59% Age: 55 ± 6 | 3 | Dual-energy X-ray absorptiometry (DXA, GE-LUNAR Prodigy Advance PA+130510, GE Medical Systems, Lunar, Madison, WI, USA) | Diet, exercise - Within groups: IG1 (diet) IG2 (diet and exercise) - Between groups: IG1 vs. IG2 IG1 vs. CG IG2 vs. CG | YES/NO p < 0.001 p < 0.001 NS p < 0.01 p < 0.01 | YES/NO p < 0.001 p < 0.001 NS p < 0.01 p < 0.01 | YES/NO p < 0.001 p < 0.001 NS p < 0.01 p < 0.01 | YES/NO p < 0.001 p < 0.001 NS p < 0.05 p < 0.01 p < 0.01 | BW: IG1: 7.1 ± 2.9 kg IG2: 8.7 ± 4.6 kg BF: IG1: 5.2± 3.0 kg IG2: 7.0± 3.9 kg BMI: IG1: 2.4± 1.0 kg/m2 IG2: 2.9± 1.4 kg/m2 WC: IG1: 6.7±3.2 cm IG2: 10.0±5.2cm |
| [45] | North America (USA) | RCT (parallel-arm) | ATPIII | n = 32 IG1: 8 IG2: 9 IG3: 8 IG4: 7 Men: 100% Age: 59 ± 7 | 3 | Tanita BC-418 Segmental Body Composition Analyzer/Scale (Tanita Inc. Tokyo, Japan), which has been shown to correlate strongly (r ≥ 0.95, p < 0.001) with both whole-body and regional composition values obtained using the gold standard, dual-energy X-ray absorptiometry (DEXA) | Diet, exercise - Within groups: IG1 (low fat diet) IG2 (low fat diet and exercise) IG3 (carbohydrate-restricted diet) IG4 (carbohydrate-restricted diet and exercise) -Between groups | NO/NO | NO/NO | NO/NO | YES/NO p < 0.01 p < 0.01 p < 0.01 p < 0.01 NS | WC: IG1: 5 cm IG2: 10 cm IG3: 8 cm IG4: 10 cm |
| [46] | South America (Brazil) | RCT | ATPIII | n = 75 IG1: 25 IG2: 25 CG: 25 Men: 65% Age: 30–55 | 12 | Bioelectrical impedance (Omron HBF 306 Bioimpedance Analyzer) and WC was measured between the last rib and the iliac crest | Diet, exercise CG (high CH diet and exercise recommendations) - Within groups: IG1 (low CH diet and walking) IG2 (low CH diet and aerobic exercise) -Between groups | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | BW: IG1: 9 kg IG2: 11 kg CG: 8 kg BF: IG1: 3% IG2: 3% CG: 2% BMI: IG1: 2.9 kg/m2 IG2: 3.5 kg/m2 CG: 2.9 kg/m2 WC: IG1: 14 cm IG2: 14 cm CG: 14 cm |
| [47] | Oceania (Australia) | RCT (parallel group) | ATPIII | n = 38 IG1: 13 IG2: 13 CG: 12 Women: 100% Age: 55 ± 1 | 3 | DEXA scan (GE-LUNAR Prodigy Advance PAþ130510; GE Medical Systems, Lunar, Madison, Wisconsin, USA); BW, using a digital scale. WC at the midpoint between the lowest rib and iliac crest, and hip circumference at the level of the greater trochanters | Diet, exercise - Within groups: IG1 (diet) IG2 (diet and exercise) - Between groups: IG1 vs. IG2 IG1 vs. CG IG2 vs. CG | YES/YES p < 0.001 p < 0.001 p < 0.05 p < 0.01 p < 0.01 | YES/NO p < 0.001 p < 0.001 p < 0.005 p < 0.001 p < 0.001 | YES/NO p < 0.001 p < 0.001 NS p < 0.01 p < 0.00 | YES/NO p < 0.001 p < 0.001 p < 0.01 p < 0.001 p < 0.001 | BW: IG1: 7.9 ± (0.8) kg IG1: 8.2 ± (0.8)% IG2: 10.4 ± (1.1) kgIG2: 10.7 ± (0.8)% BF: IG1: 5.7 ± (0.9) kg IG2: 8.5 ± (1.0) kg BMI: IG1: 2.7 ± (0.3) kg/m2 IG2: 3.4 ± (0.3) kg/m2 WC: IG1: 7.0 ± (0.8) cm IG2: 10.9 ± (1.2) cm |
| [48] | North America (USA) | RCT | ATPIII | n = 24 IG1: 12 IG2: 12 Women: 83% Age: 25–80 | 3 | NE | Diet, exercise - Within groups: IG1 (without interest, for the use of supplementation) IG2 (Mediterranean diet, exercise) - Between groups | NO/YES p < 0.01 p < 0.01 NS | NO/NO | YES/YES p < 0.01 p < 0.01 NS | NO/YES p < 0.01 p < 0.01 NS | BW: IG1: 6.8 ± (1.1)% IG2: 5.2 ± (1.1)%BMI: IG1:2.1 ± (0.3) kg/m2 IG1: 6.7± (0.9)% IG2: 1.8 ± (1.1) kg/m2 IG2: 5.2 ± (1.1)% WC: IG1: 5.9 ± (1.1)% IG2: 5.4 ± (1.1)% |
| [49] | Oceania (Australia) | RCT | ATPIII | n = 59 IG1: 20 IG2: 20 CG: 19 Men: 59% Age: 55 ± 1 | 3 | Dual-energy X-ray absorptiometry scan (GE-LUNAR Prodigy Advance PA+130510; GE Medical Systems, Lunar, Madison, WI); BW was measured using a digital scale and WC was measured at the midpoint between the lowest rib and iliac crest and hip circumference at the level of the greater trochanters | Diet, exercise - Within groups: IG1 (diet) IG2 (diet and exercise) - Between groups: IG1 vs. IG2 IG1 vs. CG IG2 vs. CG | YES/YES p < 0.001/NE p < 0.001/NE NS/NS p < 0.01/NE p < 0.01/NE | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS p < 0.01 p < 0.01 | YES/NO p < 0.001 p < 0.001 p < 0.01 p < 0.01 p < 0.01 | BW: IG1: 7.1 ± (0.6) kg IG1: 7.6 ± (0.7)% IG2: 8.4 ± (0.1) kg IG2: 8.7 ± (0.9)% BF: IG1:5.2 ± (0.7) kg IG2: 6.9 ± (0.9) kg BMI: IG1:2.4 ± (0.2) kg/m2 IG2: 2.8 ± (0.3) kg/m2 WC: IG1: 6.7 ± (0.7) cm IG2: 9.8 ± (1.2) cm |
| [50] | Oceania (Australia) | RCT | ATPIII | n = 34 IG1: 15 IG2: 19 Men: 62% Age: 55 ± 1 | 3 | NE | Diet, exercise - Within groups: IG1 (exercise) IG2 - Between groups | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 NS | NO/NO | YES/NO p < 0.001 p < 0.001 NS | BW: All: 8.2 ± (0.7) kg IG1: 8.4 ± (1.1) kg IG2: 8.1 ± (0.9) kg BF: All: 6.4 ± (0.6) kg IG1: 6.9 ± (1.1) kg IG2: 6.0 ± (0.7) kg WC: All: 8.6 ± (0.8) cm IG1: 9.8 ± (1.3) cm IG2: 7.6 ± (0.9) cm |
| [51] | North America (USA) | RCT | ATPIII | n = 24 IG1: 12 IG2: 12 Women: 62.5% Age: 65.5 ± 5.0 | 3 | Hydrostatic weighing, and fat mass and fat-free mass were estimated using the equation of Siri | Diet, exercise - Within groups: IG1 IG2 (diet) - Between groups | YES/NO p < 0.001 p < 0.001 p < 0.05 | YES/NO p < 0.001 p < 0.001 NS | YES/NO p < 0.001 p < 0.001 p < 0.05 | YES/NO p < 0.001 p < 0.001 NS | BW: IG1: 3.7 ± 3.4 kg IG2: 6.8 ± 2.7 kg BF: IG1: 6.0 kg IG2: 4.5 kg BMI: IG1: 1.3 kg/m2 IG2: 2.4 kg/m2 WC: IG1: 5.6 cm IG2: 6.5 cm |
| [52] | North America (USA) | RCT (parallel-arm) | ATPIII | n = 47 IG1: 24 IG2: 23 Men: 50% Age: 20–65 | 3 | DXA (QDR-4500W; Hologic Corp, Waltham, MA); BW by electronic scale (model CN20; Cardinal/Detecto, Webb City, MO); WC was measured according to guidelines of the National Heart, Lung, and Blood Institute (NHLBI) | Diet, exercise - Within groups: IG1 (without refined grain diet) IG2 (refined grain diet) - Between groups | YES/NO p < 0.001 p < 0.001 NS | YES (%)/NO p < 0.001 p < 0.001 NS | NO/NO | YES/NO p < 0.001 p < 0.001 NS | BW: IG1: 3.7 ± 3.5 kg IG2: 5.3 ± 5.2 kg BF: IG1: 1.2 ± 1.3% IG2: 1.0 ± 1.6% WC: IG1: 2.5 ± 3.7 cm IG2: 4.7 ± 6.4 cm |
| [53] | Asia (Thailand) | RCT | IDF | n = 110 IG1: 52 IG2: 58 Women: 83% Age: 42.5 ± 1.1 | 3 | Body composition were measured using BIA (TANITA® BC-418, Tanita corp., Tokyo, Japan). WC was measured using a no stretchable tape with measurement taken at a horizontal line midway between the highest point of iliac crest and the lowest ribs | Diet, intervention in lifestyle Within IG1: Lifestyle intervention IG2: lifestyle intervention plus meal replacement Between groups: | YES/NO p < 0.01 p < 0.01 p < 0.05 | YES/YES p < 0.01 p < 0.01 NS | YES/NO p < 0.01 p < 0.01 p < 0.05 | YES/NO p < 0.01 p < 0.01 NS | BW: IG1: 1.4 kg IG1: 1.53% IG2: 2.3 kg IG2: 2.86% BF: IG1: 1.05 kg IG1: 0.8% IG2: 1.58 kg IG2: 1% BMIIG1: 0.49 kg/m2 IG2: 0.94 kg/m2 WC IG1: 2.5 cm IG2: 3.25 cm |
| [54] | Asia (Iran) | RCT | ATPIII | n = 117 IG: 64 CG: 53 Men: 66.3% Age: 44.2 (s.d. = 10.0) | 6 | BW by a calibrated scale (Seca, Hamburg, Germany model 8811021658) to the nearest of 0.1 kg; Height by stadiometer (Seca, Hamburg, Germany) to the nearest of 0.1 cm | Diet, intervention in lifestyle - Within groups: IG (My Healthy Heart Profile interactive web) - Between groups | YES/NO p < 0.001 p < 0.05 | NO/NO | YES/NO p < 0.001 NS | NO/NO | BW: IG: 4 kg BMI: IG: 1.2 kg/m2 |
| [55] | Europe (Greece) | RCT | ATP III | n = 47 CG: 13 IG1: 16 IG2: 18 Men: 57% Age: 49.0 ± 11.8 | 6 | Weight and height were measured on a leveled platform scale and a wall-mounted stadiometer, to the nearest 0.5 kg and 0.5 cm; WC was measured in the middle between the 12th rib and the iliac crest | Diet, intervention in lifestyle CG (usual care) - Within groups: IG1 (face-to-face) IG2 (telephone group) - Between groups: IG1 vs. CG IG2 vs. CG | NO/NO | NO/NO | YES/NO p < 0.001 p < 0.001 p < 0.001 p < 0.001 | YES/NO p < 0.001 p < 0.001 p < 0.001 p < 0.05 | BMI: CG: 0.1 ± 1.0 kg/m2 IG1: 1.4 ± 1.5 kg/m2 IG2: 1.2 ± 1.4 kg/m2 WC: CG: 0.5 ± 4.4 cm IG1: 4.1 ± 5.0 cm IG2: 3.5 ± 4.4 cm |
| [56] | South America (Brazil) | RCT | ATP III | n = 58 CG: 17 IG1: 21 IG2: 20 Women: 55.5% Age: 30–59 | 3 | Body weight measured, using a properly calibrated 160 kg Cauduro scale; WC, with a millimeter no extensible long tape at the abdomen’s maximum extension | Diet, exercise, intervention in lifestyle CG: (standard intervention) - Within groups: IG1 (group intervention) IG2 (individual intervention) - Between groups: IG1 vs. CG IG2 vs. CG IG1 vs. IG2 | NO/NO | NO/NO | YES/NO p < 0.01 p < 0.05 p < 0.05 p < 0.05 NS | YES/NO p < 0.05 p < 0.05 p < 0.05 p < 0.05 NS | BMI: IG1: 1.8 kg/m2 IG2: 1.5 kg/m2 WC: IG1: 4.4cm IG2: 5.3cm |
| [57] | Europe (Spain) | RCT | IDF | n = 406 IG: 230 CG: 176 Men: 55% Age: 18–80 | 36 | NE | Diet, exercise, intervention in lifestyle CG: 176 (healthy diet with general physical activity) - Within groups: IG (Mediterranean diet and exercise) - Between groups | YES/NO NE NS | NO/NO | YES/NO NE NS | YES/NO NE p < 0.001 | BW: IG: increase BMI: IG: increase WC: IG: 0.3 ± 6.0 cm |
| [58] | Europe (Germany) | RCT (parallel-group) groups | IDF | n = 178 CG: 60 IG1: 60 IG2: 58 Men: 57% Age: 30–60 | 12 | NE | Diet, exercise, intervention in lifestyle Within groups: IG1 (monitored weekly)IG2 (monitored monthly) - Between groups: IG1 vs. IG2 IG1 vs. CG IG1 vs. CG | YES/NO p < 0.001 p < 0.001 p < 0.05 p < 0.001 p < 0.01 | NO/NO | YES/NO p < 0.001 p < 0.001 p < 0.05 p < 0.001 p < 0.01 | YES/NO p < 0.001 p < 0.001 p < 0.05 p < 0.001 p < 0.05 | BW: IG1: 12.2 kg (8.8–10.5) IG1: 11.4% (9.8–12.9) IG2: 8.8 kg (7.1–10.4) IG2: 8.6% (7–10.2) BMI: IG1: 4.1 kg/m2 (3.6–4.6) IG2: 2.8 kg/m2 (2.3–3.4) WC: IG1: 14.3 cm (12.3–16.3) IG2: 10.8 cm (8.9–12.8) |
| [59] | Oceania (Australia) | RCT | ATP III | n = 66 IG: 31 CG: 35 Women: 68% Age: 18–60 | 12 | Tanita BC-418 segmental body composition analyzer (Tanita Corporation of America Inc., Arlington Heights, IL). WC was measured midway between the top of the iliac crest and the most inferior part of the rib cage | Diet, exercise, intervention in lifestyle IG: without interest, for the use of the gastric balloon - Within groups: CG (diet and exercise) | YES/YES p < 0.05 | NO/NO | YES/NO NE | YES/NO NE | BW: CG: 5.3 kg CG: 5.2% BMI: CG: 1.9 kg/m2 WC: CG: 6.4 cm |
| [60] | Europe (Greece) | RCT | ATP III | n = 88 CG: 29 IG1: 29 IG2: 30 Men: 57% Age: 49.9 ± 10.8 | 6 | BW and height were measured on a levelled platform scale and a wall-mounted stadiometer | Diet, exercise, intervention in lifestyle - Within groups: IG1 (healthy food) IG2 (healthy food and decrease of less healthy food) - Between groups: IG1 vs. CG IG2 vs. CG | NO/NO | NO/NO | YES/NO p < 0.05 p < 0.05 p < 0.05 p < 0.05 | YES/NO p < 0.05 p < 0.05 p < 0.05 p < 0.05 | BMI: CG: 0.1 ± 1.0 kg/m2 IG1: 1.2 ± 1.4 kg/m2 IG2: 1.2 ± 1.4 kg/m2 WC: CG: 0.4 ± 4.4 cm IG1: 3.5 ± 4.4 cm IG2: 3.1 ± 4.0 cm |
| [61] | Asia (South Korea) | RCT | ATPIII | n = 48 IG: 27 CG: 21 Women: 100% Age: 62.7 ± 9.0 | 12 | BW was measured with a high-precision scale (InBody 220; Biospace company, Seoul, Korea); WC was measured midway between the lowest rib and the iliac crest | Diet, exercise, intervention in lifestyle - Within groups: IG - Between groups | YES/NO p < 0.001 p < 0.001 | NO/NO | YES/NO p < 0.001 p < 0.001 | YES/NO p < 0.001 p < 0.001 | BW: IG: 4.3 kg BMI: IG: 1.4 kg/m2 WC: IG: 9.4 cm |
| [62] | Asia (South Korea) | RCT | ATPIII | n = 29 IG: 16 CG: 13 Women: 100% Age: 66.7 ± 9.7 | 1 | BW was measured with a high-precision scale (GM1000; Neo GMTEC, Seoul, Korea); WC was measured midway between the lowest rib and the iliac crest | Diet, exercise, intervention in lifestyle - Within groups: IG - Between groups | YES/NO p < 0.001 p < 0.001 | NO/NO | YES/NO p < 0.001 p < 0.001 | YES/NO p < 0.001 p < 0.001 | BW: IG: 4.6 kg BMI: IG: 2 kg/m2 WC: IG: 6.2 cm |
| Author [67,68,69,70,71,72,73,74] | Recommendations in Dietary Intervention and Exercise | ||
|---|---|---|---|
| Overweight and Obesity | AACE/ACE | [67] | Dietary intervention: energy reduction† and several types of diets stated with indications for different macronutrients (section algorithm: lifestyle therapy); reducing total energy (caloric) intake should be the main component of any weight-loss intervention (grade A; BEL 1); even though the macronutrient composition of meals has less impact on weight loss than adherence rates in most patients. In certain patient populations, modifying macronutrient compositions may be considered to optimize adherence, eating patterns, weight loss, metabolic profiles, risk factor reduction, and/or clinical outcomes (grade A; BEL 1). Physical exercise: recommendations†; resistance training should be prescribed to patients with overweight or obesity undergoing weight-loss therapy to promote fat loss while preserving fat-free mass; involvement of an exercise physiologist or certified fitness professional in the care plan should be considered to individualize the physical activity prescription and improve outcomes (grade A; BEL 1). Behavior interventions: lifestyle therapy in patients with overweight or obesity should include behavioral interventions that enhance adherence to prescriptions for a reduced-calorie meal plan and increased physical activity; behavioral lifestyle intervention and support should be intensified if patients do not achieve a 2.5% weight loss in the first month of treatment, as early weight reduction is a key predictor of long-term weight-loss success (grade A; BEL 1). Degrees of evidence: Origin from American Association of Clinical Endocrinologists 2010 [68]. |
| European Guidelines | [69] | Dietary intervention: energy reduction† (evidence, grade A, B); VLCDs† are unsuitable as a sole source of nutrition for children and adolescents, pregnant or lactating women and the elderly (level 2); the combination of exercise with caloric restriction helps in reducing body weight and body fat and preserving FFM, as compared to diet alone (level 1; grade B) Physical exercise: recommendations† (level 2; grade B) BW: A decrease of 5–15% over a period of 6 months is realistic and of proven health benefit (evidence, level 1)† Levels and degrees of evidence. Origin: [70]. | |
| T2DM | ADA | [71] | Dietary intervention: energy reduction† Physical exercise: recommendations† (grade B) BW: in overweight and obesity with T2DM, a sustained reduction of 5%, improves glycemic control and reduces the need for glucose-lowering drugs; in obese patients with T2DM, weight loss >5% produces benefits in the control of blood glucose, lipids and blood pressure |
| AACE/ACE | [72] | Lifestyle therapy: the key components are medical nutrition therapy, regular physical activity, enough hours of sleep (6–9 h), behavioral support, smoking cessation and avoidance of all tobacco products (this component should be left for the end of the intervention) (see Integral algorithm for the management of type 2 diabetes, prediabetes and obesity). Coulston and his colleagues present another approach in the definition of “medical nutrition therapy” [73]. | |
| MS | [74] | Dietary intervention and physical exercise: recommendations † BW: 7–10% reduction of body weight in a period of 6 to 12 months and achieve an ideal BMI < 25 kg m−2 | |
| AHA/NHLBI | [64] | Dietary intervention: reduction of intake of saturated fat, trans fat, cholesterol Physical exercise: recommendations† BW: 7–10% during the 1 year of therapy, continue with the goal of achieving a desirable weight (BMI < 25 kg m−2) |
| Dietary Intervention | ||
| Energy Density Restriction/Energy Density recommends | Overweight and obesity | ±500–750 kcal day−1 [66]; ± 600 kcal day−1 [69]; 800–1200 kcal day−1 [69] |
| T2DM | ±500–750 kcal day−1 [2017 [71]]/1200–1500 kcal day−1 in women and 1500–1800 kcal day−1 in men [71] | |
| MS | Reduction of 500–1000 kcal day−1 [74] | |
| VLCD | Overweight and obesity | <800 kcal day−1 [69] |
| T2DM and MS | ND | |
| Macronutrients and diets | Overweight and obesity | Different amounts of macronutrients (hydrates, proteins and fats) and giving rise to different types of diets [66]; hypocaloric balanced diets result in clinically significant weight loss independent of macronutrients [69] |
| T2DM and MS | Recommended diets may differ in advising foods high in fat or in hydrates; the recommendation for consumption of recommended foods does not differ: whole grains, vegetables, fruits, legumes, low-fat dairy products, lean meats, nuts and seeds; it is recommended to adapt the diet to the health status and the preferences of the patient [64,71,74] | |
| Physical Exercise | ||
| Overweight and obesity | Aerobic exercise > 150 min wk−1 (3 to 5 days wk−1) [67]; moderate aerobic exercise: 150 min wk−1 (energetically walking) [69] | |
| T2DM | Greater than or equal to 150 min of physical exercise a week at moderate intensity, 3 days a week at least; In the US Department of Health, does not differentiate between indications for T1DM and T2DM [71]; 150 min wk−1 moderate effort; strength training and increase according to each individual [72] | |
| MS | ≥30 to 60 min of exercise (moderate intensity on most days of the week, according to each individual) [74]; ≥30 min from 5 days wk−1 continuous or intermittent (and preferably ≥60 min and moderate intensity) [64] | |
| Lifestyle Modification Program [72] | Duration | Body Composition vs. Duration [83,98] | Comments [86] | Initial Assessment and Monitoring Questionnaires |
|---|---|---|---|---|
| Multiannual | Several years (2–4 years) | Must depend on excess of weight (corresponding to body fat). | In this program, the subject may evolve from one stage to another (initiation, improvement or maintenance). | Activity or exercise measurement: Triaxial accelerometers are recommended [92] Food ingestion [101,102] Alcohol consumption [103] |
| Macrocycle | Several months | Considerable reduction in body fat per stage (≥ 5%). | Each macrocycle must be identified by one stage, therefore one year may have several macrocycles. | To apply questionnaires or measuring instruments as much as necessary |
| Mesocycle | Several weeks | Objectives of body fat variation should initially be measured by the kilos, but over time, the percentage should be used as the most recommended unit of measure | Weekly planning: a. variation in energy intake, macronutrients; b. in physical exercise (Table 5) [81]; c. sleep quality; d. alcohol consumption. | |
| Microcycle | Several days | It is not recommended to use body composition measuring instruments. | It is important to measure dietary intake, physical exercise characteristics (Table 5), sleep hours and alcohol consumption (extra caloric intake) | |
| Routine of one or more consultation sessions | Several hours and minutes | The evolution of body composition, body fat and other anthropometric parameters will be analyzed. | A break in training lasting more than 40 min qualifies as two separate workouts. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albert Pérez, E.; Poveda González, M.; Martínez-Espinosa, R.M.; Molina Vila, M.D.; Reig García-Galbis, M. Practical Guidance for Interventions in Adults with Metabolic Syndrome: Diet and Exercise vs. Changes in Body Composition. Int. J. Environ. Res. Public Health 2019, 16, 3481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183481
Albert Pérez E, Poveda González M, Martínez-Espinosa RM, Molina Vila MD, Reig García-Galbis M. Practical Guidance for Interventions in Adults with Metabolic Syndrome: Diet and Exercise vs. Changes in Body Composition. International Journal of Environmental Research and Public Health. 2019; 16(18):3481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183481
Chicago/Turabian StyleAlbert Pérez, Enrique, Marina Poveda González, Rosa María Martínez-Espinosa, Mariola D Molina Vila, and Manuel Reig García-Galbis. 2019. "Practical Guidance for Interventions in Adults with Metabolic Syndrome: Diet and Exercise vs. Changes in Body Composition" International Journal of Environmental Research and Public Health 16, no. 18: 3481. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph16183481